The Akin Procedure: Comprehensive Surgical Guide
Key Takeaway
The Akin procedure is a medial closing wedge osteotomy of the proximal phalanx of the great toe, primarily indicated for correcting hallux valgus interphalangeus or an abnormal distal articular set angle. This guide details the step-by-step surgical technique, including medial eminence removal, adductor tenotomy, osteotomy execution, fixation strategies, and postoperative protocols to optimize patient outcomes and minimize complications such as nonunion or malunion.
Introduction to the Akin Procedure
The Akin procedure, originally described in 1925 and subsequently modified by surgeons such as Frey and Beskin, remains a cornerstone in the operative armamentarium of the foot and ankle surgeon. It is fundamentally a medial closing wedge osteotomy of the proximal phalanx of the hallux. While historically utilized as an isolated procedure for hallux valgus, contemporary orthopedic practice predominantly employs the Akin osteotomy as a powerful adjunctive procedure. It is most frequently performed in conjunction with first metatarsal osteotomies (such as the Chevron, Scarf, or Lapidus procedures) to achieve complete multi-planar correction of complex hallux valgus deformities.
The primary objective of the Akin procedure is to correct hallux valgus interphalangeus (HVI) or an abnormal distal articular set angle (DASA). By resecting a precisely measured medially based wedge of cancellous bone from the proximal phalanx, the surgeon can realign the mechanical axis of the hallux, thereby restoring congruent joint kinematics and alleviating medial column pain.
Indications and Patient Selection
Thorough clinical and radiographic evaluation is paramount to determine the appropriateness of an Akin osteotomy. The procedure is rarely indicated for severe, incongruent metatarsophalangeal (MTP) joint deformities in isolation, as it does not address the primary pathology at the first tarsometatarsal or MTP joints.
Primary Indications
- Hallux Valgus Interphalangeus (HVI): An HVI angle exceeding the normal physiological limit of 10 degrees.
- Abnormal Distal Articular Set Angle (DASA): A DASA greater than 8 degrees, indicating an intrinsic structural deformity of the proximal phalanx.
- Adjunctive Correction: Residual clinical valgus of the hallux following a technically successful first metatarsal osteotomy and lateral soft tissue release.
- Congruent Hallux Valgus: Mild hallux valgus with a congruent MTP joint where the deformity is entirely intra-phalangeal.
Contraindications
- Degenerative Joint Disease: Advanced osteoarthritis of the first MTP joint or interphalangeal (IP) joint (requires arthrodesis).
- Incongruent MTP Joint: Performing an Akin without addressing an incongruent MTP joint will lead to rapid recurrence and altered joint mechanics.
- Short Proximal Phalanx: A congenitally short proximal phalanx may not provide adequate bone stock for a stable osteotomy and fixation.
- Active Infection or Severe Vascular Compromise: Absolute contraindications for elective osteotomies.
Surgical Anatomy and Preoperative Planning
Successful execution of the Akin procedure requires an intimate understanding of the vascular supply and soft tissue envelope surrounding the proximal phalanx. The primary blood supply to the proximal phalanx is derived from the first dorsal metatarsal artery and the plantar metatarsal arteries.

⚠️ Surgical Warning: Periosteal Preservation
The vascularity of the proximal phalanx is highly dependent on its periosteal envelope. Excessive periosteal stripping, particularly with a periosteal elevator, severely compromises the local blood supply. This is the leading iatrogenic cause of delayed union or nonunion in the Akin procedure. Dissection must be strictly sharp and limited only to the osteotomy site.
Preoperative templating involves measuring the HVI and DASA on weight-bearing anteroposterior (AP) radiographs. The width of the medially based wedge is calculated to ensure the apex of the osteotomy terminates exactly at the lateral cortex, allowing for a stable greenstick fracture (osteoclasis) rather than a complete through-and-through osteotomy, which would destabilize the phalanx.
