Medial Clavicle Resection for Chronic Sternoclavicular Joint Dislocation
Key Takeaway
Chronic sternoclavicular joint dislocations, particularly posterior variants, can cause significant mediastinal compression. When open reduction is unstable or unachievable, resection of the medial end of the clavicle provides a safe, definitive solution. This procedure relieves compressive symptoms such as dysphagia and dyspnea while preserving shoulder girdle function. Meticulous subperiosteal dissection and, when necessary, stabilization to the first rib ensure optimal biomechanical and cosmetic outcomes.
INTRODUCTION TO CHRONIC STERNOCLAVICULAR JOINT DISLOCATIONS
Dislocations of the sternoclavicular (SC) joint are relatively uncommon injuries, representing less than 3% of all shoulder girdle traumas. While anterior dislocations are the most frequently encountered, posterior dislocations—though rare—carry a disproportionately high risk of morbidity due to the immediate proximity of critical mediastinal structures.
In the acute setting, closed or open reduction is often attempted. However, when these injuries are neglected, misdiagnosed, or fail to maintain reduction, they evolve into chronic, old dislocations. Chronic anterior dislocations are often well-tolerated functionally but may present with unacceptable cosmetic deformity or localized pain. Conversely, chronic posterior dislocations are frequently symptomatic, exerting dangerous pressure on the trachea, esophagus, and great vessels.
When chronic SC joint dislocations become symptomatic, and delayed open reduction is deemed either impossible or inherently unstable, resection of the medial end of the clavicle is the gold standard surgical intervention. This procedure effectively decompresses the thoracic outlet and mediastinum, alleviates pain, and restores shoulder girdle kinematics with minimal functional deficit.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of SC joint anatomy is mandatory before undertaking medial clavicle resection, given the catastrophic potential of iatrogenic injury in this region.
The Sternoclavicular Articulation
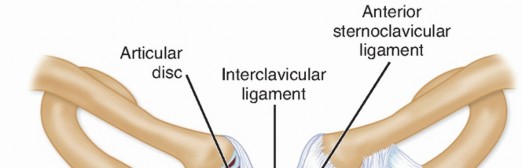
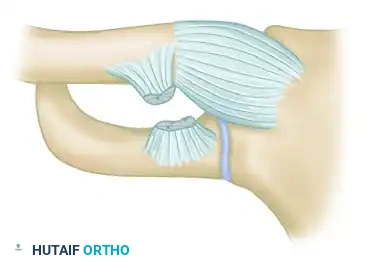
The SC joint is a diarthrodial saddle joint and represents the sole true synovial articulation between the axial skeleton and the upper extremity. The articular surface of the medial clavicle is disproportionately larger than the shallow clavicular notch of the manubrium, rendering the joint inherently unstable from a purely osseous standpoint. Stability is therefore entirely dependent on the surrounding ligamentous complex.
Ligamentous Stabilizers
- Capsular Ligaments: The anterior and posterior SC ligaments represent thickenings of the joint capsule. The posterior SC ligament is the most robust stabilizer against both anterior and posterior translation.
- Intra-articular Disc Ligament: A dense fibrocartilaginous meniscus that divides the joint into two separate synovial cavities, acting as a shock absorber and a tether against medial displacement.
- Costoclavicular (Rhomboid) Ligament: A dense, bipartite ligament connecting the inferior aspect of the medial clavicle to the first rib and its costal cartilage. It is the primary restraint to superior displacement and plays a critical role in overall shoulder girdle stability.
- Interclavicular Ligament: Connects the superomedial aspects of both clavicles across the jugular notch.
The Retrosternal "Danger Zone"
The posterior aspect of the SC joint lies in perilous proximity to vital anatomical structures.
* Vascular: The brachiocephalic (innominate) veins, superior vena cava, aortic arch, and subclavian arteries.
* Visceral: The trachea and esophagus.
* Neurological: The vagus and phrenic nerves, and the recurrent laryngeal nerve.
Surgical Warning: The brachiocephalic vein lies mere millimeters posterior to the medial clavicle and posterior SC capsule. Meticulous, strictly subperiosteal dissection is the only reliable method to protect these structures during resection.
CLINICAL PRESENTATION AND INDICATIONS
Posterior Dislocations
Posterior dislocation of the SC joint in a chronic state is a highly concerning pathology. Patients frequently present with symptoms of mediastinal compression or thoracic outlet syndrome.
* Dysphagia: Due to esophageal compression.
* Dyspnea or Stridor: Due to tracheal compression.
* Venous Congestion or Claudication: Due to great vessel impingement.
* Neurological Deficits: Brachial plexus irritation or thoracic outlet syndrome.
In view of the severe potential complications associated with chronic posterior displacement, surgical intervention is strongly recommended.
Anterior Dislocations
Chronic anterior dislocations are typically benign regarding visceral compression. Indications for surgery in anterior variants are strictly limited to:
* Intractable, localized pain that fails conservative management.
