Stop the Snap: Hip Preservation for Snapping Iliopsoas Tendon

Key Takeaway
This article provides essential research regarding Stop the Snap: Hip Preservation for Snapping Iliopsoas Tendon. Snapping iliopsoas tendon describes a condition where the iliopsoas tendon transiently subluxes from a lateral to medial position over structures like the pectineal eminence or anterior femoral head. This snapping sound or sensation typically occurs as the hip moves from a flexed, abducted, and externally rotated position into extension with internal rotation. It is present asymptomatically in at least 10% of people.
Introduction and Epidemiology
Coxa saltans, commonly referred to as snapping hip syndrome, represents a clinical entity characterized by an audible or palpable snapping sensation during movement of the hip joint. The term was popularized by Allen and subsequent co-authors to describe a phenomenon that is frequently asymptomatic but can become a source of debilitating groin or lateral hip pain. Historically, coxa saltans has been classified into three distinct categories based on the anatomical source of the mechanical snap.
The first is the internal type, which involves the iliopsoas tendon snapping over osseous prominences of the anterior pelvis or proximal femur. The second is the external type, characterized by the iliotibial band or gluteus maximus snapping over the greater trochanter. The third category, the intra-articular type, was originally attributed to diverse intra-articular pathology, including loose bodies, synovial chondromatosis, and labral tears. However, with the advent of high-resolution magnetic resonance arthrography and advanced hip arthroscopy, there is now significantly more accuracy in the description and diagnosis of intra-articular hip pathology. Consequently, intra-articular mechanical symptoms are now diagnosed specifically based on their primary pathology (e.g., femoroacetabular impingement, acetabular labral tear) and the term snapping hip is generally reserved for the extra-articular internal and external variants.




This comprehensive review focuses specifically on the internal type of coxa saltans—the snapping iliopsoas tendon. Internal snapping hip is predominantly observed in young, active populations. It is particularly prevalent in athletes whose disciplines require repetitive hip flexion, extension, and extreme ranges of motion, such as ballet dancers, gymnasts, martial artists, and soccer players. In the ballet community, the condition is so ubiquitous that it is colloquially referred to as "dancer's hip," with some epidemiological studies suggesting that up to 90% of professional dancers experience snapping, though a smaller percentage present with functionally limiting pain.
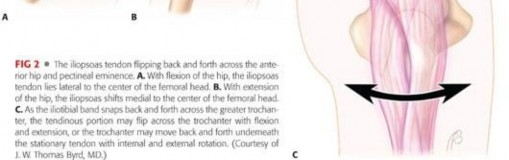
The pathophysiology of internal snapping hip is mechanical. As the hip transitions from a flexed, abducted, and externally rotated position into an extended, adducted, and internally rotated position, the iliopsoas tendon translates laterally. During this dynamic arc of motion, the tendon can catch and snap abruptly over the iliopectineal eminence, the anterior aspect of the femoral head, or the lesser trochanter. Repetitive friction leads to tenosynovitis, thickening of the tendon, and inflammation of the underlying iliopsoas bursa, culminating in pain and functional limitation. Furthermore, a tight iliopsoas tendon can exert excessive pressure on the anterior capsulolabral complex, leading to secondary anterior labral tears, a phenomenon frequently observed at the 3 o'clock position (anterior) on the acetabular clock face.





The clinical presentation typically involves a patient reporting a deep-seated groin pain associated with an audible clunk or snap. Unlike external snapping hip, which is often visible as the IT band subluxates over the greater trochanter, internal snapping hip is primarily palpable and audible. The pain is often exacerbated by activities requiring repetitive hip flexion, such as rising from a seated position, running, or performing high kicks. In chronic cases, the persistent mechanical irritation can lead to significant structural changes within the tendon itself, including mucoid degeneration and partial interstitial tearing, which further complicates the clinical picture and necessitates careful diagnostic evaluation.





