Shoulder And Elbow: And Emqs A Review | Dr Hutaif Shoul -...
14 Apr 2026
133 min read
82 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Shoulder And Elbow: And Emqs A Review | Dr Hu...
00:00
Start Quiz
Question 1High Yield
Slide 1 Slide 2 Slide 3
A patient with diabetes and severe peripheral neuropathy has been treated for a C harcot ankle deformity for 9 months (Slide 1, Slide 2, and Slide 3). An ankle foot orthosis has been used for 4 months. No skin breakdown occurred in the brace. Swelling is present but has decreased over the past month. Ankle range of motion is limited, and crepitus is present upon examination of the ankle. Which surgical procedure is most consistent with the future treatment of this patient:
A patient with diabetes and severe peripheral neuropathy has been treated for a C harcot ankle deformity for 9 months (Slide 1, Slide 2, and Slide 3). An ankle foot orthosis has been used for 4 months. No skin breakdown occurred in the brace. Swelling is present but has decreased over the past month. Ankle range of motion is limited, and crepitus is present upon examination of the ankle. Which surgical procedure is most consistent with the future treatment of this patient:
Explanation
The indication for surgery is intractable deformity, which is refractory to all forms of bracing. By refractory, one implies that skin breakdown or imminent infection is present. If surgery were performed, then it would consist of a tibiotalocalcaneal arthrodesis. There are no indications for this surgery in this patient. Once the neuropathic process has reached a stable point, a deformity is not likely to progress.
Question 2High Yield
Treatment for this injury can be surgical or nonsurgical. Which outcome is more likely with surgical treatment?
Explanation
- Wound-healing problems_
Question 3High Yield
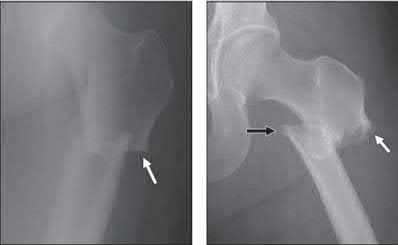
A 70-year-old female presents with right thigh ache for 6 months. Except for a history of osteoporosis, she is otherwise healthy. She has been on antiresorptive therapy for 8 years. Her radiograph is shown in Figure A. Four months later, she trips over a rug and falls, sustaining the injury shown in Figures B and C. Which of these statements is TRUE regarding surgical fixation of this fracture compared with conventional fractures?





Explanation
This patient has a bisphosphonate-related (BP) fracture. There is increased risk of iatrogenic fracture with IM nailing of this fracture.
Subtrochanteric fractures are fractures extending from the lesser trochanter to 5cm distal to it. BP fractures are characterized by (1) focal lateral cortical thickening, (2) transverse fracture orientation, (3) medial spike and (4) lack of comminution. There is increased risk of iatrogenic fracture with IM nailing because BP fractures have thickened, brittle cortices and the mismatch between medullary diameter and increased proximal nail diameter results in iatrogenic fracture.
Weil et al. reviewed the outcome of surgically treated bisphosphonate fractures. IM nailing resulted in healing in 54% of bisphosphonate fractures
with 98-99% of conventional fractures. In their study, 46% required revision procedures.
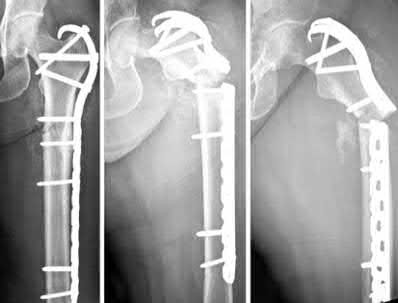
Prasarn et al. compared plate and nail treated bisphosphonate fractures with conventional fractures. They found that the bisphosphonate group had more major and minor complications (68%) than the conventional group (10%). The most common complications were intraoperative femoral shaft comminution (nail) and hardware failure (plate).
Figure A shows diffuse cortical thickening with an antero-lateral cortical ridge. Figure B shows a transverse subtrochanteric fracture extending through the middle of the cortical ridge seen previously. Note also healed fractures of the left superior and inferior rami. Figure C is a post-reduction radiograph showing the transverse fracture through the beak-shaped region of the previous insufficiency fracture. Illustration A shows a typical bisphosphonate-related fracture with transverse fracture orientation, focal lateral cortical thickening (white arrows), medial beak (black arrow), and lack of comminution.
Illustration B shows a conventional subtrochanteric fracture. Illustration C shows intraoperative iatrogenic fracture with anterolateral comminution during nailing. Illustration D shows fixation with a proximal femoral hook LCP Plate with late hardware failure at 3 months.
Incorrect Answers:
Answers 1, 3: Increased non-union after IM nailing has been observed, necessitating more revision surgery compared with conventional fractures. Revision surgery includes nail dynamization, exchange nailing, and conversion to plating. These procedures are more frequently performed for osteoporotic fractures.
Answer 2: Compared with conventional fractures, there is no increased risk of iatrogenic fracture with plating.
Answer 5: There is an increased risk of plate hardware failure because of because of a varus moment arm and dependence on intramembranous healing inhibited by bisphosphonates.
Subtrochanteric fractures are fractures extending from the lesser trochanter to 5cm distal to it. BP fractures are characterized by (1) focal lateral cortical thickening, (2) transverse fracture orientation, (3) medial spike and (4) lack of comminution. There is increased risk of iatrogenic fracture with IM nailing because BP fractures have thickened, brittle cortices and the mismatch between medullary diameter and increased proximal nail diameter results in iatrogenic fracture.
Weil et al. reviewed the outcome of surgically treated bisphosphonate fractures. IM nailing resulted in healing in 54% of bisphosphonate fractures
with 98-99% of conventional fractures. In their study, 46% required revision procedures.
Prasarn et al. compared plate and nail treated bisphosphonate fractures with conventional fractures. They found that the bisphosphonate group had more major and minor complications (68%) than the conventional group (10%). The most common complications were intraoperative femoral shaft comminution (nail) and hardware failure (plate).
Figure A shows diffuse cortical thickening with an antero-lateral cortical ridge. Figure B shows a transverse subtrochanteric fracture extending through the middle of the cortical ridge seen previously. Note also healed fractures of the left superior and inferior rami. Figure C is a post-reduction radiograph showing the transverse fracture through the beak-shaped region of the previous insufficiency fracture. Illustration A shows a typical bisphosphonate-related fracture with transverse fracture orientation, focal lateral cortical thickening (white arrows), medial beak (black arrow), and lack of comminution.
Illustration B shows a conventional subtrochanteric fracture. Illustration C shows intraoperative iatrogenic fracture with anterolateral comminution during nailing. Illustration D shows fixation with a proximal femoral hook LCP Plate with late hardware failure at 3 months.
Incorrect Answers:
Answers 1, 3: Increased non-union after IM nailing has been observed, necessitating more revision surgery compared with conventional fractures. Revision surgery includes nail dynamization, exchange nailing, and conversion to plating. These procedures are more frequently performed for osteoporotic fractures.
Answer 2: Compared with conventional fractures, there is no increased risk of iatrogenic fracture with plating.
Answer 5: There is an increased risk of plate hardware failure because of because of a varus moment arm and dependence on intramembranous healing inhibited by bisphosphonates.
Question 4High Yield
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?**
Explanation
The patient has a global loss of motion that has failed to improve with 6 months of nonsurgical treatment; because he has reached a plateau, further nonsurgical management will likely be ineffective. Revision in the form of an open release is indicated to lyse intra- and extra-articular adhesions; subscapularis lengthening may be done concurrently as needed. Revising to a smaller head can be considered if adequate motion is not achieved. The radiographs reveal an adequate neck cut with appropriate seating of the component. Removing the glenoid component will decrease capsular tension but will probably increase pain because of the lack of glenoid resurfacing. Increasing humeral retroversion will not improve motion.
REFERENCES: Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
REFERENCES: Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 5High Yield
Which surgical approach is less useful for children who have reached walking age because it does not allow for capsulorrhaphy?
Explanation
- Medial_
Question 6High Yield
-A 41-year-old man is involved in a high-speed motor vehicle crash and sustains a closed femoral midshaft fracture and a unilateral pulmonary contusion with a hemothorax, requiring placement of a chest tube.He has an initial blood pressure of 90/50 mm Hg. After receiving two liters of crystalloid, he has a blood pressure of 115/70 mm Hg and a heart rate of 90 bpm. He has normal mentation and does not require ventilator support. An arterial blood gas reveals that his delta base is -2 mmol/L. What is the most appropriate treatment for his femoral fracture?
Explanation
No detailed explanation provided for this question.
Question 7High Yield
Marjolinâs ulcers are risk factors for which of the following tumors:
Explanation
Marjolinâs ulcers are malignant degenerations in chronic skin ulcers, sinuses, and burn scars and are risk factors for squamous cell carcinoma. Any patient with chronic, nonhealing ulcers should undergo biopsy for malignant degeneration. Basal cell carcinoma, malignant melanoma, synovial sarcoma, and osteosarcoma are not commonly associated with Marjolin's ulcer.
Question 8High Yield
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
Internal impingement of the shoulder is a leading cause of shoulder pain in the throwing athlete. The primary lesion in pathologic internal impingement is excessive tightening of the posterior band of the inferior glenohumeral ligament complex. To obtain an accurate assessment of true glenohumeral rotation, the scapula is stabilized during examination. A loss of 20 degrees or more of internal rotation, as measured with the shoulder positioned in 90 degrees of abduction, indicates excessive tightness of the posterior band of the inferior glenohumeral ligament complex.
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
Question 9High Yield
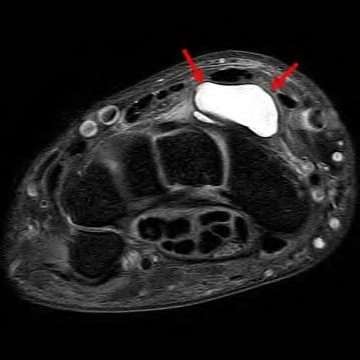
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
1. [Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. ](http://www.ncbi.nlm.nih.gov/pubmed/21823110)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21823110)
2. Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. _Enzinger & Weiss’s Soft Tissue Tumors_. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
3. [Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/27267143)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/27267143)
4. [Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. ](http://www.ncbi.nlm.nih.gov/pubmed/26222558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26222558)
5. [Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.](http://www.ncbi.nlm.nih.gov/pubmed/24898549)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24898549)
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
1. [Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. ](http://www.ncbi.nlm.nih.gov/pubmed/21823110)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21823110)
2. Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. _Enzinger & Weiss’s Soft Tissue Tumors_. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
3. [Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/27267143)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/27267143)
4. [Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. ](http://www.ncbi.nlm.nih.gov/pubmed/26222558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26222558)
5. [Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.](http://www.ncbi.nlm.nih.gov/pubmed/24898549)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24898549)
Question 10High Yield
volar tenderness along the flexor sheath
Patients commonly present 24 to 48 hours after onset of symptoms. The standard of care is “urgent surgical drainage” to avoid tendon scarring or necrosis with subsequent impairment of finger function followed by intravenous antibiotic administration.
According to Hand Surgery Update 3, open sheath irrigation has been replaced
largely by closed sheath irrigation. These authors cite a retrospective study that showed no statistical difference in resolution of infection using open sheath irrigation or closed sheath irrigation, however, there was a trend towards more frequent complications and reoperations in the open drainage group.
Lille et al reviewed the records of 75 patients with pyogenic flexor tenosynovitis and found that there was no difference in outcomes between those who received intraoperative irrigation only versus those receiving intraoperative irrigation and continuous postoperative irrigation.
A 50-year-old woman is diagnosed with carpal tunnel syndrome. She is prescribed a cock-up wrist splint at 30 degrees of extension to wear at night. This splint has what effect on the carpal tunnel?
Patients commonly present 24 to 48 hours after onset of symptoms. The standard of care is “urgent surgical drainage” to avoid tendon scarring or necrosis with subsequent impairment of finger function followed by intravenous antibiotic administration.
According to Hand Surgery Update 3, open sheath irrigation has been replaced
largely by closed sheath irrigation. These authors cite a retrospective study that showed no statistical difference in resolution of infection using open sheath irrigation or closed sheath irrigation, however, there was a trend towards more frequent complications and reoperations in the open drainage group.
Lille et al reviewed the records of 75 patients with pyogenic flexor tenosynovitis and found that there was no difference in outcomes between those who received intraoperative irrigation only versus those receiving intraoperative irrigation and continuous postoperative irrigation.
A 50-year-old woman is diagnosed with carpal tunnel syndrome. She is prescribed a cock-up wrist splint at 30 degrees of extension to wear at night. This splint has what effect on the carpal tunnel?





























