Orthopedic Shoulder & Elbow MCQs: Practice Questions & Exam Preparation
14 Apr 2026
50 min read
71 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Shoulder & Elbow MCQs: Practice Qu...
00:00
Start Quiz
Question 1High Yield
When attempting to treat a proximal tibial metadiaphyseal fracture with an intramedullary nail, what is the most common angular malalignment?
Explanation
No detailed explanation provided for this question.
Question 2High Yield
Which surgical approach is less useful for children who have reached walking age because it does not allow for capsulorrhaphy?
Explanation
- Medial_
Question 3High Yield
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
Mallet fingers without DIP joint subluxation can be treated with extension splinting. Surgical fixation may be necessary in bony mallet injuries when the joint is subluxated. Size of the bony fragment, while often correlating with stability, is not always an indication for fixation. Buddy taping allows motion; therefore, the fragment will not heal in the appropriate position. Intermittent splinting with range-of-motion exercises also will not allow the fragment to heal in the appropriate position.
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 4High Yield
Surgical repair of the injury shown in the MRI scans in Figures 1 through 4 through a single-incision approach has a higher incidence of
33
33
Explanation
The MRI scans show a distal biceps tendon avulsion with significant retraction. When addressing these injuries, a single-incision approach has been associated with an increased risk of lateral antebrachial cutaneous nerve injury. A two-incision approach has been associated with an increased risk of heterotopic ossification, second surgeries and posterior interosseous nerve injury.
34
34
Question 5High Yield
A 32-year-old soccer player presents with severe right ankle pain and inability to bear weight after sustaining a slide-tackle injury during a game. Radiographs are shown in Figures A and B. Given the nature of his injury, he is taken for surgical reduction and fixation. Following medial malleolar fixation, the syndesmosis is addressed. All of the following are true regarding the most appropriate intraoperative technique for anatomic syndesmotic reduction EXCEPT:




Explanation
When placing a clamp across the syndesmosis to facilitate reduction, the lateral tine should be placed directly on the lateral malleolar ridge. Placing the lateral tine either more anteriorly or posteriorly has been shown to result in sagittal malreduction from fibular translation.
Syndesmotic reduction has proven to be technically challenging, with reportedly greater than 50% of cases resulting in malreduction. Provisional reduction is most often attained via a pointed reduction clamp. Placement of the lateral tine is outlined above. The medial tine should be placed at the anatomic midportion of the medial tibia, which can be confirmed
fluoroscopically as the anterior third of the tibia on a true lateral view of the ankle. It is important to maintain the axis of the clamp parallel to the joint line and to the anatomic syndesmotic angle. The clamp should furthermore be maintained 1-2cm proximal to the mortise, at the level of the incisura, to avoid deformation or undue translation of the fibula. Lastly, over-compression of the syndesmosis has been demonstrated, though the clinical implications remain controversial.
Putnam et al. performed a radiographic analysis of the ideal orientation for placement of a syndesmotic reduction clamp. Based on the CT scans of uninjured adult ankles, the authors showed that the trans-syndesmotic axis could be most reliably paralleled by a reduction clamp by placing the lateral tine on the lateral malleolar ridge and the medial tine radiographically within the anterior third of the tibia, anatomically half-way between the anterior and posterior cortices. They further specified that the ideal location was within the central one-third of the distance from the anterior tibial cortex to the anterior fibular cortex.
Cosgrove et al. prospectively evaluated the effect of medial clamp tine positioning on the incidence of syndesmotic malreduction. The authors found that malreduction most often resulted from deviation of the clamp axis from the syndesmotic axis. With the clamp at 1-2cm proximal to the mortise and the lateral tine on the lateral malleolar ridge, the ideal position of the medial tine was within the anterior third of the tibia. The rate of sagittal malreduction increased substantially with increasingly posterior placement of the medial tine. The medial clamp position did not affect coronal plane malreduction.
Gardner et al. review the technical considerations in reduction and fixation of syndesmotic injuries. The authors stress careful positioning of the reduction clamp, advocating that the clamp should be placed from the lateral malleolar ridge to the center of the anteroposterior width of the medial tibia.
Additionally, they note that placement too proximal or distal results in coronal plane deformity of the fibula, and that over-compression of the syndesmosis is certainly possible.
Figure A is the AP radiograph of the left ankle demonstrating a displaced medial malleolar fracture and syndesmotic widening. Figure B is the lateral radiograph of the ipsilateral knee showing an associated proximal fibular fracture.
Illustration A shows the syndesmotic angle and anatomic trans-syndesmotic axis as compared to the AP and lateral fluoroscopic axes. Illustration B shows the ideal positioning of the medial tine within the anterior third of the tibia on a true lateral view of the ankle.
Incorrect answers:
Answer 1: The axis of the reduction camp should parallel that of the trans-syndesmotic axis.
Answer 3: The medial tine is ideally placed within the anterior third of the tibia, and moreover within the central third of the distance between the anterior tibial and fibular cortices on a true lateral view of the ankle.
Answer 4: The clamp is ideally placed 1-2cm proximal to the tibial plafond at the level of the incisura to avoid deformation of the fibula, which has been associated with placement too proximal or distal.
Answer 5: Over-compression of the syndesmosis has been demonstrated radiographically, though the effect on the range of motion and clinical outcomes remains unclear.
Syndesmotic reduction has proven to be technically challenging, with reportedly greater than 50% of cases resulting in malreduction. Provisional reduction is most often attained via a pointed reduction clamp. Placement of the lateral tine is outlined above. The medial tine should be placed at the anatomic midportion of the medial tibia, which can be confirmed
fluoroscopically as the anterior third of the tibia on a true lateral view of the ankle. It is important to maintain the axis of the clamp parallel to the joint line and to the anatomic syndesmotic angle. The clamp should furthermore be maintained 1-2cm proximal to the mortise, at the level of the incisura, to avoid deformation or undue translation of the fibula. Lastly, over-compression of the syndesmosis has been demonstrated, though the clinical implications remain controversial.
Putnam et al. performed a radiographic analysis of the ideal orientation for placement of a syndesmotic reduction clamp. Based on the CT scans of uninjured adult ankles, the authors showed that the trans-syndesmotic axis could be most reliably paralleled by a reduction clamp by placing the lateral tine on the lateral malleolar ridge and the medial tine radiographically within the anterior third of the tibia, anatomically half-way between the anterior and posterior cortices. They further specified that the ideal location was within the central one-third of the distance from the anterior tibial cortex to the anterior fibular cortex.
Cosgrove et al. prospectively evaluated the effect of medial clamp tine positioning on the incidence of syndesmotic malreduction. The authors found that malreduction most often resulted from deviation of the clamp axis from the syndesmotic axis. With the clamp at 1-2cm proximal to the mortise and the lateral tine on the lateral malleolar ridge, the ideal position of the medial tine was within the anterior third of the tibia. The rate of sagittal malreduction increased substantially with increasingly posterior placement of the medial tine. The medial clamp position did not affect coronal plane malreduction.
Gardner et al. review the technical considerations in reduction and fixation of syndesmotic injuries. The authors stress careful positioning of the reduction clamp, advocating that the clamp should be placed from the lateral malleolar ridge to the center of the anteroposterior width of the medial tibia.
Additionally, they note that placement too proximal or distal results in coronal plane deformity of the fibula, and that over-compression of the syndesmosis is certainly possible.
Figure A is the AP radiograph of the left ankle demonstrating a displaced medial malleolar fracture and syndesmotic widening. Figure B is the lateral radiograph of the ipsilateral knee showing an associated proximal fibular fracture.
Illustration A shows the syndesmotic angle and anatomic trans-syndesmotic axis as compared to the AP and lateral fluoroscopic axes. Illustration B shows the ideal positioning of the medial tine within the anterior third of the tibia on a true lateral view of the ankle.
Incorrect answers:
Answer 1: The axis of the reduction camp should parallel that of the trans-syndesmotic axis.
Answer 3: The medial tine is ideally placed within the anterior third of the tibia, and moreover within the central third of the distance between the anterior tibial and fibular cortices on a true lateral view of the ankle.
