SC Joint Disorders: Causes, Symptoms & Effective Relief
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about SC Joint Disorders: Causes, Symptoms & Effective Relief. SC joint disorders are conditions affecting the sternoclavicular joint, located where the clavicle meets the sternum. These commonly arise from injuries such as sprains, fractures, or dislocations, often from accidents or sports. Degenerative changes, where articular cartilage wears away, also cause SC joint disorders, leading to pain, stiffness, and reduced motion. Posterior dislocations are severe and require urgent medical care.
Introduction and Epidemiology
The sternoclavicular (SC) joint represents the sole bony articulation between the upper extremity and the axial skeleton. Despite its critical role in shoulder girdle stability and mobility, pathological conditions affecting the SC joint are relatively uncommon compared to other shoulder pathologies, yet they can be debilitating and, in specific contexts, life-threatening. Disorders of the SC joint encompass a spectrum from acute traumatic injuries to chronic degenerative processes and inflammatory arthropathies. Traumatic injuries are frequently encountered in younger, active populations, often as a sequela of high-energy motor vehicle accidents or participation in collision sports such as football and rugby. Degenerative changes, conversely, are more prevalent in older demographics, reflecting the cumulative effects of microtrauma and biomechanical stresses over time.
Epidemiologically, SC joint dislocations constitute a small fraction of all shoulder girdle dislocations, with an estimated incidence of 1-3% of all dislocations of the shoulder girdle. Anterior dislocations are significantly more common than posterior dislocations, with a reported ratio ranging from 9:1 to 20:1. While anterior dislocations are typically less severe and often amenable to non-operative management, posterior dislocations demand immediate attention due to the high propensity for life-threatening complications involving critical mediastinal structures. Medial clavicle fractures, while rare, can also involve the SC joint, presenting unique challenges in stabilization. Inflammatory conditions, such as rheumatoid arthritis, psoriatic arthritis, or septic arthritis, though infrequent, must also be considered in the differential diagnosis, particularly in at-risk patient populations. The rarity of SC joint pathology often leads to delayed diagnosis or misdiagnosis, underscoring the necessity for a comprehensive understanding of its anatomy, biomechanics, and clinical manifestations among orthopedic surgeons.
Surgical Anatomy and Biomechanics
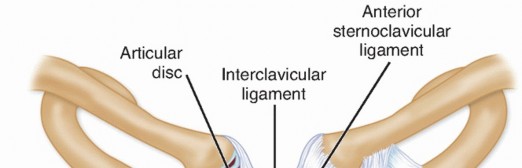
The sternoclavicular joint is a diarthrodial saddle joint formed by the articulation of the medial end of the clavicle with the manubrium of the sternum and the first costal cartilage. Despite the incongruity of the articulating surfaces, which is typically found in diarthrodial joints, the SC joint exhibits remarkable stability primarily through its robust ligamentous apparatus and the presence of an intra-articular disc.
Osseous Structures
The medial clavicular head is larger and convex in both the anteroposterior and superoinferior directions, while the sternal facet on the manubrium is concave. The first costal cartilage also contributes to the articular surface. This inherent bony incongruity highlights the critical role of soft tissue stabilizers. The epiphysis of the medial clavicle is the last to fuse, typically between 20-25 years of age, which has implications for injuries in skeletally immature patients, where physeal fractures may be mistaken for dislocations.
Ligamentous Stabilizers
The joint capsule itself is relatively thin but reinforced by a complex arrangement of ligaments:
- Anterior Sternoclavicular Ligament: This broad, strong ligament covers the anterior aspect of the joint and resists posterior displacement of the clavicle.
- Posterior Sternoclavicular Ligament: Thicker and stronger than its anterior counterpart, this ligament is the primary restraint against anterior displacement of the clavicle. Its integrity is paramount in preventing the more dangerous posterior dislocations.
- Interclavicular Ligament: Connecting the superior aspects of the medial ends of both clavicles, this ligament crosses the sternal notch and limits excessive depression of the clavicle.
- Costoclavicular (Rhomboid) Ligament: An extrinsic ligament located inferior to the joint, connecting the inferior surface of the medial clavicle to the superior surface of the first rib. It is a crucial primary stabilizer, resisting superior clavicular displacement and excessive elevation, and providing significant static stability against both anterior and posterior translation.
