Arthroscopic Transosseous Repair of Foveal Detachments of the Triangular Fibrocartilage Complex
Key Takeaway
Arthroscopic transosseous repair of foveal detachments of the triangular fibrocartilage complex (TFCC) restores distal radioulnar joint (DRUJ) stability. This advanced technique utilizes a specialized targeting guide to create transosseous tunnels through the ulnar fovea. By passing nonabsorbable sutures through the TFCC and securing them to the ulnar cortex, anatomic reduction of the radioulnar ligaments is achieved, facilitating robust biological healing and functional recovery.
INTRODUCTION TO TFCC FOVEAL DETACHMENTS
The triangular fibrocartilage complex (TFCC) is the primary stabilizer of the distal radioulnar joint (DRUJ) and the ulnocarpal articulation. Foveal detachments of the TFCC—often classified under the Palmer classification as 1B tears, and more specifically delineated by the Atzei classification as Class 2 or 3 lesions—represent a complete avulsion of the deep radioulnar ligaments (RULs) from their anatomic footprint at the ulnar fovea.
Because the deep fibers of the TFCC insert into the fovea at the axis of forearm rotation, their detachment leads to profound DRUJ instability, ulnar-sided wrist pain, and significant functional impairment. While peripheral capsular repairs are sufficient for superficial tears, true foveal detachments require anatomic reattachment to the bone to restore the isometric stabilizing function of the RULs. Arthroscopic transosseous repair offers a minimally invasive, biologically robust solution that promotes direct tendon-to-bone healing while preserving the surrounding capsular anatomy.
SURGICAL ANATOMY AND BIOMECHANICS
The Ulnar Fovea and Radioulnar Ligaments
The TFCC is a complex, three-dimensional structure comprising the articular disc, the dorsal and volar radioulnar ligaments, the meniscus homologue, the ulnocarpal ligaments, and the extensor carpi ulnaris (ECU) subsheath.
The radioulnar ligaments possess two distinct insertions on the ulna:
1. Superficial Fibers: Insert onto the base and body of the ulnar styloid. These fibers primarily stabilize the ulnocarpal joint.
2. Deep Fibers (Ligamentum Subcruentum): Insert into the ulnar fovea, a distinct depression located at the base of the ulnar styloid.
Clinical Pearl: The foveal insertion is the true isometric center of DRUJ rotation. Biomechanical studies consistently demonstrate that the deep foveal fibers are the critical stabilizers of the DRUJ during pronation and supination. Failure to recognize and anatomically repair a foveal avulsion will result in persistent DRUJ instability, regardless of superficial capsular repair.
Kinematics of the DRUJ
During forearm rotation, the radius translates and rotates around the fixed ulna. The dorsal and volar RULs experience reciprocal tensioning. In supination, the volar RUL is taut; in pronation, the dorsal RUL is taut. Anatomic transosseous repair to the fovea restores this reciprocal tensioning mechanism, preventing dorsal or volar subluxation of the ulnar head.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Acute or Chronic Foveal Detachment: Confirmed via clinical examination (positive DRUJ ballottement test) and advanced imaging (MRI/MR Arthrogram).
- Persistent DRUJ Instability: Symptomatic instability that has failed conservative management (immobilization, physical therapy).
- Atzei Class 2 and 3 Tears: Repairable deep foveal avulsions with or without concurrent superficial tears.
Contraindications
- Absolute:
- Advanced DRUJ osteoarthritis.
- Fixed, irreducible DRUJ subluxation or dislocation.
- Active local or systemic infection.
- Relative:
- Severe ulnar positive variance (>2 mm) causing ulnocarpal impaction syndrome (may require a concurrent ulnar shortening osteotomy).
- Poor bone quality at the ulnar fovea (e.g., severe osteopenia or cystic changes) that may compromise transosseous suture fixation.
