Hallux Rigidus: Pathogenesis, Evaluation, and Surgical Management
Key Takeaway
Hallux rigidus is a progressive degenerative arthropathy of the first metatarsophalangeal joint, characterized by restricted dorsiflexion and dorsal osteophyte formation. This comprehensive guide details the underlying biomechanics, clinical evaluation, and evidence-based surgical interventions. From joint-sparing cheilectomy for early-stage disease to first MTP arthrodesis for end-stage arthritis, mastering these techniques ensures optimal restoration of foot biomechanics and durable pain relief for patients.
Introduction and Historical Context
Hallux rigidus is a progressive, debilitating arthropathy of the first metatarsophalangeal (MTP) joint characterized by a marked limitation of motion, particularly dorsiflexion, accompanied by periarticular osteophyte formation and pain. The term hallux rigidus was originally coined by Cotterill in 1888 to describe this specific limitation of motion at the great toe. However, the earliest surgical intervention for this disorder was reported a year prior, in 1887, by Davies-Colley. He performed the first resection of the base of the proximal phalanx for this condition, which he termed hallux flexus due to the characteristic flexion posture of the MTP joint when the foot is plantigrade, alongside its severely limited extension.
Although our understanding of the condition has advanced significantly through modern radiographic and histological techniques, the exact pathogenesis of hallux rigidus remains a subject of academic debate. What is universally appreciated, however, is its unrelenting, destructive clinical course. The cascade of joint degradation is believed to initiate with localized articular cartilage damage, which precipitates a reactive synovitis. This inflammatory environment leads to further cartilage destruction, robust osteophyte proliferation (particularly dorsally), and eventual subchondral bone destruction.
Pathoanatomy and Biomechanics
The first MTP joint is a complex articulation essential for normal gait. During the terminal stance phase of the gait cycle, the first MTP joint must dorsiflex between 65 and 75 degrees to engage the windlass mechanism, which stabilizes the medial longitudinal arch and allows for an efficient push-off. In hallux rigidus, this biomechanical requirement is severely compromised.
The McMaster Cleavage Lesion
Histological and operative observations have provided critical insights into the early stages of hallux rigidus. McMaster reported that the most common microscopic finding in early-stage hallux rigidus is a distinct cleavage lesion in the articular cartilage of the first metatarsal head, occurring without any detached subchondral bone.

Radiographically, the earliest sign of this lesion is a subtle, easily overlooked depression in the dome of the metatarsal head. Anatomically, this cleavage lesion is consistently located between the apex of the metatarsal dome and the dorsal margin of the articular surface.
McMaster postulated a biomechanical etiology for the characteristic clinical presentation:
* Pain Mechanism: When the hallux is extended during gait, the proximal phalanx abuts directly against this cleavage lesion.
* Instinctive Flexion: This abutment produces sharp pain, leading to an instinctive, protective flexion of the joint, thereby actively limiting extension.
* Mechanical Block: As the disease progresses, a prominent osteophyte forms at the dorsal articular margin of the metatarsal head, transitioning the limitation of motion from a pain-mediated response to a rigid mechanical abutment.
Clinical Pearl: The classic site of the cleavage lesion explains why patients present with exquisite tenderness specifically over the dorsum of the first MTP joint and why dorsiflexion is the earliest and most severely restricted plane of motion.
Etiology and Demographics
The etiology of hallux rigidus is multifactorial and varies significantly between adolescent and adult populations.
Adolescent Hallux Rigidus
In adolescents, the process typically begins following a single traumatic event at the MTP joint that damages the dorsal articular surface of the metatarsal head. Alternatively, repeated microtrauma can lead to cumulative articular cartilage damage. Other suggested etiologies in the younger population include:
* Osteochondritis dissecans of the first metatarsal head.
* Osteochondral fractures over the dorsal convexity of the joint surface.
* Hyperextension injuries of the first metatarsal ("turf toe" variants).
* An abnormally long first metatarsal.
* Severe pronation of the foot.
Adult Hallux Rigidus
Adult-onset hallux rigidus is most frequently the result of primary degenerative osteoarthritis of the first MTP joint.
The Role of Metatarsus Primus Elevatus:
Metatarsus primus elevatus—defined as the dorsal positioning of the first metatarsal relative to the lesser metatarsals on a weight-bearing lateral radiograph—has historically been suggested as a primary causative factor. However, rigorous biomechanical and radiographic studies have failed to clearly prove this association. Currently, the elevation of the first metatarsal is considered to be secondary to the arthritic changes within the first MTP joint, rather than the primary causal factor.
