Hallux Rigidus: Comprehensive Nonoperative and Operative Management
Key Takeaway
Hallux rigidus is a progressive osteoarthritic condition of the first metatarsophalangeal (MTP) joint characterized by pain and restricted dorsiflexion. Management begins with nonoperative modalities, including rigid Morton's extensions and intra-articular injections. When conservative measures fail, operative interventions are dictated by disease severity. Cheilectomy is preferred for early-stage disease (Grades 1-2), while first MTP arthrodesis remains the gold standard for advanced degeneration (Grades 3-4), providing reliable pain relief and restoration of propulsive gait mechanics.
INTRODUCTION AND PATHOMECHANICS
Hallux rigidus is a progressive, degenerative osteoarthritic condition affecting the first metatarsophalangeal (MTP) joint, characterized by debilitating pain, osteophyte formation, and a profound restriction of sagittal plane motion—specifically dorsiflexion. The pathomechanics of hallux rigidus are deeply tied to the disruption of the windlass mechanism. During the terminal stance phase of gait, the first MTP joint must dorsiflex to allow the body's center of mass to advance over the foot. In hallux rigidus, dorsal impingement and joint space narrowing prevent this essential kinematic function, leading to compensatory gait abnormalities, lateral column overload, and transfer metatarsalgia.
The pathogenesis often involves repetitive microtrauma. Forceful extension and impaction of the metatarsal head against the proximal phalanx produce localized chondral or osteochondral lesions, typically initiating at the dorsal aspect of the metatarsal head. Over time, this mechanical impingement stimulates the formation of a dorsal osteophyte (cheilon), which further blocks dorsiflexion and exacerbates cartilage degradation.
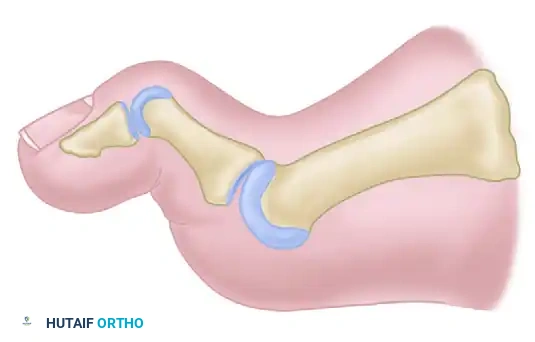
Location of chondral or osteochondral lesion produced by forceful extension and impaction of the metatarsal head. (Redrawn from McMaster MJ: The pathogenesis of hallux rigidus, J Bone Joint Surg 60B:82, 1978.)
CLINICAL EVALUATION AND GRADING
A rigorous clinical and radiographic evaluation is paramount for dictating the treatment algorithm. Patients typically present with a palpable dorsal exostosis, pain exacerbated by toe-off during gait, and a stiff first ray. Radiographic evaluation must include weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. The oblique view is particularly critical, as it frequently demonstrates remaining joint space that is obscured or not visible on standard AP and lateral projections.
The Coughlin and Shurnas Grading System is the universally accepted standard for classifying the severity of hallux rigidus, correlating radiographic findings with clinical symptoms and joint mobility:
- Grade 0:
- Radiograph: Normal.
- Pain: None.
- Motion: Stiffness or slight loss of MTP joint motion.
- Grade 1:
- Radiograph: Minor narrowing of the MTP joint space; minimal osteophyte formation.
- Pain: Intermittent.
- Motion: Mild restriction.
- Grade 2:
- Radiograph: Moderate joint space narrowing; distinct dorsal, lateral, and/or medial osteophyte formation.
- Pain: More constant.
- Motion: Moderate restriction.
- Grade 3:
- Radiograph: Severe joint space narrowing; extensive osteophyte formation; subchondral sclerosis and cysts.
- Pain: Constant, but notably no pain at the midrange of MTP joint motion.
- Motion: Moderately severe restriction (less than 20 degrees of total motion).
- Grade 4:
- Radiograph: Same as Grade 3 (severe narrowing, extensive osteophytes).