Intra-articular Disc
A fibrocartilaginous disc is consistently present within the SC joint, dividing the joint into two separate synovial compartments. This disc attaches superiorly to the clavicle, inferiorly to the first costal cartilage, and anteriorly and posteriorly to the joint capsule. Functionally, the disc enhances joint congruence, acts as a shock absorber, and contributes significantly to joint stability, particularly against medial and superior displacement of the clavicle. Degeneration or tears of this disc can lead to pain and instability.

Illustrative representation of the sternoclavicular joint anatomy, highlighting the osseous structures and key ligamentous stabilizers.
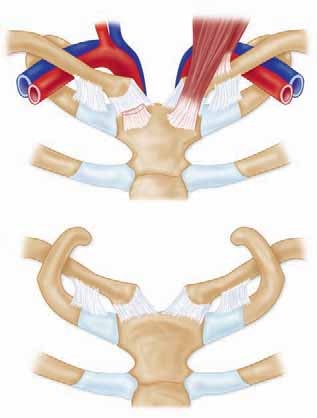
Adjacent Vital Structures
The posterior aspect of the SC joint is in intimate proximity to several critical neurovascular and visceral structures, making posterior dislocations particularly hazardous:
- Vascular Structures: Brachiocephalic (innominate) artery and vein, subclavian artery and vein, internal jugular vein, common carotid artery.
- Visceral Structures: Trachea, esophagus, apex of the lung (pleural dome).
- Nerves: Vagus nerve, recurrent laryngeal nerve, phrenic nerve.
Damage to these structures can result in life-threatening hemorrhage, airway compromise, esophageal perforation, or neurological deficits. This anatomical relationship necessitates an urgent and often multidisciplinary approach to posterior SC joint dislocations.

Detailed anatomical view demonstrating the sternoclavicular joint and its close relationship to vital mediastinal structures.
Biomechanics
The SC joint is a triaxial joint, permitting movements in three planes:
1. Elevation and Depression: Approximately 35-45 degrees of elevation and 10 degrees of depression.
2. Protraction and Retraction: Approximately 15-20 degrees of protraction and retraction.
3. Axial Rotation: Approximately 30-50 degrees of posterior axial rotation, coupled with glenohumeral abduction.
These movements are critical for the full range of motion of the upper extremity. The SC joint acts as the fulcrum for much of the shoulder girdle's motion, translating forces from the arm to the trunk. The coupled motion between the SC, AC, and glenohumeral joints ensures smooth, coordinated movement of the entire upper limb. Disruption of SC joint mechanics can significantly impair shoulder function and strength.
Indications and Contraindications
The decision-making process for the management of SC joint disorders is guided by the specific pathology, acuity, patient symptomatology, and potential for complications. A thorough clinical assessment, complemented by appropriate imaging, is paramount.
Indications for Operative Intervention
Operative management is generally reserved for situations where non-operative measures have failed, or for conditions presenting an immediate threat to the patient.
Contraindications for Operative Intervention
Absolute contraindications for SC joint surgery are rare and primarily revolve around patient stability and infection. Relative contraindications require careful consideration of risks versus benefits.