Answer 4: The clamp is ideally placed 1-2cm proximal to the tibial plafond at the level of the incisura to avoid deformation of the fibula, which has been associated with placement too proximal or distal.
Answer 5: Over-compression of the syndesmosis has been demonstrated radiographically, though the effect on the range of motion and clinical outcomes remains unclear.
Question 6High Yield
A 23-year-old right-hand dominant professional baseball pitcher has right shoulder pain when releasing the ball. He has noticed his velocity has decreased over the past 2 months. Examination reveals supine abducted external rotation of 110 degrees compared to 100 degrees on the left side. His internal rotation is 30 degrees on the right compared to 70 degrees on the left side. Rotator cuff strength is normal. All other clinical tests are normal. MRI with contrast reveals no intra-articular lesions. What is the best course of treatment?
Explanation
DISCUSSION: The examination reveals that the patient has posterior capsular tightness. Surgery should not be considered until the patient has failed to respond to nonsurgical management. The internal rotation contracture (GIRD - glenohumeral internal rotation deficit) should be addressed with appropriate posterior capsular stretching. This should then be followed by appropriate rotator cuff and scapular stabilization exercises. Only if this management fails to relieve the patient’s symptoms should surgery be considered. This patient clearly does not need external rotation stretching given the fact that he has normal external rotation.
REFERENCES: Meister K: Injuries to the shoulder in the throwing athlete. Part two: evaluation/ treatment. Am J Sports Med 2000;28:587-601.
Liu SH, Boynton E: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
Tyler TF, Nicholas SJ, Roy T, et al: Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am J Sports Med 2000;28:668-673.
2010 Sports Medicine Examination Answer Book • 21
DISCUSSION: The examination reveals that the patient has posterior capsular tightness. Surgery should not be considered until the patient has failed to respond to nonsurgical management. The internal rotation contracture (GIRD - glenohumeral internal rotation deficit) should be addressed with appropriate posterior capsular stretching. This should then be followed by appropriate rotator cuff and scapular stabilization exercises. Only if this management fails to relieve the patient’s symptoms should surgery be considered. This patient clearly does not need external rotation stretching given the fact that he has normal external rotation.
REFERENCES: Meister K: Injuries to the shoulder in the throwing athlete. Part two: evaluation/ treatment. Am J Sports Med 2000;28:587-601.
Liu SH, Boynton E: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
Tyler TF, Nicholas SJ, Roy T, et al: Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am J Sports Med 2000;28:668-673.
2010 Sports Medicine Examination Answer Book • 21
Question 7High Yield
The mean C obb measurement for idiopathic scoliosis curves with a 7° angle of trunk rotation (ATR) is:
Explanation
Although the angle of trunk rotation (ATR) does not convert directly to a C obb angle, there are population-based figures for mean curve at each ATR. The mean C obb angle for curves having a 7° ATR is 20°.
Question 8High Yield
Figures 1 and 2 are the radiographs of a 12-year-old boy who has been experiencing increased pain in his right, dominant elbow while pitching. He notes that his velocity is decreasing, and he can no longer throw as many pitches without discomfort. Examination reveals tenderness on palpation of his medial distal humerus, but no evidence is seen of instability to valgus stress at either 0° or 30° of elbow flexion. What is the most appropriate recommendation at this time?

Explanation
■
Radiographs and examination are consistent with medial epicondylar apophysitis, or "Little Leaguer elbow," which is thought to be secondary to repetitive traction stresses across the open physis while throwing. MRI generally does not change the treatment in these patients. Surgical fixation is indicated in patients with displaced avulsion fractures of the medial epicondyle, particularly in throwing athletes. In light of the lack of clinical instability, ulnar collateral ligament reconstruction is not indicated in this patient.
■
Radiographs and examination are consistent with medial epicondylar apophysitis, or "Little Leaguer elbow," which is thought to be secondary to repetitive traction stresses across the open physis while throwing. MRI generally does not change the treatment in these patients. Surgical fixation is indicated in patients with displaced avulsion fractures of the medial epicondyle, particularly in throwing athletes. In light of the lack of clinical instability, ulnar collateral ligament reconstruction is not indicated in this patient.
Question 9High Yield
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 4 through 8 are the axial and coronal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
---
---
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 4 through 8 are the axial and coronal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
---
---






Explanation
Medial plateau fracture dislocations are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the anteroposterior radiograph include an intact lateral column (lateral articular surface still in continuity with tibial shaft), centrolateral articular impaction, shortening, and condylar widening. The medial femoral condyle stays with the fractured medial tibial plateau segment.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 10High Yield
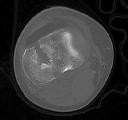
The mechanism for the osseous destruction is attributable to
Explanation
This scenario is a classic example of the development of Charcot foot. A red, swollen, deformed foot without ulceration suggests neuroarthropathy. Normal inflammatory marker findings, no history of fever or chills, and radiographs demonstrating bone loss support the diagnosis. Limb elevation with dramatic reduction in erythema is also characteristic of this disease process and does not occur with infection. Total-contact casting is the cornerstone of treatment for acute Charcot disease. Hemoglobin A1C is an indicator of glucose averaged over a 3-month period, providing the most reliable indication of a patient's ongoing glucose control. The pathophysiology of bone destruction is believed to be hypervascularity of bone. Infection and Charcot disease may develop simultaneously, but the combination is rare.
RECOMMENDED READINGS
[Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.](http://www.ncbi.nlm.nih.gov/pubmed/23919113)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23919113)
[Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. ](http://www.ncbi.nlm.nih.gov/pubmed/16701052)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16701052)
RECOMMENDED READINGS
[Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.](http://www.ncbi.nlm.nih.gov/pubmed/23919113)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23919113)
[Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. ](http://www.ncbi.nlm.nih.gov/pubmed/16701052)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16701052)
Question 11High Yield
Which of the following materials has mainly osteoinductive properties with little or no osteoconductive ability:
Explanation
Grafting materials may include osteoconductive and/or osteoinductive properties and osteoprogenitor cells.
Cancellous bone and vascularized bone graft are the only materials that have significant osteoconductive, osteoinductive, and osteoprogenitor cells.
Several materials are mainly osteoinductive. Remember the definition of osteoinductive and osteoconductive properties: Osteoinductive factors: Molecules that have the capability of inducing osteoblastiCprecursors to differentiate into mature bone
forming cells.
Osteoinductive factors (without significant osteoconductive properties) include growth factors such as BMP-2 and rhBMP-7 (OP-1, Stryker Biotech, Hopkinton, Mass) and demineralized bone matrix.
Osteoconductive factors: The ability of a porous material to provide a scaffold for new bone formation.
Osteoconductive materials (without significant osteoinductive properties) include ceramics such as coral-based hydroxyapatite graft substitutes, Norian skeletal repair system (Norian Corporation, Cupertino, Calif), and calcium sulfate pellets (Osteoset, Wright Medical Technology Inc., Arlington, Tenn).
Bone marrow has the potential of supplying osteoprogenitor cells but has little osteoinductive or osteoconductive properties. Correct Answer: Recombinant bone morphogenetiCprotein-7 (rhBMP-7)
Cancellous bone and vascularized bone graft are the only materials that have significant osteoconductive, osteoinductive, and osteoprogenitor cells.
Several materials are mainly osteoinductive. Remember the definition of osteoinductive and osteoconductive properties: Osteoinductive factors: Molecules that have the capability of inducing osteoblastiCprecursors to differentiate into mature bone
forming cells.
Osteoinductive factors (without significant osteoconductive properties) include growth factors such as BMP-2 and rhBMP-7 (OP-1, Stryker Biotech, Hopkinton, Mass) and demineralized bone matrix.
Osteoconductive factors: The ability of a porous material to provide a scaffold for new bone formation.
Osteoconductive materials (without significant osteoinductive properties) include ceramics such as coral-based hydroxyapatite graft substitutes, Norian skeletal repair system (Norian Corporation, Cupertino, Calif), and calcium sulfate pellets (Osteoset, Wright Medical Technology Inc., Arlington, Tenn).