Explanation
No detailed explanation provided for this question.
Question 11High Yield
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
In a young individual with a chronic dislocation of the elbow and heterotopic bone formation, the treatment of choice is open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a dynamic hinged fixator to begin protected early postoperative range of motion. It is important to understand that the fixator protects the reconstruction and allows early range of motion, but it does not maintain the reduction and should not be expected to do so. Pin fixation across the elbow delays early motion and is not recommended. Total elbow arthroplasty is not indicated, and ulnohumeral arthroplasty is for a primary arthritic condition.
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 12High Yield
A
B
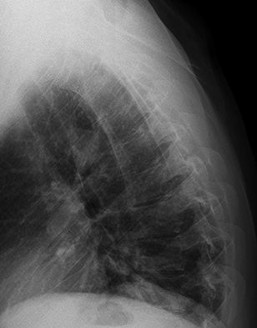
Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?
B
Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?

Explanation
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
RECOMMENDED READINGS
[Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. ](http://www.ncbi.nlm.nih.gov/pubmed/20421858)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20421858)
[Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. ](http://www.ncbi.nlm.nih.gov/pubmed/8141015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8141015)
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
RECOMMENDED READINGS
[Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. ](http://www.ncbi.nlm.nih.gov/pubmed/20421858)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20421858)
[Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. ](http://www.ncbi.nlm.nih.gov/pubmed/8141015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8141015)
Question 13High Yield
Evidence of cementless acetabular implant loosening is radiographically observed as:
Explanation
Of the choices listed, only radiolucency provides evidence of acetabular loosening. CystiClesions, known as osteolysis, may exist without the presence of loosening
Question 14High Yield
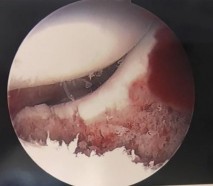
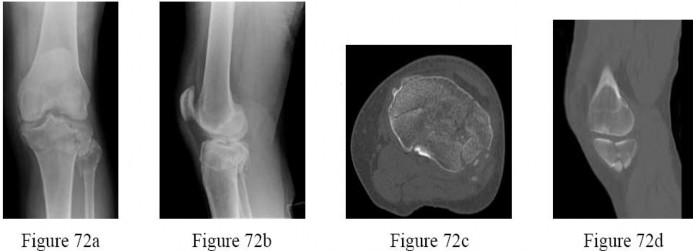
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
---
---
---
---
---
---
---
---



Explanation
The images show a full-thickness cartilage defect with significant bony involvement >4 cm2. Microfracture should be considered for lesions <2 cm2 without an underlying osseous defect. Autologous chondrocyte implantation, although used for lesions between 1 and 10 cm2, should be restricted for defects with minimal (<8 mm depth) bone loss. Osteochondral allograft transfer with the mosaicplasty technique (transfer of multiple plugs) would be well-suited for this large defect with significant osseous involvement. Dejour trochleoplasty is performed for patellar instability to correct trochlear dysplasia and _would not be indicated in this case._
Question 15High Yield
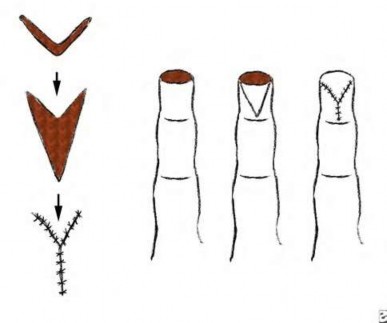
Figure 60a is the radiograph of an 18-year-old right-hand-dominant man who has pain and stiffness 3 months after sustaining an injury to his dominant ring finger while playing basketball. An examination reveals significant proximal interphalangeal (PIP) joint swelling with active and passive PIP joint motion of 15/40 degrees of flexion. What is the best next step?


Explanation
This patient has a subacute PIP joint dorsal fracture dislocation with involvement of 50% to 60% of the palmar articular surface of the base of P2. A “V sign” (Figure 60b) is evident, indicating
dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress.
Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 60c through 60e.
RECOMMENDED READINGS
16. Calfee RP, Kiefhaber TR, Sommerkamp TG, Stern PJ. Hemi-hamate arthroplasty provides functional reconstruction of acute and chronic proximal interphalangeal fracture-dislocations. J Hand Surg Am. 2009 Sep;34(7):1232-41. doi: 10.1016/j.jhsa.2009.04.027. PubMed PMID: 19700071.
17. Frueh FS, Calcagni M, Lindenblatt N. The hemi-hamate autograft arthroplasty in proximal interphalangeal joint reconstruction: a systematic review. J Hand Surg Eur Vol. 2015 Jan;40(1):24-32. doi: 10.1177/1753193414554356. Epub 2014 Oct 22. Review. PubMed PMID: 25342651.
18. Williams RM, Hastings H 2nd, Kiefhaber TR. PIP Fracture/Dislocation Treatment Technique: Use of a Hemi-Hamate Resurfacing Arthroplasty. Tech Hand Up Extrem Surg. 2002 Dec;6(4):185-92. PubMed PMID: 16520599.
19. Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519.
dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress.
Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 60c through 60e.
RECOMMENDED READINGS
16. Calfee RP, Kiefhaber TR, Sommerkamp TG, Stern PJ. Hemi-hamate arthroplasty provides functional reconstruction of acute and chronic proximal interphalangeal fracture-dislocations. J Hand Surg Am. 2009 Sep;34(7):1232-41. doi: 10.1016/j.jhsa.2009.04.027. PubMed PMID: 19700071.
17. Frueh FS, Calcagni M, Lindenblatt N. The hemi-hamate autograft arthroplasty in proximal interphalangeal joint reconstruction: a systematic review. J Hand Surg Eur Vol. 2015 Jan;40(1):24-32. doi: 10.1177/1753193414554356. Epub 2014 Oct 22. Review. PubMed PMID: 25342651.
18. Williams RM, Hastings H 2nd, Kiefhaber TR. PIP Fracture/Dislocation Treatment Technique: Use of a Hemi-Hamate Resurfacing Arthroplasty. Tech Hand Up Extrem Surg. 2002 Dec;6(4):185-92. PubMed PMID: 16520599.
19. Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519.
Question 16High Yield
First metatarsophalangeal prosthetic joint replacements:
Explanation
First metatarsophalangeal joint replacement in this prospective comparative study performed poorly compared to arthrodesis. Patients with arthroplasties had greater pain and little improvement in range of motion.
Question 17High Yield
A 44-year-old man who sustained an elbow dislocation 3 months ago now reports pain and restricted elbow motion. Radiographs are shown in Figures 27a and 27b. Management should consist of
Explanation
The treatment of choice for an ankylosed chronically dislocated elbow is surgical reduction. Open reduction with application of an external fixator provides excellent results for this complex problem. Radial head arthroplasty is indicated for a radial head fracture that cannot be reconstructed. Attempts at closed reduction will be unsuccessful and should not be attempted in a stiff elbow. In chronic dislocations, direct reinsertion of injured ligaments is not feasible because of soft-tissue contracture.
REFERENCES: Jupiter J, Ring D: Treatment of unreduced elbow dislocation with hinged external fixation. J Bone Joint Surg Am 2002;84:1630-1635.
Moro JK, Werier J, MacDermid JC, et al: Arthroplasty with a metal radial head for unreconstructible fractures of the radial head. J Bone Joint Surg Am 2001;83:1201-1211.
REFERENCES: Jupiter J, Ring D: Treatment of unreduced elbow dislocation with hinged external fixation. J Bone Joint Surg Am 2002;84:1630-1635.
Moro JK, Werier J, MacDermid JC, et al: Arthroplasty with a metal radial head for unreconstructible fractures of the radial head. J Bone Joint Surg Am 2001;83:1201-1211.
Question 18High Yield
Osteoid osteoma with 1 year of symptoms
Explanation
- Cortical thickening in the region of the lesion
Question 19High Yield
A 58-year-old man has had increasing midback pain for 8 weeks. Radiographs reveal mild osteopenia and mild disk degeneration but no fractures or lesions. An MRI of the spine reveals diskitis with a small-intensity signal within the spinal canal that is consistent with an epidural abscess at T11-12. The patient is neurologically intact but in significant pain. CT-guided biopsy of the disk space is positive for methicillin-sensitive Staphylococcus aureus. What is the most appropriate treatment?
Explanation
The treatment of spinal infections is variable. A diskitis in a patient with a mechanically stable spine without neurologic compromise is typically treated with needle biopsy/culture and appropriate IV antibiotics. Epidural abscess often is considered one of the true orthopaedic emergencies that necessitates surgical intervention. However, there is growing evidence that medical management can be appropriate to treat epidural abscesses in certain cases. In cases involving neurologic deterioration, surgical decompression, drainage, and systemic IV antibiotics is the treatment of choice. Medical management of spinal abscesses can be considered when a patient refuses surgical decompression; surgery is contraindicated because of high risk, pain, or
infection; or paralysis lasting longer than 24 to 36 hours results in a likely inability to reverse the paralysis. Patients who are neurologically intact may also be treated with medical management alone if they are stable and have an identifiable microorganism that can be observed closely to assess for neurologic deterioration. If neurologic changes are noted, surgical decompression and debridement and continued IV antibiotic therapy are appropriate.
RECOMMENDED READINGS
[Darouiche RO. Spinal epidural abscess. N Engl J Med. 2006 Nov 9;355(19):2012-20. Review. PubMed PMID: 17093252.](http://www.ncbi.nlm.nih.gov/pubmed/17093252)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17093252)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683.](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. Review. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
[Siddiq F, Chowfin A, Tight R, Sahmoun AE, Smego RA Jr. Medical vs surgical management of spinal epidural abscess. Arch Intern Med. 2004 Dec 13-27;164(22):2409-12. PubMed PMID: 15596629. ](http://www.ncbi.nlm.nih.gov/pubmed/15596629)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15596629)
infection; or paralysis lasting longer than 24 to 36 hours results in a likely inability to reverse the paralysis. Patients who are neurologically intact may also be treated with medical management alone if they are stable and have an identifiable microorganism that can be observed closely to assess for neurologic deterioration. If neurologic changes are noted, surgical decompression and debridement and continued IV antibiotic therapy are appropriate.
RECOMMENDED READINGS
[Darouiche RO. Spinal epidural abscess. N Engl J Med. 2006 Nov 9;355(19):2012-20. Review. PubMed PMID: 17093252.](http://www.ncbi.nlm.nih.gov/pubmed/17093252)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17093252)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683.](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. Review. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
[Siddiq F, Chowfin A, Tight R, Sahmoun AE, Smego RA Jr. Medical vs surgical management of spinal epidural abscess. Arch Intern Med. 2004 Dec 13-27;164(22):2409-12. PubMed PMID: 15596629. ](http://www.ncbi.nlm.nih.gov/pubmed/15596629)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15596629)
Question 20High Yield
The most appropriate course of treatment is
Explanation
- hemi-hamate arthroplasty._
Question 21High Yield
If growth arrest is suspected after the fracture shown in the radiographs in Figures 17a through 17c, what is the most appropriate imaging modality to verify the presence of a physeal bar?