| Condition | Operative Indications | Non-Operative Indications |
|---|---|---|
| Acute Anterior Dislocation | Irreducible closed dislocation, open dislocation, recurrent symptomatic instability after initial reduction, associated neurovascular injury requiring exploration. | Majority of cases: Closed reduction followed by immobilization (sling or figure-of-eight brace) for 3-6 weeks. Success rates of non-operative management are high for primary anterior dislocations. |
| Acute Posterior Dislocation | ALL posterior dislocations, especially irreducible ones, and those with signs of mediastinal compromise (dyspnea, dysphagia, vascular compromise). Often requires urgent open reduction with vascular/thoracic surgery standby. | None, as these are considered orthopedic emergencies. Closed reduction should always be attempted first, but even successful closed reduction often warrants surgical stabilization to prevent recurrence and protect vital structures. |
| Chronic Anterior Instability | Persistent symptomatic instability (pain, clicking, subjective instability) significantly impacting activities of daily living or athletic performance, after failed extensive conservative management (physical therapy, bracing, activity modification). | Initial management: Activity modification, physical therapy focusing on periscapular and rotator cuff strengthening, bracing. Avoidance of provocative activities. Analgesics and anti-inflammatory medications. |
| Chronic Posterior Instability | Persistent symptomatic instability affecting function or causing pain, particularly if there is a recurrent risk to mediastinal structures. Often requires ligamentous reconstruction. | Rarely non-operative, given the inherent risk and significant functional impairment. May be considered in extremely low-demand patients with minimal symptoms, but with caution. |
| Degenerative Osteoarthritis | Persistent, severe pain refractory to extensive non-operative treatment (NSAIDs, corticosteroid injections, physical therapy, activity modification) significantly impairing function. Symptomatic osteophyte formation. | First-line treatment: Activity modification, NSAIDs, corticosteroid injections (guided if possible), physical therapy. Weight loss (if applicable). |
| Medial Clavicle Fractures | Displaced fractures leading to significant deformity, skin tenting, neurovascular compromise, or irreducible fractures. Open fractures. Unstable fractures with significant displacement or comminution. | Non-displaced or minimally displaced fractures that are stable. Immobilization in a sling or figure-of-eight brace for 4-8 weeks, followed by progressive rehabilitation. |
| Infection (Septic Arthritis) | Failure of intravenous antibiotics to control infection, presence of abscess, persistent pain, joint destruction. Surgical debridement and washout are typically required. | Early, localized infection responsive to targeted intravenous antibiotic therapy, without significant joint destruction or abscess formation. |
| Tumors | Symptomatic benign tumors unresponsive to conservative management. Malignant tumors requiring oncologic resection with clear margins, often necessitating reconstruction. | Asymptomatic benign tumors that are stable over time and not causing functional impairment or cosmetic concerns. |
| Other Conditions | Post-traumatic osteolysis of the medial clavicle if highly symptomatic and refractory to conservative care (resection arthroplasty). Chronic inflammatory arthropathies with severe joint destruction and persistent pain despite medical management. | Most inflammatory arthropathies are primarily managed medically. Post-traumatic osteolysis may initially be managed with activity modification, NSAIDs. |
General Contraindications
- Absolute: Active infection (local or systemic), severe medical comorbidities precluding safe anesthesia and surgery, patient refusal.
- Relative: Poor soft tissue envelope, severe osteoporosis (may limit fixation options), smoking (impairs healing), uncontrolled diabetes.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical for optimizing outcomes and mitigating risks in SC joint surgery, particularly given the complex anatomy and proximity to vital structures.
Imaging Modalities
- Plain Radiographs: Anteroposterior (AP) and oblique views are standard. The "serendipity view" (40-degree cephalic tilt) is especially useful for evaluating vertical displacement of the medial clavicle relative to the sternum.
- Computed Tomography (CT) Scan: The gold standard for assessing SC joint pathology, particularly for dislocations and fractures. A CT scan with intravenous contrast provides detailed osseous anatomy, confirms the direction of dislocation (anterior vs. posterior), evaluates the integrity of the articular surfaces, and is crucial for identifying any impingement or damage to posterior mediastinal structures (e.g., vascular compromise, tracheal deviation). Three-dimensional reconstructions are invaluable for surgical planning.
- Magnetic Resonance Imaging (MRI): Useful for evaluating soft tissue injuries (ligamentous tears, meniscal pathology, capsular integrity), bone marrow edema, and inflammatory changes. Less crucial for acute dislocations unless soft tissue injury is suspected as the primary pathology or contributing factor to chronic instability.
- Vascular Studies (e.g., CT angiography): Mandatory for suspected posterior dislocations, especially if there is any clinical suspicion of vascular compromise or if the CT scan demonstrates close proximity to great vessels.
Preoperative Consultations
For posterior SC joint dislocations, or any case with suspected mediastinal involvement, a multidisciplinary approach is essential.
* Thoracic Surgery/Vascular Surgery: Mandated for posterior dislocations to manage potential great vessel injury, pneumothorax, or tracheal/esophageal compromise. Their presence during reduction, especially open reduction, is often necessary.
* Anesthesiology: Thorough evaluation, including assessment of airway patency, especially in cases of tracheal compression. Arterial line placement may be indicated.
* Interventional Radiology: May be consulted for preoperative embolization in rare cases of severe vascular injury.
Patient Positioning and Setup
- General Anesthesia: Typically required. Regional nerve blocks are generally not used as primary anesthesia due to the proximity of the SC joint to the neck and chest, but may be used postoperatively for pain control.