Surgical Anatomy and Biomechanics
Musculotendinous Architecture
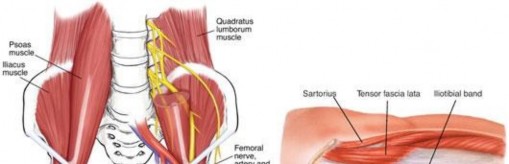
A profound understanding of the iliopsoas complex is mandatory for the orthopedic surgeon contemplating surgical intervention. The iliopsoas is a composite muscle formed by the confluence of the psoas major and the iliacus muscles. The psoas major originates from the transverse processes, intervertebral discs, and vertebral bodies of T12 through L5. It courses inferiorly through the pelvis, where it is joined by the iliacus muscle, which originates from the superior two-thirds of the iliac fossa, the inner lip of the iliac crest, and the anterior sacroiliac and iliolumbar ligaments.





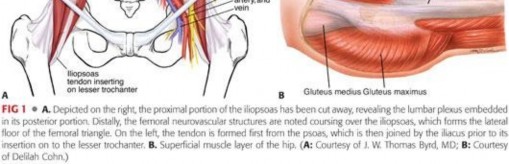
As these muscles traverse the pelvic brim, they pass over the iliopectineal eminence and the anterior capsule of the hip joint. The musculotendinous junction is highly variable. The psoas major typically becomes tendinous superior to the joint line, while the iliacus remains predominantly muscular, inserting directly into the lesser trochanter and the anterior surface of the psoas tendon. The distinct tendinous portion of the psoas major and the muscular portion of the iliacus are critical landmarks during arthroscopic release. Surgeons must recognize that the tendon lies posteromedial to the muscle belly at the level of the joint line.
Anatomical Variants and the Bifid Tendon
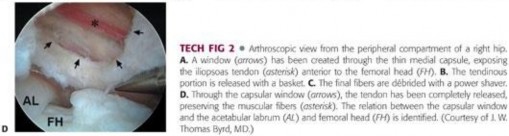
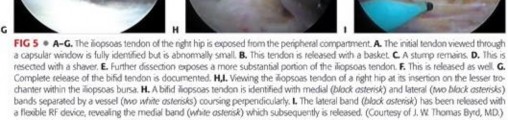
Recent anatomical studies have highlighted the frequent presence of multiple tendinous slips within the iliopsoas complex. A bifid or even trifid iliopsoas tendon is not an anomaly but rather a common anatomical variant, reported in up to 60% of cadaveric specimens. Failure to recognize and release all tendinous slips during surgery is a primary cause of recurrent snapping and surgical failure. The accessory slips often originate from the iliacus muscle and insert separately onto the lesser trochanter. Meticulous dissection and visualization of the entire anterior capsular interval are required to ensure complete release of the tendinous components while preserving the muscular elements.





Neurovascular Proximity
The proximity of critical neurovascular structures dictates the safety corridors for surgical approach. The femoral nerve lies immediately lateral to the psoas muscle belly, innervating the iliacus and providing sensory branches to the anterior thigh. The external iliac artery and vein, which transition into the femoral vessels at the inguinal ligament, lie medial to the iliopsoas complex. The iliopectineal fascia separates the muscle from these medial vascular structures. During transcapsular arthroscopic release, the surgeon operates from within the joint outward, utilizing the anterior capsule as a protective barrier. The release must be performed strictly at the tendinous portion, directing instruments away from the neurovascular bundle.





Biomechanical Considerations
Biomechanically, the iliopsoas is the most powerful flexor of the hip joint and a weak external rotator. It acts as a dynamic anterior stabilizer of the femoral head, particularly in positions of extension and external rotation. This stabilizing role is crucial in patients with underlying acetabular dysplasia or capsular laxity. In such patients, the iliopsoas may hypertrophy as a compensatory mechanism to prevent anterior subluxation of the femoral head. Consequently, releasing the iliopsoas tendon in a dysplastic hip can lead to catastrophic iatrogenic anterior instability, rapid chondrolysis, and failure of the joint.





