Cheilectomy for Hallux Rigidus: A Comprehensive Surgical Guide
Key Takeaway
Cheilectomy is a joint-sparing surgical procedure designed to treat early to moderate hallux rigidus. By resecting the dorsal metatarsal head osteophytes and proliferative bone, the procedure eliminates mechanical impingement and restores dorsiflexion of the first metatarsophalangeal joint. This guide details the precise surgical technique, biomechanical considerations, and postoperative protocols required to achieve optimal functional outcomes and relieve pain in patients suffering from symptomatic dorsal impingement.
Introduction to Cheilectomy and Hallux Rigidus
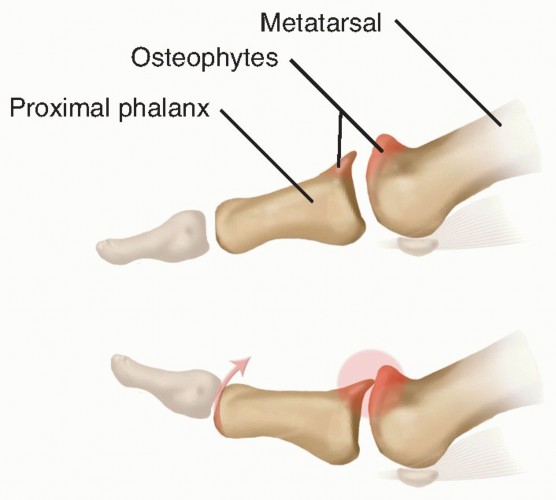
Hallux rigidus is a progressive osteoarthritic condition of the first metatarsophalangeal (MTP) joint, characterized by diminished dorsiflexion, periarticular osteophyte formation, and debilitating pain during the terminal stance phase of gait. The term "cheilectomy," derived from the Greek word cheilos (meaning "lip"), refers to the surgical excision of the proliferative dorsal bony lip (osteophyte) that forms around the metatarsal head.
The primary goal of a cheilectomy is to remove the mechanical buttress that prevents the proximal phalanx from gliding dorsally over the metatarsal head. By excising this dorsal exostosis, the surgeon decompresses the joint, eliminates dorsal impingement, and restores a functional arc of motion. This joint-sparing procedure remains the gold standard for early to moderate stages of hallux rigidus (Coughlin and Shurnas Grades I and II, and select Grade III cases) where the plantar articular cartilage remains largely viable.
Biomechanics and Pathoanatomy
Understanding the kinematics of the first MTP joint is critical for executing a successful cheilectomy. The first MTP joint is a complex hinge joint that must accommodate up to 65 to 75 degrees of dorsiflexion to allow for a normal windlass mechanism during the toe-off phase of gait.
In hallux rigidus, repetitive microtrauma, altered metatarsal length, or metatarsus primus elevatus leads to cartilage degradation, primarily on the dorsal aspect of the metatarsal head. As the cartilage wears, reactive woven bone forms a dorsal osteophyte. This osteophyte acts as a physical block. When the patient attempts to dorsiflex the hallux, the dorsal base of the proximal phalanx impinges against the metatarsal osteophyte, causing acute pain, capsular stretching, and eventual joint stiffness. Furthermore, the sesamoid complex, which normally glides distally during dorsiflexion, often becomes contracted and tethered by fibrotic volar structures, further restricting motion.
💡 Clinical Pearl: The Cam Effect
The first metatarsal head is not perfectly spherical; it functions as a cam. The center of rotation shifts plantarly as the toe dorsiflexes. If the dorsal osteophyte is not adequately resected, the proximal phalanx cannot translate dorsally, and the cam mechanism is abruptly halted, leading to jamming of the joint surfaces.
Preoperative Evaluation and Imaging
A meticulous preoperative assessment is mandatory. Patients typically present with a palpable dorsal prominence, pain with push-off, and a stiff first MTP joint. Clinical examination must quantify the active and passive range of motion, specifically noting the degree of dorsiflexion at which pain is elicited.
Standard weight-bearing radiographs (anteroposterior, lateral, and oblique views) are essential to evaluate the extent of joint space narrowing, the size of the dorsal exostosis, and the presence of loose bodies.

Anteroposterior and oblique views demonstrating severe hallux rigidus with extensive periarticular osteophyte formation and joint space obliteration.
In many instances, hallux rigidus presents bilaterally, necessitating a comprehensive evaluation of the contralateral foot to plan for staged or concurrent interventions.

Anteroposterior view of bilateral hallux rigidus, highlighting the symmetric nature of the degenerative process in susceptible individuals.
Historical Context and Failed Arthroplasty Alternatives
Historically, various interpositional arthroplasties and silastic implants were utilized to maintain joint space in advanced hallux rigidus. However, these procedures have largely fallen out of favor due to high complication rates, including implant fragmentation, reactive synovitis, and profound osteolysis.

Hallux rigidus previously treated with silicone-rubber spacers. Note the severe erosion of bone at the metatarsal head and the marked thickening of the soft tissue of the hallux resulting from silicone synovitis and edema. In such cases, the prosthesis must be removed, often requiring salvage arthrodesis.
Given the catastrophic failures associated with silicone implants, modern orthopedic practice heavily favors joint-sparing procedures like cheilectomy for early disease, and first MTP arthrodesis for end-stage disease.
Surgical Anatomy
A thorough understanding of the dorsal surgical anatomy is required to prevent iatrogenic injury during exposure:
* Extensor Hallucis Longus (EHL): The primary dorsiflexor of the interphalangeal joint, running centrally over the MTP joint.
* Extensor Hallucis Brevis (EHB): Inserts on the dorsal base of the proximal phalanx, lateral to the EHL.
* Dorsal Cutaneous Nerves: The dorsomedial cutaneous nerve (a branch of the superficial peroneal nerve) and the deep peroneal nerve supply sensation to the dorsal hallux. These must be meticulously protected during the superficial dissection.
* Extensor Hood: The fascial expansion that stabilizes the extensor tendons.
Step-by-Step Surgical Technique (Mann, Clanton, and Thompson)
The following technique outlines the classic, highly effective approach to cheilectomy, emphasizing precise bone resection and soft tissue release.
1. Patient Positioning and Anesthesia
The patient is placed in the supine position on the operating table. The procedure can be performed under a regional ankle block, spinal anesthesia, or general anesthesia, depending on patient preference and comorbidities. A calf or thigh tourniquet is applied to ensure a bloodless surgical field.
2. Incision and Superficial Dissection
- Make a longitudinal dorsal skin incision beginning approximately 1 cm proximal to the interphalangeal (IP) joint.
- Continue the incision proximally for about 5 cm, crossing directly over the first MTP joint.
- Deepen the incision carefully through the subcutaneous tissue and fat.
- Use blunt dissection to mobilize the skin flaps, taking great care to identify and retract the dorsal cutaneous nerve branches.
- Expose the extensor tendon (EHL) and the underlying extensor hood.
3. Capsulotomy and Joint Exposure
- Identify the EHL tendon and retract it medially (or laterally, depending on the exact location of the osteophytes, though lateral capsulotomy is standard).
- Make a longitudinal incision through the extensor hood and joint capsule, lateral to the EHL tendon.
- Elevate the capsule via sharp subperiosteal dissection to expose the dorsal, medial, and lateral aspects of the metatarsophalangeal joint.
- Use a self-retaining retractor or Hohmann retractors to maintain exposure of the metatarsal head and the base of the proximal phalanx.
4. Joint Debridement and Inspection
- Perform a thorough synovectomy to remove hypertrophic, inflamed synovial tissue that contributes to capsular impingement.
- Locate the dorsal and dorsolateral osteophytes on both the metatarsal head and the base of the proximal phalanx.