Patient Positioning and Anesthesia
- Anesthesia: The procedure is typically performed under a regional ankle block or popliteal fossa block, supplemented with monitored anesthesia care (MAC) or general anesthesia depending on patient preference and concurrent procedures.
- Positioning: The patient is placed in the supine position on the operating table.
- Tourniquet: A calf or thigh tourniquet is applied to provide a bloodless surgical field. Exsanguination is achieved using an Esmarch bandage prior to tourniquet inflation.
Step-by-Step Surgical Technique
1. Incision and Medial Eminence Removal
The approach begins with meticulous soft tissue handling to expose the medial aspect of the first MTP joint and the proximal phalanx.
- Incision: Make a longitudinal medial incision along the proximal two-thirds of the proximal phalanx. Extend this incision proximally over the medial eminence to expose the distal metatarsal shaft capsule, stopping approximately 2 to 3 mm proximal to its attachment on the metatarsal neck.
- Dissection: Expose the proximal phalanx utilizing strictly sharp dissection (scalpel only). Do not use a periosteal elevator. Expose just enough bone to safely make the osteotomy cuts.
- Capsular Management: Raise the capsule surrounding the exostosis by sharp dissection to expose the medial eminence. It is critical to preserve as much of the proximal capsular attachment to the metatarsal neck as possible to facilitate robust closure and maintain joint stability.
- Exostectomy: Remove the medial eminence using the parasagittal groove as a starting anatomical landmark. Following the resection, use a rongeur or a fine rasp to smooth the rough margins of the remaining cancellous bone.
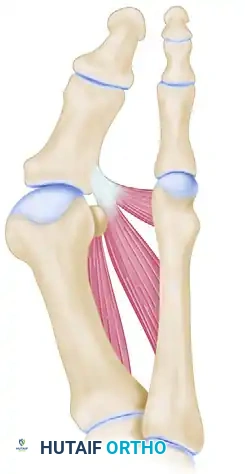
2. Adductor Tenotomy (Lateral Release)
If the Akin is being performed as part of a broader hallux valgus correction, an adductor tenotomy is often required to release the deforming lateral forces.
- Second Incision: Make a second linear incision dorsally to expose the adductor tendon. Begin this incision 2.5 to 3.0 cm proximal to the dorsal edge of the first web space, ending it 2.0 to 3.0 mm before entering the skin fold.
- Soft Tissue Preservation: Carefully preserve as many superficial veins as possible. If branches of the first dorsal metatarsal artery limit the exposure, they must be carefully ligated or coagulated.
- Nerve Retraction: Identify and gently retract the branches of the deep peroneal nerve.
- Tenotomy: Identify the adductor hallucis tendon. Incise it sharply from its insertion at the base of the proximal phalanx and from the lateral edge of the fibular sesamoid.
3. The Proximal Phalangeal Osteotomy
This is the most critical phase of the procedure. Precision in the osteotomy cuts dictates the final alignment and stability of the hallux.
- Exposure: Return to the initial medial incision. Use small, right-angle retractors (such as Senn or Ragnell retractors) to protect the dorsal and plantar soft tissues.
- First Osteotomy Cut (Distal): Begin the proximal phalangeal transverse osteotomy 6 to 8 mm distal to the MTP joint articular surface. The cut must be parallel to the apex of the concavity of the proximal articular surface of the phalanx. Utilize a power oscillating saw with a 4-mm-wide blade.
- Lateral Cortex Preservation: It is imperative to cut through the medial, dorsal, and plantar cortices while leaving the lateral cortex intact to act as a mechanical hinge.
- Second Osteotomy Cut (Proximal): Begin the second osteotomy 3 to 4 mm distal to the first cut. Direct the saw blade obliquely and proximally so that it intersects the first osteotomy precisely at the lateral cortex.

