First MTP Joint Arthrodesis: Surgical Guide & Techniques
Key Takeaway
Arthrodesis of the first metatarsophalangeal (MTP) joint is the gold-standard surgical intervention for severe hallux valgus, hallux rigidus, and failed previous forefoot reconstructions. By providing a stable, pain-free plantigrade foot, this procedure reliably corrects complex deformities. Modern techniques utilizing cup-and-cone preparation combined with a dorsal precontoured plate and an independent lag screw offer superior biomechanical stability, allowing for early weight-bearing and excellent long-term clinical outcomes.
ARTHRODESIS OF THE FIRST METATARSOPHALANGEAL JOINT
Arthrodesis of the first metatarsophalangeal (MTP) joint is a highly reliable, durable, and definitive surgical intervention. In properly selected patients, arthrodesis of the first MTP joint for severe or recurrent hallux valgus is the most appropriate and biomechanically sound operation. By converting a painful, deformed, or unstable articulation into a solid, plantigrade construct, the procedure restores the weight-bearing capacity of the medial column and effectively eliminates forefoot pain.
Historically, resection arthroplasty (such as the Keller procedure) was utilized for similar indications; however, arthrodesis of the first MTP joint is vastly preferred, particularly in patients younger than 55 to 60 years of age, due to the preservation of the windlass mechanism and the avoidance of transfer metatarsalgia. Long-term clinical data strongly support this approach. Grimes and Coughlin reported excellent or good outcomes in 24 (72%) of 33 feet at an average of 8 years after arthrodesis for the treatment of a variety of failed hallux valgus procedures, including proximal and distal osteotomies, the McBride procedure, exostectomy, and resection arthroplasty.
Biomechanical Considerations and the Intermetatarsal Angle
A common misconception in forefoot reconstruction is that a severe intermetatarsal angle (IMA) mandates a concurrent proximal metatarsal osteotomy alongside the MTP arthrodesis. However, biomechanical and clinical evidence demonstrates that stabilizing the first MTP joint inherently reduces the intermetatarsal angle.
Mann and Katchurian reported a 4- to 5-degree average reduction in the intermetatarsal angle after arthrodesis alone. This spontaneous reduction occurs because the retrograde deforming force of the laterally deviated hallux is eliminated, allowing the medial capsule and the adductor hallucis to rebalance the first ray. Consequently, proximal metatarsal osteotomy combined with arthrodesis is generally not indicated except for the most extreme, rigid deformities where the intermetatarsal angle cannot be manually reduced intraoperatively.
Indications for First MTP Arthrodesis
The decision to proceed with a first MTP arthrodesis relies on a comprehensive clinical and radiographic evaluation. The procedure is indicated in the following specific circumstances:
1. Severe Hallux Valgus Deformity
Arthrodesis is the procedure of choice for severe deformity, typically defined by an intermetatarsal angle greater than 20 to 22 degrees, a hallux valgus angle (HVA) greater than 45 degrees, and severe pronation of the hallux.

FIGURE 81-58 A, Hallux valgus in a 46-year-old woman demonstrating severe lateral deviation and pronation of the great toe.

FIGURE 81-58 B, One year after arthrodesis, demonstrating excellent clinical alignment and restoration of the medial column.
This is especially critical when painful callosities are present beneath the second and third metatarsal heads in conjunction with an atrophic forefoot pad. The arthrodesis restores weight-bearing to the first ray, alleviating the transfer metatarsalgia.
2. Degenerative Arthritis with Hallux Valgus (Hallux Rigidus)
In the presence of advanced osteoarthritis (Grade III or IV hallux rigidus) combined with a valgus deformity, joint-sparing procedures will fail to relieve pain. Although uncommon, erosion along the lateral aspect of the sagittal groove with complete loss of articular cartilage is occasionally seen, particularly in patients older than 60 years. Arthrodesis definitively addresses both the deformity and the arthritic pain.