Bone marrow has the potential of supplying osteoprogenitor cells but has little osteoinductive or osteoconductive properties. Correct Answer: Recombinant bone morphogenetiCprotein-7 (rhBMP-7)
Question 12High Yield
What is the best next treatment step?
Explanation
Figures 72a and 72b provide evidence of a posterior dislocation. These are often missed, occurring in only 2% to 4% of dislocations. The anteroposterior radiographs show the “lightbulb” sign and loss of the normal overlap of the humerus on the glenoid. Axillary radiographs are the preferred means of diagnosis. The MR image clearly shows a locked posterior dislocation. This necessitates
urgent reduction under anesthesia. If the reduction is stable, nonsurgical treatment can be indicated. If unstable, the modified McLaughlin procedure, which involves transferring the lesser tuberosity into the anterior Hill-Sachs lesion, can be effective.
RECOMMENDED READINGS
16. [Hawkins RJ, Neer CS 2nd, Pianta RM, Mendoza FX. Locked posterior dislocation of the shoulder. J Bone Joint Surg Am. 1987 Jan;69(1):9-18. PubMed PMID: 3805075. ](http://www.ncbi.nlm.nih.gov/pubmed/3805075)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3805075)
17. [McLAUGHLIN HL. Posterior dislocation of the shoulder. J Bone Joint Surg Am. 1952 Jul;24 A(3):584-90. PubMed PMID: 14946209. ](http://www.ncbi.nlm.nih.gov/pubmed/14946209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14946209)
18. [Checchia SL, Santos PD, Miyazaki AN. Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg. 1998 Jan-Feb;7(1):53-65. PubMed PMID: 9524341. ](http://www.ncbi.nlm.nih.gov/pubmed/9524341)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9524341)
urgent reduction under anesthesia. If the reduction is stable, nonsurgical treatment can be indicated. If unstable, the modified McLaughlin procedure, which involves transferring the lesser tuberosity into the anterior Hill-Sachs lesion, can be effective.
RECOMMENDED READINGS
16. [Hawkins RJ, Neer CS 2nd, Pianta RM, Mendoza FX. Locked posterior dislocation of the shoulder. J Bone Joint Surg Am. 1987 Jan;69(1):9-18. PubMed PMID: 3805075. ](http://www.ncbi.nlm.nih.gov/pubmed/3805075)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3805075)
17. [McLAUGHLIN HL. Posterior dislocation of the shoulder. J Bone Joint Surg Am. 1952 Jul;24 A(3):584-90. PubMed PMID: 14946209. ](http://www.ncbi.nlm.nih.gov/pubmed/14946209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14946209)
18. [Checchia SL, Santos PD, Miyazaki AN. Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg. 1998 Jan-Feb;7(1):53-65. PubMed PMID: 9524341. ](http://www.ncbi.nlm.nih.gov/pubmed/9524341)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9524341)
Question 13High Yield
Physeal sparing and physeal respecting anterior cruciate ligament (ACL) reconstruction techniques have been developed for use in skeletally immature athletes to minimize the risk of
Explanation
■
Several physeal sparing and physeal respecting ACL reconstruction techniques have been developed to use in skeletally immature patients to minimize the risk of growth disturbance. Growth disturbance can occur after ACL surgery in skeletally immature athletes and includes tibial recurvatum resulting from tibial tubercle apophyseal arrest, as well as limb length inequality and / or angular deformity, typically femoral valgus resulting from physeal arrest or overgrowth. Procurvatum does not occur. A stable ACL reconstruction will also minimize meniscal injury and chondral injury.
Several physeal sparing and physeal respecting ACL reconstruction techniques have been developed to use in skeletally immature patients to minimize the risk of growth disturbance. Growth disturbance can occur after ACL surgery in skeletally immature athletes and includes tibial recurvatum resulting from tibial tubercle apophyseal arrest, as well as limb length inequality and / or angular deformity, typically femoral valgus resulting from physeal arrest or overgrowth. Procurvatum does not occur. A stable ACL reconstruction will also minimize meniscal injury and chondral injury.
Question 14High Yield
The risk of progression with congenital kyphosis is greatest with which of the following?
Explanation
DISCUSSION: The risk of neurologic compromise associated with congenital kyphosis is normally secondary to risk of progression. The classic study of the natural history of congenital spinal deformity by McMaster and Singh confirms that an anterolateral bar with contralateral quadrant vertebrae has the greatest risk.
REFERENCES: McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, p 351.
REFERENCES: McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, p 351.
Question 15High Yield
A 15-year-old boy has a fracture of the proximal tibia extending from the apophysis of the tubercle up through the posterior part of the proximal tibial epiphysis and into the joint. What is the most likely mechanism of injury?
Explanation
Tibial Tuberosity Fractures Fractures of the tibial tuberosity are uncommon avulsion injuries. Most are sportsrelated and occur in older adolescents. Type I fractures represent an avulsion of a small fragment of the tuberosity. Type II fractures involve the entire anterior tuberosity with extension proximally to the level of the horizontal portion of the proximal tibial physis. Type III injuries involve the entire tuberosity with extension proximally into the articular surface, a SalterHarris type III fracture. Patients present with pain, swelling, and tenderness over the tuberosity. Patella alta may be present. Surgical treatment of type I fractures is needed if patella alta (compared to the normal uninjured side) and a significant bony prominence are present. Displaced types II and III fractures are treated with open reduction and internal fixation. A cancellous interfragmentary screw may be placed through the tuberosity into the metaphysis. Because this injury occurs in patients near skeletal maturity, growth arrest with secondary genu recurvatum is rare.
Question 16High Yield
Epiphysiodesis for macrodactyly should be performed at the following location:
Explanation
Treatment by epiphysiodesis for macrodactyly is ineffective if only single phalanges are treated. Therefore, treatment of the proximal phalanx, distal phalanx, or the middle phalanx alone is incorrect. The author prefers to perform epiphysiodesis only on the proximal and distal phalanges. The middle phalanx is not treated to preserve motion at the proximal interphalangeal joint.
Question 17High Yield
Figures 23a and 23b show
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
Explanation
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Penn I: Infections in the diabetic foot, in Samarco GJ (ed): The Foot in Diabetes. Philadelphia, PA, Lea & Febiger, 1991, pp 109-121. Wagner FW: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981, pp 66-122.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Penn I: Infections in the diabetic foot, in Samarco GJ (ed): The Foot in Diabetes. Philadelphia, PA, Lea & Febiger, 1991, pp 109-121. Wagner FW: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981, pp 66-122.
#
Question 18High Yield
History of high-dose steroid treatment after renal transplantation
Explanation
- Figure 51a
Question 19High Yield
Figures 44a through 94c
Explanation
- MYH3 mutation
Question 20High Yield
A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
Explanation
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower reoperation rate; one-quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed reduction and percutaneous pinning studies have not been published on the adult population.
25
25
Question 21High Yield
Figure 58 is the CT scan of a 50-year-old man who has fallen from a height of 12 feet. He has a reported incomplete spinal cord injury. He is intubated and sedated prior to an examination. What are the likely neurological examination findings?

Explanation
This patient has sustained a fracture dislocation of his spine at T5. At this level of injury, the incident is unlikely to affect motor strength in the upper extremities, but it can affect motor function below T5. Sensation to the nipple line is typically at T4 and the umbilicus at T10. The absence of the bulbocavernosus reflex indicates spinal shock. Bulbocavernosus reflex refers to anal sphincter contraction in response to squeezing the glans penis or pulling on the Foley. Spinal shock usually resolves within 48 hours, and the return of the reflex signals termination of spinal shock. With this degree of fracture dislocation, it is unlikely that motor function is spared without sensation changes.
RECOMMENDED READINGS
5. [Ko HY, Ditunno JF Jr, Graziani V, Little JW. The pattern of reflex recovery during spinal shock. Spinal Cord. 1999 Jun;37(6):402-9. PubMed PMID: 10432259.](http://www.ncbi.nlm.nih.gov/pubmed/10432259)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432259)
6. [Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M, Jones L, Krassioukov A, Mulcahey MJ, Schmidt-Read M, Waring W. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med. 2011 Nov;34(6):535-46. doi: 10.1179/204577211X13207446293695. PubMed PMID: 22330108. ](http://www.ncbi.nlm.nih.gov/pubmed/22330108)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22330108)
7. American Spinal Injury Association Standards for neurological classification of spinal injured patients. Chicago, IL: ASIA; 1982.
