Mastering Wrist Arthroscopy: A Comprehensive Surgical Guide
Key Takeaway
Wrist arthroscopy has evolved into an indispensable diagnostic and therapeutic modality in orthopedic surgery. This comprehensive guide details the precise indications, intricate portal anatomy, and step-by-step surgical techniques required for successful radiocarpal and midcarpal evaluation. By mastering patient positioning, fluid management, and instrument triangulation, surgeons can effectively manage complex carpal instability, triangular fibrocartilage complex (TFCC) tears, and intra-articular fractures while minimizing iatrogenic complications.
INTRODUCTION TO WRIST ARTHROSCOPY
Wrist arthroscopy has fundamentally transformed the diagnostic and therapeutic landscape of hand and upper extremity surgery. Originally conceived as a purely diagnostic adjunct, advancements in optical technology, fluid management, and miniaturized instrumentation have elevated wrist arthroscopy to a primary therapeutic modality. For the modern orthopedic surgeon, mastery of wrist arthroscopy is essential for the management of complex carpal kinematics, ligamentous instability, and intra-articular fractures.
This comprehensive guide elucidates the evidence-based indications, precise portal anatomy, biomechanical considerations, and step-by-step surgical techniques required to perform wrist arthroscopy safely and effectively.
INDICATIONS AND CLINICAL UTILITY
The indications for wrist arthroscopy have expanded exponentially. While advanced imaging modalities such as high-resolution MRI and triple-injection cinearthrography provide valuable data, arthroscopy remains the gold standard for evaluating the dynamic stability of the carpus and the structural integrity of the articular surfaces.
Diagnostic Indications
- Evaluation of Chronic Wrist Pain: Arthroscopy is invaluable when clinical examination and advanced imaging yield equivocal results. Studies by Adolfsson demonstrated that arthroscopy identifies the etiology of chronic wrist pain in up to 70% of previously undiagnosed patients.
- Assessment of Ligamentous Integrity: Arthroscopy provides superior diagnostic accuracy over arthrography for identifying the exact location, size, and dynamic significance of Triangular Fibrocartilage Complex (TFCC) tears, Scapholunate (SL) interosseous ligament injuries, and Lunotriquetral (LT) ligament tears.
- Chondral Surface Evaluation: Direct visualization allows for the precise grading of chondromalacia and osteochondral lesions, which is critical for preoperative planning in joint-preserving procedures.
Therapeutic Indications
- TFCC Management: Arthroscopic debridement of central perforations and repair of peripheral (vascular zone) tears.
- Carpal Instability: Debridement of partial SL or LT ligament tears, thermal shrinkage (though used with caution), and arthroscopically assisted percutaneous pinning.
- Fracture Management: Arthroscopically assisted reduction and internal fixation (ARIF) of intra-articular distal radius fractures, scaphoid fractures, and perilunate fracture-dislocations. It ensures anatomic restoration of the articular step-off and allows concurrent management of associated soft-tissue injuries.
- Bone Excision Procedures: Radial styloidectomy, partial distal ulnar resection (wafer procedure), proximal row carpectomy, and excision of the proximal pole of the scaphoid.
- Synovial and Soft Tissue Pathology: Synovectomy for inflammatory arthritides, lavage of septic arthritis, release of intra-articular adhesions, and dorsal ganglion excision.
💡 Clinical Pearl: Diagnostic Superiority
Chung, Zimmerman, and Travis compared triple-injection arthrography with wrist arthroscopy in 150 patients, revealing that over 50% of patients had their arthrographic diagnoses altered following arthroscopic evaluation. Arthroscopy remains the definitive diagnostic arbiter for intrinsic carpal ligament pathology.