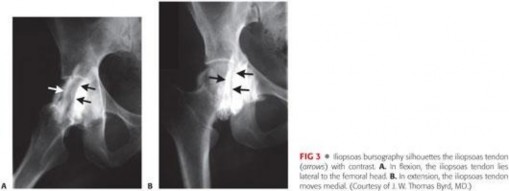
The mechanics of the snap itself are a product of the tendon's path over the anterior hemipelvis. In flexion, abduction, and external rotation (the FABER position), the tendon lies lateral to the center of the femoral head. As the hip is brought into extension, adduction, and internal rotation, the tendon abruptly translates medially across the iliopectineal eminence and the anterior femoral head. If the tendon is abnormally tight or the bursa is inflamed and thickened, this translation is no longer smooth, resulting in the characteristic mechanical "clunk."



Indications and Contraindications
The decision to proceed with surgical intervention for internal snapping hip must be made judiciously. The majority of patients respond favorably to a comprehensive non-operative regimen. Surgery is strictly reserved for recalcitrant cases that have failed exhaustive conservative measures and exhibit clear functional impairment.
Non Operative Management Strategy
Initial management should always consist of activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), and a targeted physical therapy protocol. Physical therapy must focus on stretching the iliopsoas complex, strengthening the core and pelvic stabilizers, and correcting any lumbopelvic biomechanical deficits. If symptoms persist after 6 to 12 weeks of physical therapy, an ultrasound-guided corticosteroid injection into the iliopsoas bursa is indicated. This serves both a therapeutic and diagnostic purpose. Complete, albeit temporary, relief of pain following the injection confirms the iliopsoas as the primary pain generator.




Surgical Indications
Surgical release of the iliopsoas tendon is indicated in patients who have failed a minimum of 3 to 6 months of dedicated non-operative management, including at least one ultrasound-guided corticosteroid injection. Furthermore, surgery is highly indicated when the snapping hip is accompanied by significant intra-articular pathology, such as femoroacetabular impingement (FAI) or an anterior labral tear. In the setting of FAI, the tight iliopsoas may exacerbate anterior impingement mechanics, and addressing the tendon concurrently with osseous decompression and labral repair yields superior clinical outcomes.



Contraindications
Absolute contraindications include active local or systemic infection, severe osteoarthritis (Tönnis grade 2 or 3), and profound acetabular dysplasia (Lateral Center Edge Angle < 20 degrees). In dysplastic hips, the iliopsoas is a critical dynamic stabilizer; its release can precipitate rapid subluxation and catastrophic joint failure. Relative contraindications include generalized ligamentous laxity (e.g., Ehlers-Danlos syndrome), where capsular plication may be required, and isolated snapping without pain, which should never be operated upon regardless of the mechanical severity of the snap.
| Parameter | Operative Indications | Non-Operative Indications | Contraindications |
|---|---|---|---|
| Duration of Symptoms | > 3-6 months | < 3 months | N/A |
| Conservative Therapy | Failed PT, NSAIDs, CSI | First-line treatment | N/A |
| Pain Level | Functionally limiting | Mild to moderate | Asymptomatic snap |
| Intra-articular Pathology | Concomitant FAI, Labral tear | Isolated tendonitis | Severe OA (Tönnis 2-3) |
| Diagnostic Injection | Positive relief | Not yet attempted | N/A |
| Bony Morphology | Normal coverage (LCEA > 25°) | Normal coverage | Dysplasia (LCEA < 20°) |





Pre Operative Planning and Patient Positioning
Clinical Evaluation and Imaging
Pre-operative planning begins with a meticulous physical examination. The Stinchfield test (resisted hip flexion at 30 degrees) typically elicits deep groin pain. The dynamic snapping can be reproduced by passively moving the hip from a flexed, abducted, and externally rotated position into extension, adduction, and internal rotation.
Standard radiographic evaluation includes an AP pelvis, false profile, and Dunn lateral views to assess for dysplasia, FAI (cam/pincer morphology), and joint space narrowing. Magnetic Resonance Arthrography (MRA) is the gold standard for evaluating the labrum, articular cartilage, and the iliopsoas tendon. MRA can reveal tendinosis, peritendinous edema, bursitis, and the characteristic 3 o'clock anterior labral tear associated with psoas impingement. Dynamic ultrasound is highly valuable for visualizing the tendon snapping in real-time over the iliopectineal eminence.