Explanation
Premature growth arrest of a physis may occur after fracture, infection, or ischemia. In the setting of fracture this is relatively rare, although certain physes have proven more susceptible than others. In the distal radius, premature growth arrest is more common after wide displacement, redisplacement, or manipulation after a fracture has begun to heal (> 7-10 days after injury). Arrest may take 6 to 12 months to become evident on radiographs and it may take even longer for a patient to experience pain or deformity, depending upon the rate of growth at the time of arrest. Surveillance should take place during the 6- to 12-month time frame with radiographs.
A physeal bar is difficult to rule in or out on radiographs because of natural undulations in the physis or a residual angular deformity after fracture that causes the physis to be less clearly visible. Often, the best clue that indicates physeal arrest after distal radius fracture is clinical prominence of the ulna head or increasing ulna-positive variance. The posteroanterior view of the wrist should be taken with the shoulder abducted to 90 degrees and elbow flexed to 90 degrees. This places the forearm in neutral rotation, and changes in ulnar variance can more accurately be detected. Comparison views of the other side may be warranted.
If a growth arrest is suspected, CT scan and MRI are both effective modalities for imaging the size and location of the bar. The bar is most easily detected on the T1-weighted MR images. Early, unossified cartilaginous bars also may be detected on some MRI sequences. MRI with 3D mapping functions is now used to map the size and location into an easy-to-visualize format, but the computer programs are not yet mainstream. A CT scan can demonstrate the bar but is not as acceptable because of the high dose of radiation (compared to MRI).
The physis has 3 main zones. The zone that is most important and susceptible to injury is the resting zone, where pluripotent chondrocytes reside. This layer is immediately adjacent to the epiphysis. If this layer is disrupted or ischemic, there is permanent growth arrest of that physis section. The central layer is the proliferative zone. The hypertrophic zone is the layer adjacent to the metaphysis and is subdivided into 3 layers: maturation, degeneration, and provisional calcification. The weakest link is the junction between the provisional calcification layer and the metaphysis. Most physeal fractures occur through this layer. Thus, growth arrest after fracture is rare because the level of injury typically is as far as possible from the delicate resting zone.
If growth arrest occurs after distal radius fracture, surgical intervention is tailored to the situation. If the child is young, an attempt at bar resection and interposition of fat or bone wax is appropriate. If a teenage child is asymptomatic and ulna variance is a few millimeters positive, simple ulna epiphysiodesis is appropriate. If there is deformity of the distal radius, corrective osteotomy may be best.
RECOMMENDED READINGS
6. [Abzug JM, Little K, Kozin SH. Physeal arrest of the distal radius. J Am Acad Orthop Surg. 2014 Jun;22(6):381-9. doi: 10.5435/JAAOS-22-06-381. Review. PubMed PMID: 24860134. ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860134)
7. [Craig JG, Cramer KE, Cody DD, Hearshen DO, Ceulemans RY, van Holsbeeck MT, Eyler WR. Premature partial closure and other deformities of the growth plate: MR imaging and three-dimensional modeling. Radiology. 1999 Mar;210(3):835-43. PubMed PMID: 10207489. ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10207489)
8. [Ecklund K, Jaramillo D. Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol. 2002 Apr;178(4):967-72. PubMed PMID: 11906884. ](http://www.ncbi.nlm.nih.gov/pubmed/11906884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11906884)
A physeal bar is difficult to rule in or out on radiographs because of natural undulations in the physis or a residual angular deformity after fracture that causes the physis to be less clearly visible. Often, the best clue that indicates physeal arrest after distal radius fracture is clinical prominence of the ulna head or increasing ulna-positive variance. The posteroanterior view of the wrist should be taken with the shoulder abducted to 90 degrees and elbow flexed to 90 degrees. This places the forearm in neutral rotation, and changes in ulnar variance can more accurately be detected. Comparison views of the other side may be warranted.
If a growth arrest is suspected, CT scan and MRI are both effective modalities for imaging the size and location of the bar. The bar is most easily detected on the T1-weighted MR images. Early, unossified cartilaginous bars also may be detected on some MRI sequences. MRI with 3D mapping functions is now used to map the size and location into an easy-to-visualize format, but the computer programs are not yet mainstream. A CT scan can demonstrate the bar but is not as acceptable because of the high dose of radiation (compared to MRI).
The physis has 3 main zones. The zone that is most important and susceptible to injury is the resting zone, where pluripotent chondrocytes reside. This layer is immediately adjacent to the epiphysis. If this layer is disrupted or ischemic, there is permanent growth arrest of that physis section. The central layer is the proliferative zone. The hypertrophic zone is the layer adjacent to the metaphysis and is subdivided into 3 layers: maturation, degeneration, and provisional calcification. The weakest link is the junction between the provisional calcification layer and the metaphysis. Most physeal fractures occur through this layer. Thus, growth arrest after fracture is rare because the level of injury typically is as far as possible from the delicate resting zone.
If growth arrest occurs after distal radius fracture, surgical intervention is tailored to the situation. If the child is young, an attempt at bar resection and interposition of fat or bone wax is appropriate. If a teenage child is asymptomatic and ulna variance is a few millimeters positive, simple ulna epiphysiodesis is appropriate. If there is deformity of the distal radius, corrective osteotomy may be best.
RECOMMENDED READINGS
6. [Abzug JM, Little K, Kozin SH. Physeal arrest of the distal radius. J Am Acad Orthop Surg. 2014 Jun;22(6):381-9. doi: 10.5435/JAAOS-22-06-381. Review. PubMed PMID: 24860134. ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860134)
7. [Craig JG, Cramer KE, Cody DD, Hearshen DO, Ceulemans RY, van Holsbeeck MT, Eyler WR. Premature partial closure and other deformities of the growth plate: MR imaging and three-dimensional modeling. Radiology. 1999 Mar;210(3):835-43. PubMed PMID: 10207489. ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10207489)
8. [Ecklund K, Jaramillo D. Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol. 2002 Apr;178(4):967-72. PubMed PMID: 11906884. ](http://www.ncbi.nlm.nih.gov/pubmed/11906884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11906884)
Question 22High Yield
What percent of the adult human meniscus is vascularized?
Explanation
The adult menisci are considered to be relatively avascular structures, with the peripheral blood supply originating predominately from the lateral and medial genicular arteries. Branches of these vessels form the perimeniscal capillary plexus, which supplies the peripheral border throughout its attachment to the joint capsule. Vascular penetration studies have shown that 10% to 30% of the peripheral portion of the medial meniscus and 10% to 25% of the lateral meniscus are vascularized.
REFERENCES: Arnoczky SP, Warren RF: Microvasculature of the human meniscus. Am J Sports Med 1982;10:90-95.
Arnoczky SP, Warren RF: The microvasculature of the meniscus and its response to injury: An experimental study in the dog. Am J Sports Med 1983;11:131-141.
REFERENCES: Arnoczky SP, Warren RF: Microvasculature of the human meniscus. Am J Sports Med 1982;10:90-95.
Arnoczky SP, Warren RF: The microvasculature of the meniscus and its response to injury: An experimental study in the dog. Am J Sports Med 1983;11:131-141.
Question 23High Yield
Which of the following is most important to achieve a good outcome following a Syme amputation?
Explanation
A Syme amputation is effectively a tibiotalar disarticulation, which provides an end-bearing stump that could potentially allow ambulation without a prosthesis over short distances. It works better for tumor and trauma, but the heel pad must be viable. The two most common problems are 1) skin sloughing from compromised vascular supply and 2) migration of the heel pad due to instability. A hypermobile heel pad can cause difficulty with prosthesis wear and damage to the soft tissues which can eventually lead to failure. Both malleoli are usually removed in the procedure, except in children or during the first stage procedure of a diabetic or infection case. The tibialis anterior is usually tenodesed to the anterior heel pad along with the EDL tendon to avoid posterior migration of the heel pad.
Question 24High Yield
A 47-year-old man is seen in consultation in the ICU after being admitted and treated emergently for a dissecting aortic aneurysm. Current examination reveals generalized weakness of the lower extremities with a significant decrease in pain and temperature sensation from approximately the waist down.Proprioception is maintained. What is the most likely diagnosis at this time?
Explanation
Incomplete cord syndromes include anterior cord syndrome, Brown-Sequard syndrome,central cord syndrome, and posterior cord syndrome. The anterior cord syndrome involves a variable loss of motor function and pain and/or temperature sensation, with preservation of proprioception as seen in this patient. The Brown-Sequard syndrome involves an ipsilateral loss of proprioception and motor function, with contralateral loss of pain and temperature sensation. The posterior cord syndrome is a rare injury and is characterized by preservation of motor function, sense of pain and light touch, with loss of proprioception and temperature sensation below the level of the lesion. The central cord syndrome is characterized with greater motor weakness in the upper extremities than in the lower extremities. The pattern of motor weakness shows greater distal involvement in the affected extremity than proximal muscle weakness.
Spinal shock is the period of time, usually 24 hours, after a spinal injury characterized by absent reflexes, flaccidity, and loss of sensation below the level of the injury.
Spinal shock is the period of time, usually 24 hours, after a spinal injury characterized by absent reflexes, flaccidity, and loss of sensation below the level of the injury.
Question 25High Yield
A 68-year-old woman who underwent left total hip arthroplasty 14 years ago now reports pain in her thigh. A radiograph is shown in Figure 14. What is the most reliable method for reconstructing the femoral component?