Established Associations:
While no definitive association has been identified between hallux rigidus and first ray hypermobility, Achilles/gastrocnemius tightness, abnormal foot posture, symptomatic hallux valgus, shoe wear, or occupation, it is statistically associated with:
* Hallux valgus interphalangeus.
* Bilateral involvement (strongly correlated with a familial history).
* Unilateral involvement (strongly correlated with a history of trauma).
* Female gender.
Clinical Evaluation
Patients typically present with an insidious onset of pain, stiffness, and swelling at the first MTP joint. The pain is exacerbated by activities requiring maximum dorsiflexion, such as running, walking up inclines, or wearing high-heeled shoes.
Physical Examination
- Inspection: A palpable and often visible dorsal prominence (osteophyte) is noted over the first MTP joint. The hallux may rest in a slightly flexed position.
- Palpation: Tenderness is localized to the dorsal aspect of the joint, corresponding to the underlying osteophyte and capsular distension.
- Range of Motion (ROM): Dorsiflexion is markedly restricted and painful. Plantarflexion is usually preserved until the end stages of the disease.
- Grind Test: Axial compression combined with circumduction of the proximal phalanx on the metatarsal head will elicit crepitus and pain, indicating global joint space narrowing.

Radiographic Evaluation and Grading
Standard weight-bearing radiographs (anteroposterior, lateral, and sesamoid views) are mandatory. Early radiographic findings may be limited to the subtle dorsal depression described by McMaster. As the disease progresses, classic osteoarthritic changes appear: joint space narrowing, subchondral sclerosis, cystic changes, and prominent dorsal, lateral, and medial osteophytes.
Grading System for Hallux Rigidus
A standardized grading system (such as the Coughlin and Shurnas classification) utilizes passive ROM, clinical symptoms, and radiographic findings to assign a grade from 0 to 4. This system is highly reliable in predicting the outcome of operative treatment:
- Grade 0: Normal radiographs; stiffness and pain only at extreme dorsiflexion.
- Grade 1: Mild dorsal osteophyte; preserved joint space; pain at extremes of motion.
- Grade 2: Moderate dorsal osteophyte; joint space narrowing (dorsal > plantar); pain throughout the ROM.
- Grade 3: Severe osteophytes; global joint space loss; constant pain, including at rest.
- Grade 4: Same radiographic findings as Grade 3, but with severe pain throughout the entire ROM, including mid-arc motion.
Non-Operative Management
Conservative management should be exhausted before considering surgical intervention, particularly in Grade 0 to 2 disease.
* Shoe Modifications: A stiff-soled shoe with a rocker-bottom modification reduces the need for first MTP dorsiflexion during the terminal stance phase of gait. A wide toe box accommodates the dorsal osteophyte.
* Orthotics: A rigid Morton's extension orthotic can splint the first MTP joint, reducing painful motion.
* Pharmacotherapy: Nonsteroidal anti-inflammatory drugs (NSAIDs) help manage synovitis.
* Injections: Intra-articular corticosteroid injections can provide temporary relief of acute inflammatory flares, though they do not alter the disease's natural history.
Surgical Management
When conservative measures fail, operative intervention is dictated by the clinical and radiographic grade of the disease. The primary goals are pain relief, restoration of functional ambulation, and correction of deformity.
1. Cheilectomy (Joint-Sparing)
Cheilectomy is the procedure of choice for Grade 1 and Grade 2 hallux rigidus, and select cases of Grade 3 where mid-arc motion is pain-free. The procedure involves the resection of the dorsal osteophyte and the dorsal 30% of the metatarsal head to remove the mechanical block to dorsiflexion.
Surgical Technique:
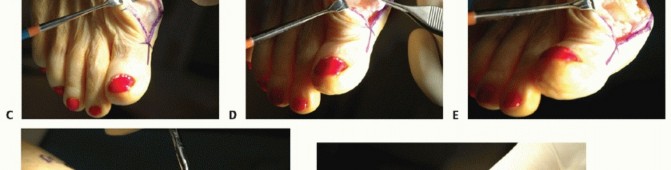
1. Positioning and Approach: The patient is placed supine. A dorsal longitudinal incision is made centered over the first MTP joint, medial to the extensor hallucis longus (EHL) tendon.
2. Neuroma Prevention: The dorsal medial cutaneous nerve branches must be meticulously identified and retracted to prevent painful postoperative neuromas.
3. Capsulotomy: A longitudinal capsulotomy is performed. The capsule and periosteum are elevated sharply from the dorsal metatarsal head and the base of the proximal phalanx.