SURGICAL ANATOMY AND BIOMECHANICS
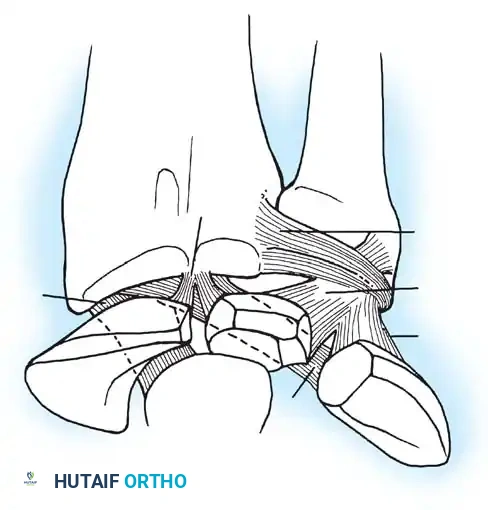
A profound understanding of the dorsal extensor compartments and the underlying capsuloligamentous structures is non-negotiable for safe portal placement. The radiocarpal joint is a complex, multi-axial articulation. The distal radius possesses a normal volar tilt of 11 to 12 degrees and a radial inclination of 22 degrees. This osseous geometry dictates the trajectory of instrument insertion; all radiocarpal portals must be established with a corresponding 10 to 15-degree volar and proximal angulation to avoid iatrogenic scuffing of the articular cartilage.
The intrinsic and extrinsic ligaments of the wrist form a complex stabilizing network. The volar extrinsic ligaments (e.g., radioscaphocapitate, radiolunotriquetral) are stout and provide primary stability, while the dorsal ligaments are thinner. Arthroscopic evaluation allows direct probing of the SL and LT interosseous ligaments to assess for dynamic widening (the "drive-through" sign).
EQUIPMENT AND INSTRUMENTATION
Successful wrist arthroscopy requires specialized, small-joint equipment designed to navigate the tight confines of the carpus without causing iatrogenic trauma.
Optical and Visual Equipment
- Arthroscope: A 2.5 mm to 3.0 mm diameter arthroscope with a 30-degree lens-offset angle is optimal for routine radiocarpal and midcarpal evaluation. A 1.7 mm or 1.9 mm scope may be utilized for the distal radioulnar joint (DRUJ) or in severely contracted wrists. A 70-degree scope is occasionally useful for visualizing the volar capsule or the foveal attachment of the TFCC.
- Camera and Illumination: A high-definition, solid-state chip television camera coupled with a high-intensity xenon or LED light source.
Fluid Management
- Irrigation System: While gravity feed can be satisfactory, a dedicated mechanical infusion pump is vastly superior. It maintains a constant intra-articular pressure (typically 30-40 mm Hg) and flow rate, optimizing visualization while clearing debris during motorized resection.
- Warning: Strict monitoring of fluid extravasation is mandatory to prevent forearm compartment syndrome, particularly during fracture management where capsular integrity is compromised.
Surgical Instruments
- Manual Instruments: 2.0 mm to 3.0 mm basket forceps (straight and rotary), grasping forceps, and a specialized small-joint probe (1.5 mm diameter, 40 mm length with a shallow hook).
- Motorized Shavers: 2.0 mm to 3.0 mm full-radius resectors and burrs.
- Advanced Modalities: Holmium:YAG (Ho:YAG) lasers and radiofrequency (RF) wands are utilized for synovectomy and tissue ablation. However, thermal devices must be used judiciously; Pell and Uhl reported severe complications, including tendon ruptures and full-thickness skin burns, associated with excessive thermal energy.
PATIENT POSITIONING AND SETUP
Meticulous patient positioning is the foundation of a successful procedure. Wrist arthroscopy is typically performed under regional anesthesia (brachial plexus block) or general anesthesia, depending on the anticipated duration and the need for concurrent procedures (e.g., bone grafting).
Step-by-Step Positioning
- Patient Orientation: Place the patient supine on the operating table. The operative arm is abducted and placed on a radiolucent hand table.
- Tourniquet Application: Apply a well-padded pneumatic tourniquet to the proximal arm. While optional for simple diagnostic procedures, it is highly recommended for therapeutic interventions and fracture management to ensure a bloodless field.