- Positioning: The patient is placed supine on the operating table. A rolled towel or beanbag placed longitudinally between the scapulae can help extend the thoracic spine and retract the shoulders, making the SC joint more prominent and facilitating posterior access if needed.
- Arm Draping: The ipsilateral arm should be draped free to allow for intraoperative manipulation (traction, adduction, abduction, rotation) to aid in reduction and assessment of stability.
- Imaging Access: Ensure unrestricted access for a C-arm fluoroscope to obtain intraoperative anteroposterior and serendipity views, which are critical for confirming reduction and hardware placement.
- Sterile Field: Broad sterile prep and drape from the mandible to the umbilicus and mid-axillary line, allowing for potential extension of the incision or emergent thoracotomy if mediastinal injury occurs.
- Vascular Access: Large-bore intravenous access is crucial for potential blood transfusion in emergency scenarios.
- Surgical Team: Ensure vascular or thoracic surgeons are immediately available or present in the operating room for high-risk posterior dislocations.
Detailed Surgical Approach and Technique
Surgical intervention for SC joint disorders encompasses a variety of techniques tailored to the specific pathology, including closed reduction, open reduction and internal fixation (ORIF), ligament reconstruction, and resection arthroplasty.
Incision and Exposure
- Incision: A transverse incision directly over the SC joint, approximately 5-7 cm in length, is generally preferred for cosmetic reasons and extensibility. Alternatively, an oblique incision along Langer's lines can be used. For extensive reconstruction or complex cases, a vertical incision over the medial clavicle and sternum may provide broader exposure.
- Dissection: The incision is carried through the skin and subcutaneous tissue. The platysma muscle is identified and carefully divided in line with the incision. Supraclavicular nerves should be identified and protected to avoid sensory deficits. The anterior sternoclavicular ligament and joint capsule are exposed. For anterior approaches, care must be taken to stay strictly anterior to avoid damaging the posterior structures.
Reduction Techniques
Acute Anterior Dislocation
- Closed Reduction: Often attempted first. The patient is supine with a bolster between the scapulae. Axial traction is applied to the ipsilateral arm, which is abducted to 90 degrees and extended. Direct posterior pressure is applied to the medial clavicle to reduce the anterior displacement.
- Open Reduction: If closed reduction fails or for open dislocations, the joint is exposed. The anterior capsule and ligaments are incised or elevated. The clavicle is manipulated to restore anatomical alignment.
Acute Posterior Dislocation
This is an orthopedic emergency requiring immediate attention and frequently, open reduction.
1. Closed Reduction:
* Patient positioned supine with a bolster between the scapulae.
* Axial traction on the abducted and extended arm.
* A sterile towel clip or a grasping forceps is often used to grasp the medial clavicle directly and lift it anteriorly.
* Some techniques advocate for placing a hand or fingers in the supraclavicular fossa to apply direct anterior pressure to the clavicle, while applying traction and adduction to the arm.
* The head of the table may be lowered (Trendelenburg position) to increase intrathoracic pressure, which can help in anterior translation.
* Concurrently, a vascular or thoracic surgeon should be prepared for emergent intervention if signs of mediastinal compromise worsen.
2. Open Reduction:
* If closed reduction fails or is contraindicated.
* A transverse or oblique incision. Dissection carefully proceeds to identify and protect vital structures.
* The posterior capsule and ligaments are often torn or avulsed.
* The medial clavicle is grasped and carefully reduced into its anatomical position, often requiring gentle traction and elevation.
* Vascular/thoracic surgeon present and prepared for direct visualization and repair of any injured mediastinal structures.
Stabilization Techniques
Once reduced, stability must be achieved to prevent recurrence.
Ligament Repair and Reconstruction
- Acute Instability (Anterior or Posterior): Direct repair of the torn anterior or posterior sternoclavicular ligaments and capsule is performed using strong non-absorbable sutures. The costoclavicular ligament, if injured, may also be repaired.
- Chronic Instability (Anterior or Posterior): For chronic dislocations, direct repair is often not feasible due to tissue attenuation. Ligamentous reconstruction is typically indicated.
- Graft Options: Autografts (e.g., palmaris longus, semitendinosus, gracilis) or allografts (e.g., semitendinosus, tibialis anterior). Autografts avoid disease transmission risks but require a donor site.