RECOMMENDED READINGS
5. [Ko HY, Ditunno JF Jr, Graziani V, Little JW. The pattern of reflex recovery during spinal shock. Spinal Cord. 1999 Jun;37(6):402-9. PubMed PMID: 10432259.](http://www.ncbi.nlm.nih.gov/pubmed/10432259)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432259)
6. [Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M, Jones L, Krassioukov A, Mulcahey MJ, Schmidt-Read M, Waring W. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med. 2011 Nov;34(6):535-46. doi: 10.1179/204577211X13207446293695. PubMed PMID: 22330108. ](http://www.ncbi.nlm.nih.gov/pubmed/22330108)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22330108)
7. American Spinal Injury Association Standards for neurological classification of spinal injured patients. Chicago, IL: ASIA; 1982.
Question 22High Yield
Contracture of which structure causes hammertoe deformity?
Explanation
A patient with a flexible hammertoe deformity has the deformity while standing, but practically no deformity when seated with the foot in equinus. The metatarsophalangeal joint is not involved. The deformity is created by contracture of the flexor digitorum longus tendon.
RECOMMENDED READINGS
[Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-44. Review. PubMed PMID: 12690869.](http://www.ncbi.nlm.nih.gov/pubmed/12690869)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690869)
Couglin MJ. Lesser toe deformities. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 1. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:363-464.
RECOMMENDED READINGS
[Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-44. Review. PubMed PMID: 12690869.](http://www.ncbi.nlm.nih.gov/pubmed/12690869)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690869)
Couglin MJ. Lesser toe deformities. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 1. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:363-464.
Question 23High Yield
Figures 13a through 13c



Explanation
- Posterior wall fracture_
Question 24High Yield
When performing a tendon transfer to restore thumb index finger lateral pinch in an ulnar nerve palsy, which tendon, when transferred to the 1st dorsal interosseous provides the greatest power?
Explanation
The EC RB transfer gives the greatest return of power pinch due to the strength of this wrist motor. This transfer should be coupled with a thumb MP arthrodesis to provide the best results. The ideal pinch transfer is an extensor pollicis brevis to first dorsal interosseous with a metaphalangeal (MP) arthrodesis at the thumb. The FDP and EDC tendons are not good choices because they are not independent tendons. The EIP provides power, but the vector of the transfer is not ideal. Transfer of the EC RL would unbalance the wrist.
Question 25High Yield
A trauma patient presents with a major head injury and femoral shaft fracture. He undergoes early fixation of the femur fracture with a prolonged period of intraoperative hypotension. What is the most likely outcome to be expected post-operatively in this patient?
Explanation
Prolonged periods of hypoxia and hypotension are associated with lower GCS scores in polytrauma patients with major head injuries.
The timing of fracture fixation in polytrauma patients with major head injuries has been controversial. Most studies support early fixation despite some literature reporting adverse affects on CNS outcomes. This is largely related to hypoxemia and hypotension intraoperatively, as well as greater fluid administration, which should be avoided. Hypoxia and hypotension are associated with lower GCS scores at the time of discharge.
In a study by Jaicks et al found a lower discharge GCS in the early fracture fixation group compared with the late group. However, they also found that this association was due to hypoxemia and hypotension.
The referenced study by Scalea et al reviewed 171 patients with pelvic or lower extremity fractures and head injuries; they showed no difference in CNS outcomes or mortality in patients who underwent early fixation.
Brundage et al showed improved outcomes (including high GCS scores at time of discharge) in those who had early fixation of femoral shaft fractures in the head-injured patient.
Incorrect Answers:
Answer 1: There is no direct correlation between intra-operative bleeding and post-operative bleeding. They is literature to support that hypotension my decrease bleeding at the time of surgery.
Answer 2: There is no direct correlation between early fixation rates and postoperative pneumonia.
Answer 3: Intraoperative hypotension is correlated with increased IV fluid administration.
Answer 4: Intraoperative hypotension is associated with decreased central nervous system outcomes.
The timing of fracture fixation in polytrauma patients with major head injuries has been controversial. Most studies support early fixation despite some literature reporting adverse affects on CNS outcomes. This is largely related to hypoxemia and hypotension intraoperatively, as well as greater fluid administration, which should be avoided. Hypoxia and hypotension are associated with lower GCS scores at the time of discharge.
In a study by Jaicks et al found a lower discharge GCS in the early fracture fixation group compared with the late group. However, they also found that this association was due to hypoxemia and hypotension.
The referenced study by Scalea et al reviewed 171 patients with pelvic or lower extremity fractures and head injuries; they showed no difference in CNS outcomes or mortality in patients who underwent early fixation.
Brundage et al showed improved outcomes (including high GCS scores at time of discharge) in those who had early fixation of femoral shaft fractures in the head-injured patient.
Incorrect Answers:
Answer 1: There is no direct correlation between intra-operative bleeding and post-operative bleeding. They is literature to support that hypotension my decrease bleeding at the time of surgery.
Answer 2: There is no direct correlation between early fixation rates and postoperative pneumonia.
Answer 3: Intraoperative hypotension is correlated with increased IV fluid administration.
Answer 4: Intraoperative hypotension is associated with decreased central nervous system outcomes.
Question 26High Yield
Which surgical approach will provide the most exposure and pose the lowest risk?
Explanation
- Lateral and medial approach with a medial malleolar osteotomy, if needed_
Question 27High Yield
The gold standard for the diagnosis of avascular necrosis of the femoral head is:
Explanation
The gold standard for the diagnosis of avascular necrosis is magnetiCresonance imaging. Changes can be seen earliest with this technique before there are changes on routine roentgenogram and even before a patient is symptomatic
Question 28High Yield
Figures 1 and 2 are the radiographs of a 37-year-old left-hand dominant man with left elbow pain and stiffness. He has a history of elbow dislocation as a child but denies any recent injuries. He has an arc of motion of 105° and stable ligaments. He describes crepitus and locking during elbow range of motion. He is an avid Crossfit athlete, intending to return to this activity and improve his range of motion. What is the best treatment?
Explanation
14
This is a young, high-demand patient with early posttraumatic arthritis of the elbow. A debridement and capsular release has the ability to address his mechanical symptoms, improve his range of motion, and not result in any post- operative functional restrictions. While this may be a temporizing procedure in this patient, it will allow him to return to weight bearing recreational activities in the near term, which is his goal. A TEA would not be indicated based on the patient's age, his degree of arthritis, and his desire to remain active post- operatively. A radial head replacement would not address the patient's ulnohumeral arthritis. Similarly, an ulnohumeral distraction interposition arthroplasty would not address the patient's radiocapitellar arthritis. Both procedures would also require adjustments to his recreational activities post- operatively to prevent progressive failure of the reconstruction.
This is a young, high-demand patient with early posttraumatic arthritis of the elbow. A debridement and capsular release has the ability to address his mechanical symptoms, improve his range of motion, and not result in any post- operative functional restrictions. While this may be a temporizing procedure in this patient, it will allow him to return to weight bearing recreational activities in the near term, which is his goal. A TEA would not be indicated based on the patient's age, his degree of arthritis, and his desire to remain active post- operatively. A radial head replacement would not address the patient's ulnohumeral arthritis. Similarly, an ulnohumeral distraction interposition arthroplasty would not address the patient's radiocapitellar arthritis. Both procedures would also require adjustments to his recreational activities post- operatively to prevent progressive failure of the reconstruction.
Question 29High Yield
A 54-year-old woman undergoes an interposition arthroplasty that fails and requires conversion to a total elbow arthroplasty. She has progressive elbow pain and radiographic loosening. Erythrocyte sedimentation rate and C-reactive protein are normal. Joint aspiration is positive for Staphylococcus epidermidis. What surgical treatment would best optimize function and decrease risk of recurrence?