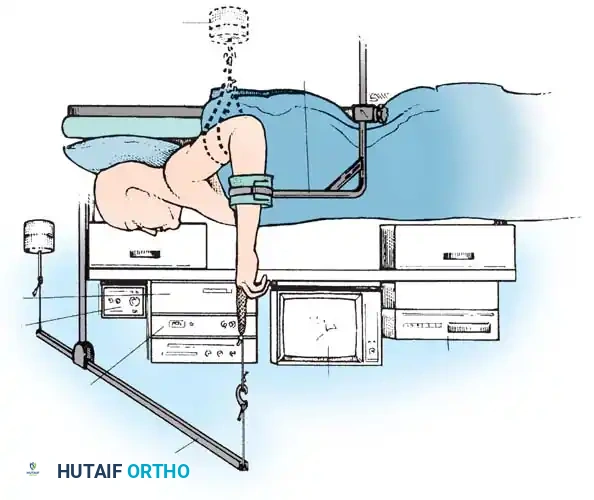
- Traction Setup: Suspend the hand using sterile finger-traps applied to the index and long fingers (and occasionally the thumb).
- Distraction: Apply 5 to 10 lbs (2.2 to 4.5 kg) of longitudinal traction. This can be achieved via an overhead pulley system with counterweights or a dedicated robotic/mechanical traction tower.
- Joint Angulation: Maintain the elbow in 90 degrees of flexion to neutralize the deforming forces of the forearm musculature. The wrist should be in neutral to slight flexion (10-20 degrees) to open the dorsal radiocarpal space.
- Alternative Position: The horizontal position (elbow extended, forearm pronated on the hand table with longitudinal traction) may be utilized, particularly when arthroscopy is combined with volar plating of distal radius fractures.
🚨 Surgical Warning: Traction Complications
Excessive traction weight (>10 lbs) or prolonged traction time (>2 hours) significantly increases the risk of neurapraxia, skin sloughing at the finger-traps, and postoperative joint stiffness. Always use the minimum weight necessary to achieve adequate joint distraction.
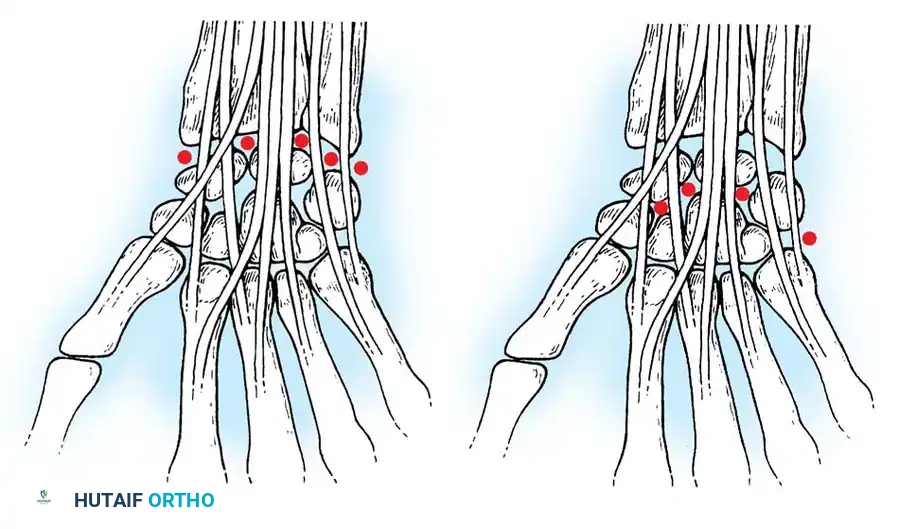
PORTAL ANATOMY AND PLACEMENT
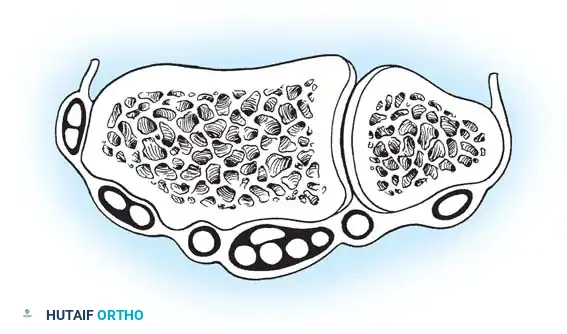
Wrist arthroscopy portals are anatomically defined by their relationship to the six dorsal extensor compartments. Precise portal placement is critical to avoid injury to cutaneous nerves, extensor tendons, and articular cartilage.