PREOPERATIVE PLANNING AND IMAGING
A thorough clinical examination is paramount. The "fovea sign" (tenderness in the soft spot between the ulnar styloid, FCU tendon, volar surface of the ulnar head, and pisiform) is highly sensitive for foveal pathology. DRUJ ballottement in neutral, full pronation, and full supination must be compared to the contralateral wrist.
Standard posteroanterior (PA) and lateral radiographs evaluate ulnar variance and rule out fractures. High-resolution MRI (preferably a 3-Tesla MR arthrogram) is the gold standard for visualizing the deep fibers of the TFCC and confirming the foveal avulsion.
PATIENT POSITIONING AND SETUP
- Anesthesia: Regional anesthesia (supraclavicular or axillary brachial plexus block) combined with intravenous sedation or general anesthesia.
- Positioning: The patient is placed supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm.
- Traction: The hand is placed in a specialized wrist arthroscopy traction tower. Chinese finger traps are applied to the index and middle fingers. Approximately 10 to 15 lbs (4.5–6.8 kg) of longitudinal traction is applied to distract the radiocarpal and midcarpal joints.
- Preparation: The arm is prepped and draped in a standard sterile fashion.
DIAGNOSTIC ARTHROSCOPY
Before proceeding with the transosseous repair, a comprehensive diagnostic arthroscopy is performed to confirm the foveal detachment and assess for concomitant intra-articular pathology.
- Radiocarpal Joint Assessment: The arthroscope is introduced through the standard 3-4 portal. The 4-5 or 6R portal is established as the primary working portal.
- The Trampoline Test: A probe is used to assess the tension of the TFCC articular disc. A loss of the normal elastic rebound (a "positive trampoline test") indicates a loss of peripheral or foveal tethering.
- The Hook Test: The probe is inserted through the 4-5 or 6R portal and hooked under the ulnar border of the TFCC. If the TFCC can be easily pulled proximally and radially toward the center of the joint, a foveal detachment is confirmed.
- DRUJ Assessment: If necessary, the arthroscope can be introduced into the distal radioulnar joint via the proximal DRUJ portal to directly visualize the bare fovea.
Surgical Warning: Care must be taken when establishing the 6R and 6U portals to avoid injury to the dorsal ulnar sensory nerve (DUSN). Blunt dissection with a hemostat down to the capsule is mandatory before introducing the trocar.
STEP-BY-STEP SURGICAL TECHNIQUE: ARTHROSCOPIC TRANSOSSEOUS REPAIR
Once a foveal detachment is confirmed, the procedure transitions to the transosseous repair utilizing a specialized targeting guide (e.g., Nakashima Medical, Okayama, Japan).
Step 1: Preparation of the Foveal Footprint
Using a motorized shaver or an arthroscopic burr introduced through the 4-5 or 6R portal, the ulnar fovea is meticulously debrided of fibrous scar tissue. The bone must be decorticated to a bleeding cancellous bed to optimize biological tendon-to-bone healing.
Step 2: Ulnar Cortical Approach
- Identify the tip of the ulnar styloid via palpation and fluoroscopy.
- Make a 1-cm longitudinal incision on the ulnar side of the distal ulna, precisely 15 mm proximal to the tip of the ulnar styloid.
- Carefully dissect through the subcutaneous tissue, protecting the branches of the DUSN.
- Develop the interval between the extensor carpi ulnaris (ECU) and the flexor carpi ulnaris (FCU).
- Incise and elevate the periosteum off the ulnar cortex to expose the bone for drilling and subsequent suture knot tying.
Step 3: Targeting and Transosseous Drilling
- Introduce the specialized targeting device (Nakashima Medical guide) through the 4-5 or 6R portal.
- Position the small intra-articular spike of the target device precisely on the ulnar half of the triangular fibrocartilage, directly overlying the anatomic foveal footprint.
- Align the extra-articular drill sleeve with the exposed ulnar cortex at the 1-cm incision site.