3. Mild-to-Moderate Deformity with Painful, Limited Motion
In cases where the deformity may not be radiographically severe, but the MTP joint exhibits significantly limited and painful range of motion (often due to previous trauma or early degenerative changes), arthrodesis is highly effective. While resection arthroplasty is a reasonable alternative in low-demand, elderly patients, arthrodesis remains the gold standard for active individuals.
4. Recurrent or Failed Hallux Valgus Surgery
Iatrogenic deformities or recurrences following previous forefoot surgeries (such as a failed McBride procedure, a collapsed metatarsal osteotomy, or a destabilizing Keller procedure) are prime indications for salvage via arthrodesis.

FIGURE 81-59 Severe hallux valgus is a good indication for arthrodesis of the first metatarsophalangeal joint, particularly in recurrent hallux valgus after a previous attempt at correction (left foot).
5. Neuromuscular Disorders
Hallux valgus caused by muscle imbalance in patients with neuromuscular disorders, such as cerebral palsy, Charcot-Marie-Tooth disease, or stroke, has an unacceptably high recurrence rate with soft-tissue or osteotomy-based procedures. Arthrodesis provides a static, bony block to recurrence.
6. Posttraumatic Hallux Valgus
Severe disruption of all medial capsular structures (often from crush injuries or high-energy trauma) that cannot be adequately reconstructed necessitates joint fusion to restore stability.
7. Rheumatoid Arthritis
Patients with rheumatoid arthritis often present with severe, progressive forefoot destruction. Arthrodesis of the first MTP joint, often combined with lesser metatarsal head resections (Hoffmann procedure), provides a durable, pain-free forefoot.
Clinical Pearl: In cases of severe metatarsus primus varus combined with hallux valgus, carefully assess the mobility of the first tarsometatarsal (TMT) joint. While MTP arthrodesis alone often reduces the IMA, a hypermobile or rigidly deviated first ray may occasionally require a concurrent proximal osteotomy or Lapidus procedure.

FIGURE 81-60 A, Severe hallux valgus with severe metatarsus primus varus.

FIGURE 81-60 B, After proximal metatarsal osteotomy and arthrodesis of the first metatarsophalangeal joint.
Surgical Technique: Joint Preparation and Fixation Constructs
The surgical technique for arthrodesis of the first metatarsophalangeal joint may vary according to the type of osteotomy (joint preparation) and the kind of fixation used.
Joint Surface Preparation
Historically, joint surfaces were cut flat using an oscillating saw. While this allows for correction of severe deformities, it shortens the first ray significantly and offers limited adjustability once the cuts are made.
Modern techniques predominantly utilize specialized hemispherical reamers to create a “cup-and-cone” configuration. The metatarsal head is reamed into a convex cone, and the base of the proximal phalanx is reamed into a concave cup.
* Advantages of Cup-and-Cone: This configuration preserves metatarsal length, maximizes the cancellous bone surface area for fusion, and allows for infinite multiplanar adjustability (dialing in the exact degrees of valgus, dorsiflexion, and rotation) prior to definitive fixation.
Fixation Biomechanics
Fixation may include Kirschner wires, crossed cortical screws, lag (compression) screws, or dorsal plates.
Extensive biomechanical assessment of five commonly used arthrodesis techniques determined that the most stable construct is obtained with an oblique lag screw combined with a dorsal neutralization plate.
* The Lag Screw: Provides critical interfragmentary compression across the prepared cancellous bone surfaces, which is essential for primary bone healing.
* The Dorsal Plate: Acts as a tension-band and neutralization device, resisting the plantar-gapping forces exerted on the joint during the toe-off phase of gait.
Various arthrodesis plates are now manufactured with contoured dorsiflexion angles of 9 to 10 degrees. These low-profile plates, in combination with a lag or compression screw, provide strong fixation that allows immediate full weight-bearing in a stiff-soled postoperative shoe or boot, eliminating the need for a cast.