Radiocarpal Portals
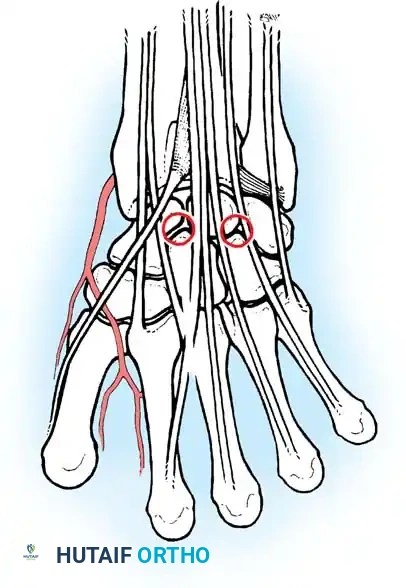
- 1-2 Portal: Located between the first compartment (APL, EPB) and the second compartment (ECRL, ECRB). It is situated in the anatomic snuffbox. Risk: The superficial branch of the radial nerve (SBRN) and the radial artery.
- 3-4 Portal: The primary viewing portal. Located between the third compartment (EPL) and the fourth compartment (EDC), just distal to Lister's tubercle. It provides an excellent panoramic view of the SL ligament, volar ligaments, and the radial aspect of the TFCC.
- 4-5 Portal: The primary working portal. Located between the fourth compartment (EDC) and the fifth compartment (EDM). It provides direct access to the TFCC and the LT ligament.
- 6R Portal: Located immediately radial to the sixth compartment (ECU tendon). Used for viewing the ulnar periphery of the TFCC and the ulnocarpal ligaments.
- 6U Portal: Located immediately ulnar to the ECU tendon. Risk: The dorsal sensory branch of the ulnar nerve (DSBUN).
Midcarpal Portals
The midcarpal joint is a separate synovial cavity and must be evaluated independently to assess the distal aspects of the SL and LT ligaments and the capitohamate articulation.
* Midcarpal Radial (MCR) Portal: Located approximately 1 cm distal to the 3-4 portal, in a palpable soft depression between the capitate, scaphoid, and lunate. It is in line with the radial border of the third metacarpal.
* Midcarpal Ulnar (MCU) Portal: Located approximately 1 cm distal to the 4-5 portal, aligned with the axis of the fourth metacarpal, providing access to the triquetrohamate and lunotriquetral articulations.
Volar Portals
While less commonly used, volar portals (volar radial and volar ulnar) are gaining traction for specific indications, such as evaluating dorsal capsular avulsions or repairing volar TFCC tears. These require meticulous blunt dissection due to the proximity of major neurovascular bundles (radial artery, median nerve, ulnar artery/nerve).
SURGICAL TECHNIQUE: DIAGNOSTIC RADIOCARPAL EXAMINATION
A systematic, reproducible approach is mandatory to ensure no pathology is overlooked.
Step 1: Surface Anatomy and Marking
Before exsanguination and tourniquet inflation, meticulously palpate and mark the surface landmarks: Lister's tubercle, the distal radius articular margin, the ulnar head, the ECU tendon, and the anticipated portal sites.
Step 2: Joint Distension
- Identify the 3-4 portal site.
- Insert an 18-gauge needle attached to a 10 mL syringe of normal saline.
- Crucial Angulation: Angle the needle 10 to 15 degrees proximally and volarly to match the anatomic tilt of the distal radius.
- Inject 5 to 10 mL of saline. A distinct "flash" of fluid or easy distension confirms intra-articular placement. The wrist will visibly swell dorsally.
Step 3: Establishing the Viewing Portal (3-4 Portal)
- Remove the needle and make a transverse or longitudinal skin incision (approximately 3-4 mm) using a No. 11 scalpel blade. Only incise the epidermis.
- Use a small, curved hemostat to bluntly dissect through the subcutaneous tissue down to the dorsal capsule. Spread the hemostat parallel to the extensor tendons to protect the cutaneous nerves and retract the EPL radially.
- Puncture the dorsal capsule with the hemostat or the sharp tip of the No. 11 blade.
- Insert the arthroscopic cannula with a blunt obturator to prevent iatrogenic scuffing of the scaphoid or lunate cartilage.
- Remove the obturator, insert the arthroscope, and establish inflow.
