Mastering Shoulder Arthroscopy: Indications, Positioning, and Anesthesia
Key Takeaway
Shoulder arthroscopy is a highly reproducible, low-risk procedure indicated for developmental, traumatic, degenerative, or inflammatory glenohumeral conditions failing conservative management. Success relies heavily on meticulous patient positioning—primarily the lateral decubitus or beach chair configurations—and precise anesthetic management. Proper traction vectors, pressure point padding, and cerebral perfusion monitoring are critical to minimizing complications such as brachial plexus neurapraxia or catastrophic cerebral hypoperfusion during hypotensive anesthesia.
INTRODUCTION TO SHOULDER ARTHROSCOPY
Over the past several decades, shoulder arthroscopy has evolved from a purely diagnostic modality into a highly sophisticated therapeutic intervention. When performed by a skilled orthopedic surgeon, arthroscopic treatment of the shoulder yields a low-risk, high-reward, and highly reproducible outcome. The transition from open arthrotomy to minimally invasive arthroscopic techniques has drastically reduced perioperative morbidity, minimized disruption of the deltoid and rotator cuff footprint, and accelerated postoperative rehabilitation. However, the success of these procedures is inextricably linked to strict adherence to surgical indications, meticulous patient positioning, and a profound understanding of the physiological implications of regional and general anesthesia.
INDICATIONS AND CONTRAINDICATIONS
Primary Indications
Arthroscopic intervention is indicated for a broad spectrum of developmental, traumatic, degenerative, and inflammatory conditions of the shoulder that result in recalcitrant pain, mechanical instability, or functional disability. Crucially, surgical intervention should generally be reserved for patients whose symptoms cannot be adequately controlled by a comprehensive regimen of conservative measures, including physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), and targeted corticosteroid or orthobiologic injections.
Common indications include, but are not limited to:
* Rotator Cuff Pathology: Partial-thickness tears, full-thickness tears, and subacromial impingement syndrome requiring acromioplasty.
* Glenohumeral Instability: Anterior, posterior, or multidirectional instability requiring capsulolabral repair (e.g., Bankart repair, capsular plication).
* Biceps and Superior Labral Pathology: SLAP (Superior Labrum Anterior and Posterior) lesions and long head of the biceps tendinopathy requiring tenotomy or tenodesis.
* Degenerative and Inflammatory Conditions: Early glenohumeral osteoarthritis (for debridement or chondroplasty), adhesive capsulitis requiring capsular release, and inflammatory synovitis requiring synovectomy.
* Trauma: Selected intra-articular fractures, such as greater tuberosity avulsions or bony Bankart lesions.
Contraindications
While shoulder arthroscopy is minimally invasive, it is not without risk. Surgeons must rigorously screen patients for contraindications to prevent catastrophic complications.
- Absolute Contraindications: Active local skin conditions (e.g., cellulitis, severe psoriasis plaques over planned portal sites), remote active infections that risk hematogenous seeding to the joint (e.g., untreated urinary tract infections, dental abscesses), and severe medical comorbidities precluding safe anesthesia (ASA Class IV or V).
- Relative Contraindications: Severe glenohumeral osteoarthritis with profound bone loss (where arthroplasty is more appropriate), massive irreparable rotator cuff tears with advanced pseudoparalysis (unless performing a palliative debridement or superior capsular reconstruction), and profound joint stiffness where an open release might be deemed safer by the operating surgeon.
Surgical Warning: Surgeons considering arthroscopic procedures must always advise patients during the informed consent process about the possibility of converting to an open procedure if arthroscopic findings warrant it, or if technical difficulties arise that compromise patient safety or procedural efficacy.