Explanation
DISCUSSION
The most reliable surgical option in this case for eradicating a deep infection following a total elbow arthroplasty is a two-stage revision. One study, however, reported that staged reimplantation of an infected total elbow replacement could be successful in the setting of organisms other than S epidermidis. Arthroscopic debridement is not a viable option with poorly fixed or loose components. A single-stage revision, while considered an option in hip and knee arthroplasty, has not been definitively proven to be an option for revision total elbow arthroplasty. Single-stage revision has shown moderate success in the setting of Staphylococcus aureus infections, although with only short-term follow-up. A resection arthroplasty would likely be successful in managing the deep infection but would not optimize the functional result. Resection arthroplasty
is best reserved for low-demand or infirm patients.
DISCUSSION
The most reliable surgical option in this case for eradicating a deep infection following a total elbow arthroplasty is a two-stage revision. One study, however, reported that staged reimplantation of an infected total elbow replacement could be successful in the setting of organisms other than S epidermidis. Arthroscopic debridement is not a viable option with poorly fixed or loose components. A single-stage revision, while considered an option in hip and knee arthroplasty, has not been definitively proven to be an option for revision total elbow arthroplasty. Single-stage revision has shown moderate success in the setting of Staphylococcus aureus infections, although with only short-term follow-up. A resection arthroplasty would likely be successful in managing the deep infection but would not optimize the functional result. Resection arthroplasty
is best reserved for low-demand or infirm patients.
Question 30High Yield
Figure 92
Explanation
- Infantile vascular interruption
Question 31High Yield
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
Because the patient has failed to respond to appropriate nonsurgical management and imaging studies are normal, the use of arthroscopy not only aids in the diagnosis of chronic ankle pain, but is also helpful in its treatment. In patients with this condition, typical findings include synovitis in the lateral gutter and fibrosis along the talofibular articulation; syndesmosis chondromalacia of the talus and ankle also may be found. In patients with anterior soft-tissue impingement, approximately 84% who have a poor response to nonsurgical management will have a good to excellent response after arthroscopic synovectomy and debridement.
REFERENCES: Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
REFERENCES: Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
Question 32High Yield
A 68-year-old man presents 15 days after left total hip arthroplasty with increasing pain and subjective fevers for the last 3 days. Physical exam reveals a healing surgical incision with moderate erythema and no drainage and pain with range of motion of the hip. ESR is 44 and CRP is 32.4. Hip aspiration reveals 8000 WBC, 80% polymorphonuclear leukocytes (PMN), and two cultures positive for Cutibacterium acnes. Based on the recommendations of the 2018 Second International Consensus Meeting on Musculoskeletal Infection, what is the most appropriate treatment?
Explanation
61
The patient has a clinical picture concerning for infection. The patient meets major criteria for infection, as a sinus tract or two positive cultures of the same organism are necessary for diagnosis. The minor criteria for diagnosis of infection differs for acute and chronic infection, with WBC levels of 10,000 and 90% PMN. C acnes, although considered a benign contaminant in the past, is now specifically recognized as a pathogen to be treated. DAIR is considered appropriate in acute postoperative joints <3 months from surgery with symptoms occurring in <3 weeks.
The patient has a clinical picture concerning for infection. The patient meets major criteria for infection, as a sinus tract or two positive cultures of the same organism are necessary for diagnosis. The minor criteria for diagnosis of infection differs for acute and chronic infection, with WBC levels of 10,000 and 90% PMN. C acnes, although considered a benign contaminant in the past, is now specifically recognized as a pathogen to be treated. DAIR is considered appropriate in acute postoperative joints <3 months from surgery with symptoms occurring in <3 weeks.
Question 33High Yield
The patient develops painful posttraumatic arthritis and marked restriction of motion. Arthrodesis is selected as the next step in treatment. Which degree of flexion is recommended?
Explanation
Fractures of the volar base of the middle phalanx are very common injuries. After a congruent reduction, stability of the PIP joint is the most important treatment consideration. If the joint is stable, simple immobilization for comfort followed by early protected motion is adequate treatment. Clinical and cadaveric studies have demonstrated that injuries involving 20% of the volar articular surface of the middle phalanx are uniformly stable, whereas compromise of 60% of the articular surface leads to uniform instability. The threshold at which dorsal subluxation becomes problematic appears to be fractures involving 40% or more of the articular surface. Injuries of this pattern need to be examined carefully for evidence of instability and treated accordingly.
Regarding acute treatment options, extension block splinting is not recommended because of the inherent instability associated with this injury. The case in question involves a young patient; therefore, the use of primary implant arthroplasty is not the treatment of choice. In the ring finger, motion is important for power grip, so arthrodesis should be avoided if a reasonable alternative exists. Volar plate arthroplasty, although an option, has generated disappointing results for longterm joint motion and stability. Hemi-hamate arthroplasty has been described as a useful and predictable method with which to reconstruct the volar base of the middle phalanx in cases in which comminution prevents direct internal fixation. When performing hemi-hamate arthroplasty, a free osteocartilaginous graft is harvested from the dorsal and distal surface of the hamate. Using the portion of the hamate that articulates with the concave contour of the fourth to fifth
carpometacarpal joints provides a midline ridge that approximates that of the native middle phalangeal base.
Reconstruction with hemi-hamate autograft can restore the concavity of the middle phalangeal base in the anteroposterior direction. This concavity provides a volar buttress-to-dorsal subluxation of the middle phalanx. Hemi-hamate grafting is performed to the middle phalanx, not the proximal phalanx. Collateral ligament integrity is generally sacrificed to achieve adequate exposure to perform this procedure. It is not generally necessary to perform formal collateral ligament repair or reconstruction once adequate bony reconstruction is achieved. Volar plate integrity is not the primary aim of hemi-hamate arthroplasty; however, the volar plate is repaired to the middle phalangeal insertion of the collateral ligaments at the conclusion of the procedure.
Arthrodesis of the small joints of the hand is a predictable and effective method with which to control pain and instability when preservation of functional motion is not possible. This procedure offers a lower complication rate than prosthetic arthroplasty and yields satisfactory functional results. The trend is to favor arthrodesis for the radial digits and arthroplasty for the ulnar digits because of the importance of PIP flexion in the ulnar digits for power grip. Another consideration is age; younger, more active patients are more prone to eventual prosthetic failure and recurrence of digital deformity. A variety of recommendations have been made by various authors regarding the optimal position for PIP arthrodesis. The consensus is that approximately 40 degrees of flexion is optimal for the ring finger PIP joint.
RECOMMENDED READINGS
1. [Tyser AR, Tsai MA, Parks BG, Means KR Jr. Stability of acute dorsal fracture dislocations of the proximal interphalangeal joint: a biomechanical study. J Hand Surg Am. 2014 Jan;39(1):13-8. doi: 10.1016/j.jhsa.2013.09.025. Epub 2013 Nov 6. PubMed PMID: 24211175.](http://www.ncbi.nlm.nih.gov/pubmed/24211175)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24211175)
2. [Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519. ](http://www.ncbi.nlm.nih.gov/pubmed/14507519)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14507519)
3. [Capo JT, Hastings H 2nd, Choung E, Kinchelow T, Rossy W, Steinberg B. Hemicondylar hamate replacement arthroplasty for proximal interphalangeal joint fracture dislocations: an assessment of graft suitability. J Hand Surg Am. 2008 May-Jun;33(5):733-9. doi: 10.1016/j.jhsa.2008.01.012. PubMed PMID: 18590857. ](http://www.ncbi.nlm.nih.gov/pubmed/18590857)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18590857)
4. Woodworth JA, McCullough MB, Grosland NM, Adams BD. Impact of simulated proximal interphalangeal arthrodeses of all fingers on hand function. J Hand Surg Am. 2006 Jul-Aug;31(6):940-
[6/. PubMed PMID: 16843153. ](http://www.ncbi.nlm.nih.gov/pubmed/16843153)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16843153)
Regarding acute treatment options, extension block splinting is not recommended because of the inherent instability associated with this injury. The case in question involves a young patient; therefore, the use of primary implant arthroplasty is not the treatment of choice. In the ring finger, motion is important for power grip, so arthrodesis should be avoided if a reasonable alternative exists. Volar plate arthroplasty, although an option, has generated disappointing results for longterm joint motion and stability. Hemi-hamate arthroplasty has been described as a useful and predictable method with which to reconstruct the volar base of the middle phalanx in cases in which comminution prevents direct internal fixation. When performing hemi-hamate arthroplasty, a free osteocartilaginous graft is harvested from the dorsal and distal surface of the hamate. Using the portion of the hamate that articulates with the concave contour of the fourth to fifth
carpometacarpal joints provides a midline ridge that approximates that of the native middle phalangeal base.