Explanation
DISCUSSION: The patient has a loose, cemented femoral component. The proximal femur is deficient and may not have adequate strength to support a proximally porous-coated cementless implant. Cemented hip implants have shown higher rates of failure when used for revision surgery. An extensively coated, cementless stem that engages the diaphysis has been shown to have excellent long-term durability in patients such as this, where the diaphysis is preserved and more than 4 cm of intact diaphysis is available for fixation. Allograft-prosthetic composites and tumor replacement prostheses are used for patients with more severe bone loss of the proximal femur and would not be indicated for this patient.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and
Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 457474.
Della Valle CJ, Paprosky WG: The femur in revision total hip arthroplasty: Evaluation and classification. Clin Orthop Relat Res 2004;420:55-62.
Engh CA Jr, Ellis TJ, Koralewicz LM, et al: Extensively porous-coated femoral revision for severe femoral bone loss: Minimum 10-year follow-up. J Arthroplasty 2002;8:955-960.
Figure 15
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and
Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 457474.
Della Valle CJ, Paprosky WG: The femur in revision total hip arthroplasty: Evaluation and classification. Clin Orthop Relat Res 2004;420:55-62.
Engh CA Jr, Ellis TJ, Koralewicz LM, et al: Extensively porous-coated femoral revision for severe femoral bone loss: Minimum 10-year follow-up. J Arthroplasty 2002;8:955-960.
Figure 15
Question 26High Yield
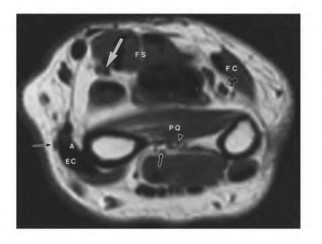
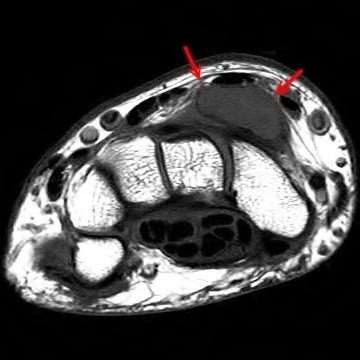
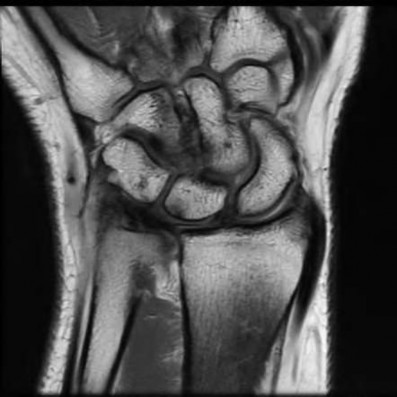
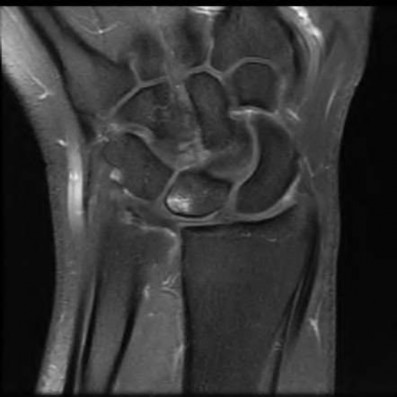
The video in Figure 56 depicts a 20-year-old right-hand-dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?

Explanation
Upon examination, this patient is exhibiting dislocation of the ECU tendon because of a disrupted sheath. He has failed nonsurgical measures, so surgery that would involve either direct repair or reconstruction of the tendon sheath is indicated. An option for reconstruction is to use a portion of the extensor retinaculum as a sheath substitute. Deepening of the ECU tendon groove at the distal ulna with direct repair of the sheath is another option, although a 2016 paper by Ghatan and associates did not find depth of the groove as a risk factor for subluxation. TFCC repair, lunotriquetral fusion, and DRUJ tenodesis are not appropriate because the examination clearly shows ECU tendon dislocation. TFCC and lunotriquetral ligament tears can occur along with ECU tendon dislocation, but no other examination findings suggest these conditions for this patient.
RECOMMENDED READINGS
4. [MacLennan AJ, Nemechek NM, Waitayawinyu T, Trumble TE. Diagnosis and anatomic reconstruction of extensor carpi ulnaris subluxation. J Hand Surg Am. 2008 Jan;33(1):59-64. doi: 10.1016/j.jhsa.2007.10.002. PubMed PMID: 18261666. ](http://www.ncbi.nlm.nih.gov/pubmed/18261666)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18261666)
5. [Allende C, Le Viet D. Extensor carpi ulnaris problems at the wrist--classification, surgical treatment and results. J Hand Surg Br. 2005 Jun;30(3):265-72. Epub 2005 Apr 7.](http://www.ncbi.nlm.nih.gov/pubmed/15862366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15862366)
6. [Inoue G, Tamura Y. Surgical treatment for recurrent dislocation of the extensor carpi ulnaris tendon. J Hand Surg Br. 2001 Dec;26(6):556-9. PubMed PMID: 11884112. ](http://www.ncbi.nlm.nih.gov/pubmed/11884112)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884112)
7. [Ghatan AC, Puri SG, Morse KW, Hearns KA, von Althann C, Carlson MG. Relative Contribution of the Subsheath to Extensor Carpi Ulnaris Tendon Stability: Implications for Surgical Reconstruction and Rehabilitation. J Hand Surg Am. 2016 Feb;41(2):225-32. doi: 10.1016/j.jhsa.2015.10.024. Epub 2015 Dec 12. PubMed PMID: 26691954. ](http://www.ncbi.nlm.nih.gov/pubmed/26691954)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26691954)
RECOMMENDED READINGS
4. [MacLennan AJ, Nemechek NM, Waitayawinyu T, Trumble TE. Diagnosis and anatomic reconstruction of extensor carpi ulnaris subluxation. J Hand Surg Am. 2008 Jan;33(1):59-64. doi: 10.1016/j.jhsa.2007.10.002. PubMed PMID: 18261666. ](http://www.ncbi.nlm.nih.gov/pubmed/18261666)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18261666)
5. [Allende C, Le Viet D. Extensor carpi ulnaris problems at the wrist--classification, surgical treatment and results. J Hand Surg Br. 2005 Jun;30(3):265-72. Epub 2005 Apr 7.](http://www.ncbi.nlm.nih.gov/pubmed/15862366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15862366)
6. [Inoue G, Tamura Y. Surgical treatment for recurrent dislocation of the extensor carpi ulnaris tendon. J Hand Surg Br. 2001 Dec;26(6):556-9. PubMed PMID: 11884112. ](http://www.ncbi.nlm.nih.gov/pubmed/11884112)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884112)
7. [Ghatan AC, Puri SG, Morse KW, Hearns KA, von Althann C, Carlson MG. Relative Contribution of the Subsheath to Extensor Carpi Ulnaris Tendon Stability: Implications for Surgical Reconstruction and Rehabilitation. J Hand Surg Am. 2016 Feb;41(2):225-32. doi: 10.1016/j.jhsa.2015.10.024. Epub 2015 Dec 12. PubMed PMID: 26691954. ](http://www.ncbi.nlm.nih.gov/pubmed/26691954)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26691954)
Question 27High Yield
A 55-year-old man has had progressive right shoulder pain for the past 2 years. Examination reveals active elevation to 120 degrees, external rotation to 20 degrees, and internal rotation to the sacrum. AP and axillary radiographs are shown in Figures 23a and 23b. Which of the following procedures would result in the most predictable long-term pain relief?
Explanation
Total shoulder arthroplasty yields excellent pain relief and function in patients with osteoarthritis. It is favored over humeral arthroplasty, especially when there is asymmetric posterior glenoid wear and posterior humeral subluxation as shown on the axillary radiograph. Arthroscopic debridement of the glenohumeral joint may be helpful in delaying the need for arthroplasty when the arthritic changes are mild to moderate but is not indicated for advanced osteoarthritis.
REFERENCES: Cofield RH, Frankle MA, Zuckerman JD: Humeral head replacement for glenohumeral arthritis. Semin Arthroplasty 1995;6:214-221.
Levine WN, Djurasovic M, Glasson JM, Pollock RG, Flatow EL, Bigliani LU: Hemiarthroplasty for glenohumeral osteoarthritis: Results correlated to degree of glenoid wear. J Shoulder Elbow Surg 1997;6:449-454.
Matsen FA III: Early effectiveness of shoulder arthroplasty for patients who have primary glenohumeral degenerative joint disease. J Bone Joint Surg Am 1996;78:260-264.
REFERENCES: Cofield RH, Frankle MA, Zuckerman JD: Humeral head replacement for glenohumeral arthritis. Semin Arthroplasty 1995;6:214-221.
Levine WN, Djurasovic M, Glasson JM, Pollock RG, Flatow EL, Bigliani LU: Hemiarthroplasty for glenohumeral osteoarthritis: Results correlated to degree of glenoid wear. J Shoulder Elbow Surg 1997;6:449-454.
Matsen FA III: Early effectiveness of shoulder arthroplasty for patients who have primary glenohumeral degenerative joint disease. J Bone Joint Surg Am 1996;78:260-264.
Question 28High Yield
Which of the following is an effective medication for osteopetrosis:
Explanation
Interferon gamma-1 is the only treatment for osteopetrosis that is approved by the Food and Drug Administration
Question 29High Yield
A 72-year-old woman experiences left shoulder pain and dysfunction. An examination demonstrates 45 degrees of active forward elevation with 2/5 strength. The deltoid fires in the anterior, middle, and posterior heads (Figure 93).