PREOPERATIVE EVALUATION AND ANESTHESIA
Examination Under Anesthesia (EUA)
Regardless of the chosen position or anesthetic technique, a thorough Examination Under Anesthesia (EUA) is mandatory. After the induction of anesthesia and before moving the patient into the final surgical position, both shoulders must be examined and compared. The surgeon should systematically evaluate the range of motion (forward elevation, internal/external rotation at varying degrees of abduction) and perform stability testing (load-and-shift, sulcus sign, anterior/posterior drawer). This provides a baseline assessment free of patient guarding and confirms the preoperative diagnosis.
Anesthetic Considerations
Shoulder arthroscopy can be performed under general anesthesia, regional anesthesia (interscalene nerve block), or a combination of both.
If the lateral decubitus position is utilized, general anesthesia with endotracheal intubation is strongly preferred to ensure airway security and patient comfort during prolonged traction. Conversely, the "beach chair" position allows for the use of regional anesthesia alone with deep sedation, though many surgeons prefer a combined approach to manage airway reflexes and ensure absolute immobility.
Clinical Pearl: We advocate for the use of hypotensive anesthesia (maintaining mean arterial pressure between 60 and 70 mm Hg) to minimize intra-articular bleeding and optimize arthroscopic visualization. However, cerebral perfusion is more reliably maintained in the lateral decubitus position than in the "beach chair" position during hypotensive episodes.
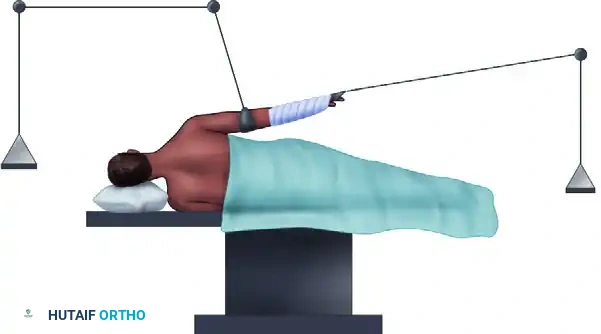
PATIENT POSITIONING: THE LATERAL DECUBITUS POSITION
The lateral decubitus position is arguably the most commonly utilized configuration for shoulder arthroscopy. Its primary advantages include superior access to the posterior and inferior shoulder compartments, excellent visualization of the glenohumeral joint through applied traction, and a safer physiological profile regarding cerebral perfusion.
Setup and Biomechanics
The patient is placed in the lateral decubitus position with the affected shoulder exposed superiorly. Stability is achieved using a vacuum beanbag and a kidney rest, supplemented by a secure chest strap.
Meticulous attention must be paid to protecting the patient's dependent structures:
* The head is supported by a specialized foam rest, ensuring the cervical spine remains in a neutral alignment.
* Strict care is taken to protect the eyes and the downside ear from pressure necrosis.
* An axillary roll is routinely placed just caudal to the dependent axilla to prevent compression of the dependent brachial plexus and to improve ventilation.
* All pressure points are heavily padded. A pillow is placed beneath the down leg to protect the common peroneal nerve at the fibular head and the lateral malleolus, with additional pillows placed between the knees and ankles.
Peripheral pulses and pulse oximeter readings on the dependent arm must be continuously evaluated by the anesthesia team to ensure axillary vascular structures are not compromised.
The Gross and Fitzgibbons Modification
Gross and Fitzgibbons described a highly effective modification to the standard straight lateral decubitus position. By tilting the patient 20 to 30 degrees posteriorly, the glenoid articular surface is brought parallel to the floor.
This modification offers three distinct biomechanical advantages:
1. Reduced Traction Requirements: It necessitates less traction weight to distract the joint, thereby decreasing the risk of neurapraxia to the brachial plexus.
2. Accentuation of Pathology: It accentuates tears of the glenoid labrum, as gravity and positioning pull the torn tissue away from the glenoid bed rather than compressing it in line with the articular surface.
3. Enhanced Access: It significantly improves arthroscopic access to the inferior third of the glenoid labrum and the inferior capsule, which is critical for complex instability repairs.