Reconstruction with hemi-hamate autograft can restore the concavity of the middle phalangeal base in the anteroposterior direction. This concavity provides a volar buttress-to-dorsal subluxation of the middle phalanx. Hemi-hamate grafting is performed to the middle phalanx, not the proximal phalanx. Collateral ligament integrity is generally sacrificed to achieve adequate exposure to perform this procedure. It is not generally necessary to perform formal collateral ligament repair or reconstruction once adequate bony reconstruction is achieved. Volar plate integrity is not the primary aim of hemi-hamate arthroplasty; however, the volar plate is repaired to the middle phalangeal insertion of the collateral ligaments at the conclusion of the procedure.
Arthrodesis of the small joints of the hand is a predictable and effective method with which to control pain and instability when preservation of functional motion is not possible. This procedure offers a lower complication rate than prosthetic arthroplasty and yields satisfactory functional results. The trend is to favor arthrodesis for the radial digits and arthroplasty for the ulnar digits because of the importance of PIP flexion in the ulnar digits for power grip. Another consideration is age; younger, more active patients are more prone to eventual prosthetic failure and recurrence of digital deformity. A variety of recommendations have been made by various authors regarding the optimal position for PIP arthrodesis. The consensus is that approximately 40 degrees of flexion is optimal for the ring finger PIP joint.
RECOMMENDED READINGS
1. [Tyser AR, Tsai MA, Parks BG, Means KR Jr. Stability of acute dorsal fracture dislocations of the proximal interphalangeal joint: a biomechanical study. J Hand Surg Am. 2014 Jan;39(1):13-8. doi: 10.1016/j.jhsa.2013.09.025. Epub 2013 Nov 6. PubMed PMID: 24211175.](http://www.ncbi.nlm.nih.gov/pubmed/24211175)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24211175)
2. [Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519. ](http://www.ncbi.nlm.nih.gov/pubmed/14507519)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14507519)
3. [Capo JT, Hastings H 2nd, Choung E, Kinchelow T, Rossy W, Steinberg B. Hemicondylar hamate replacement arthroplasty for proximal interphalangeal joint fracture dislocations: an assessment of graft suitability. J Hand Surg Am. 2008 May-Jun;33(5):733-9. doi: 10.1016/j.jhsa.2008.01.012. PubMed PMID: 18590857. ](http://www.ncbi.nlm.nih.gov/pubmed/18590857)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18590857)
4. Woodworth JA, McCullough MB, Grosland NM, Adams BD. Impact of simulated proximal interphalangeal arthrodeses of all fingers on hand function. J Hand Surg Am. 2006 Jul-Aug;31(6):940-
[6/. PubMed PMID: 16843153. ](http://www.ncbi.nlm.nih.gov/pubmed/16843153)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16843153)
Question 34High Yield
While performing the modified Stoppa approach for fixation of an acetabular fracture, a vascular anastomosis, the “corona mortis,” will be encountered. Which 2 blood vessels contribute to this anastomosis?
Explanation
The corona mortis is a vascular anastomosis between the external iliac and the obturator vessels. It is encountered during the modified Stoppa approach, which is an exposure used for fixation of a variety of acetabular fractures. It is present in the inferior portion of the exposure during deep dissection near the superior pubic ramus. This anastomosis must be ligated to avoid excessive bleeding. The obturator and superior gluteal vessels are a branch of the internal iliac vessels.
RECOMMENDED READINGS
8. [Ponsen KJ, Joosse P, Schigt A, Goslings JC, Luitse JS. Internal fracture fixation using the Stoppa approach in pelvic ring and acetabular fractures: technical aspects and operative results. J Trauma. 2006 Sep;61(3):662-7. Erratum in: J Trauma. 2007 Jun;62(6):1490. Goslings, Carel J [corrected to Goslings, J Carel]. PubMed PMID: 16967004.](http://www.ncbi.nlm.nih.gov/pubmed/16967004)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16967004)
9. [Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified Stoppa approach for acetabular fracture. J Am Acad Orthop Surg. 2011 Mar;19(3):170-5. PubMed PMID: 21368098. ](http://www.ncbi.nlm.nih.gov/pubmed/21368098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21368098)
RESPONSES FOR QUESTIONS 41 THROUGH 44
1. Tibial and/or fibular osteotomy with open reduction and internal fixation (ORIF)
2. Ankle distraction arthroplasty
3. Ankle fusion
4. Total ankle arthroplasty (TAA)
For each scenario described below, select the most appropriate treatment listed above.
RECOMMENDED READINGS
8. [Ponsen KJ, Joosse P, Schigt A, Goslings JC, Luitse JS. Internal fracture fixation using the Stoppa approach in pelvic ring and acetabular fractures: technical aspects and operative results. J Trauma. 2006 Sep;61(3):662-7. Erratum in: J Trauma. 2007 Jun;62(6):1490. Goslings, Carel J [corrected to Goslings, J Carel]. PubMed PMID: 16967004.](http://www.ncbi.nlm.nih.gov/pubmed/16967004)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16967004)
9. [Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified Stoppa approach for acetabular fracture. J Am Acad Orthop Surg. 2011 Mar;19(3):170-5. PubMed PMID: 21368098. ](http://www.ncbi.nlm.nih.gov/pubmed/21368098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21368098)
RESPONSES FOR QUESTIONS 41 THROUGH 44
1. Tibial and/or fibular osteotomy with open reduction and internal fixation (ORIF)
2. Ankle distraction arthroplasty
3. Ankle fusion
4. Total ankle arthroplasty (TAA)
For each scenario described below, select the most appropriate treatment listed above.
Question 35High Yield
Which of the following materials is biocompatible in bulk form but may cause severe soft tissue reactions and damage in particulate form:
Explanation
Ultra-high molecular weight polyethylene is inert in bulk form but may cause severe bone loss when found in a particulate form. Wear debris that is generated at a polyethylene metal articulation is ingested by macrophages and an inflammatory response is generated. Bone resorption often results with aseptic loosening of the involved component.
C orrect Answer: Ultra-high molecular weight polyethylene
C orrect Answer: Ultra-high molecular weight polyethylene
Question 36High Yield
A 24-year-old man presents to the emergency department. He was bitten on his fist while fighting with another man. You notice teeth marks on the dorsum of the metacarpophalangeal (MC P) joint of the right middle finger. The bite does not appear to be deep because the joint is not exposed, and you can see the extensor tendon, which seems intact. The patient has active extension at the MC P joint. The wound is red and swollen, but there is no tenderness or redness on the volar aspect of the MC P joint. The patient has some limitation in range of motion. He is afebrile. Radiographs reveal soft tissue involvement but no joint dislocation or fracture, and there is no neurovascular deficit. An important step in assessment of human bites is:
Explanation
Evaluation for tendon injury in a clenched-fist position is essential because tendons slide proximally in the open-hand position. Involvement of tendon or joint usually necessitates surgical debridement.
Question 37High Yield
Slide 1
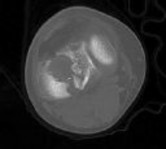
A 42-year-old man with diabetes presents for treatment of a swollen foot (Slide). He does not recall the onset of swelling, and he states that his foot is not painful. On examination, the foot is hot to touch and swollen. Upon radiographic examination, no deformities are evident. Which of the following treatment options should be used next:
A 42-year-old man with diabetes presents for treatment of a swollen foot (Slide). He does not recall the onset of swelling, and he states that his foot is not painful. On examination, the foot is hot to touch and swollen. Upon radiographic examination, no deformities are evident. Which of the following treatment options should be used next:
Explanation
This patient presents with an acute neuroarthropathy. The acute painless swelling, associated with warmth and absence of radiographic findings, is typical of the acute phase of a C harcot process. A short leg cast or a boot to immobilize the foot is ideal, and no weight bearing should be permitted until the acute phase of this neuroarthropathy has subsided.