Patient Positioning and Setup
The procedure is typically performed under general anesthesia with profound muscle relaxation to facilitate joint distraction. The patient is positioned either supine or in the lateral decubitus position on a specialized hip distraction table, depending on surgeon preference. The supine position is generally favored for its ease of setup and anatomical orientation.
A well-padded oversized perineal post is utilized to provide counter-traction. The operative leg is placed in the traction boot, and traction is applied with the hip in slight flexion (10-15 degrees), neutral rotation, and slight abduction. Fluoroscopy is brought in from the contralateral side to confirm adequate joint distraction (typically 10-12 mm of joint space is required to safely establish central compartment portals). The non-operative leg is abducted to accommodate the fluoroscopy C-arm.





Careful attention must be paid to the duration and magnitude of traction to minimize the risk of neuropraxia to the pudendal and sciatic nerves. Traction time should ideally be limited to less than 90 minutes. Once the central compartment work is complete, traction is released, and the hip is flexed to 45 degrees to relax the anterior capsule and facilitate access to the peripheral compartment and the iliopsoas tendon.





Detailed Surgical Approach and Technique
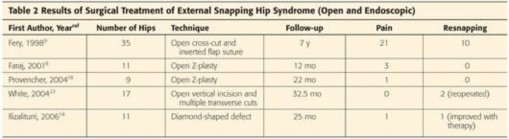
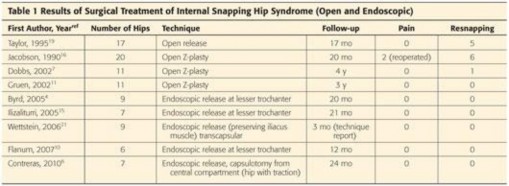
Surgical management has evolved significantly from open procedures to advanced arthroscopic and endoscopic techniques. Arthroscopic release offers the advantages of smaller incisions, less soft tissue morbidity, concurrent management of intra-articular pathology, and accelerated rehabilitation. There are three primary arthroscopic/endoscopic techniques described for iliopsoas release: the central compartment (transcapsular) release, the peripheral compartment release, and the endoscopic lesser trochanteric release.
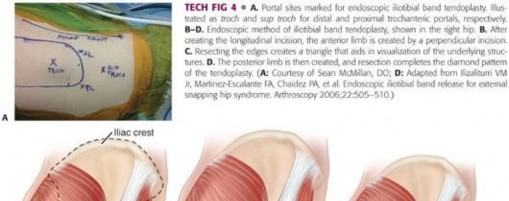
Portal Placement and Diagnostic Arthroscopy
Standard arthroscopic portals are established. The Anterolateral (AL) portal is created first under fluoroscopic guidance, entering the joint just superior to the femoral neck and lateral to the acetabular rim. A diagnostic arthroscopy is performed. The Mid-Anterior (MAP) portal is then established under direct visualization. An interportal capsulotomy is typically performed connecting the AL and MAP portals to enhance mobility and visualization within the central compartment. Any intra-articular pathology, such as labral tears or chondral defects, is addressed at this stage.





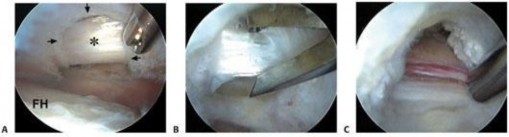
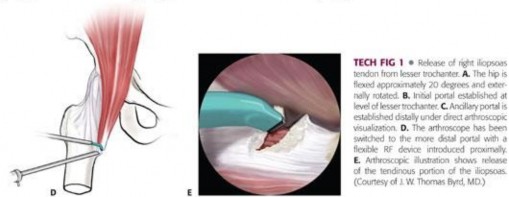
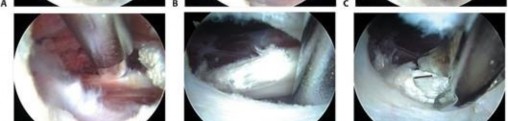
Central Compartment Transcapsular Release
The transcapsular release
Clinical & Radiographic Imaging
















































































You Might Also Like