* Severe cosmetic deformity that is unacceptable to the patient.
* Symptomatic degenerative joint disease (post-traumatic osteoarthritis) secondary to the chronic dislocation.
PREOPERATIVE EVALUATION AND PLANNING
Imaging Modalities
Standard orthogonal radiographs (including the serendipity view) are often insufficient for detailed preoperative planning in chronic SC dislocations.
* Computed Tomography (CT): A high-resolution CT scan of the upper thorax and shoulder girdle is mandatory. It precisely defines the direction of the dislocation, the presence of degenerative changes, and the exact distance between the displaced medial clavicle and the mediastinal structures.
* CT Angiography (CTA) / Arteriography: If vascular compromise is suspected clinically, or if the CT scan demonstrates the clavicle abutting the great vessels, a CTA is required to rule out pseudoaneurysm, thrombosis, or direct vessel adherence.
Multidisciplinary Approach
Clinical Pearl: Never undertake a medial clavicle resection for a chronic posterior dislocation without a cardiothoracic or vascular surgeon available on standby. The risk of catastrophic hemorrhage from the brachiocephalic vein or subclavian artery, while rare, requires immediate sternotomy capabilities.
SURGICAL TECHNIQUE: MEDIAL CLAVICLE RESECTION
Patient Positioning and Anesthesia
- Anesthesia: General endotracheal anesthesia is required. The endotracheal tube should be secured away from the operative field.
- Positioning: The patient is placed in the beach-chair or supine position with a bump between the scapulae to allow the shoulders to fall posteriorly, opening the SC joint anteriorly.
- Preparation: The surgical prep must include the entire shoulder girdle, the anterior chest down to the costal margin, and the contralateral sternum to allow for a median sternotomy if an emergency vascular injury occurs.
Incision and Exposure
- Make a transverse incision approximately 6 cm in length, centered over the medial end of the clavicle and running parallel to the longitudinal axis of the bone.
- Dissect through the subcutaneous tissue and platysma to expose the investing fascia of the clavicle.
- Identify the clavicular head of the sternocleidomastoid (SCM) muscle superiorly and the pectoralis major inferiorly.
- Incise the periosteum longitudinally along the anterior midline of the medial clavicle.
- Subperiosteal Dissection: Using a sharp Cobb elevator or periosteal elevator, meticulously expose the medial end of the clavicle subperiosteally.
Surgical Warning: The subperiosteal envelope must be maintained, particularly along the posterior cortex. The periosteum acts as the primary physical barrier protecting the retrosternal great vessels.
Mobilization of the Medial Clavicle
- Free the medial end of the bone circumferentially within its periosteal sleeve.
- Grasp the medial clavicle with a heavy bone-holding forceps (e.g., a Lewin clamp) and lift it anteriorly and superiorly.
- Carefully clear the bone of any remaining soft tissue attachments posteriorly using blunt dissection or a periosteal elevator.
- Assess the status of the costoclavicular (rhomboid) ligaments. In chronic dislocations, these ligaments are usually torn, attenuated, or scarred.
Osteotomy and Resection
The extent of the resection is dictated by the integrity of the costoclavicular ligaments.
- Scenario A (Ligaments Intact but Stretched): If the costoclavicular ligaments are still attached to the clavicle but stretched, resect only that part of the clavicle that lies medial to these ligaments. Preserving the ligamentous insertion maintains the intrinsic stability of the remaining clavicle.
- Scenario B (Ligaments Torn): If the ligaments are completely torn or non-functional, resect approximately 2 cm of the medial bone.
FIGURE 61-4A: Technique for resecting the medial end of the clavicle. The site of the osteotomy is carefully outlined with a drill to prevent splintering, and approximately 2 to 2.5 cm of bone is then resected using a sharp osteotome or oscillating saw.
- Cosmetic Beveling: Once the primary resection is complete, use a rongeur or a high-speed burr to bevel the anterosuperior corner of the remaining medial clavicle. This prevents a sharp, unsightly bony prominence under the skin, which is a common source of postoperative patient dissatisfaction.
Periosteal Plication and Closure
If the remaining clavicle is stable within its bed, meticulous closure of the periosteal sleeve is performed.
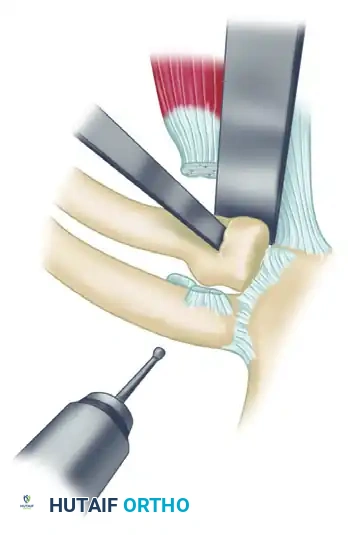
FIGURE 61-4B: The empty periosteal sleeve is plicated and closed securely around the remaining medial end of the clavicle. This robust closure acts as a biologic tether, preventing superior or anterior migration of the clavicular stump.