💡 Clinical Pearl: Preventing Dorsiflexion Malunion
When making the osteotomy cuts, ensure the saw blade is perfectly perpendicular to the longitudinal axis of the phalanx in the sagittal plane. A plantar-convergent wedge will inadvertently cause a dorsiflexion malunion of the hallux, leading to loss of toe purchase and transfer metatarsalgia.
4. Deformity Correction and Osteoclasis
- Wedge Removal: Carefully remove the excised wedge of cancellous bone by gently rocking it back and forth with a small Kocher clamp or a towel clip.
- Osteoclasis: Close the osteotomy by applying a gentle, steady valgus force to the distal phalanx, creating a greenstick fracture (osteoclasis) of the intact lateral cortex.
- Rotational Correction: During the closure of the osteotomy, a few degrees of pronation of the hallux (often present in hallux valgus) can be simultaneously corrected by gently supinating the toe as the bony surfaces are compressed.
- Medial Flare Resection: If the medial flare of the base of the proximal phalanx produces an annoying bony prominence after closure, it can be carefully resected with a rongeur to ensure a smooth medial contour.
Alternative: Distal Phalangeal Neck Osteotomy
While the basilar (proximal) Akin is the most common, the same geometric principles can be applied to the neck of the proximal phalanx. This distal Akin is specifically indicated when the deformity (HVI) is localized entirely to the interphalangeal joint rather than the proximal diaphysis.

5. Fixation Techniques
Rigid fixation is required to maintain the correction and promote primary bone healing. Several techniques are viable, depending on surgeon preference and bone quality.
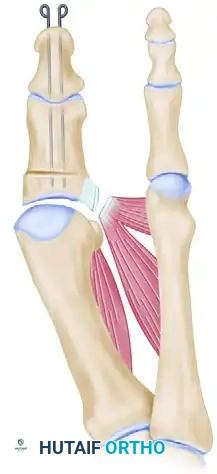
Kirschner Wire (K-wire) Fixation
- Primary Wire: Drill a 0.062-inch smooth K-wire through the distal and proximal phalanges while holding the IP joint in a neutral position. Inserting this wire 2 to 3 mm plantar to the tip of the nail facilitates its passage into the medullary canals of both phalanges. Advance the wire across the osteotomy site and into the subchondral bone of the proximal phalanx base.
- Rotational Control: Place a second 0.062-inch or 0.045-inch K-wire parallel to the first to control rotation at the osteotomy site.
- Capsular Protection: If the medial capsule is too attenuated to hold the hallux reduced on the metatarsal head, the K-wires can be driven across the MTP joint and into the metatarsal head to temporarily protect the capsular repair.
- Crossed Wires: If parallel wires are insufficient to maintain the corrected position, two crossed K-wires can be placed from distal to proximal. The ends are bent outside the skin to prevent migration.
Intraosseous Suture Fixation (Beskin Technique)
As an alternative to metallic hardware, heavy absorbable sutures can provide excellent dynamic compression.
* Using a 0.045-inch K-wire as a drill, place two sets of parallel holes medially on either side of the osteotomy site.
* Leave a 2 to 3-mm bone bridge on either side of the osteotomy to prevent suture pull-through.
* Angle the drill holes at 45 to 60 degrees to allow for easier passage of the needle.
* Pass a 2-0 absorbable, monofilament, polydioxanone (PDS) suture through the holes.
* Biomechanical Advantage: Beskin noted that PDS suture possesses a slight elasticity that provides continuous, excellent compression at the osteotomy site. This precludes the need for buried metallic wires or percutaneous pins, thereby eliminating the risk of pin tract infections and hardware irritation.
6. Capsular Closure and Dressing
- Capsulorrhaphy: Overlap the medial capsule to judge redundancy. Excise an appropriate amount of redundant tissue from the dorsal side to ensure a tight medial reefing.
- Suturing: Use 2-0 or 3-0 absorbable sutures (e.g., Vicryl) for a robust capsular closure.