- Assess the degree of articular cartilage loss. In early hallux rigidus, the plantar two-thirds of the metatarsal head cartilage is typically preserved, while the dorsal one-third is fibrillated or absent.
- Identify and remove any loose bodies (joint mice) from the intra-articular space.
5. The Cheilectomy (Bone Resection)
The critical step of the procedure is determining the appropriate volume of bone to resect. Under-resection leads to persistent impingement, while over-resection can compromise the joint's weight-bearing capacity or destabilize the MTP joint.
- Sharply plantarflex the MTP joint to maximize exposure of the dorsal metatarsal head.
- Utilize a 6-mm osteotome (or a microsagittal saw) to remove 20% to 30% of the dorsal metatarsal head.
- The Resection Rule: The amount of bone removed is directly proportional to the size of the dorsal exostosis and the severity of articular cartilage destruction.
- If cartilage damage is minimal and the primary pathology is the exostosis, remove approximately 20% of the dorsal aspect.
- If articular damage is more extensive, increase the resection.
- In cases of severe dorsal articular damage (borderline Grade III), up to one-third (33%) of the dorsal aspect of the metatarsal head can be safely removed.
- Begin the resection just dorsal to the edge of what appears to be viable, healthy articular cartilage. The cut should be angled slightly dorsal-distal to plantar-proximal to ensure a smooth transition.
- Remove the osteophytes on the lateral and medial aspects of the joint in line with the long axis of the metatarsal. This narrows the metatarsal head less medially to laterally than dorsally to plantarly, preserving the collateral ligament origins where possible.
🚨 Surgical Warning: Angle of Resection
Do not direct the osteotome or saw blade too plantarly. The resection must remain parallel to the weight-bearing surface of the foot, not the anatomical axis of the elevated metatarsal. An overly aggressive plantar cut will compromise the articulation with the sesamoids and lead to transfer metatarsalgia.
6. Cartilage Contouring and Proximal Phalanx Debridement
- Use a rongeur or a high-speed burr to smooth the edges of the osteotomy, correcting any irregularities in the remaining articular cartilage.
- Remove any residual synovial tissue that may become pinched during dorsiflexion.
- Direct attention to the base of the proximal phalanx. Remove any corresponding dorsal osteophytes that could impinge against the newly contoured metatarsal head.
7. Intraoperative Assessment of Motion
- Once the bony resection is complete, assess the range of motion.
- Dorsiflexion of the MTP joint should now be possible to approximately 70 degrees.
- If 70 degrees of dorsiflexion cannot be achieved smoothly, the surgeon must re-evaluate the joint. The most common cause of restricted motion at this stage is inadequate bone removal from the metatarsal head, necessitating further resection.
8. Sesamoid Release
A frequently overlooked cause of persistent stiffness after cheilectomy is tethering of the sesamoid apparatus.
- Sharply plantarflex the MTP joint and visually inspect the sesamoid area beneath the metatarsal head.
- As the hallux is passively extended, the sesamoid bones should glide freely in a distal direction.
- If the sesamoids do not move freely, it indicates contracture of the volar plate and suspensory ligaments.
- Place a smooth instrument, such as a Freer elevator, between the plantar aspect of the metatarsal head and the dorsal surface of the sesamoids.
- Gently lever the instrument up and down, sweeping medially and laterally, to release the contracted volar structures and lyse adhesions until the sesamoids mobilize completely.
9. Closure
- Irrigate the joint copiously with sterile saline to remove all bone debris.
- Close the joint capsule and extensor hood over the EHL tendon using absorbable sutures (e.g., 2-0 or 3-0 Vicryl). Ensure the EHL is centralized and glides freely.
- Close the subcutaneous tissue and skin in a standard layered fashion.
- Apply a sterile, mildly compressive dressing.
Salvage Procedures: First MTP Arthrodesis
If intraoperative assessment reveals that the articular cartilage destruction is far more severe than anticipated (Grade IV hallux rigidus), or if the joint remains grossly unstable or painful, the surgeon must be prepared to convert the cheilectomy to a first MTP arthrodesis. Arthrodesis provides definitive pain relief at the cost of joint motion.