- Technique (Figure-of-Eight): A common technique involves drilling tunnels through the medial clavicle and the manubrium (or first rib) to create an anatomical or isometric reconstruction.
- Two drill holes are made obliquely through the medial clavicle, approximately 1-2 cm from the articular surface.
- Two corresponding drill holes are made through the sternal manubrium or the sternal end of the first rib, ensuring careful control of drill depth to avoid mediastinal penetration.
- The graft is passed in a figure-of-eight fashion through these tunnels, recreating the stabilizing function of the torn ligaments (e.g., anterior and posterior sternoclavicular ligaments or costoclavicular ligament).
- The graft is then tensioned with the shoulder in a neutral position (or slight retraction for posterior instability) and secured with sutures or interference screws.
- Modified Loop Reconstruction (e.g., Rockwood technique): Involves passing a graft or strong suture around the medial clavicle and through drill holes in the manubrium and first rib, creating a broad sling effect.
- Tension Band Wiring/Sutures: Rarely used alone but may supplement graft reconstruction.
Internal Fixation (Adjunctive)
- Suture Anchor Fixation: Suture anchors can be used to reattach avulsed ligaments to bone, particularly useful for avulsions from the sternum.
- K-wires/Pins: Historically used for temporary stabilization, but largely discouraged due to the high risk of migration into the mediastinum (e.g., pulmonary artery, aorta, heart), particularly with movement. If used, they must be bent, capped, and removed early.
- Plates and Screws: Occasionally used for specific medial clavicle fractures involving the SC joint, but challenging due to small bone fragments and limited purchase. Contourable mini-plates or specialized clavicular plates may be employed.
- Suture Augmentation: High-strength sutures (e.g., FiberWire) can be used to augment repairs or reconstructions, especially for acute repairs.

Illustrative diagram depicting a common sternoclavicular joint reconstruction technique using a graft passed through drill holes in the medial clavicle and sternum.
Resection Arthroplasty
- Indications: Primarily for symptomatic degenerative osteoarthritis, post-traumatic osteolysis of the medial clavicle, or chronic septic arthritis unresponsive to debridement, where pain persists despite conservative measures.
- Technique: A small segment (typically 1-2 cm) of the medial clavicle is resected to create a pseudoarthrosis, thereby relieving impingement and pain. Care must be taken to preserve the costoclavicular ligament if possible, or reconstruct it, to maintain adequate shoulder stability.
- Interposition Arthroplasty: Some surgeons advocate for interposing soft tissue (e.g., local muscle flap, fascia lata autograft, synthetic material) into the resection space to prevent bone-on-bone articulation and promote a pain-free pseudoarthrosis.

Pre-operative image of a sternoclavicular joint disorder, likely an anterior subluxation or dislocation, prior to surgical planning.
Medial Clavicle Fractures
- ORIF: For significantly displaced, unstable, or open medial clavicle fractures involving the SC joint.
- Plating: Small fragment plates or specialized clavicle plates can be used if adequate bone stock allows for stable screw fixation. This can be challenging due due to the short segment of the medial clavicle.
- Tension Band Wiring/Cerclage: May be employed for comminuted fractures where plate fixation is difficult, or as an adjunct.
- Intramedullary Nailing: Less commonly used but may be considered in specific fracture patterns.
Wound Closure
After achieving satisfactory reduction and stabilization, the wound is irrigated, and hemostasis is ensured. The platysma and subcutaneous tissues are closed meticulously. The skin is closed with absorbable sutures or staples. A sterile dressing is applied, and the arm is immobilized as per postoperative protocol.
Complications and Management
Complications associated with SC joint surgery can range from minor to life-threatening, reflecting the anatomical complexity and the nature of the pathologies treated. Vigilant attention to detail during preoperative planning, surgical execution, and postoperative care is paramount for minimizing these risks.