- Pain: Constant, including pain at the midrange of passive MTP joint motion.
- Motion: Same as Grade 3 (less than 20 degrees of total motion).
Clinical Pearl: The critical distinction between Grade 3 and Grade 4 hallux rigidus is clinical, not radiographic. Grade 4 is defined by pain throughout the entire arc of motion (midrange pain), indicating global articular degeneration. This distinction is vital, as midrange pain is an absolute contraindication for joint-sparing procedures like cheilectomy.
NONOPERATIVE TREATMENT
In most patients, operative correction is ultimately required to relieve pain and improve function; however, conservative management should always be the first line of defense. Yee and Lau, in a comprehensive review of the literature on hallux rigidus, determined that robust evidence supports the use of nonoperative measures before surgical intervention is considered.
Orthoses and Shoe Modifications
The primary biomechanical goal of nonoperative treatment is to limit the demand for dorsiflexion at the first MTP joint during the propulsive phase of gait.
* Shoe Modifications: A stiff-soled shoe with a rigid rocker bottom is highly effective. The rocker bottom artificially simulates the toe-off phase, allowing the foot to roll forward without requiring the first MTP joint to dorsiflex. A wide toe box is also necessary to accommodate the dorsal osteophyte and prevent direct friction.
* Foot Orthoses: A rigid carbon-fiber insert or a custom orthotic with a Morton's extension (a rigid extension under the first MTP joint and hallux) splints the joint, reducing painful motion.
Pharmacologic and Injectable Therapies
- NSAIDs: Oral nonsteroidal anti-inflammatory drugs provide symptomatic relief of synovitis.
- Intra-articular Injections: Image-guided (ultrasound or fluoroscopic) intra-articular injections of corticosteroids can provide profound, albeit temporary, relief of acute inflammatory flares. Additionally, injections of sodium hyaluronate (viscosupplementation) have shown efficacy in reducing pain and improving function in early-to-moderate stages of the disease, delaying the need for surgical intervention.
OPERATIVE TREATMENT: PRINCIPLES AND DECISION MAKING
When nonoperative measures fail, surgical intervention is indicated. Although numerous operations have been recommended—including dorsal wedge osteotomies at the base of the proximal phalanx (Moberg) or distal first metatarsal, the Keller resection arthroplasty, and various implant arthroplasties—no single joint-sparing procedure has proven universally superior.
The surgical algorithm is heavily dependent on the Coughlin and Shurnas grade:
* Grades 1 and 2: Joint-sparing procedures, primarily Cheilectomy.
* Grades 3 and 4: Joint-sacrificing procedures, primarily First MTP Arthrodesis (the gold standard).
Cheilectomy
The rationale for cheilectomy is the relief of painful mechanical impingement of the proximal phalanx against the dorsal osteophyte of the first metatarsal head. By removing this bony block, the procedure decompresses the joint and restores the arc of dorsiflexion.
Indications and Outcomes:
Cheilectomy is indicated for Grade 1 and Grade 2 hallux rigidus, and select Grade 3 cases where midrange motion is completely pain-free and more than half of the metatarsal head cartilage remains viable. Reported success rates range broadly from 56% to 92%. Outcomes are significantly better in less severe grades of involvement and in patients older than 60 years.
Surgical Warning: Gait analysis has demonstrated that increased lateral metatarsal-head loading may occur after cheilectomy. These alterations in foot kinematics can result in transfer metatarsalgia and may precipitate further degenerative joint changes over time.
Surgical Technique:
1. Approach: A dorsal longitudinal incision is made centered over the first MTP joint, lateral to the extensor hallucis longus (EHL) tendon.
2. Exposure: The EHL is retracted medially or laterally, and a dorsal capsulotomy is performed. The collateral ligaments are partially released to allow plantarflexion of the hallux, fully exposing the metatarsal head.
3. Resection: The dorsal osteophyte and any medial/lateral bony excrescences are excised using an oscillating saw or osteotome.
4. Cartilage Excision: It is critical to resect as much of the dorsal lip of the articular cartilage and underlying bone as necessary to allow at least 70 degrees of passive intraoperative dorsiflexion. Typically, this requires removing the dorsal 20% to 30% of the metatarsal head.
5. Closure and Postoperative Care: The capsule is meticulously repaired. Patients are placed in a rigid postoperative shoe and encouraged to begin immediate active and passive range-of-motion exercises to prevent capsular scarring.
First MTP Joint Arthrodesis (The Gold Standard)
Arthrodesis of the first MTP joint remains the most reliable, durable, and definitive procedure for advanced hallux rigidus. Suggested indications include loss of joint space evident on AP, lateral, or oblique views, and Grade 3 or Grade 4 hallux rigidus.
Biomechanics and Outcomes:
Modern fixation techniques utilizing interfragmentary compression screws, dorsal contoured plates, or a combination of both have produced exceptionally high rates of fusion (94% to 98%) and excellent patient satisfaction. Postoperative gait studies have shown significant improvements in propulsive power, weight-bearing function of the medial column, and overall stability during gait after arthrodesis.
Surgical Technique (McKeever Arthrodesis):
1. Approach: A dorsal longitudinal incision is utilized. The joint is exposed, and the remaining cartilage and subchondral bone are meticulously denuded.
2. Joint Preparation: The articular surfaces can be prepared using flat cuts or cup-and-cone reamers. Cup-and-cone reaming is highly favored as it preserves bone stock, allows for infinite adjustments in positioning prior to fixation, and maximizes the cancellous bone contact area.
3. Positioning: Optimal positioning is the most critical step of the procedure. The hallux must be positioned in:
* 10 to 15 degrees of valgus (to rest parallel to the second toe and allow shoe wear).
* 15 degrees of dorsiflexion relative to the floor (or approximately 25 to 30 degrees of dorsiflexion relative to the longitudinal axis of the first metatarsal).
* Neutral rotation (ensuring the toenail faces directly dorsal).
4. Fixation: Once provisional fixation with Kirschner wires is achieved and the position is verified clinically (using a flat plate against the foot) and fluoroscopically, definitive fixation is applied. A classic McKeever arthrodesis utilizes crossed interfragmentary compression screws.
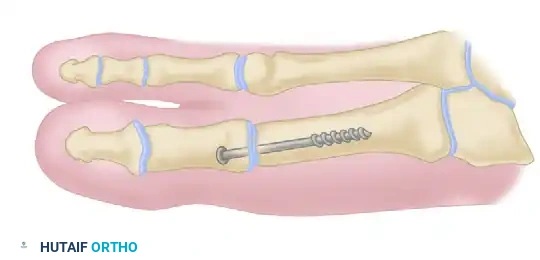
McKeever arthrodesis. A, Anteroposterior view demonstrating a 4.0-millimeter cancellous screw utilized for interfragmentary internal fixation.
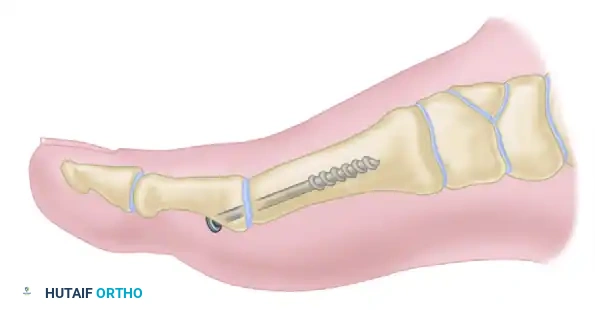
McKeever arthrodesis. B, Lateral diagrammatic view of the interfragmentary screw compressing the prepared MTP joint surfaces.

McKeever arthrodesis. C, Completed arthrodesis demonstrated on a lateral postoperative radiograph.
Pitfall: Fusing the joint in excessive plantarflexion will result in severe interphalangeal joint arthritis and a painful dorsal impingement against the shoe toe box. Conversely, excessive dorsiflexion leads to transfer metatarsalgia and loss of hallux purchase during gait.
Alternative and Salvage Procedures
While arthrodesis is the gold standard for advanced disease, several alternative arthroplasty techniques exist, primarily reserved for older, lower-demand patients or those who absolutely refuse a fusion.
Keller Resection Arthroplasty and Interposition
The Keller procedure involves the resection of the base of the proximal phalanx to decompress the joint. To mitigate the complications of a standard Keller (such as a "cock-up" deformity, loss of push-off power, and transfer metatarsalgia), modifications have been developed.
* Soft Tissue Interposition: The extensor hallucis brevis (EHB) tendon and local capsular tissue can be mobilized and sutured into the joint space as interposition materials.
* Oblique Resection: Interposition arthroplasty has also been modified by making an oblique proximal phalangeal resection that exits at the subchondral bone of the plantar aspect of the proximal phalanx. This specific geometry is an attempt to preserve the critical attachment of the flexor hallucis brevis (FHB) on the plantar base of the proximal phalanx, thereby maintaining intrinsic stability and plantarflexion power.
Despite these modifications, reported results for resection and interposition arthroplasties vary widely, and they are generally considered inferior to arthrodesis in active patients.
Implant Arthroplasty
- Silicone Elastomer Implants: Silicone-rubber, single-stem or double-stem replacement arthroplasty components have been utilized historically to maintain motion and joint space. While some studies report satisfactory short-term results, the overwhelming concern with this technique is the high incidence of silicone-rubber synovitis, particulate wear debris, and subsequent massive osteolysis. Their use is largely discouraged in modern orthopedic practice.
- Metallic Hemiarthroplasty: Hemiarthroplasty of the proximal phalanx base or the metatarsal head with a metallic resurfacing component has been described as a motion-preserving alternative. High short-term success rates have been reported; for instance, one study of 23 hemiarthroplasties reported that 91% of patients were satisfied with their outcomes at a 5.7-year follow-up, with all patients making significant gains in American Orthopaedic Foot and Ankle Society (AOFAS) scores. However, large, randomized controlled studies with long-term follow-up (greater than 10 years) remain unavailable. Concerns regarding implant subsidence, loosening, and progressive wear of the opposing native cartilage limit its widespread adoption over arthrodesis.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Postoperative management is dictated by the procedure performed:
* Following Cheilectomy: Early mobilization is imperative. Patients are allowed to weight-bear as tolerated in a stiff-soled surgical shoe immediately. Aggressive active and passive dorsiflexion exercises begin at 3 to 5 days postoperatively to prevent intra-articular adhesions.
* Following Arthrodesis: Patients are typically placed in a rigid postoperative shoe, walking boot, or short-leg cast. Heel-touch weight-bearing or flat-foot weight-bearing in a rigid sole is permitted, but propulsive toe-off is strictly prohibited until radiographic evidence of bridging trabecular bone is observed, usually between 6 to 8 weeks. Transition to standard footwear is allowed once clinical and radiographic union is confirmed.
📚 Medical References
- hallux rigidus, and metatarsus primus varus, J Bone Joint Surg 34A:129, 1952.
- Miller GM, Hsu JD, Hoffer MM, et al: Posterior tibial tendon transfer: a review of the literature and analysis of 74 procedures, J Pediatr Orthop 2:363, 1982.
- Moreau MJ, Lake DM: Outpatient percutaneous heel cord lengthening in children, J Pediatr Orthop 7:253, 1987.
- Mosca VS: Calcaneal lengthening for valgus deformity of the hindfoot, J Bone Joint Surg 77A:500, 1995.
- Narayanan UG: The role of gait analysis in the orthopaedic management of ambulatory cerebral palsy, Curr Opin Pediatr 19:38, 2007.
- Noritake K, Yoshihashi Y, Miyata T: Calcaneal lengthening for planovalgus foot deformity in children with spastic cerebral palsy, J Pediatr Orthop B 14:274, 2005.
- O’Connell PA, D’Souza L, Dudeney S, Stephens M: Foot deformities in children with cerebral palsy, J Pediatr Orthop 18:743, 1998.
- Ono K, Hiroshima K, Tada K, et al: Anterior transfer of the toe fl exors for equinovarus deformity of the foot, Int Orthop 4:255, 1980.
- Perry J, Hoffer MM, Giovani P, et al: Gait analysis of the triceps surae in cerebral palsy: a preoperative and postoperative clinical and electromyographic study, J Bone Joint Surg 56A:511, 1974.
- Phillips JE, Hooper G: A simple technique for arthrodesis of the fi rst metatarsophalangeal joint, J Bone Joint Surg 68B:774, 1986.
- Pierrot AH, Murphy OB: Albert E. Klinkicht Award, 1972.
- Heel cord advancement: a new approach to the spastic equinus deformity, Orthop Clin North Am 5:117, 1974.
- Rattey TE, Leahey L, Hyndman J, et al: Recurrence after Achilles tendon lengthening in cerebral palsy, J Pediatr Orthop 13:184, 1993.
- Rathgen KE, Mubarak SJ: Calcaneal-cuboid-cuneiform osteotomy for the correction of valgus foot deformities in children, J Pediatr Orthop 18:775, 1998.
- Reimers J: Functional changes in the antagonists after lengthening the agonists in cerebral palsy, I: triceps surae lengthening, Clin Orthop Relat Res 253:30, 1990.
- Root L: Varus and valgus foot in cerebral palsy and its management, Foot Ankle 4:174, 1984.
- Root L, Miller SR, Kirz P: Posterior tibial-tendon transfer in patients with cerebral palsy, J Bone Joint Surg 69A:1133, 1987.
- Rose SA, DeLuca PA, Davis RB III, et al: Kinematic and kinetic evaluation of the ankle after lengthening of the gastrocnemius fascia in children with cerebral palsy, J Pediatr Orthop 13:727, 1993.
- Rosenthal RK: The use of orthotics in foot and ankle problems in cerebral palsy, Foot Ankle 4:195, 1984.
- Ryan DD, Rethlefsen SA, Skaggs DL, et al: Results of tibial rotational osteotomy without concomitant fi bular osteotomy in children with cerebral palsy, J Pediatr Orthop 25:84, 2005.
- Sala DA, Grant AD, Kummer FJ: Equinus deformity in cerebral palsy: recurrence after tendo Achilles lengthening, Dev Med Child Neurol 39:45, 1997.
- Samilson RL: Crescentic osteotomy of the os calcis for calcaneocavus feet. In Bateman JE, ed: Foot science, Philadelphia, 1976, Saunders. Saraph V, Zwick EB, Uitz C, et al: The Baumann procedure for fi xed contracture of the gastrosoleus in cerebral palsy, J Bone Joint Surg 82B:535, 2000.
- Scott SM, Janes PC, Stevens PM: Grice subtalar arthrodesis followed to skeletal maturity, J Pediatr Orthop 8:176, 1988.
- Sharrard WJW, Bernstein S: Equinus deformity in cerebral palsy: a comparison between elongation of the tendo calcaneus and gastrocnemius recession, J Bone Joint Surg 54B:272, 1972.
- Sharrard WJW, Smith TWD: Tenodesis of fl exor hallucis longus for paralytic clawing of the hallux in childhood, J Bone Joint Surg 58B:224, 1976.
- Silfverskiöld N: Reduction of the uncrossed two-joint muscles of the leg to one-joint muscles in spastic conditions, Acta Chir Scand 56:315, 1923-1924.
- Silver CM, Simon SD: Gastrocnemius muscle recession (Silfverskiöld operation) for spastic equinus deformity in cerebral palsy, J Bone Joint Surg 41A:1021, 1959.
- Silver CM, Simon SD, Litchman HM: Long term follow-up observations on
You Might Also Like