Postoperative anteroposterior radiograph demonstrating a solid first MTP arthrodesis using a dorsal plate and interfragmentary screw construct.
The success of an arthrodesis relies heavily on the precise positioning of the hallux. The toe must be positioned in approximately 10 to 15 degrees of valgus and 15 to 20 degrees of dorsiflexion relative to the first metatarsal to allow for normal toe-off during gait.

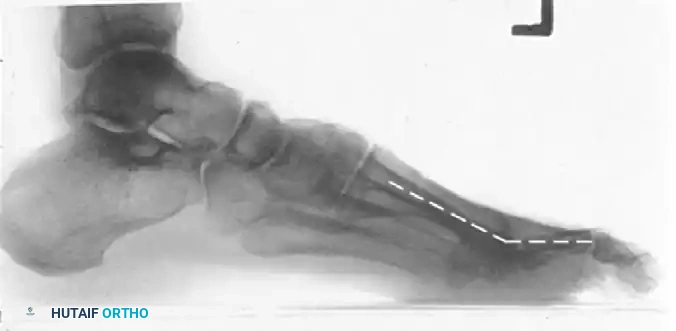
Postoperative lateral radiograph of a first MTP arthrodesis. Note the hardware placement and the preservation of the weight-bearing arch.

Postoperative lateral radiograph with dashed lines illustrating the optimal angle of arthrodesis, ensuring the hallux clears the ground slightly during the swing phase while providing a stable platform during stance.
Postoperative Protocol and Rehabilitation
The success of a cheilectomy is heavily dependent on aggressive postoperative rehabilitation to prevent capsular scarring and preserve the newly acquired range of motion.
- Weeks 0-2: The patient is placed in a rigid, flat-bottomed postoperative shoe. Weight-bearing to tolerance on the heel and lateral border of the foot is permitted immediately. The foot should be elevated to minimize edema. Sutures are typically removed at 10 to 14 days.
- Weeks 2-6: Once the incision is healed, aggressive physical therapy is initiated. The patient is instructed to perform active and passive dorsiflexion and plantarflexion exercises multiple times a day. The goal is to maintain the 70 degrees of dorsiflexion achieved intraoperatively.
- Weeks 6+: Transition to normal, supportive footwear. High-impact activities and sports can gradually be resumed as tolerated, usually around 8 to 12 weeks postoperatively.
Complications and Pitfalls
While cheilectomy is highly successful in appropriately selected patients, complications can occur:
- Inadequate Resection: Failing to remove enough of the dorsal metatarsal head or neglecting the sesamoid release will result in persistent stiffness and impingement pain.
- Over-Resection: Removing more than 30-40% of the metatarsal head can destabilize the joint, alter the mechanics of the intrinsic muscles, and lead to transfer metatarsalgia or a "cock-up" deformity of the hallux.
- Nerve Injury: Iatrogenic injury to the dorsomedial cutaneous nerve can cause painful neuromas or numbness over the hallux.
- Progression of Osteoarthritis: Cheilectomy does not halt the underlying degenerative process. Patients must be counseled that while the procedure provides excellent medium-to-long-term relief (often 10+ years), progressive joint space narrowing may eventually necessitate an arthrodesis.
- EHL Adhesions: Failure to initiate early range of motion can lead to the EHL tendon scarring down to the joint capsule, severely limiting active dorsiflexion.
Conclusion
Cheilectomy remains a highly effective, joint-preserving surgical intervention for early to moderate hallux rigidus. By meticulously resecting the dorsal osteophytes, contouring the metatarsal head, and ensuring the free excursion of the sesamoid apparatus, orthopedic surgeons can reliably restore functional dorsiflexion and eliminate impingement pain. Strict adherence to the surgical principles outlined above, combined with aggressive postoperative mobilization, ensures optimal outcomes and high patient satisfaction.
You Might Also Like