| Complication | Incidence (Approximate) | Salvage Strategy/Management |
|---|---|---|
| Intraoperative Neurovascular Injury | Rare, but significantly higher (up to 25-30%) with posterior dislocations, especially during closed reduction attempts or uncontrolled open reduction. Injuries to subclavian vessels, brachiocephalic vessels, vagus/phrenic nerves. | Immediate recognition is critical. Vascular surgeon must be on standby for posterior dislocations. Direct repair of injured vessels. Nerve repair if feasible, though prognosis is guarded. Emergent thoracotomy/sternotomy may be required. |
| Tracheal/Esophageal Injury | Rare, primarily with posterior dislocations (0.5-5%). | Immediate consultation with thoracic/ENT surgeon. Primary repair if identified intraoperatively. Postoperative management includes antibiotics, nutritional support, and close monitoring for mediastinitis. |
| Pneumothorax | Rare (1-2%), mainly associated with posterior dislocations or aggressive deep dissection. | Chest tube insertion. Close monitoring for respiratory distress. |
| Hardware Migration | Up to 25% with K-wires; significantly lower with modern suture/graft fixation. K-wire migration into mediastinum is a known, severe risk. | K-wire migration necessitates immediate removal, often requiring cardiothoracic surgery. For other hardware (screws, plates), if symptomatic or unstable, removal may be indicated. Redo fixation with alternative techniques may be necessary. Strict avoidance of K-wires in favor of safer fixation methods (suture, graft reconstruction) is paramount. |
| Infection (Superficial/Deep) | 1-5% (similar to other orthopedic procedures); higher in open fractures or with prolonged procedures. | Superficial infections: Oral antibiotics, local wound care. Deep infections: Surgical debridement and irrigation, intravenous antibiotics (culture-directed). Hardware removal may be necessary if infection persists or involves the implant. |
| Persistent Instability/Recurrence | 5-15% (variable depending on technique and pathology; higher for chronic cases or inadequate primary stabilization). | Thorough investigation (CT/MRI) to determine cause (graft failure, inadequate tension, persistent ligamentous laxity). Revision surgery: Often involves a more robust reconstruction technique, potentially with different graft material or fixation methods. May require re-evaluation of patient-specific biomechanics. |
| Stiffness/Reduced Range of Motion | Common (10-20%) post-operatively, especially with prolonged immobilization. | Aggressive, structured physical therapy focusing on early controlled motion, stretching, and mobilization. Manipulation under anesthesia or even arthroscopic capsular release may be considered in refractory cases, though rare for SC joint. |
| Nonunion/Pseudoarthrosis | Primarily relevant for medial clavicle fractures or after resection arthroplasty (if symptomatic). Rare otherwise. | Medial clavicle fractures: Revision ORIF with bone grafting. Symptomatic pseudoarthrosis after resection: May require further debridement or interposition material. |
| Post-Traumatic Osteolysis | Rare, typically seen after acute trauma or chronic stress (e.g., weightlifting). Can cause pain and swelling. | Initial: Conservative (NSAIDs, activity modification, steroid injections). Persistent symptoms: Resection arthroplasty of the medial clavicle. |
| Complex Regional Pain Syndrome (CRPS) | Rare (up to 5%). | Multidisciplinary approach: Aggressive physical therapy, pain management (nerve blocks, neuromodulation, pharmacotherapy), psychological support. Early diagnosis and intervention are key. |
| Cosmetic Deformity/Scarring | Inherent risk of any surgical incision. More pronounced with larger incisions or keloid formers. | Meticulous wound closure, patient education on scar care. Revision scar excision in severe cases after adequate healing. |
General Management Principles for Complications
- Prevention: Meticulous surgical technique, proper patient selection, use of appropriate and safe fixation methods, and intraoperative imaging. For posterior dislocations, vascular and thoracic surgical standby is a critical preventative measure for severe complications.
- Early Recognition: High index of suspicion for developing complications. Close postoperative monitoring, particularly for vital signs, respiratory status, and neurovascular checks.
- Timely Intervention: Prompt and appropriate management, ranging from antibiotics for infection to emergent re-operation for severe issues like vascular injury or hardware migration.
- Multidisciplinary Approach: Collaboration with other specialties (e.g., vascular, thoracic, infectious disease, pain management) is often essential for complex complications.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is crucial for optimizing functional outcomes, restoring range of motion, and preventing recurrence of instability. Protocols vary based on the specific surgical procedure, quality of repair/reconstruction, and surgeon preference, but generally follow a phased approach.
General Principles
- Protection: Initial phase focuses on protecting the surgical repair/reconstruction, minimizing stress on healing tissues.
- Gradual Progression: Exercise intensity and range of motion are gradually increased as healing progresses.
- Pain Management: Effective pain control is essential to facilitate participation in rehabilitation.
- Patient Education: Comprehensive education on activity restrictions, home exercise programs, and warning signs is critical.
Phase I: Protection and Early Motion (0-4 or 0-6 Weeks Post-Op)
- Goals: Protect the surgical repair, minimize pain and swelling, prevent shoulder stiffness, promote wound healing.
- Immobilization: Sling or shoulder immobilizer is typically worn continuously, removing only for hygiene and specified exercises. Duration varies:
- Acute repair of ligaments/capsule: 3-4 weeks.
- Ligament reconstruction (graft): 4-6 weeks (some protocols extend to 8 weeks for chronic instability).
- Resection arthroplasty: 2-3 weeks (primarily for comfort).
- Restrictions:
- No active range of motion (AROM) of the ipsilateral shoulder, especially movements that stress the SC joint (e.g., extreme abduction, external rotation, pushing/pulling).
- No weight-bearing on the affected arm.
- No lifting objects.
- Exercises (Passive and Pendulum):
- Passive Range of Motion (PROM): Gentle, pain-free PROM of the glenohumeral joint (flexion to 90-120 degrees, external rotation to 0-30 degrees) performed by a therapist or with the unaffected arm.
- Pendulum Exercises: Gentle circular motions of the arm with the body bent forward, using gravity for motion.
- Elbow, Wrist, Hand Exercises: AROM to prevent stiffness.
- Scapular Retractions: Gentle isometric scapular squeezes (while in sling).
- Cryotherapy: Application of ice to reduce pain and swelling.
Phase II: Controlled Motion and Early Strengthening (4-12 Weeks Post-Op)
- Goals: Restore full pain-free passive and active range of motion, initiate gentle strengthening, improve neuromuscular control.
- Immobilization: Discontinue sling/immobilizer as tolerated, typically around 4-6 weeks.
- Restrictions: Continue to avoid heavy lifting, pushing, pulling, or sudden, forceful movements. Avoid contact sports.
- Exercises:
- Active-Assisted Range of Motion (AAROM): Progress from PROM to AAROM, then to AROM, gradually increasing range as pain allows.
- Isometric Strengthening: Initiate gentle isometric exercises for rotator cuff (internal/external rotation), deltoid, and scapular stabilizers.
- Light Resistance Training: Progress to light resistance with elastic bands for rotator cuff and periscapular muscles (e.g., rows, external rotation).
- Proprioceptive Exercises: Wall slides, rhythmic stabilization drills.
- Posture Correction: Emphasis on maintaining upright posture and shoulder retraction.
Phase III: Progressive Strengthening and Advanced Activity (12-24 Weeks Post-Op)
- Goals: Achieve full strength and endurance, restore sport-specific or activity-specific function, prepare for return to full activity.
- Restrictions: Gradual reintroduction of heavier lifting. Contact sports and overhead activities are still generally restricted until 6 months or later.
- Exercises:
- Progressive Resistance Training: Increase resistance and intensity for all shoulder and scapular musculature. Focus on functional movements.
- Core Strengthening: Integrate core stability exercises to support overall movement.
- Endurance Training: Light cardiovascular exercise.
- Plyometrics/Sport-Specific Drills: For athletes, initiate controlled plyometric exercises and sport-specific movements as appropriate.
- Overhead Activities: Gradually introduce controlled overhead movements and activities, ensuring no pain or instability.
Phase IV: Return to Activity (6-12 Months Post-Op)
- Goals: Full, unrestricted return to all activities, including contact sports and overhead athletics.
- Criteria for Return:
- Full, pain-free range of motion.
- Strength symmetrical to the contralateral side (or >90%).
- Absence of pain or instability during functional or sport-specific movements.
- Subjective confidence in the shoulder.
- Gradual Return: Even after meeting criteria, a gradual return to high-impact or contact activities is recommended to allow for adaptation and minimize risk of re-injury. For collision athletes, full return is often delayed until 9-12 months post-reconstruction.
Special Considerations
- Resection Arthroplasty: Rehabilitation is typically accelerated, focusing on early range of motion to prevent adhesions and achieve pain-free pseudoarthrosis.
- Adolescents: Special attention to growth plates. Rehabilitation may be more conservative in the initial phases.