- Using a 1.2-mm Kirschner wire (K-wire), drill the first transosseous tunnel from the ulnar cortex, aiming distally and radially, exiting precisely at the fovea and penetrating the ulnar half of the TFCC.
- Leave the first K-wire in place or use a specialized drill sleeve to maintain the tunnel.
- Adjust the targeting guide slightly (approximately 3–4 mm adjacent to the first hole) and drill a second 1.2-mm transosseous tunnel in the same manner, creating a robust bony bridge on the ulnar cortex.
Pitfall: Ensure the bony bridge between the two drill holes on the ulnar cortex is at least 3 to 4 mm wide. A bridge that is too narrow risks cortical blowout during suture tensioning, which will compromise the entire repair.
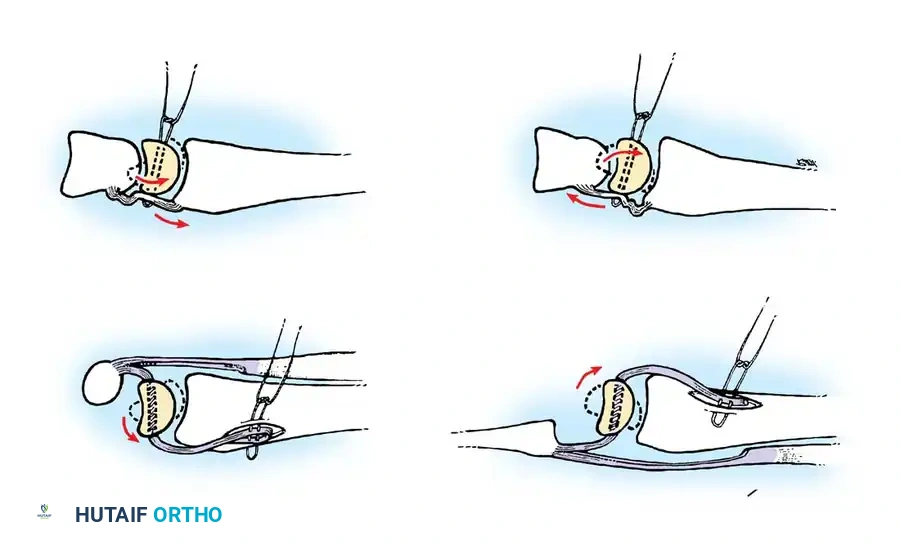
Step 4: Suture Passing and Relaying
- Remove the K-wires.
- Pass a 21-gauge spinal needle through the first transosseous tunnel from the outside (ulnar cortex) into the radiocarpal joint, penetrating the TFCC.
- Feed a looped 4-0 nylon suture (or a dedicated nitinol wire loop) through the needle into the joint to act as a shuttle.
- Repeat this process for the second tunnel, passing another looped 4-0 nylon suture.
- Using blunt mosquito forceps or an arthroscopic grasper, retrieve both looped nylon sutures through the 4-5 or 6R portal.
Step 5: Suture Management and TFCC Advancement
- Outside the 4-5 or 6R portal, thread two strands of heavy, nonabsorbable 3-0 polyester (or ultra-high-molecular-weight polyethylene) sutures through the retrieved nylon loops.
- Place proximal traction on the extra-articular ends of the nylon looped sutures at the ulnar cortex.
- This action shuttles the permanent 3-0 polyester sutures through the 4-5/6R portal, into the radiocarpal joint, down through the substance of the TFCC, and out through the transosseous tunnels to the ulnar cortex.
- The result is a horizontal mattress suture configuration capturing the deep fibers of the TFCC.
Step 6: Tensioning, Fixation, and DRUJ Transfixation
- Release the arm from the traction tower.
- Assess the DRUJ stability. Supinate the forearm to a neutral or slightly supinated position to approximate the TFCC to the fovea.
- Apply firm, even tension to the polyester sutures exiting the ulnar cortex. Arthroscopic visualization will confirm the TFCC being drawn down tightly against the decorticated foveal footprint.