- Hemostasis: Deflate the tourniquet and secure meticulous hemostasis using electrocautery before skin closure to prevent postoperative hematoma.
- Skin Closure: Close the skin using non-absorbable monofilament sutures (e.g., 4-0 Nylon) in a simple interrupted or horizontal mattress fashion.
- Pin Management: If percutaneous K-wires were used, bend loops in the tips protruding from the distal end of the toe to prevent proximal migration.
- Dressing: Apply a sterile, mildly compressive dressing, ensuring the hallux is splinted in the corrected, neutral alignment.
Postoperative Care and Rehabilitation
The postoperative protocol is designed to protect the osteotomy while allowing for early mobilization to prevent stiffness.
- Phase 1 (0 to 72 Hours): The patient is instructed to strictly rest and elevate the extremity above heart level to minimize edema. Bathroom privileges only are permitted.
- Phase 2 (3 Days to 4 Weeks): Weight-bearing to tolerance is generally allowed in a rigid-soled postoperative shoe. A cast is typically unnecessary for adults. However, in adolescent patients with excessive hallux valgus interphalangeus or questionable compliance, a short-leg walking cast extending past the toes is highly recommended for the first month.
- Phase 3 (3 to 4 Weeks): Skin sutures and percutaneous K-wires are removed in the clinic. The patient may transition to a deep, wide, soft-accommodative shoe.
- Phase 4 (4 Weeks and Beyond): Once the pins are removed, gentle active and passive range of motion (ROM) exercises of the MTP and IP joints are initiated to prevent arthrofibrosis.
Clinical stability of the osteotomy is usually achieved at 4 to 6 weeks. However, surgeons must counsel patients that complete radiographic healing (consolidation of the osteotomy site) may take 3 to 6 months or longer.
Complications and Management
While the Akin procedure is highly successful when executed correctly, complications can occur.
- Delayed Union and Nonunion: Nonunion is relatively uncommon, occurring in approximately 1% of patients. It is almost exclusively the result of excessive periosteal stripping or thermal necrosis from the saw blade. Management includes prolonged immobilization, bone stimulators, or revision surgery with bone grafting and rigid internal fixation.
- Malunion: Asymmetric wedge resection can lead to dorsiflexion or plantarflexion malunion. A dorsiflexion malunion is particularly problematic as it results in a "floating toe" with loss of hallux purchase and subsequent transfer metatarsalgia to the lesser metatarsals.
- Hardware Complications: Percutaneous K-wires carry a risk of pin tract infection and migration. If infection occurs, prompt removal of the pin and oral antibiotics are usually curative.
- Overcorrection/Undercorrection: Over-resection of the medial wedge can result in hallux varus, while under-resection leaves residual valgus deformity. Precise preoperative templating and intraoperative fluoroscopy are essential to prevent these geometric errors.
- Lateral Cortex Fracture: If the lateral hinge is inadvertently breached during the osteotomy, the construct becomes highly unstable. The surgeon must immediately transition from simple K-wire or suture fixation to a more rigid construct, such as a miniature locking plate or crossed compression screws, to prevent displacement.
📚 Medical References
- : an analysis of results, Foot Ankle 12:1, 1991.
- Gazdag A, Cracchiolo A: Surgical treatment of patients with painful instability of the second metatarsophalangeal joint, Foot Ankle Int 19:137, 1998.
- Haddad SL, Sabbagh RC, Resch S, et al: Results of fl exor-toextensor and extensor brevis tendon transfer for correction of the crossover second toe deformity, Foot Ankle Int 20:781, 1999.
- Mann RA, Mizel MS: Monarticular nontraumatic synovitis of the metatarsophalangeal joint: a new diagnosis? Foot Ankle 6:18, 1985.
- Martin MG, Masear VR: Triggering of the lesser toes at a previously undescribed distal pulley stem, Foot Ankle Int 19:113, 1998.
- Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint, Foot Ankle Int 18:424, 1997.
You Might Also Like