Summary of Key Literature and Guidelines
The literature concerning SC joint disorders, while less extensive than for other major joints, provides a framework for evidence-based management. Key themes include the emphasis on anatomical reduction for posterior dislocations, the evolution of reconstruction techniques for chronic instability, and the recognition of non-operative efficacy for many anterior dislocations.
Diagnosis and Initial Management
- Imaging: Consensus unequivocally highlights the CT scan as the definitive diagnostic tool for SC joint dislocations and fractures. Its superior resolution for osseous detail and ability to assess mediastinal compromise are unmatched by plain radiographs. MRI is reserved for soft tissue assessment, particularly for chronic instability or inflammatory conditions (Brennan et al., 2011; Rockwood et al., 2017).
- Posterior Dislocations: Universal agreement on the urgent nature of posterior dislocations. Early closed reduction attempts are recommended, ideally under general anesthesia with immediate surgical standby due to the high risk of mediastinal complications (Netto et al., 2008; Spencer et al., 2007). Failed closed reduction necessitates immediate open reduction.
Surgical Techniques for Instability
- Ligamentous Reconstruction: For chronic instability, various techniques using autograft (semitendinosus, gracilis, palmaris longus) or allograft are described. The figure-of-eight reconstruction through clavicular and sternal/first rib tunnels, often attributed to Rockwood, remains a widely accepted and biomechanically sound approach for both anterior and posterior chronic instability (Rockwood et al., 2017; Booth & Roper, 1979). Comparative studies, while limited, suggest comparable outcomes between autograft and allograft in terms of stability, though autograft avoids donor site morbidity (Frank et al., 2013).
- Fixation Methods: The use of K-wires for internal fixation is strongly discouraged due to the unacceptably high risk of mediastinal migration and life-threatening complications (Sewell et al., 2004; Thobani et al., 2011). Modern consensus favors robust suture-based fixation, high-strength suture augmentation, or interference screws for graft fixation. Biodegradable implants have shown promise but require further long-term data.
- Medial Clavicle Resection Arthroplasty: For symptomatic degenerative arthritis or post-traumatic osteolysis, medial clavicle resection has demonstrated good to excellent results in relieving pain (Simovitch et al., 2009). The extent of resection (typically 1-2 cm) is critical, along with preservation or reconstruction of the costoclavicular ligament to maintain stability. Interpositional material remains a surgeon preference, with no clear superior option in the literature.
Outcomes and Complications
- Outcomes: Generally favorable for acute anterior dislocations managed non-operatively. Surgical outcomes for chronic instability, particularly with modern reconstruction techniques, report good to excellent functional results in 70-90% of cases (Thobani et al., 2011; Spencer et al., 2007).
- Complications: Persistent pain, stiffness, and recurrent instability are the most common post-surgical complications. The critical importance of preventing mediastinal injury during posterior dislocation reduction and avoiding K-wire fixation is a consistent message across the literature (Sewell et al., 2004; Rockwood et al., 2017).
Rehabilitation Guidelines
- Literature emphasizes phased rehabilitation protocols tailored to the surgical procedure, with initial protection followed by gradual increases in range of motion and strength. Prolonged immobilization (4-6 weeks) for ligament reconstructions is generally recommended to allow for graft healing and integration (Thobani et al., 2011). Return to high-impact or overhead activities is typically delayed for 6-12 months.
Emerging Concepts and Future Directions
Research continues to refine surgical techniques, particularly in understanding the optimal biomechanics of reconstruction. Areas of ongoing interest include:
* Biomechanical studies comparing different graft materials and fixation techniques.
* Long-term outcomes of modern reconstruction techniques, especially for chronic instability.
* The role of arthroscopy in SC joint disorders for diagnosis, debridement, and potentially assisted reduction or reconstruction, though currently limited due to technical challenges and proximity to vital structures.
* Development of patient-reported outcome measures specifically validated for SC joint pathology.
In conclusion, management of SC joint disorders necessitates a detailed understanding of the complex anatomy, a high index of suspicion for severe injuries (especially posterior dislocations), and a systematic approach to diagnosis and treatment. While conservative management remains the cornerstone for many anterior dislocations and early degenerative changes, surgical intervention offers effective relief for refractory pain, instability, and life-threatening conditions, with an ongoing evolution of safe and efficacious techniques.
Clinical & Radiographic Imaging

You Might Also Like