Arthroscopic Management of Triangular Fibrocartilage Complex Tears: Débridement and Foveal Repair
Key Takeaway
Arthroscopic management of triangular fibrocartilage complex (TFCC) tears requires precise portal placement and meticulous evaluation of the distal radioulnar joint. Central Palmer Class 1A lesions are treated with arthroscopic débridement, preserving a 2-mm peripheral rim to maintain biomechanical stability. Conversely, Class 1B foveal detachments necessitate transosseous or anchor-based repair to restore DRUJ kinematics. Concurrent ulnar styloid fractures and extensor carpi ulnaris tendon subluxations must be addressed simultaneously to ensure optimal functional outcomes.
Introduction to Triangular Fibrocartilage Complex (TFCC) Pathology
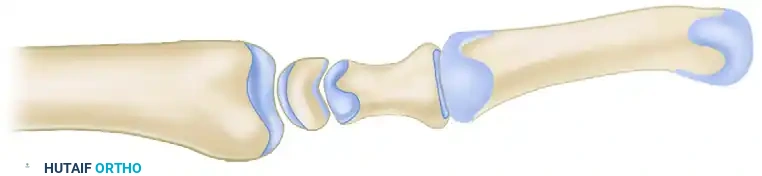
The triangular fibrocartilage complex (TFCC) is the primary stabilizer of the distal radioulnar joint (DRUJ) and serves as a critical load-bearing structure for the ulnocarpal articulation. It transmits approximately 20% of the axial load from the carpus to the forearm, with the remaining 80% passing through the radiocarpal joint. Pathologic lesions of the TFCC are broadly categorized by the Palmer classification system into traumatic (Class 1) and degenerative (Class 2) tears.
Arthroscopic intervention has become the gold standard for both the definitive diagnosis and surgical management of TFCC pathology. Central articular disc tears (Palmer Class 1A) are largely avascular and lack healing potential, making them ideal candidates for arthroscopic débridement. In contrast, peripheral tears, particularly ulnar-sided foveal detachments (Palmer Class 1B), occur in the vascularized zone of the complex and require anatomical repair to restore DRUJ stability.
This comprehensive guide details the surgical techniques for arthroscopic débridement of central TFCC tears and the transosseous repair of foveal detachments, alongside critical perioperative considerations.
Preoperative Evaluation and Indications
Clinical Examination
A meticulous clinical examination is paramount. The surgeon must evaluate for:
* Ulnar-Sided Wrist Pain: Exacerbated by pronation, supination, and ulnar deviation (ulnocarpal impaction test).
* Mechanical Symptoms: The presence of crepitus, "clicks," or catching during forearm rotation.
* DRUJ Instability: Assessed via the DRUJ ballottement test in neutral, full pronation, and full supination. Increased translation compared to the contralateral wrist indicates disruption of the deep radioulnar ligaments (foveal attachment).
* Extensor Carpi Ulnaris (ECU) Pathology: Evaluate for ECU tendon subluxation or tendinopathy, which frequently co-occurs with traumatic TFCC injuries. ECU subluxation is a strong preoperative indicator of significant ulnar-sided structural disruption.
Imaging
Standard posteroanterior (PA) and lateral radiographs are required to assess ulnar variance, DRUJ congruity, and the presence of ulnar styloid fractures. Magnetic Resonance Imaging (MRI) or MR arthrography provides high-resolution visualization of the TFCC, intrinsic interosseous ligaments, and chondral surfaces.
💡 Clinical Pearl: Ulnar Variance
Ulnar variance plays a critical role in surgical decision-making. In wrists with positive ulnar variance, isolated TFCC repair may fail due to excessive shear stress between the ulnar head and the repaired TFCC. In such cases, a concurrent ulnar shortening osteotomy is strongly recommended to decompress the ulnocarpal joint and protect the repair.
Patient Positioning and Setup
- Anesthesia: The procedure is typically performed under regional anesthesia (supraclavicular or axillary block) or general anesthesia, depending on patient preference and the anticipated duration of the surgery.
- Tourniquet: A pneumatic tourniquet is applied to the proximal arm and inflated as needed. Tourniquet use is especially critical when shaving or burring bone and soft tissue to maintain a clear visual field.
- Positioning: The patient is positioned supine. The operative arm is placed on a hand table.
- Traction: A wrist traction tower is utilized. Finger traps are applied to the index and middle fingers, and 10 to 15 pounds of longitudinal traction is applied to distract the radiocarpal and midcarpal joints. Countertraction is achieved via a padded strap across the distal humerus.
Arthroscopic Débridement of Central TFCC Tears (Class 1A)
Central tears of the TFCC articular disc are typically unstable flap tears that cause mechanical symptoms. Because this region is avascular, repair is not viable; therefore, meticulous débridement is the treatment of choice.
Step 1: Portal Placement and Diagnostic Arthroscopy
- 3-4 Portal: Establish the 3-4 portal (between the 3rd and 4th extensor compartments) as the primary viewing portal. Perform a systematic diagnostic sweep of the radiocarpal and ulnocarpal joints.
- 6R and 6U Portals: Establish the 6R portal (radial to the ECU tendon) and 6U portal (ulnar to the ECU tendon) for further ulnocarpal examination and instrumentation.
- Midcarpal Examination: Establish the midcarpal portals (radial midcarpal and ulnar midcarpal) to evaluate the scapholunate and lunotriquetral intervals, ruling out concurrent intrinsic ligament pathology.
⚠️ Surgical Warning: Portal Anatomy
When establishing the 6U portal, extreme caution must be exercised to avoid injury to the dorsal sensory branch of the ulnar nerve (DSBUN). Always use blunt dissection with a hemostat down to the capsule after making the skin incision.
Step 2: Establishing Working Portals
After completing the midcarpal examination, return the arthroscope to the 3-4 portal. Insert an 18-gauge spinal needle under direct visualization to determine the optimal trajectory for the working portals (typically 6R or 4-5). This "outside-in" needle localization prevents iatrogenic damage to the articular cartilage during instrument insertion.
Step 3: Synovectomy and Probing
- Introduce a 2.0-mm to 3.0-mm full-radius suction shaver through the 6R portal.
- Débride hypertrophic synovium as needed to obtain an unobstructed view of the ulnocarpal joint and the TFCC.
- Insert an arthroscopic probe. Systematically assess the central portion of the TFCC, the ulnar lunotriquetral ligament, and the dorsal and palmar radioulnar ligaments. Assess the tension and integrity of the TFCC by applying a "trampoline test." A loss of the normal trampoline effect suggests a peripheral detachment.
Step 4: Débridement of the Flap Tear
- Utilize the full-radius shaver, arthroscopic suction punches (biters), or small retrograde blades to excise the unstable flap portion of the central tear.
- Crucial Step: Trim the margins of the tear carefully to a stable, smooth contour. You must leave the peripheral 2 mm of the TFCC rim intact. This peripheral rim contains the critical radioulnar ligaments that maintain DRUJ stability. Over-resection will lead to iatrogenic DRUJ instability.
Step 5: Closure
- Thoroughly irrigate the joint to remove all cartilaginous debris.
- Remove instruments and release traction.
- Close the portal sites using 4-0 or 5-0 nylon sutures.
Management of Foveal Detachments (Class 1B Lesions)
Class 1B lesions represent traumatic detachments of the TFCC from its ulnar insertion, with or without an associated ulnar styloid fracture.
Biomechanics of the Ulnar Attachment
The TFCC has two distinct ulnar attachments: the superficial fibers attach to the tip of the ulnar styloid, while the deeper, biomechanically critical fibers (the ligamentum subcruentum) attach to the fovea at the base of the ulnar styloid.
* Styloid Tip Fractures: Fractures at the tip of the styloid often leave the deep foveal fibers intact, resulting in a stable DRUJ.
* Styloid Base Fractures: Fractures through the base of the ulnar styloid indicate a significant detachment of the deep radioulnar ligaments, leading to profound DRUJ instability.
Surgical Strategy for Class 1B Lesions
If the ulnar styloid is fractured at the base, open reduction and internal fixation (ORIF) of the fracture, or excision of a small comminuted fragment with concurrent open repair of the TFCC, is the standard treatment.
Significant injury to the ECU sheath frequently accompanies traumatic TFCC injuries. If ECU tendon subluxation is identified preoperatively or intraoperatively, the surgeon must be prepared to perform an arthroscopic repair of the TFCC combined with an open ECU sheath reconstruction.
Arthroscopic Transosseous Repair of Foveal Detachments (Nakamura Technique)
For complete or partial ulnar disruptions of the TFCC at the fovea without a large styloid fracture, arthroscopic repair is highly effective. Nakamura et al. described a robust arthroscopic technique utilizing transosseous sutures to reattach the deep fibers to the fovea.
Indications and Ulnar Variance Considerations
This technique is specifically recommended for wrists with ulnar neutral or ulnar minus variance.
In wrists with a positive ulnar variance, the inherent shear stress between the prominent ulnar head and the suture site of the repaired TFCC is highly likely to rupture the sutures or cause repair failure. In such cases, an ulnar shortening osteotomy must be performed concurrently.
Anatomical Basis of the Transosseous Tunnel
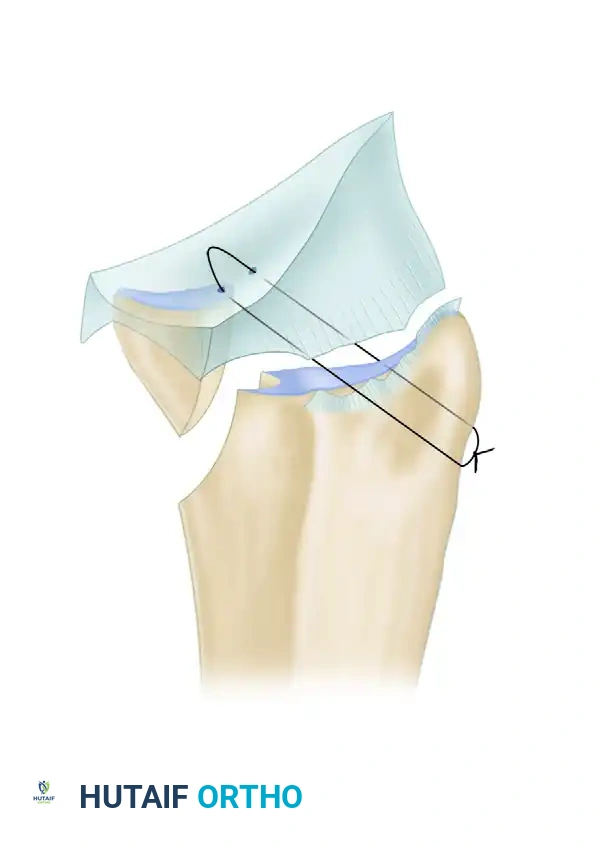
The concept of this repair relies on precise anatomical targeting. A linear trajectory drawn from a point on the ulnar cortex (15 mm proximal to the tip of the ulnar styloid) through the ulnar half of the triangular fibrocartilage will pass directly through the anatomical foveal insertion. Sutures placed along this vector can securely reattach the TFCC to the fovea using an outside-in pull-out technique.
Figure 69-58: Arthroscopic repair of foveal detachment of the triangular fibrocartilage complex (TFCC). The transosseous suture trajectory passes from the ulnar cortex, through the fovea, capturing the articular disc.
Step-by-Step Transosseous Repair
- Preparation of the Fovea: Viewing from the 3-4 portal, introduce a shaver or burr through the 6R or 6U portal. Decorticate the foveal footprint down to bleeding cancellous bone to promote a robust healing response.
- Guide Pin Placement: Make a small longitudinal incision over the ulnar aspect of the distal forearm, approximately 15 mm proximal to the ulnar styloid tip. Protect the DSBUN.
- Drilling the Tunnel: Using a specialized TFCC drill guide, advance a Kirschner wire from the ulnar cortex (15 mm proximal to the styloid) into the fovea. Overdrill the K-wire with a 2.0-mm cannulated drill bit to create the transosseous tunnel.
- Suture Passing: Utilize an outside-in suture passing device (e.g., a spinal needle or specialized suture lasso). Pass a non-absorbable 2-0 or 0 suture through the ulnar capsule, capturing the substantial peripheral rim of the detached TFCC, and retrieve it through the transosseous tunnel.
- Securing the Repair: Pass at least two suture limbs to create a horizontal mattress configuration across the TFCC. Retrieve the suture ends out of the ulnar cortical tunnel.
- Tensioning: While holding the forearm in neutral rotation to ensure appropriate tensioning of the radioulnar ligaments, tie the sutures securely over the ulnar cortical bone bridge or over a small cortical button.
- Verification: Re-evaluate the DRUJ stability arthroscopically and clinically. The "trampoline effect" should be restored, and DRUJ translation should be symmetric to the contralateral side.
Postoperative Care and Rehabilitation
The postoperative protocol must balance the protection of the healing tissues with the prevention of arthrofibrosis. The protocol varies slightly depending on whether a simple débridement or a structural repair was performed.
Following Arthroscopic Débridement (Class 1A)
- Immobilization: Apply a volar short-arm splint immediately postoperatively.
- Suture Removal: Portal sutures are removed at 10 to 14 days.
- Early Motion: Protected range-of-motion (ROM) exercises are initiated immediately after suture removal.
- Splinting Duration: Splint wear is continued for up to 4 weeks, titrated based on patient symptoms and comfort.
- Activity Modification: Strenuous pronation-supination and heavy grasping activities must be strictly avoided during the first 4 weeks.
- Rehabilitation: Therapist-supervised rehabilitation is added as needed to restore grip strength and terminal rotation.
Following Foveal Repair (Class 1B)
- Phase 1 (0-4 Weeks): The wrist and forearm are immobilized in a Muenster-style or long-arm cast/splint in neutral rotation to completely eliminate pronation and supination, protecting the foveal repair.
- Phase 2 (4-8 Weeks): Transition to a short-arm splint. Initiate active-assisted range of motion (AAROM) for flexion and extension. Gentle, gravity-eliminated pronation and supination may begin, but loaded rotation is strictly prohibited.
- Phase 3 (8-12 Weeks): Discontinue the splint. Begin progressive strengthening, focusing on the ECU and dynamic wrist stabilizers.
- Return to Play/Work: Unrestricted heavy labor or return to contact sports is typically delayed until 4 to 6 months postoperatively, contingent upon the restoration of symmetric DRUJ stability and pain-free grip strength.
Complications and Pitfalls
- Nerve Injury: The dorsal sensory branch of the ulnar nerve is highly vulnerable during the establishment of the 6U portal and during the ulnar approach for transosseous drilling. Meticulous blunt dissection is mandatory.
- Iatrogenic Instability: Over-resection of the central TFCC (failing to leave the 2-mm peripheral rim) during débridement will compromise the radioulnar ligaments, leading to catastrophic DRUJ instability.
- Repair Failure: Performing an isolated foveal repair in a patient with positive ulnar variance without addressing the bony anatomy (via ulnar shortening) will almost certainly result in suture cut-out and recurrent tearing due to ulnocarpal abutment.
- Stiffness: Prolonged immobilization beyond the recommended timeframes, particularly in supination or pronation, can lead to severe rotational stiffness. Adherence to a phased, therapist-guided rehabilitation protocol is essential.
You Might Also Like