Surgical Warning: Specially designed, precontoured plates are strongly preferred over improvised, manually bent straight plates. Manual bending leads to poor control over the final dorsiflexion angle, creates stress risers in the titanium or stainless steel, and significantly increases the incidence of catastrophic plate failure and nonunion.
Step-by-Step Surgical Approach
1. Patient Positioning and Anesthesia
The patient is placed supine on the operating table. A regional ankle block or popliteal sciatic nerve block is highly recommended for postoperative pain control, supplemented by general anesthesia or deep sedation. A calf or thigh tourniquet is applied to ensure a bloodless surgical field. A small bump may be placed under the ipsilateral hip to internally rotate the leg to a neutral position, ensuring the foot rests perfectly vertical.
2. Incision and Exposure
A dorsal or dorsomedial longitudinal incision is made, approximately 5 to 6 cm in length, centered over the first MTP joint.
* Careful blunt dissection is utilized to identify and protect the extensor hallucis longus (EHL) tendon, which is retracted laterally.
* The dorsomedial cutaneous nerve branches must be identified and gently retracted to prevent painful postoperative neuromas.
* A longitudinal capsulotomy is performed, and the capsule is elevated off the metatarsal head and the base of the proximal phalanx via sharp dissection, exposing the joint completely. Collateral ligaments are released to allow full plantarflexion of the phalanx, providing access to the entire metatarsal head.
3. Joint Preparation (Cup-and-Cone Technique)
Aggressive osteophytes (dorsal, medial, and lateral) are resected using a rongeur or oscillating saw to restore the normal anatomic footprint of the bones.
* A guide pin is driven centrally into the metatarsal head, aligned with the anatomical axis of the first metatarsal.
* The convex reamer is passed over the pin to remove the remaining articular cartilage and expose bleeding subchondral bone. Care must be taken to avoid over-reaming, which can compromise the structural integrity of the metatarsal head.
* The process is repeated on the proximal phalanx using the concave reamer.
* The subchondral bone is then aggressively fenestrated with a 2.0 mm drill bit or K-wire to promote marrow venting and osteogenesis.
4. Positioning and Alignment (The Critical Step)
Achieving the correct three-dimensional alignment is the most crucial step in preventing postoperative complications such as interphalangeal joint arthritis, hallux hammering, or transfer metatarsalgia.
* Valgus: The hallux should be positioned in 10 to 15 degrees of valgus, ensuring it rests parallel to the second toe without impinging on it.
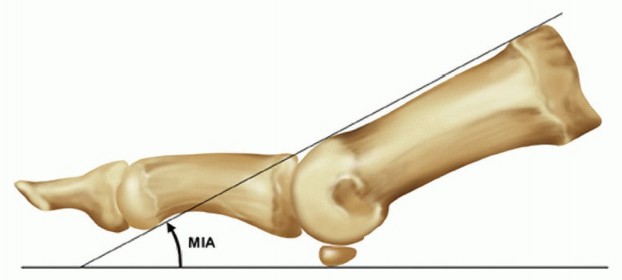
* Dorsiflexion: The hallux must be positioned in 10 to 15 degrees of dorsiflexion relative to the floor (simulated weight-bearing), which equates to approximately 20 to 25 degrees of dorsiflexion relative to the longitudinal axis of the first metatarsal.
* Rotation: The toe must be in neutral rotation. The toenail should face directly dorsal.
Pitfall: Excessive dorsiflexion leads to shoe-wear irritation and a "cocked-up" toe. Inadequate dorsiflexion (a toe that is too straight or plantarflexed) causes severe vaulting during gait, excessive pressure on the interphalangeal joint leading to rapid arthritis, and an inability to wear shoes with any heel elevation.
5. Temporary Fixation and Fluoroscopic Verification
Once the ideal position is achieved, two crossed 0.062-inch Kirschner wires are driven across the joint to hold the alignment. The foot is loaded with a flat plate (simulating weight-bearing) to clinically verify that the pulp of the toe rests appropriately on the ground. Anteroposterior and lateral fluoroscopic views are obtained to confirm alignment, hardware trajectory, and complete apposition of the bony surfaces.
6. Definitive Fixation
- Lag Screw Insertion: A 3.5 mm or 4.0 mm cannulated or non-cannulated lag screw is inserted. The trajectory is typically from the medial-plantar aspect of the proximal phalanx, directed proximally and laterally into the metatarsal head. The screw is tightened to achieve rigid interfragmentary compression.
- Plate Application: A precontoured dorsal plate (with 9 to 10 degrees of built-in dorsiflexion) is placed over the dorsal aspect of the joint. It is secured with locking or non-locking screws. Ensure that the proximal screws have adequate purchase in the metatarsal diaphyseal bone and the distal screws are securely anchored in the proximal phalanx without penetrating the interphalangeal joint.
7. Closure
The surgical site is irrigated copiously. The capsule and extensor retinaculum are repaired over the plate using absorbable sutures to provide a soft-tissue buffer between the hardware and the skin. The subcutaneous tissue and skin are closed meticulously. A sterile, bulky compressive dressing is applied.
Postoperative Protocol
Modern rigid fixation techniques have revolutionized the postoperative rehabilitation of the first MTP arthrodesis, shifting away from prolonged cast immobilization.
- Weeks 0 to 2: The patient is placed in a rigid postoperative shoe or a controlled ankle motion (CAM) boot. Immediate heel-weight-bearing or flat-foot weight-bearing is permitted, strictly avoiding toe-off loading. The foot must remain elevated as much as possible to minimize edema and promote wound healing.
- Weeks 2 to 6: Sutures are removed at 14 days. The patient continues weight-bearing in the rigid shoe. Radiographs are obtained at 6 weeks to assess for bridging trabecular bone and maintenance of alignment.
- Weeks 6 to 10: Once clinical and radiographic signs of union are evident, the patient is transitioned into a stiff-soled athletic shoe with a wide toe box. Normal gait mechanics are gradually reintroduced.
- Return to Activity: High-impact activities and sports are typically restricted until 3 to 4 months postoperatively, ensuring complete bony consolidation.
Complications and Management
While highly successful, first MTP arthrodesis carries potential complications that the orthopedic surgeon must be prepared to manage:
- Nonunion: The rate of nonunion ranges from 5% to 10%. Risk factors include smoking, diabetes, poor bone stock, and inadequate fixation. Asymptomatic nonunions (fibrous unions) may be observed. Symptomatic nonunions require revision arthrodesis, often utilizing structural bone graft (autograft or allograft) and revision hardware.
- Malunion: Incorrect intraoperative positioning is the most common cause of patient dissatisfaction. Excessive plantarflexion causes IP joint arthritis; excessive valgus causes impingement on the second toe. Symptomatic malunions require corrective closing-wedge or opening-wedge osteotomies through the fusion mass.
- Hardware Prominence: The dorsal plate may become palpable and irritating, particularly in patients with thin soft-tissue envelopes. Once the arthrodesis is solidly fused (typically after 6 to 12 months), the hardware can be safely removed in a minor outpatient procedure.
- Interphalangeal (IP) Joint Degeneration: Over time, the IP joint compensates for the lack of MTP motion. While mild radiographic changes are common, severe symptomatic arthritis is rare unless the MTP joint was fused in inadequate dorsiflexion.
In conclusion, arthrodesis of the first metatarsophalangeal joint remains an indispensable procedure in the orthopedic armamentarium. By adhering to strict biomechanical principles, utilizing modern cup-and-cone preparation, and applying rigid lag screw and plate fixation, surgeons can reliably provide patients with a durable, pain-free, and highly functional foot.
You Might Also Like