- Tie the sutures securely over the cortical bone bridge.
- DRUJ Transfixation: To protect the repair during the initial healing phase, reduce the DRUJ in neutral rotation and percutaneously drive a 1.5-mm (0.062-inch) K-wire transversely from the distal ulna into the distal radius, just proximal to the DRUJ.
- Cut the transfixation pin outside the skin and bend it for easy removal in the clinic.
- Close the portals and the ulnar incision with nonabsorbable skin sutures.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is critical to ensure biological healing of the transosseous repair while preventing debilitating wrist stiffness.
Phase 1: Maximum Protection (Weeks 0 to 4)
- Immobilization: Immediately postoperatively, the patient is placed in a well-padded long-arm cast or a rigid sugar-tong splint with the forearm in neutral rotation.
- Suture Removal: Skin sutures are removed at 10 to 14 days postoperatively. The cast is changed, ensuring the forearm remains immobilized in neutral rotation.
- Pin Management: The DRUJ transfixation pin remains in place to neutralize rotational forces across the healing foveal footprint.
- Activity: Active range of motion (ROM) of the digits, thumb, elbow, and shoulder is encouraged immediately to prevent secondary stiffness and reduce edema.
Phase 2: Pin Removal and Transition (Week 4 to 6)
- Pin Removal: At exactly 4 weeks post-surgery, the radioulnar transfixation pin is removed in the clinic.
- Immobilization: Following pin removal, a short-arm cast or a rigid Munster-style splint is applied for an additional 2 weeks. Forearm rotation is still strictly prohibited.
Phase 3: Early Mobilization (Weeks 6 to 10)
- Immobilization: The cast is completely removed at 6 weeks. The patient is transitioned to a custom-molded, removable wrist splint.
- Rehabilitation: A therapist-supervised rehabilitation program is initiated.
- Range of Motion: Gentle, active-assisted ROM exercises for wrist flexion/extension and forearm pronation/supination begin.
- Restrictions: Forceful pronation, forceful supination, and heavy grasping must be strictly avoided.
Phase 4: Strengthening and Return to Activity (Weeks 10 to 12+)
- Strengthening: At 10 to 12 weeks, progressive isometric and isotonic strengthening exercises are introduced. Focus is placed on the ECU and pronator quadratus to provide dynamic DRUJ stability.
- Return to Play/Work: Unrestricted activities, heavy lifting, and return to contact sports are generally permitted between 4 to 6 months postoperatively, contingent upon the restoration of painless, stable DRUJ kinematics and near-normal grip strength.
COMPLICATIONS AND MANAGEMENT
While arthroscopic transosseous repair is highly effective, surgeons must be vigilant regarding potential complications:
- Dorsal Ulnar Sensory Nerve (DUSN) Injury: The DUSN is highly vulnerable during the creation of the 6R/6U portals and the ulnar cortical incision. Meticulous blunt dissection and the use of drill guides are mandatory. Neuropraxia usually resolves, but a transected nerve may lead to painful neuromas requiring surgical excision.
- Cortical Blowout: Drilling the transosseous tunnels too close together can fracture the bony bridge. If this occurs, the surgeon must convert to a suture anchor technique placed directly into the fovea.
- Hardware Irritation / ECU Tendinitis: Sutures tied over the ulnar cortex can occasionally irritate the overlying ECU tendon. Ensuring the knots are buried deep to the periosteum minimizes this risk.
- Postoperative Stiffness: Prolonged immobilization can lead to severe pronosupination stiffness. Strict adherence to the timeline for pin removal (4 weeks) and initiation of therapy (6 weeks) is crucial.
- Recurrent Instability: Failure of the repair can occur due to noncompliance with postoperative restrictions, poor tissue quality, or failure to recognize and treat concurrent ulnar positive variance. Revision surgery may require open reconstruction using tendon autografts (e.g., Adams-Berger procedure).
You Might Also Like