Management of Instability and First Rib Stabilization
Following resection, the surgeon must dynamically assess the stability of the remaining clavicular stump. If the costoclavicular ligaments were resected or incompetent, the clavicle may exhibit severe multidirectional instability, particularly superior migration due to the unopposed pull of the SCM and trapezius muscles.
If instability is a problem, the clavicle must be surgically stabilized to the first rib.
- Preparation of the First Rib: Carefully expose the anterior aspect of the first rib, remaining strictly subperiosteal to avoid injury to the subclavian vein, which crosses the first rib laterally.
- Graft Selection: Stabilization can be achieved using a 3-mm cotton Dacron tape, a robust strip of autologous fascia lata, or an allograft tendon (e.g., semitendinosus).
- Passage of the Graft: Pass the graft or tape around the first rib and through drill holes created in the medial stump of the clavicle.
- Fixation: Tie the graft or tape securely while holding the clavicle in an anatomically reduced, depressed position.
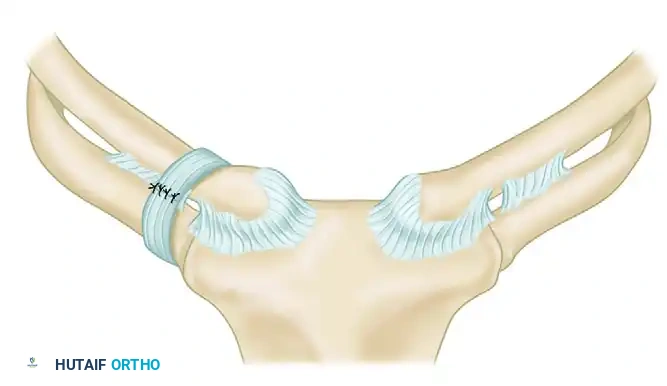
FIGURE 61-5: Stabilization of the unstable medial clavicle to the first rib utilizing robust fascial loops. This figure-of-eight or cerclage technique effectively substitutes for the deficient costoclavicular ligaments.
- Muscle Detachment: To further reduce deforming forces on the newly stabilized clavicle, detach the clavicular head of the sternocleidomastoid muscle from its insertion.
- Final Closure: Plicate and close the periosteum over the reconstruction. Close the platysma and skin in standard layered fashion.
POSTOPERATIVE CARE AND REHABILITATION
The success of a medial clavicle resection, particularly when soft tissue stabilization to the first rib is performed, relies heavily on strict adherence to postoperative protocols.
Phase I: Maximum Protection (Weeks 0-3)
- Immobilization: The affected shoulder girdle is strictly immobilized in a Velpeau-type dressing or a commercial shoulder immobilizer for 3 weeks.
- Restrictions: No active range of motion (ROM) of the shoulder. No lifting, pushing, or pulling.
- Permitted Activities: Active ROM of the elbow, wrist, and hand is encouraged to prevent distal stiffness. Pendulum exercises may be initiated at the surgeon's discretion toward the end of this phase.
Phase II: Progressive Range of Motion (Weeks 4-8)
- Mobilization: The immobilizer is discontinued.
- Exercises: A progressive active and active-assisted ROM exercise program is begun. Focus is placed on restoring forward elevation and external rotation.
- Scapular Mechanics: Scapular retraction and stabilization exercises are initiated to ensure proper shoulder girdle kinematics and prevent impingement of the medial clavicular stump.
Phase III: Strengthening and Return to Function (Weeks 8-12+)
- Strengthening: Isotonic strengthening of the deltoid, rotator cuff, and periscapular musculature is introduced.
- Return to Play/Work: Patients can typically return to heavy labor or contact sports between 3 to 4 months postoperatively, provided they have achieved full, painless ROM and symmetric strength.
COMPLICATIONS AND PITFALLS
While medial clavicle resection is highly effective, surgeons must be vigilant regarding potential complications:
- Vascular Injury: The most feared complication. Strict adherence to subperiosteal dissection is the only preventative measure.
- Inadequate Resection: Resecting less than 1.5 cm may lead to recurrent impingement of the clavicular stump against the manubrium during shoulder protraction.
- Excessive Resection: Resecting more than 2.5 to 3 cm risks violating the coracoclavicular ligamentous complex distally, leading to catastrophic global shoulder girdle instability.
- Cosmetic Deformity: Failure to bevel the anterosuperior cortex will result in a visible and palpable subcutaneous spike.
- Recurrent Instability: Failure to recognize incompetence of the costoclavicular ligaments and omitting the first rib stabilization step will result in a highly symptomatic, superiorly migrating clavicular stump.
Except for a mild cosmetic defect (a visible depression at the base of the neck), no significant functional disability has been noted from this procedure when executed correctly. Patients consistently report high satisfaction rates, complete resolution of mediastinal compressive symptoms, and a return to baseline shoulder function.
You Might Also Like