Explanation
- Reverse total shoulder arthroplasty (rTSA)_
Question 30High Yield
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of**
Explanation
Immediate repair of the tuberosity and rotator cuff is recommended on identifying the avulsion or nonunion. Revising the humeral component to increase tension and length will overtighten the cuff and increase the chance of tuberosity pull-off. The glenoid is uninvolved and should not be replaced. Attempts to strengthen the rotator cuff will be unsuccessful because the insertions are no longer attached to the humerus when the tuberosities avulse.
REFERENCES: Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
Muldoon MP, Cofield RH: Complications of humeral head replacement for proximal humeral fractures. Instr Course Lect 1997;46:15-24.
REFERENCES: Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
Muldoon MP, Cofield RH: Complications of humeral head replacement for proximal humeral fractures. Instr Course Lect 1997;46:15-24.
Question 31High Yield
- are the radiographs and CT scans of a 45-year-old man who fell 10 feet from a ladder and sustained an injury to the right knee. Examination reveals no open wounds and the skin was in good condition with moderate swelling and no fracture blisters. The patient is neurovascularly intact.What is the most appropriate treatment?
Explanation
No detailed explanation provided for this question.
Question 32High Yield
Slide 1
A patient presents with a claw toe deformity (Slide). What is the strongest flexor of the metatarsophalangeal joint, which in this patient is not functioning adequately:
A patient presents with a claw toe deformity (Slide). What is the strongest flexor of the metatarsophalangeal joint, which in this patient is not functioning adequately:
Explanation
Although the long and short flexor tendons have some effect albeit indirect on the flexion of the metatarsophalangeal joint, the flexor that acts directly on the joint is the interosseous muscle. Intrinsic atrophy will lead to claw toe deformity.
Question 33High Yield
A magnetic resonance image of a 7-year-old girl shows a line of high-signal intensity within the cord on T2 sequences that parallels the ventral surface of the cord and appears as a syrinx. However, on the axial images and on the T1 sequences, this finding is not evident. The most likely diagnosis is:
Explanation
A Gibbs artifact is a linear focus in the cord on T2-weighted images that parallels the ventral aspect of the cord and mimics a syrinx. The Gibbs artifact is due to the linear interface between two tissues of differing signal intensity. It is not seen on axial images or T1-weighted images.
Motion artifact is a blurring of the image due to patient motion, respiration, or cerebral spinal fluid pulsation. Ependymoma and astrocytoma are seen on both the axial and the sagittal images.
Motion artifact is a blurring of the image due to patient motion, respiration, or cerebral spinal fluid pulsation. Ependymoma and astrocytoma are seen on both the axial and the sagittal images.
Question 34High Yield
During the approach to the lumbar spine for an L4-L5 anterior lumbar interbody fusion, which structure generally is found overlying the anterior surface of the L4 vertebra?
Explanation
■
During an anterior approach to the L4-L5 disk space for anterior lumbar interbody fusion, meticulous exposure is paramount to allow for safe preparation of the disk space and subsequent arthrodesis. Although all of these structures can come into play during the exposure, the aorta lies anterior to the L4 vertebral body and bifurcates at this level. The vena cava bifurcates just distal to this. The ureters lie to both sides of the anterior spine. The right common iliac artery and the left common iliac vein originate after the bifurcation of the great vessels and lie caudal to the L4 vertebra.
During an anterior approach to the L4-L5 disk space for anterior lumbar interbody fusion, meticulous exposure is paramount to allow for safe preparation of the disk space and subsequent arthrodesis. Although all of these structures can come into play during the exposure, the aorta lies anterior to the L4 vertebral body and bifurcates at this level. The vena cava bifurcates just distal to this. The ureters lie to both sides of the anterior spine. The right common iliac artery and the left common iliac vein originate after the bifurcation of the great vessels and lie caudal to the L4 vertebra.
Question 35High Yield
A 9-year-old girl, who is an avid soccer player, has intermittent spontaneous snapping in her left knee that has worsened. There is no reported trauma or prior surgeries to her knee. Despite working with her trainer, she has developed anterior-based knee pain and lacks full extension. Her knee skin is unremarkable, but there is fullness to palpation on the lateral aspect of her knee. Her range of motion demonstrates a lack of 15° of terminal extension and ligamentous examination is unremarkable. Considering possible surgical treatments for this patient, what is the most appropriate surgical treatment?
Explanation
Surgical intervention of discoid meniscus is based on symptomatic patients. Complete discoid menisci are typically stable but are expected to have >4.5 times incidence of surgical intervention. Saucerization of symptomatic discoid meniscus is associated with better results with younger patients with increases of poor outcomes in adult-aged patients. Meniscal transplant may be an option, although long-term results _are unknown._
Question 36High Yield
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
Explanation
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted.
REFERENCES: Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Leffert RD: Neurological Problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 759-760.
REFERENCES: Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Leffert RD: Neurological Problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 759-760.
Question 37High Yield
Which of the following is the most definitive means of making a diagnosis of active skeletal tuberculosis:
Explanation
An early histology confirmed later by a culture is considered the definitive means of diagnosis for active skeletal tuberculsosis.
The tuberculin tine tests do not indicate active disease, only exposure.
Magnetic resonance imaging is not specific for a particular infectious organism.
The enzyme linked immunosorbent assay (ELISA) test is used to diagnose Lyme disease.
The tuberculin tine tests do not indicate active disease, only exposure.
Magnetic resonance imaging is not specific for a particular infectious organism.
The enzyme linked immunosorbent assay (ELISA) test is used to diagnose Lyme disease.
Question 38High Yield
38A
B
Three months later this patient has continued swelling and giving-way episodes. Figures 38a and 38b are his stress radiographs. This study indicates laxity in which ligament?
B
Three months later this patient has continued swelling and giving-way episodes. Figures 38a and 38b are his stress radiographs. This study indicates laxity in which ligament?


Explanation
- Anterior talofibular
Question 39High Yield
The most common problem encountered with total knee arthroplasty (TKA) after high tibial osteotomy is:
Explanation
Patella infera is encountered 80% of the time after a high tibial osteotomy. Patella infera makes it difficult for a surgeon to visualize and dislocate the patella laterally, and it also makes for a difficult salvage for a total knee replacement
Question 40High Yield
What is the most appropriate initial diagnostic imaging study for a patient with presumed diskogenic low-back pain?
Explanation
Radiography is the best initial study. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain such as osteoporotic collapse, osteolytic collapse, and deformity also can be evaluated. The other tests may be beneficial and are more appropriate as later imaging options.
RECOMMENDED READINGS
Yu WD, Williams SL. Spinal imaging: Radiographs, computed tomography, and magnetic resonance imaging. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine
3/. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:57-67.
Bess RS, Brodke DS. Degenerative disease of the lumbar spine. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:551-563.
RECOMMENDED READINGS
Yu WD, Williams SL. Spinal imaging: Radiographs, computed tomography, and magnetic resonance imaging. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine
3/. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:57-67.
Bess RS, Brodke DS. Degenerative disease of the lumbar spine. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:551-563.
Question 41High Yield
A 15-year-old girl who plays high school basketball has had worsening forefoot pain and swelling that is aggravated by activity for the past 5 weeks. She denies any history of an injury. Examination reveals no deformities. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
Freiberg’s infraction is believed to be an osteochondrosis of the second metatarsal head. It is the only osteochondrosis that has a predilection for females. The typical patient is an athletically active adolescent female. The radiograph shows stage II disease wherein reossification is occurring; it is at this time that the second metatarsal head is most susceptible to deformation. Therefore, initial management should consist of a short leg
walking cast.
REFERENCE: Mann RA, Coughlin MJ: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 413-415.
walking cast.
REFERENCE: Mann RA, Coughlin MJ: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 413-415.
Question 42High Yield
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---



Explanation
Medial plateau fracture dislocations are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the anteroposterior radiograph include an intact lateral column (lateral articular surface still in continuity with tibial shaft), centrolateral articular impaction, shortening, and condylar widening. The medial femoral condyle stays with the fractured medial tibial plateau segment.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 43High Yield
An infant is born with fibular hemimelia and has 20% shortening of the involved below-knee segment. Four rays are present on the foot, and the ankle is in slight valgus. Limb lengthening is likely to be superior to Syme disarticulation in which of the following parameters:
Explanation
The cost of prosthetics is greater in the disarticulation group.
Pain is greater in the lengthened group.
Function is equal to or better in the group who had disarticulation. Psychological acceptance is greater in the disarticulation group.
The lengthened group requires more than twice the number of procedures.
Pain is greater in the lengthened group.
Function is equal to or better in the group who had disarticulation. Psychological acceptance is greater in the disarticulation group.
The lengthened group requires more than twice the number of procedures.
Question 44High Yield
An 82-year-old female sustains a valgus-impacted subcapital femoral neck fracture and undergoes cannulated screw fixation as shown in Figure A. She returns for her first follow-up visit one week later following another fall and now complains of severe hip pain. She is unable to bear weight on the limb, and a new radiograph reveals varus displacement of her fracture. She subsequently undergoes revision fixation but during this procedure, the femoral neck fracture displaces and becomes comminuted. Which is the most appropriate next step in management?