Question 38High Yield
Which of the following blood vessels supplies the majority of the scaphoid:
Explanation
Gelberman and Menon used injection studies to demonstrate that the majority of scaphoid blood flow stems from branches of the radial artery entering the scaphoid at the distal pole. Of these, the branch entering the dorsal ridge supplies 70% to 80% of the intraosseous vascularity of the scaphoid bone. The proximal pole is completely dependent on the intraosseous blood supply and is vulnerable to avascular necrosis when fracture disrupts this vascular source.
Question 39High Yield
What part of the glenoid labrum has the least vascularity?
Explanation
The glenoid labrum receives its blood supply from the suprascapular, posterior humeral circumflex, and circumflex scapular arteries. The labral vessels arise from the capsular and periosteal vessels that penetrate the periphery of the labrum. The bone does not appear to be a source of vascularity. The posterior/superior and inferior labrum have a fairly robust vascular supply, whereas the anterior/superior labrum has relatively poor vascularity, which may influence the success of superior lateral repairs.
REFERENCE: Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
REFERENCE: Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
Question 40High Yield
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Explanation
Although management of shoulder pain in the throwing athlete is controversial, there are some general principles. Initial management generally includes rest from throwing, restoring normal joint function, specifically motion and strength as well as eliminating pain. In this patient, examination reveals excessive external rotation and decreased internal rotation. This pattern is common in pitchers; however, the total arc of motion should remain close to 180 degrees in abduction. In this patient, the total arc is 140 degrees. Treatment should first focus on restoring a 180-degree arc with posterior scapular stretching, as well as pain control and muscle rehabilitation. Injections and surgery are generally reserved for patients who fail to respond to rest and rehabilitation.
REFERENCE: Burkhart SS, Morgan CD, Kibler WB: Shoulder injuries in overhead athletes: The “dead arm” revisited. Clin Sports Med 2000;19:125-158.
REFERENCE: Burkhart SS, Morgan CD, Kibler WB: Shoulder injuries in overhead athletes: The “dead arm” revisited. Clin Sports Med 2000;19:125-158.
Question 41High Yield
Which of the following is considered an advantage of the tibial inlay fixation compared to transtibial tunnel technique when used in posterior cruciate ligament reconstruction?

Explanation
DISCUSSION: One of the most difficult aspects of posterior cruciate ligament reconstruction is placement of the tibial tunnel and passing of the graft through this tunnel. The tibial inlay technique requires a posteromedial approach to the tibia whereby the graft is directly fixed to the posterior aspect of the tibia. This obviates the need for a tibial tunnel. This technique has never been shown to be less invasive, more cosmetic,
or require decreased surgical time. It has also never been shown in a published level I study to have superior clinical results. However, it does eliminate the need for the 90-degree critical “killer” turn and passing of the tibial graft through the tibial tunnel which may lead to graft failure.
REFERENCES: McAllister DR, Petrigliano FA: Diagnosis and treatment of posterior cruciate ligament injuries. Curr Sports Med Rep 2007;6:293-299.
Cosgarea AJ, Jay PR: Posterior cruciate ligament injuries: Evaluation and management. J Am Acad Orthop Surg 2001;9:297-307.
or require decreased surgical time. It has also never been shown in a published level I study to have superior clinical results. However, it does eliminate the need for the 90-degree critical “killer” turn and passing of the tibial graft through the tibial tunnel which may lead to graft failure.
REFERENCES: McAllister DR, Petrigliano FA: Diagnosis and treatment of posterior cruciate ligament injuries. Curr Sports Med Rep 2007;6:293-299.
Cosgarea AJ, Jay PR: Posterior cruciate ligament injuries: Evaluation and management. J Am Acad Orthop Surg 2001;9:297-307.
Question 42High Yield
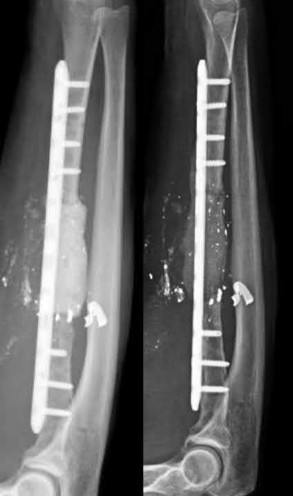
A 37-year-old male presents overnight to your busy trauma hospital after sustaining a gunshot wound to the right forearm. He is neurovascularly intact. Given the bony defect, you decide to proceed with a two-stage Masquelet technique for reconstruction. Which of the following is true with respect to this surgical technique?

Explanation
A two-stage Masquelet reconstruction technique may be used to address segmental bone loss such as that in this vignette. The induced membrane formed after the first stage will prevents the resorption of the bone graft placed during the second stage and provide a suitable environment for graft consolidation.
The Masquelet technique is a two-stage method of reconstruction of segmental bony defects resulting from trauma or following debridement of nonviable bone in the setting of infection or non-union. First described by Masquelet in 2000 for the reconstruction of tibial shaft defects, the technique has been expanded for the treatment of other bony defects including the femur, humerus, and forearm. The first stage requires debridement of devitalized or infected bone, followed by filling of the defect with an antibiotic cement spacer and provisional fixation with either external or internal fixation. In cases of infection, the patient would then undergo treatment with culture-specific antibiotics for 6 weeks and then repeat debridement (repeat stage 1) as necessary. During stage 2, the induced membrane or "pseudosynovial vascularized membrane" that forms around the cement spacer is incised and the cement spacer is removed. Autologous bone graft is then harvested (typically from either the femur or iliac crest depending on the size of the defect) and placed into the defect, followed by closure of the membrane, and placement of definitive internal fixation.
Walker et al. performed a retrospective review of 9 patients who underwent the Masquelet technique for bony defects of the forearm. Five of the patients had traumatic defects due to an acute open fracture and the other 4 had nonunions following prior ORIF. The average size of the defect was 4.7 cm. Of the 9 patients, 8 underwent bone grafting with RIA and 1 with ICBG during stage
2/. The authors found that all 9 patients went on to both clinical and radiographic union. They concluded that the Masquelet technique was successful in effectively reconstructing traumatic and posttraumatic bony defects in the forearm with a low incidence of complications.
Azi et al. present a surgical technique article on the Masquelet technique. The authors note that in the setting of infection, the antibiotic specific to the organism from the culture should be added to the cement. In culture-negative or aseptic defects, vancomycin +/- an aminoglycoside was their preferred antibiotic. They also discussed several contraindications to the Masquelet technique to include large osteochondral articular defects, prior irradiation
(given that this would impair adequate pseudomembrane formation), and soft tissue defects not amendable to bony coverage.
Micev et al. review the surgical technique of the Masquelet procedure. The authors noted that at 4 weeks, the induced membrane had the highest expression of vascular endothelial growth factor (VEGF), IL-6, and BMP-2 compared to samples taken at 6, 8 and 12 weeks. They also noted that BMP-2 production peaked at that point and gradually declined over the ensuing month. This led them to conclude that the optimal time of bone grafting to be 4 weeks after the placement of the cement spacer.
Figure A demonstrates a severely comminuted radial shaft fracture with a large bone defect.
Illustration A shows the same patient in Figure A following stage 1 of Masquelet (left) with debridement, placement of a cement spacer and internal fixation; on the right is the same patient following stage 2 with bone grafting.
Incorrect Answers:
Answer 1: The Masquelet technique is not appropriate for large articular defects, which may necessitate other advanced reconstruction techniques such as bulk allograft or prosthetic replacement.
Answer 2: Both femoral RIA and ICBG are the two most commonly used sources of autograft for the second stage of the Masquelet technique, however there is no evidence demonstrating superiority of one over the other.
Answer 3: The optimal timing of stage 2 of the Masquelet technique is 4 to 6 weeks following stage 1, given that this is the time at which the highest amount of BMPs, VEGF and IL-6 are expressed from the induced membrane. Answer 5: While culture-specific antibiotics are recommended for stage 1 in the setting of infected non-union, in the cases of acute bony defects or even aseptic nonunion, this may not be necessary. However antibiotics have not been found to affect pseudomembrane formation.