Step 4: Establishing the Working Portal (4-5 or 6R Portal)
- Under direct intra-articular visualization, localize the 4-5 portal using an 18-gauge spinal needle (outside-in technique).
- Ensure the needle trajectory allows adequate triangulation with the arthroscope.
- Make a skin incision, perform blunt dissection with a hemostat, and introduce the working cannula and probe.
Step 5: The Systematic Sweep
Perform a comprehensive 21-point examination of the radiocarpal joint:
* Radial Gutter: Assess the radial styloid, radioscaphocapitate ligament, and long radiolunate ligament.
* Scaphoid and Lunate: Evaluate the chondral surfaces and the proximal membranous portion of the SL interosseous ligament. Use the probe to test for SL ballottement.
* Volar Capsule: Inspect the short radiolunate, ulnolunate, and ulnotriquetral ligaments.
* Ulnar Periphery: Evaluate the articular disc of the TFCC. Probe the central avascular zone for perforations and the peripheral vascular zone for detachments (the "trampoline test").
Step 6: Midcarpal Examination
Following the radiocarpal sweep, the scope is withdrawn, and the midcarpal joint is accessed via the MCR portal using the same blunt dissection technique. The midcarpal joint is essential for diagnosing dynamic carpal instability. The SL and LT intervals are probed; a probe should not easily pass between the carpal bones (a positive "drive-through" sign indicates significant ligamentous disruption).
COMPLICATIONS AND RISK MANAGEMENT
While generally safe, wrist arthroscopy carries a complication rate ranging from 1.2% to 5.2%. Warhold and Ruth categorized these complications into four distinct domains:
- Traction and Positioning Complications:
- Skin sloughing or blistering from finger-traps.
- Neurapraxia of the digital nerves or brachial plexus due to excessive weight or prolonged surgical time.
- Postoperative joint stiffness.
- Portal and Insertion Complications:
- Nerve Injury: The SBRN is highly vulnerable at the 1-2 portal, and the DSBUN is at risk at the 6U portal. Strict adherence to blunt subcutaneous dissection is mandatory.
- Tendon Injury: Laceration of the EPL or EDC tendons from overzealous use of the scalpel or motorized shavers.
- Cartilage Damage: Iatrogenic scuffing of the convex proximal carpal row from improper trocar insertion angles.
- Procedure-Related Complications:
- Fluid Extravasation: Can lead to acute forearm compartment syndrome, especially during arthroscopic management of distal radius fractures where the capsule is torn. Gravity outflow or meticulous pump pressure monitoring is critical.
- Hardware complications during percutaneous pinning (e.g., K-wire migration, sensory nerve impingement).
- General Arthroscopic Complications:
- Equipment failure (e.g., broken probe tips within the joint).
- Postoperative infection (septic arthritis).
💡 Clinical Pearl: Avoiding Extravasation
When performing arthroscopy for acute fractures, limit fluid pressure to the absolute minimum required for visualization. Frequently palpate the volar forearm. If the forearm becomes tense, immediately abort fluid inflow, switch to a "dry" arthroscopy technique, or proceed to open management.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Postoperative management is highly contingent upon the specific therapeutic interventions performed.
- Diagnostic Arthroscopy / Simple Debridement: The wrist is placed in a bulky soft dressing or a removable volar splint. Immediate active range of motion (ROM) of the digits is encouraged. Wrist ROM exercises commence at 3 to 5 days postoperatively. Strengthening begins at 3 to 4 weeks.
- TFCC Repair: The wrist is immobilized in a Muenster-style cast or a long-arm splint in neutral rotation for 4 to 6 weeks to protect the peripheral repair. Gradual progression of pronation/supination begins at 6 weeks, with full unrestricted activity delayed until 10 to 12 weeks.
- Ligamentous Pinning (SL/LT): K-wires are typically left in place for 8 weeks. The wrist is strictly immobilized in a short-arm cast. Following pin removal, an aggressive, therapist-directed rehabilitation program is initiated to restore radiocarpal and midcarpal kinematics.
By adhering to strict anatomical principles, utilizing appropriate instrumentation, and maintaining a high index of suspicion for potential complications, the orthopedic surgeon can leverage wrist arthroscopy to deliver superior clinical outcomes in the management of complex carpal pathology.
You Might Also Like