Explanation
In the scenario of an elderly patient with questionable fixation into the femoral head and a non-healed femoral neck fracture, proper treatment is arthroplasty. In a physiologically younger patient, reduction and fixation of the fractures (femoral neck and subtrochanteric, if present) with methods such as a valgus producing osteotomy at the level of the subtrochanteric fracture are
recommended.
Figure A shows cannulated screw fixation of a right femoral neck fracture.
The referenced study by Oakey et al evaluated strength of proximal femurs after cannulated hip screw placement and found that placement of an inverted triangle had a higher ultimate load to failure than placement in a standard triangle format (two screws distal).
recommended.
Figure A shows cannulated screw fixation of a right femoral neck fracture.
The referenced study by Oakey et al evaluated strength of proximal femurs after cannulated hip screw placement and found that placement of an inverted triangle had a higher ultimate load to failure than placement in a standard triangle format (two screws distal).
Question 45High Yield
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include
Explanation
The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting.
REFERENCES: Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141.
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Hak DG, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178-182.
REFERENCES: Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141.
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Hak DG, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178-182.
Question 46High Yield
When comparing the direct anterior approach with the posterolateral surgical approach, the direct anterior approach is associated with
Explanation
The direct anterior approach in primary total hip arthroplasty (THA) has continued to gain in popularity. Prior investigations have shown patients do very well following a direct anterior THA with excellent rates of recovery and clinical outcomes. However, the potential for femoral-sided complications, including femoral component subsidence and fracture, may be increased via the direct anterior approach versus a posterolateral surgical approach.
Question 47High Yield
Figures 1 through 5 show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old
collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain
with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. Approximately what percentage of asymptomatic
athletes have cam deformities of the hip?
collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain
with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. Approximately what percentage of asymptomatic
athletes have cam deformities of the hip?
Explanation
Multiple studies have confirmed that cam or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, cam deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion is higher than 50% in the subgroup of athletes. Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in most nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between cam deformity and hip osteoarthritis, a corresponding link between the correction of the deformity and prevention of osteoarthritis has never been proven. The results of cam deformity correction, typically including repair of the degenerative labral tear, are much poorer when substantial joint space loss is present. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
Question 48High Yield
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Explanation
Two-dimensional CT scan is generally accepted as a superior imaging modality for evaluating bone loss in shoulder instability than two-dimensional MRI scan. This advantage is offset by the relatively high radiation dose. Although CT in most situations is less costly, MRI can provide more data regarding associated soft-tissue damage that can be associated with recurrent instability. It should be noted that three-dimensional MRI has recently been shown as equivalent to three-dimensional CT in its ability to identify glenoid bone loss.
Question 49High Yield
This patient has a normal-appearing creatinine clearance. Importantly, elderly patients have decreased muscle mass and therefore decreased creatinine production, which may cause renal function to appear normal when it is, in fact, not.
A 68-year-old female sustains a closed ankle fracture and is treated with open reduction and internal fixation. Her postoperative radiographs are shown in Figure A. Widening of the tibia-fibular clear space with external rotation stress would be a result of injury of which structure?
A 68-year-old female sustains a closed ankle fracture and is treated with open reduction and internal fixation. Her postoperative radiographs are shown in Figure A. Widening of the tibia-fibular clear space with external rotation stress would be a result of injury of which structure?




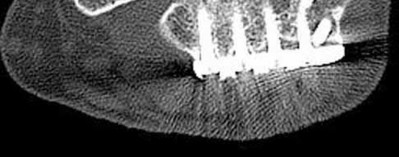










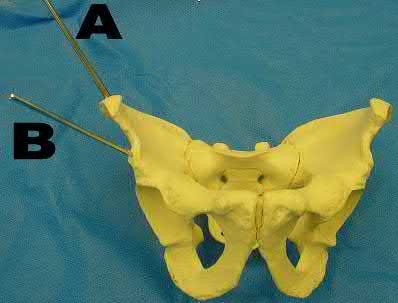














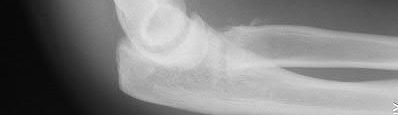





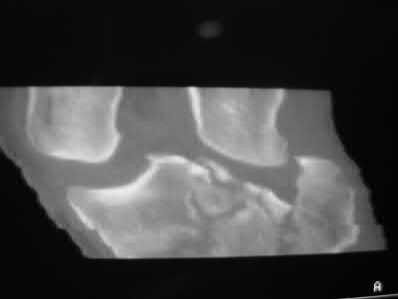

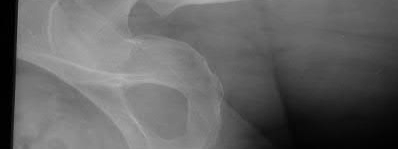


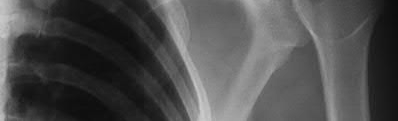






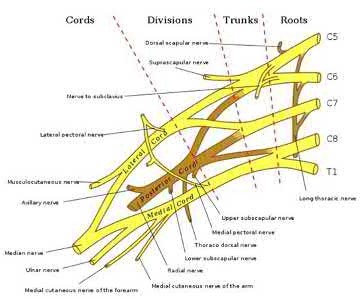








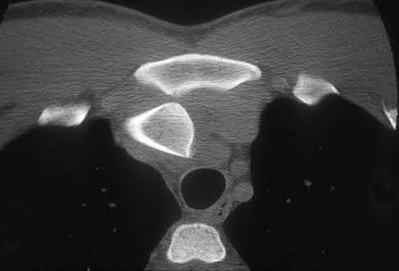

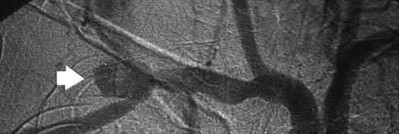
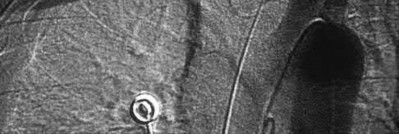



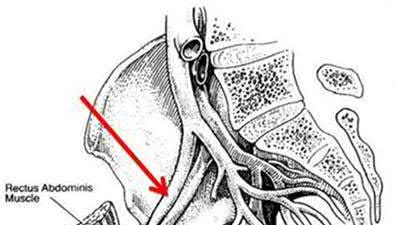
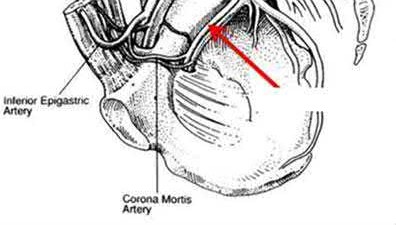
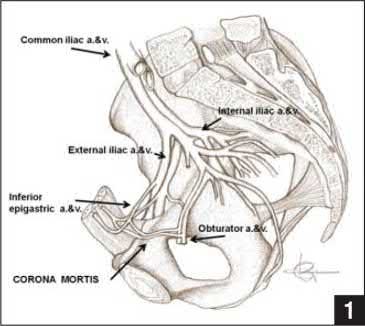































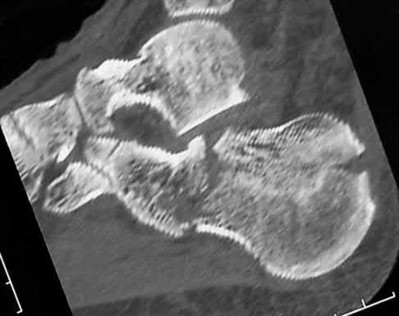
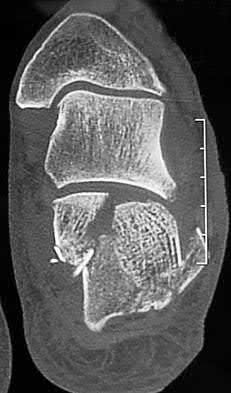