The Masquelet technique is a two-stage method of reconstruction of segmental bony defects resulting from trauma or following debridement of nonviable bone in the setting of infection or non-union. First described by Masquelet in 2000 for the reconstruction of tibial shaft defects, the technique has been expanded for the treatment of other bony defects including the femur, humerus, and forearm. The first stage requires debridement of devitalized or infected bone, followed by filling of the defect with an antibiotic cement spacer and provisional fixation with either external or internal fixation. In cases of infection, the patient would then undergo treatment with culture-specific antibiotics for 6 weeks and then repeat debridement (repeat stage 1) as necessary. During stage 2, the induced membrane or "pseudosynovial vascularized membrane" that forms around the cement spacer is incised and the cement spacer is removed. Autologous bone graft is then harvested (typically from either the femur or iliac crest depending on the size of the defect) and placed into the defect, followed by closure of the membrane, and placement of definitive internal fixation.
Walker et al. performed a retrospective review of 9 patients who underwent the Masquelet technique for bony defects of the forearm. Five of the patients had traumatic defects due to an acute open fracture and the other 4 had nonunions following prior ORIF. The average size of the defect was 4.7 cm. Of the 9 patients, 8 underwent bone grafting with RIA and 1 with ICBG during stage
2/. The authors found that all 9 patients went on to both clinical and radiographic union. They concluded that the Masquelet technique was successful in effectively reconstructing traumatic and posttraumatic bony defects in the forearm with a low incidence of complications.
Azi et al. present a surgical technique article on the Masquelet technique. The authors note that in the setting of infection, the antibiotic specific to the organism from the culture should be added to the cement. In culture-negative or aseptic defects, vancomycin +/- an aminoglycoside was their preferred antibiotic. They also discussed several contraindications to the Masquelet technique to include large osteochondral articular defects, prior irradiation
(given that this would impair adequate pseudomembrane formation), and soft tissue defects not amendable to bony coverage.
Micev et al. review the surgical technique of the Masquelet procedure. The authors noted that at 4 weeks, the induced membrane had the highest expression of vascular endothelial growth factor (VEGF), IL-6, and BMP-2 compared to samples taken at 6, 8 and 12 weeks. They also noted that BMP-2 production peaked at that point and gradually declined over the ensuing month. This led them to conclude that the optimal time of bone grafting to be 4 weeks after the placement of the cement spacer.
Figure A demonstrates a severely comminuted radial shaft fracture with a large bone defect.
Illustration A shows the same patient in Figure A following stage 1 of Masquelet (left) with debridement, placement of a cement spacer and internal fixation; on the right is the same patient following stage 2 with bone grafting.
Incorrect Answers:
Answer 1: The Masquelet technique is not appropriate for large articular defects, which may necessitate other advanced reconstruction techniques such as bulk allograft or prosthetic replacement.
Answer 2: Both femoral RIA and ICBG are the two most commonly used sources of autograft for the second stage of the Masquelet technique, however there is no evidence demonstrating superiority of one over the other.
Answer 3: The optimal timing of stage 2 of the Masquelet technique is 4 to 6 weeks following stage 1, given that this is the time at which the highest amount of BMPs, VEGF and IL-6 are expressed from the induced membrane. Answer 5: While culture-specific antibiotics are recommended for stage 1 in the setting of infected non-union, in the cases of acute bony defects or even aseptic nonunion, this may not be necessary. However antibiotics have not been found to affect pseudomembrane formation.
Question 43High Yield
A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
Explanation
DISCUSSION:
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower resurgical rate; one- quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again
superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed
reduction and percutaneous pinning studies have not been published on the adult population.
DISCUSSION:
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower resurgical rate; one- quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again
superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed
reduction and percutaneous pinning studies have not been published on the adult population.
Question 44High Yield
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy?
Explanation
Various factors affect the pseudarthrosis rate in patients who undergo anterior cervical decompression and fusion. Patient factors, including history of smoking and history of diabetes mellitus,have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category,there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
Question 45High Yield
Slide 1
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
Explanation
The extensor hallucis longus or the extensor hallucis brevis (rarely the abductor hallucis) may be used as a tendon transfer for correction. Arthrodesis of the hallux interphalangeal joint may be performed for correction of a fixed claw deformity of the interphalangeal joint, usually in conjunction with a tendon transfer. Arthrodesis of the metatarsophalangeal joint is a reasonable alternative provided there is no fixed deformity of the interphalangeal joint present and when arthritis or fixed deformity of the metatarsophalangeal joint is present.
Question 46High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
After a discussion with the patient, surgery is chosen for the right humerus. A posterior triceps-reflecting approach is selected. What structure marks the most proximal extent of the humerus that can be exposed through this approach?
---
---
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
After a discussion with the patient, surgery is chosen for the right humerus. A posterior triceps-reflecting approach is selected. What structure marks the most proximal extent of the humerus that can be exposed through this approach?
---
---


Explanation
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate
early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 47High Yield
A 60-year-old woman has progressive neck pain, upper extremity pain, and paresthesias. A lateral cervical spine radiograph and an MRI scan are shown in Figures 52a and 52b. What is the most likely underlying diagnosis?
---
---
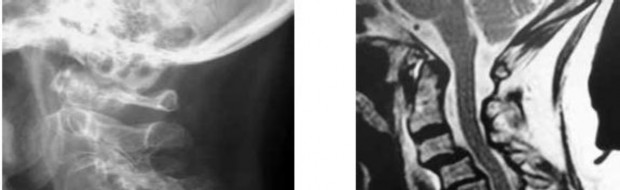
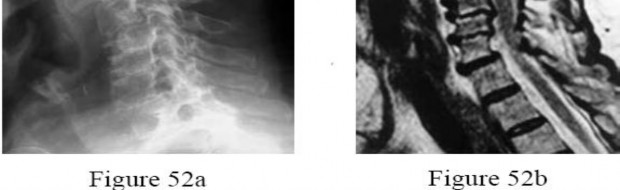
Explanation
The radiograph and sagittal T2-weighted MRI scan show multilevel degenerative changes and subaxial subluxations with anterolisthesis at C3-C4 and C4-C5 and retrolisthesis at C5-C6. In addition, there is evidence of midcervical kyphosis. Such findings are often seen in patients with rheumatoid arthritis. Patients with osteomyelitis typically show increased signal intensity in the disks and vertebral bodies. Patients with ankylosing spondylitis typically show ankylosis of the disks and vertebral
bodies. Age-related degenerative changes typically manifest as degenerative disk disease with occasional single-level spondylolisthesis, but not typically multilevel spondylolisthesis, as seen in this patient. The spinous processes are intact; these changes do not appear to be postoperative.
bodies. Age-related degenerative changes typically manifest as degenerative disk disease with occasional single-level spondylolisthesis, but not typically multilevel spondylolisthesis, as seen in this patient. The spinous processes are intact; these changes do not appear to be postoperative.
Question 48High Yield
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
Explanation
of the mechanism mediating this effect. Whereas all of the above have been postulated as explanations, more recent studies have
demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
Question 49High Yield
Initial treatment for this condition should include
Explanation
- activity modification and therapy to support the lumbar musculature.
Question 50High Yield
Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?
Explanation
The patient has osteochondritis dissecans. While location, size, and knee stability are all relevant to the overall prognosis, studies have shown that younger patients with open growth plates have a better prognosis of healing when compared with patients who have closed growth plates. The degree of pain is also relevant to treatment, but it is subjective rather than objective and is not as reliable of a prognostic indicator as age.
REFERENCES: Stanitski CL: Osteochondritis dissecans of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 387-405.
Cahill B: Treatment of juvenile osteochondritis dissecans and osteochondritis dissecans of the knee. Clin Sports Med 1985;4:367-384.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
REFERENCES: Stanitski CL: Osteochondritis dissecans of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 387-405.
Cahill B: Treatment of juvenile osteochondritis dissecans and osteochondritis dissecans of the knee. Clin Sports Med 1985;4:367-384.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon