Hallux Rigidus: Pathomechanics, Grading, and Surgical Management
Key Takeaway
Hallux rigidus is a progressive osteoarthritic condition of the first metatarsophalangeal (MTP) joint, characterized by pain and restricted dorsiflexion. Initial management includes stiff-soled shoes and activity modification. Operative interventions range from joint-preserving cheilectomy for early-stage disease to first MTP arthrodesis for advanced degeneration. Successful surgical outcomes depend on accurate radiographic grading, precise osteophyte resection, and restoration of pain-free first ray kinematics.
Introduction to Hallux Rigidus
Hallux rigidus, a term originally coined by Cotterill in 1888, refers to the progressive limitation of motion—specifically dorsiflexion—of the first metatarsophalangeal (MTP) joint due to degenerative osteoarthritis. It is the most common arthritic condition of the foot, frequently presenting with debilitating pain, dorsal osteophyte formation, and altered gait mechanics.
The etiology of hallux rigidus is multifactorial. It is strongly associated with hallux valgus interphalangeus, bilateral involvement in patients with a familial history, unilateral involvement in patients with a history of trauma, and female gender. Furthermore, specific occupational hazards or repetitive microtrauma can accelerate joint degeneration.


Pathomechanics and Etiology
Understanding the pathomechanics of hallux rigidus is critical for selecting the appropriate surgical intervention. McMaster provided foundational insights into the microscopic and macroscopic progression of the disease. In his evaluation of patients with hallux rigidus, the most common microscopic finding was a distinct cleavage lesion in the articular cartilage of the first metatarsal head, notably without any detached subchondral bone.
Radiographically, the earliest sign of this pathology is a small, subtle depression in the dome of the metatarsal head. Because this finding is easily overlooked, high clinical suspicion is required during early evaluation.
The Kinematic Cascade of Impingement
The cleavage lesion on the metatarsal head is consistently located between the apex of the dome and the dorsal margin of the articular surface. McMaster postulated that the characteristic tenderness over the dorsum of the first MTP joint, coupled with limited dorsiflexion, is directly explained by the classic site of this lesion.
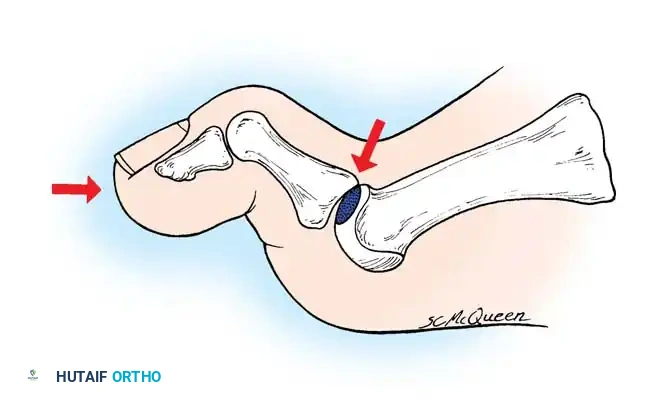
When the hallux is extended during the terminal stance phase of gait, the proximal phalanx abuts against this cleavage lesion. This abutment produces sharp pain, triggering an instinctive, protective flexion of the joint that actively limits extension.
As the disease progresses:
* Repetitive impingement leads to the formation of a proliferative dorsal osteophyte at the articular margin of the metatarsal head.
* This osteophyte creates a hard, mechanical block to extension.
* The first metatarsal is often forced dorsally, decreasing its inclination angle on a weight-bearing lateral radiograph—a condition known as primus elevatus.
Clinical Pearl: The elevation of the first metatarsal (primus elevatus) is generally considered secondary to the arthritic changes and altered mechanics of the first MTP joint, rather than the primary causal factor of hallux rigidus.

Clinical Evaluation and Grading
Accurate grading of hallux rigidus dictates the treatment algorithm. The Coughlin and Shurnas classification system is the gold standard, combining radiographic findings, clinical pain characteristics, and objective MTP joint motion.
Coughlin and Shurnas Grading System
- Grade 0:
- Radiograph: Normal.
- Pain: None.
- Motion: Stiffness or slight loss of motion.
- Grade 1:
- Radiograph: Minor narrowing of the MTP joint space; early dorsal osteophyte.
- Pain: Intermittent, mild pain at extremes of motion.
- Motion: Mild restriction.
- Grade 2:
- Radiograph: Moderate joint space narrowing; distinct osteophyte formation.
- Pain: More constant pain, particularly with activity.
- Motion: Moderate restriction.
- Grade 3:
- Radiograph: Severe joint space narrowing; extensive osteophyte formation.
- Pain: Constant pain at extremes of motion, but no pain at the midrange of MTP joint motion.
- Motion: Moderately severe restriction (< 20 degrees total motion).
- Grade 4:
- Radiograph: Same as Grade 3 (severe narrowing, extensive osteophytes).
- Pain: Pain is present even at the midrange of passive MTP joint motion.
- Motion: Same as Grade 3 (< 20 degrees total motion).
Surgical Warning: Thompson and Mann emphasized that arthrodesis should be considered if loss of joint space is evident not only on anteroposterior and lateral views but also on the oblique view. The oblique radiograph frequently reveals remaining viable joint space that is obscured on standard orthogonal views.
Nonoperative Management
In most patients, operative correction is eventually required to relieve pain and restore function. However, conservative management should always be the first line of treatment, particularly for Grades 0 through 2.
Smith, Katchis, and Ayson reported on the long-term follow-up of 18 patients (24 feet) treated nonoperatively. Over an average of 14 years, pain remained stable in 22 feet, improved in one, and worsened in only one, despite significant radiographic deterioration of the joint space.
Conservative Modalities Include:
* Shoe Modification: The most common and effective self-care measure is the use of a shoe with an ample, deep toe box to prevent dorsal pressure on the osteophyte.
* Orthotics: A stiff Morton's extension or a carbon fiber footplate limits MTP dorsiflexion during gait, reducing impingement pain.
* Pharmacotherapy: NSAIDs and targeted intra-articular corticosteroid injections can provide symptomatic relief during acute flares.
Operative Management: Decision Making
When nonoperative measures fail, surgical intervention is indicated. Historically, many operations have been recommended, including dorsal wedge osteotomies (Kessel and Bonney) for adolescents, and the Keller resection arthroplasty (Wrighton, Cleveland, Winant, Thomas). Today, the primary surgical workhorses are the Cheilectomy and First MTP Arthrodesis.
Indications by Grade
- Grades 1 and 2: Cheilectomy is highly successful. Coughlin and Shurnas reported successful pain relief and improved function in 92% of patients undergoing cheilectomy for early-stage disease.
- Grade 3: Treatment is controversial. Cheilectomy may be attempted if more than 50% of the metatarsal head cartilage remains viable. Otherwise, arthrodesis is preferred.
- Grade 4: First MTP Arthrodesis is the gold standard. Cheilectomy is contraindicated due to pain throughout the midrange of motion.
Cheilectomy: Joint-Preserving Surgery
The rationale for cheilectomy is the relief of painful mechanical impingement of the proximal phalanx on the dorsal osteophyte of the first metatarsal head. This is achieved by resecting the osteophyte, medial and lateral bony excrescences, and a portion of the dorsal articular cartilage to restore a minimum of 70 degrees of intraoperative dorsiflexion.
Mann and Clanton demonstrated that advanced arthritic changes are not an absolute contraindication to cheilectomy, provided 70 degrees of impingement-free motion is achieved. Interestingly, Feltham et al. noted that patients older than 60 years often achieve better functional results after cheilectomy than younger patients, regardless of deformity severity.
Surgical Technique: Cheilectomy
Surgical Goal: Remove the proliferative bone from around the metatarsal head to eliminate the dorsal buttress preventing dorsiflexion of the proximal phalanx.

Step 1: Approach and Exposure
* Make a dorsal longitudinal skin incision beginning approximately 1 cm proximal to the interphalangeal joint, extending proximally about 5 cm across the MTP joint.
* Deepen the incision through the subcutaneous tissue. Meticulously identify and retract the dorsal medial cutaneous nerve to prevent painful postoperative neuromas.
* Expose the extensor hallucis longus (EHL) tendon and the extensor hood. Incise the capsule longitudinally just medial or lateral to the EHL tendon.

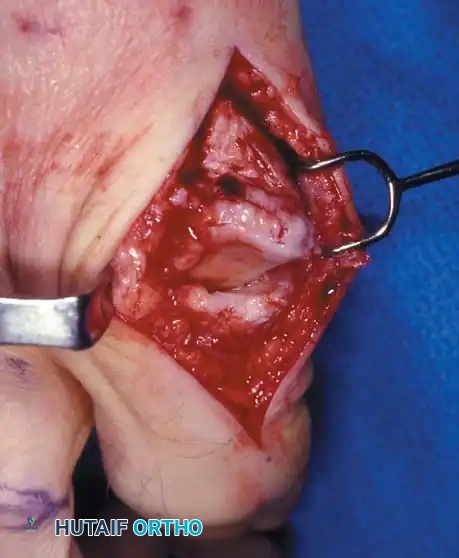
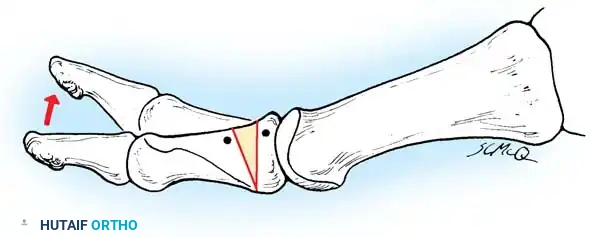
Step 2: Joint Debridement and Osteophyte Resection
* Elevate the capsule via sharp dissection to fully expose the metatarsal head and the base of the proximal phalanx.
* Identify the dorsal, medial, and lateral osteophytes. A prominent dorsolateral osteophyte is frequently present and must be completely excised.


- Using an oscillating saw or sharp osteotome, resect approximately 20% to 25% of the dorsal aspect of the metatarsal head. The cut should begin dorsally and exit just proximal to the dorsal articular margin, angling slightly plantarward.


Step 3: Dynamic Assessment and Closure
* Distract the joint and thoroughly irrigate to remove any loose cartilage, bone debris, or osteochondral fragments.
* Passively move the joint through its range of motion. You must achieve 60 to 70 degrees of impingement-free dorsiflexion. If impingement persists, resect additional dorsal bone.
* Palpate through the skin to ensure no abnormal bony prominences remain.
* Close the capsule with absorbable sutures and the skin with non-absorbable nylon sutures.

First MTP Arthrodesis: The Gold Standard for Advanced Disease
For patients with Grade 4 hallux rigidus, or Grade 3 with extensive cartilage loss, arthrodesis of the first MTP joint provides the most reliable, long-term pain relief. Fitzgerald, Moynihan, and McKeever were early pioneers of this technique.
In a randomized controlled trial, Gibson and Thompson compared arthrodesis against total replacement arthroplasty, concluding that functional outcomes and patient satisfaction were significantly superior following arthrodesis.
Biomechanics and Fixation Techniques
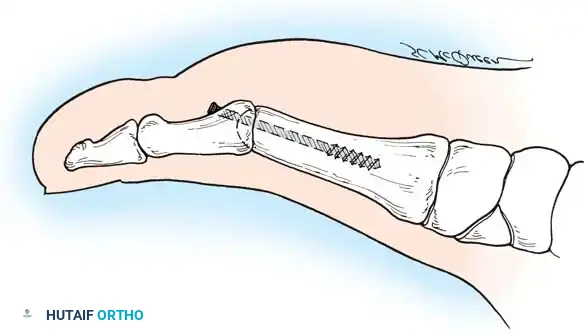
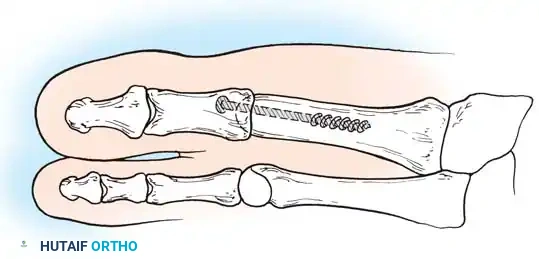
Modern fixation techniques have revolutionized fusion rates, achieving successful arthrodesis in 94% to 98% of cases. Politi et al. conducted a comprehensive biomechanical study demonstrating that the most stable fixation construct is a combination of an interfragmentary oblique lag screw and a dorsal neutralization plate.
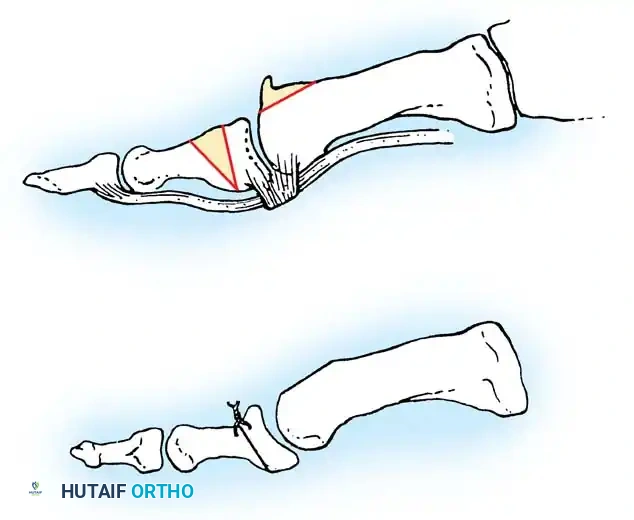
The McKeever Arthrodesis Technique
The McKeever technique utilizes conical reaming to prepare the joint surfaces, allowing for multi-planar adjustment of the toe before final fixation.
- Preparation: The metatarsal head is shaped into a convex cone, and the base of the proximal phalanx is reamed into a matching concave cup.
- **
Associated Surgical & Radiographic Imaging


You Might Also Like