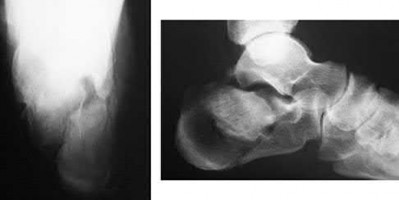











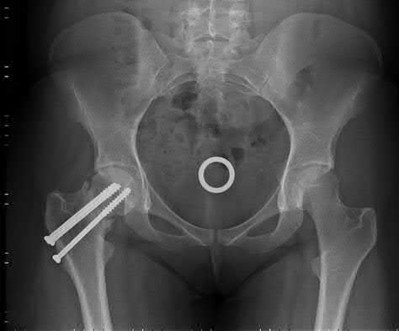












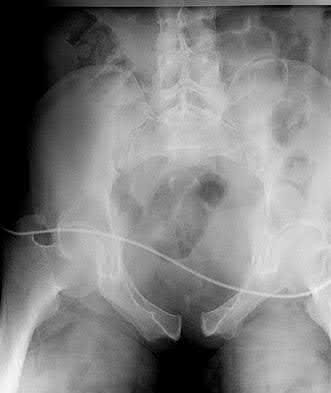
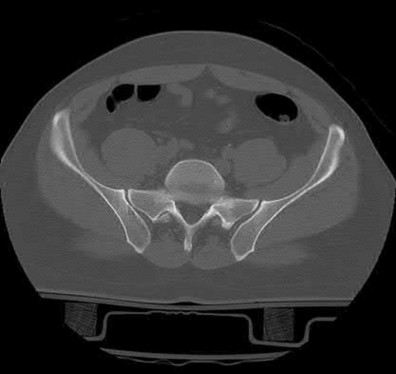
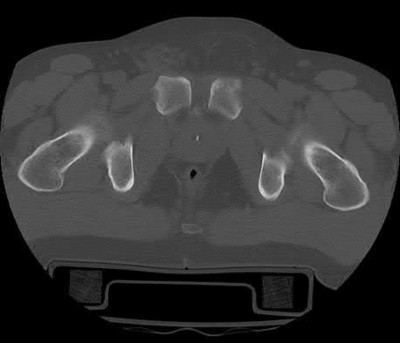