Arm Positioning and Traction Principles
Using a commercially available sterile arm traction device, approximately 10 to 13 lbs of traction is applied to the operative extremity. The fundamental principle is one of balanced suspension rather than brute distraction. Overdistraction with excessive weight must be strictly avoided; only the minimum amount of traction required for clear intra-articular viewing should be utilized.
Pitfall: Compressive damage to the superficial radial nerve is a known complication of arm traction setups. Stopping the compressive wrap (e.g., Coban) proximal to the radiocarpal joint line is a simple yet critical step to prevent this iatrogenic injury.
Historically, early investigations suggested positioning the arm in 70 degrees of abduction and 20 to 30 degrees of forward flexion. However, due to concerns regarding brachial plexus neurapraxia, Klein et al. conducted a landmark study evaluating strain on the brachial plexus across varying degrees of abduction and flexion. They concluded that two specific positions provided maximal visibility with minimal neural strain:
* 45 degrees of forward flexion with 90 degrees of abduction.
* 45 degrees of forward flexion with 0 degrees of abduction.
Despite these findings, many experienced arthroscopists continue to use 30 to 60 degrees of abduction and 20 to 30 degrees of forward flexion, mitigating risk by strictly limiting the traction weight and minimizing the overall length of the procedure. Complications following shoulder arthroscopy range between 2.3% and 3.0% in modern literature, with transient neurapraxia from excessive arm traction being the most common. Fortunately, permanent neural or vascular injuries are exceedingly rare.
Dual Traction Techniques
To further optimize visualization without subluxing the humeral head inferiorly, Gross and Fitzgibbons described the use of dual traction—applying both vertical and longitudinal vectors. Most of the traction force is applied vertically to distract the glenohumeral joint laterally.

However, vertical traction introduces specific risks regarding limb perfusion. Hennrikus et al. compared simple longitudinal traction against dual traction to evaluate changes in extremity oxygen saturation. Their findings were definitive:
* Patients with simple longitudinal traction rarely experienced ablated oxygen saturation (1 of 30 patients).
* Patients with vertical traction using a narrow 2-inch sling experienced a high rate of ablated oxygen saturation (25 of 30 patients).
* Patients with vertical traction using a wider 4-inch sling had a significantly lower rate of vascular compromise (7 of 30 patients).
Surgical Rule: If vertical traction is added to the longitudinal setup, a wide 4-inch sling must be used, and the extremity's capillary refill and pulse oximetry must be monitored continuously.
Subacromial Space Positioning
When transitioning from the glenohumeral joint to the subacromial space or the acromioclavicular (AC) joint, the arm position must be adjusted. The arm is brought down to 20 to 45 degrees of abduction and 0 degrees of flexion. This specific alignment permits mild inferior subluxation of the humeral head, effectively opening up the subacromial space and facilitating burr and shaver access during acromioplasty or rotator cuff repair.
PATIENT POSITIONING: THE "BEACH CHAIR" POSITION
The "beach chair" (or modified Fowler) position has gained immense popularity, particularly for procedures focusing on the subacromial space, rotator cuff, and anterior stabilization. Skyhar, Altchek, and Warren popularized this technique, noting its distinct advantages in a series of 100 shoulder arthroscopies.
Advantages of the Beach Chair Position
- Anatomical Orientation: The patient is seated upright, providing the surgeon with a highly intuitive, anatomic orientation of the shoulder girdle.
- Elimination of Traction: Because the arm is freely mobile and supported by an assistant or a sterile mechanical arm holder, heavy traction is not required, virtually eliminating the risk of traction-induced brachial plexus neurapraxia.
- Capsular Fidelity: There is less distortion of the intra-articular capsular anatomy, allowing for a more accurate assessment of capsular laxity.
- Ease of Conversion: If an open procedure (e.g., open Latarjet or mini-open rotator cuff repair) becomes necessary, conversion is seamless, requiring no repositioning or repreparation of the patient.
Disadvantages and Physiological Risks
The primary technical disadvantage of the beach chair position is the relative difficulty in accessing the posterior shoulder and establishing posterior portals compared to the lateral decubitus position.
However, the most critical concern is physiological. The upright posture induces a hydrostatic gradient that significantly affects cerebral perfusion, particularly when hypotensive anesthesia is employed. Complications of catastrophic stroke, anoxic brain injury, and death have been reported due to unrecognized cerebral hypoperfusion.
Surgical Warning: Blood pressure measured at the level of the brachium (arm) is significantly lower than that in the cerebrum, and this discrepancy is exacerbated if carotid artery disease is present.
According to Papadonikolakis et al., blood pressure measured via a calf cuff in a seated patient can easily read 40 mm Hg higher than the actual cerebral perfusion pressure. Therefore, relying on calf blood pressure in the beach chair position is dangerous. Blood pressure must be monitored on the non-operative brachium, and the anesthesia team must calculate the hydrostatic gradient (approximately a 1 mm Hg drop for every 1.25 cm of vertical height difference between the blood pressure cuff and the external auditory meatus). When possible, direct cerebral perfusion monitors (e.g., near-infrared spectroscopy, NIRS) should be utilized.
Furthermore, the beach chair position can trigger the Bezold-Jarisch reflex—a profound hypotensive and bradycardic event (HBE) mediated by vagal tone in response to venous pooling in the lower extremities. Prophylactic measures, including adequate intravenous hydration, the use of sequential compression devices (SCDs) on the lower extremities, and careful titration of vasoactive medications by the anesthesia team, are mandatory.
SURGICAL PREPARATION AND DRAPING
Regardless of the chosen position, meticulous sterile preparation is paramount.
- Positioning the Team: In the lateral decubitus setup, the anesthesiologist is positioned opposite the patient’s face, allowing the surgical team (surgeon, assistant, and scrub nurse) to stand posterior to the patient’s shoulder. The arthroscopic tower and viewing monitors are positioned at an angle toward the head of the table for direct, ergonomic viewing.
- Draping: A large, self-adhesive, plastic U-drape is applied along the patient’s spine, across the base of the hairline, and down the anterior chest. This isolates the unsterile anesthesia field from the operative site and protects the patient's face.
- Skin Preparation: The shoulder, axilla, and proximal arm are prepped with a chlorhexidine or iodine-based solution.
- Axillary Isolation: The axilla is a known reservoir for Cutibacterium acnes (formerly Propionibacterium acnes). To minimize contamination, a sterile 4 × 4-inch sponge is placed directly over the axillary hair and sealed tightly with an adhesive barrier drape (e.g., Ioban, 3M, St. Paul, MN).
- Final Barrier: The entire surgical field is then draped with a waterproof, adhesive surgical barrier drape, ensuring a watertight seal that will withstand the high volumes of irrigation fluid used during arthroscopy.
POSTOPERATIVE PROTOCOLS
Postoperative management is dictated by the specific pathology addressed during the arthroscopy.
- Diagnostic Arthroscopy / Simple Debridement: Patients are typically placed in a simple sling for comfort. Immediate passive and active-assisted range of motion (ROM) exercises are initiated to prevent adhesive capsulitis.
- Rotator Cuff Repair: The arm is immobilized in an abduction sling for 4 to 6 weeks. Early rehabilitation focuses on strictly passive ROM to protect the repair, progressing to active-assisted ROM at 6 weeks, and strengthening at 10 to 12 weeks.
- Instability Repair (Labral Repair): The arm is immobilized in a standard sling (or external rotation brace for specific posterior/multidirectional repairs). External rotation and combined abduction/external rotation are strictly limited for the first 6 weeks to protect the anterior capsulolabral reconstruction.
In all cases, meticulous portal site care, multimodal pain management (often extending the benefits of the preoperative interscalene block with oral analgesics), and close clinical follow-up are essential components of a successful surgical outcome.
You Might Also Like