- Osteophyte Resection: The prominent dorsal osteophyte is identified. Using an oscillating saw or sharp osteotome, the dorsal 30% of the metatarsal head is resected flush with the dorsal cortex of the metatarsal shaft.
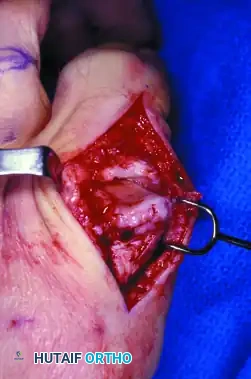
- Debridement: The joint is inspected for loose bodies. The cleavage lesion, if present, is debrided. Marginal osteophytes on the medial and lateral aspects of the metatarsal head and proximal phalanx are excised.
- Intraoperative Assessment: The hallux is dorsiflexed. A minimum of 70 degrees of passive dorsiflexion should be achieved without impingement. If dorsiflexion remains limited by soft tissue tension, a release of the plantar plate or a Moberg (dorsal closing wedge) osteotomy of the proximal phalanx may be considered.
- Closure: The capsule is closed loosely to prevent restricting postoperative motion, followed by standard skin closure.
Surgical Warning: Over-resection of the metatarsal head (greater than 30-40%) can compromise the articular surface necessary for weight-bearing and destabilize the MTP joint, leading to subluxation.
2. First MTP Joint Arthrodesis (Joint-Sacrificing)
Arthrodesis remains the gold standard for Grade 3 and Grade 4 hallux rigidus, as well as for failed cheilectomies. It provides predictable, durable pain relief and restores the weight-bearing capacity of the first ray.
Surgical Technique:
1. Approach: A dorsal or medial approach may be utilized. The joint is exposed, and all remaining articular cartilage and subchondral sclerotic bone are aggressively debrided down to bleeding cancellous bone.
2. Joint Preparation: Cup-and-cone reamers are highly recommended as they allow for multi-planar adjustment of the toe position while maximizing cancellous bone contact.
3. Positioning (CRITICAL STEP): The success of an arthrodesis relies entirely on the position of the fusion.
* Valgus: 10 to 15 degrees of valgus (parallel to the lesser toes).
* Dorsiflexion: 10 to 15 degrees of dorsiflexion relative to the floor (or 15-20 degrees relative to the first metatarsal axis). This allows the toe to clear the ground during swing phase and accommodate a standard shoe heel.
* Rotation: Neutral rotation; the toenail should face directly dorsal.
4. Fixation: Rigid internal fixation is achieved using a low-profile dorsal titanium plate combined with an interfragmentary lag screw, or crossed compression screws.
5. Closure: Standard layered closure.
Postoperative Protocol
Following Cheilectomy:
* Patients are placed in a rigid postoperative shoe and allowed immediate heel-touch or flat-foot weight-bearing.
* Active and passive ROM exercises are initiated within 3 to 5 days postoperatively to prevent capsular adhesions.
* Transition to normal footwear occurs at 3 to 4 weeks as swelling subsides.
Following Arthrodesis:
* Patients are placed in a rigid postoperative shoe or boot.
* Weight-bearing is restricted to the heel or lateral border of the foot for the first 2 to 4 weeks.
* Progressive weight-bearing is allowed as radiographic evidence of consolidation appears (typically 6 to 8 weeks).
* High-impact activities are restricted until complete radiographic union is confirmed (usually 10 to 12 weeks).
Complications and Pitfalls
While surgical outcomes for hallux rigidus are generally excellent, specific complications must be anticipated and managed.
- Recurrence of Symptoms (Cheilectomy): Progression of the underlying degenerative joint disease is the most common cause of failure following a cheilectomy, eventually necessitating conversion to an arthrodesis.
- Nonunion (Arthrodesis): Symptomatic nonunion occurs in approximately 5-10% of cases, often related to inadequate joint preparation, poor fixation, or patient non-compliance (e.g., smoking).
- Malunion (Arthrodesis): Fusing the toe in excessive plantarflexion leads to severe pain at the tip of the toe and interphalangeal joint arthritis. Excessive dorsiflexion causes transfer metatarsalgia to the lesser metatarsal heads.
- Hallux Extensus and Recurrent Valgus: Iatrogenic soft tissue imbalance or over-resection can lead to destabilization of the joint.

Pitfall: Failure to address concomitant lesser toe deformities or unrecognized midfoot arthritis can lead to persistent postoperative pain despite a technically successful first MTP intervention. Comprehensive preoperative biomechanical assessment is mandatory.
You Might Also Like