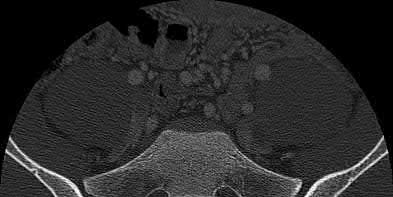


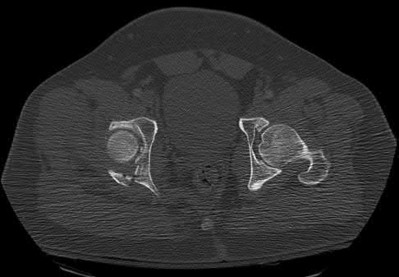












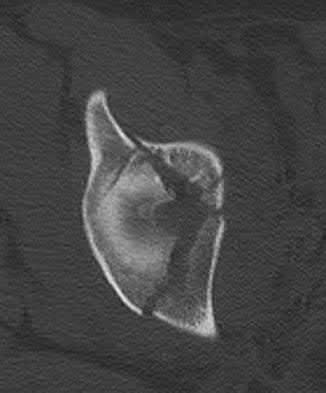





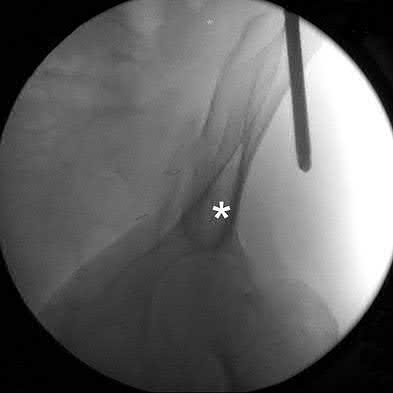












Explanation
Bone overgrowth is a poorly understood phenomenon in which the bone end undergoes disorganized appositional growth following amputation in a skeletally immature patient. Overgrowth is the most common complication following transosseous amputation in pediatric patients.
Krajbich reviews the management of pediatric patients with lower-limb deficiences and amputations. He advocates disarticulation as opposed to transosseous amputation when possible as bone overgrowth has not been observed in bone ends covered by articular cartilage.
O'neal et al retrospectively reviewed their rates of surgical revision for bone overgrowth in pediatric and adolescent amputees. The highest rates of revision were seen with metaphyseal-level amputations (50%) and with traumatic amputations (43%).
Benevenia et al reviewed their rates of overgrowth in skeletally immature transosseous amputees using an autogenous epiphyseal transplant from the amputated limb to cap the medullary canal. They found that only 1 of 10 patients undergoing amputation with this technique had complications due to bone overgrowth, compared with 6 of 7 patients undergoing traditional transosseous amputation.
Illustration A is a clinical photo of bone overgrowth eroding through the soft tissue in a transhumeral amputee. Illustration B demonstrates the radiographic appearance of bone overgrowth in a transtibial amputation.
Incorrect Answers:
. Neurogenic pain is a concern for adults, but rarely occurs in children.
Answer 3. Flexion contracture is not a common complication following amputation in pediatric patients.
Answer 4. Adduction contracture is not a common complication following amputation in this patient population.
Answer 5. The proximal tibial physis, important for longitudinal growth of the limb, would be sacrificed with a knee disarticulation, meaning the residual limb will be shorter than if the patient had a transtibial amputation.
A 52-year-old woman reports mild pain localized to the left sternoclavicular joint. History is notable for chronic renal failure requiring dialysis for the last 5 years. A clinical photograph, chest radiograph, and bone scan are shown in Figures 58a through 58c. What is the most likely diagnosis?
1) Pseudogout
2) Spontaneous subluxation
3) Postmenopausal arthritis
4) Chronic osteomyelitis
5) Friedreich’s disease
Spontaneous swelling with the appearance of joint subluxation may be associated with an acute, subacute, or chronic bacterial infection of the sternoclavicular joint. Common causes of infection include bacteremia, rheumatoid arthritis, alcoholism, intravenous drug use, and chronic debilitating diseases. Subclavian vein catheterization and renal dialysis can predispose patients to sepsis and osteomyelitis of the sternoclavicular joint.
A 19-year-old man was struck by a car and is seen in the emergency department with a grade IIIC open distal tibia and fibula fracture. Examination reveals that the toes are cool and dusky with a sluggish capillary refill. Angiography reveals a lesion in the posterior tibial artery amenable to repair. There is no sensation on the plantar aspect of the foot, and he is unable to flex his toes. A clinical photograph and radiograph are shown in Figures 2a and 2b. What is the next most appropriate step in management?
1) Irrigation and debridement with immediate intramedullary fixation, vascular repair, and primary closure
2) Irrigation and debridement with external fixation, vascular repair, and delayed closure
3) Irrigation and debridement with external fixation, vascular repair, exploration of the tibial nerve, and delayed closure
4) Guillotine amputation at the fracture site with delayed closure
5) Immediate below-knee amputation
In the past, loss of plantar sensation in this grade IIIC tibial fracture would have been an indication for below-knee amputation regardless of the potential for vascular repair. However the 2002 LEAP study divided 55 patients with loss of plantar sensation into two groups, the insensate amputation group and the insensate limb salvage group, with 55% of patients in the insensate salvage group regaining normal sensation 2 years after injury. Furthermore, those in
the salvage group who remained insensate after 2 years had equivalent outcomes to those in the amputation group. Because of these findings, limb salvage with vascular repair and external stabilization with delayed closure is deemed appropriate treatment. Immediate intramedullary fixation is not indicated. Because ischemia, contusion, and stretch can adversely affect the tibial nerve, the additional insult of exploration of the nerve is also not advisable given the soft-tissue compromise.
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?
1) Anterior tibialis tendon transfer to the dorsolateral midfoot
2) Posterior tibialis tendon transfer to the dorsolateral midfoot
3) Peroneus longus tendon transfer to the dorsolateral midfoot
4) Peroneus brevis tendon transfer to the dorsolateral midfoot
5) Flexor hallucis longus tendon transfer to the peroneus brevis
Compartment syndrome of the anterior and deep posterior compartments results in anterior tibialis and posterior tibialis tendon weakness, respectively. Furthermore, the long flexors to the hallux and lesser toes will be weak as well. The intact peroneus longus overpowers the weak anterior tibialis tendon, resulting in plantar flexion of the first metatarsal, cavus, and hindfoot varus.
Therefore, transferring the peroneus longus to the dorsolateral midfoot reduces the first metatarsal plantar flexion torque, and possibly augments ankle dorsiflexion torque.
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the
ankle is obtained. This test is designed to evaluate the integrity of what structure?
1) Posterior talofibular ligament
2) Distal tibiofibular syndesmosis
3) Anterior talofibular ligament
4) Deltoid ligament
5) Calcaneofibular ligament
In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used.
A 29-year-old patient sustains a closed, displaced joint depression intra-articular calcaneus fracture. In discussing potential complications of surgical intervention through an extensile lateral approach, which of the following is considered the most common complication following surgery?
1) Nonunion
2) Deep infection
3) Delayed wound healing
4) Peroneal tendinitis
5) Posttraumatic arthritis
Delayed wound healing and wound dehiscence is the most common complication of surgical management of calcaneal fractures through an extensile lateral approach, occurring in up to 25% of patients. Most wounds ultimately heal with local treatment; the deep infection rate is approximately 1% to 4% in closed fractures. Posttraumatic arthritis may develop despite open reduction and internal fixation, but the percentages remain low. Peroneal tendinitis may occur from adhesions within the tendon sheath or from prominent hardware but is relatively uncommon. Nonunion of a calcaneal fracture is rare.
Twelve months after open reduction and internal fixation of a comminuted distal radius fracture as seen in Figure A and B, which of the following tendons is at greatest risk of rupture?
1) Abductor Pollicis Longus
2) Extensor Pollicis Brevis
3) Extensor Indicis Proprius
4) Flexor Pollicis Brevis
5) Flexor Pollicis Longus
Figure A shows a distal radius fracture treated with a volar locked plate. Historically, distal radius fractures treated with dorsal plates were notorious for extensor tendon irritation with some cited rates as high as 50%.
In the reference by Drobetz et al, they reviewed 50 fractures treated with a volar locked plate. They noted that in 6 (12%) of cases that there was rupture of the flexor pollicis longus (FPL) at a mean of 10 months post operatively.
The second reference by Douthit is a retrospective review of 46 fractures treated with a volar locked plate. Excellent initial and maintenance of reduction was noted in 85% of cases, but FPL rupture occurred in 2 patients. Prominent plates and sharp screws were cited as reasons for tendon rupture.
Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?
1) MRI of the ankle
2) CT of the ankle
3) Technetium bone scan
4) Radiographs of the tibia and fibula
5) Repeat radiographs of the ankle in 5 to 7 days
The radiographs show an isolated posterior malleolus fracture which, given the injury mechanism, is highly suspicious for a Maisonneuve injury. As with any suspected extremity injury, radiographs including the joints above and below the level of injury are acutely indicated. Although MRI may reveal a ligamentous injury to the ankle and CT may show asymmetry of the ankle mortise or syndesmosis, both studies are considerably more costly and are not indicated in the absence of a complete radiographic work-up. Technetium bone scan is nonspecific and would be of limited value in this instance, as would repeat radiographs of the ankle.
A 25-year-old woman with a healed proximal tibiofibular fracture treated with an intramedullary nail 2 years ago is currently wearing an ankle-foot orthosis (AFO) and reports a persistent foot drop. She is unhappy with the AFO and has not seen any functional improvement despite months of physical therapy. Serial electromyograms (EMG) show no recent change over the past year. Examination and EMG findings are consistent with a tibialis anterior 1/5, extensor hallucis longus 2/5, extensor digitorum longus 2/5, posterior tibial tendon (PTT) 5/5, peroneals 3/5, flexor hallucis longus 5/5, and gastrocsoleus 5/5. No discrete nerve lesion was identified. The patient has a flexible equinovarus contracture. What is the most appropriate management?
1) Continued AFO bracing and therapy
2) Ankle fusion
3) Exploration and release of the common peroneal nerve
4) Transfer of the PTT through the interosseous membrane with attachment to the tibialis anterior and peroneus tertius above the level of the ankle, debridement of the anterior compartment, and Achilles tendon lengthening
5) Transfer of the peroneus longus to the dorsum of the foot and Achilles tendon lengthening
This pattern of injury is consistent with an unrecognized compartment syndrome of the anterior and lateral compartments. Transfer of the PTT through a long incision in the interosseous membrane corrects the foot drop deformity, and allows adequate dorsiflexion provided that the tendon to be transferred has a strength of 5/5. Muscles/tendons typically lose one grade of strength after transfer. Transfer into the tendons at the level of the ankle prevents overtensioning or pullout of a PTT tendon that is not long enough.
Debridement of the scarred muscle in the anterior compartment decreases the risk of scarring down to the tendon transfer. Transfer of the peroneus longus is not preferred given its relative lack of strength and line of pull. Continued therapy and bracing are unlikely to lead to further improvement at 2 years after injury. An ankle fusion would correct the foot drop but would not address the tendon imbalances between the tibialis anterior and the peroneus longus, and the PTT and the peroneus brevis.
When using a two-incision approach for open reduction and internal fixation of a Hawkins III talar fracture-dislocation involving
the talar neck and body, what anatomic structure must be preserved to optimize outcome?
1) Deltoid branch of the artery of the tarsal canal
2) Dorsalis pedis artery
3) Tarsal sinus artery
4) Perforating peroneal artery
5) Navicular artery
A Hawkins III fracture-dislocation generally presents with posteromedial displacement with the deltoid ligament intact. Therefore, the only remaining blood supply is the deltoid branch of the artery of the tarsal canal originating from the posterior tibial artery. Often, the medial malleolus is fractured, assisting in reduction and visualization of fracture reduction. If the medial malleolus is intact, a medial malleolus osteotomy allows visualization of the reduction without compromising the last remaining blood supply to the talus.
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort.
Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?
1) Short leg cast for 6 weeks
2) Splinting with early range of motion at 3 weeks
3) Immediate open reduction and internal fixation through a medial approach
4) Delayed open reduction and internal fixation
5) Fusion
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended.
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management?
1) Triple antibiotic coverage
2) Transfer to the ICU and a consult with infectious disease
3) Urgent irrigation and debridement with gentle skin closure
4) Urgent hyperbaric oxygen treatments and immunoglobulin
5) Urgent aggressive debridement of skin, subcutaneous fat, and fascia
The patient has necrotizing fasciitis, a rare and sometimes fatal disease that has many different etiologies. Signs that this is not a normal infection are the worsening clinical symptoms despite IV antibiotics and the systemic symptoms. He needs urgent surgical care before he becomes completely septic and unstable. He needs very aggressive debridement of his tissues. Hyperbaric oxygen and immunoglobulins are only anecdotally helpful, and would only be used after surgery.
Figures 17a through 17c show the radiographs of a 38-year-old man following a motorcycle accident. The posterior portion of the talus extruded through a posterolateral wound. The extruded talar body is visible in the wound along with some road debris. Management should now consist of surgical irrigation, debridement, and
1) removal of the extruded talus and placement of an external fixator.
2) immediate tibiocalcaneal fusion.
3) reimplantation of the talus, external fixation, and/or open reduction and internal fixation of the talar neck fracture.
4) reimplantation followed by primary tibiotalar arthrodesis.
5) Syme amputation.
The extruded talus should be placed in sterile bacitracin solution, irrigated thoroughly, gently debrided, and immediately replanted in the OR. Open reduction and internal fixation of the talar fracture may be attempted immediately depending on the soft-tissue envelope, or delayed after soft-tissue
stabilization with an external fixator. A retrospective study of 19 patients with an extruded talus reported that 12 patients had no subsequent surgery after definitive fixation, 7 had subsequent procedures, and 2 patients developed infections that were treated successfully at an average of 42-month follow-up. Successful outcome in this series was attributed to multiple debridements, soft-tissue stabilization, and primary wound closure.
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?
1) CT scan
2) Repeat period of immobilization
3) Referral to pain management for sympathetic blocks
4) Continued observation and physical therapy
5) Acupuncture
Persistent pain at the fracture site in the absence of infection is most likely due to a nonunion, best detected by CT. Walsh and DiGiovanni reported on a series of closed rotational fibular fractures in which nonunions were detected by CT in the absence of standard ankle radiographic findings. Repeat immobilization would not be appropriate at this late date. Pain management/sympathetic blocks would be considered if the patient displayed pain with light touch and disproportionate pain consistent with a complex mediated pain syndrome.
Acupuncture would be expected to be of limited benefit.
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?
1) Talectomy
2) Revision open reduction and internal fixation (ORIF) with bone grafting
3) Ankle arthrodesis
4) Tibiotalocalcaneal arthrodesis
5) Triple arthrodesis
The radiographs reveal nonunion of a talar neck fracture. There is no radiographic evidence of osteonecrosis or significant degenerative arthritis. The results of talectomy are suboptimal. Arthrodesis would be indicated for degenerative arthritis. Revision ORIF is feasible and preserves motion. A vascularized graft should be considered whenever osteonecrosis is present, but the talar body appears viable in this case.
A 27-year-old man was struck by a taxi cab and sustained comminuted right distal third tibia and fibula fractures; treatment consisted of placement of an intramedullary nail in the tibia the following morning. At his 6-month follow-up, he has clawing of all five toes. Examination reveals flexion deformities of the distal and proximal interphalangeal joints that are flexible with plantar flexion and rigid with dorsiflexion. Calluses are present on the dorsum and tip of the toes. Single heel rise is normal. He has a mild equinus contracture (relative to the left leg) that is not relieved with knee flexion. What is the most appropriate treatment option?
1) Physical therapy and bracing
2) Reassurance that the deformity will resolve with time
3) Achilles tendon lengthening, and release or retromalleolar lengthening of the flexor digitorum longus (FDL) and flexor hallucis longus (FHL)
4) FDL and FHL tenotomies at the individual digits with transfer of the posterior tibial tendon to the dorsum of the foot
5) FDL and FHL tenotomies at the individual digits with midfoot capsular release and hallux interphalangeal fusion
This is an example of tethering of the flexor hallucis longus/flexor digitorum longus (FHL/FDL) to the fracture site. Additional time and/or physical therapy and bracing would not be expected to be of benefit. Release of the FHL and FDL from the fracture site or retromalleolar lengthening will address the posttraumatic claw toe deformity and Achilles tendon lengthening will address the mild equinus. Posterior tibial tendon transfer is not appropriate as the patient demonstrates a normal heel rise. Midfoot releases and hallux fusion are also not indicated.
A 24-year-old man reports the development of a foot drop following a knee dislocation 1 year ago. The common peroneal nerve was found to be in continuity at the time of surgical reconstruction of the posterolateral corner of the knee joint. He would like to eliminate the need for an ankle-foot orthosis. What is the best option to achieve elimination of the orthosis?
1) Repeat neurolysis of the common peroneal nerve at the knee level
2) Repeat neurolysis of the common peroneal nerve with cable grafting
3) Extensor hallucis longus transfer to the distal first metatarsal
4) Anterior transfer of the tibialis posterior tendon through the interosseous membrane
5) Ankle fusion
The ankle dorsiflexor muscles have been denervated for too long a period to expect reinnervation to be successful. Even if the extensor hallucis longus tendon was functional, it is unlikely to have sufficient strength to achieve dynamic ankle dorsiflexion. The tibialis posterior tendon transfer has been shown to predictably achieve these goals in a high percentage of patients.
Successful ankle fusion is likely to fail with time due to the development of forefoot equinus.
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
1) Quicker return to activities
2) Quicker return to work
3) Increased subtalar joint range of motion
4) Decreased risk of nonunion
5) Decreased risk of posttraumatic arthritis
The radiographs and CT scans show a displaced intra-articular calcaneal fracture, with loss of calcaneal height and length. Recent multicenter, randomized, prospective studies suggest that surgical treatment of displaced intra-articular calcaneal fractures is associated with an almost six-fold decrease
in the risk of posttraumatic subtalar arthritis (necessitating subtalar arthrodesis) compared to nonsurgical treatment. Despite ongoing controversy, surgical treatment has not been shown to be advantageous with respect to activity, time to return to work, or subtalar joint range of motion. A nonunion of a calcaneal fracture is exceedingly rare regardless of the treatment method.
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments.
Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
1) surface irrigation, sterile dressing, and a short leg cast.
2) surface irrigation, sterile dressing, a short leg cast, and oral antibiotics.
3) surface irrigation, sterile dressing, a short leg cast, and IV antibiotics.
4) surgical debridement, a short leg cast, and IV antibiotics.
5) surgical debridement, external or internal fixation, and IV antibiotics.
The patient sustained a type I unstable fracture that requires debridement of superficial fragments from the sole and surgical stabilization. Low-velocity wounds less than 8 hours old are considered type I open fractures. In contrast, gunshot wounds with associated fractures more than 8 hours old are considered type II open fractures using the Gustilo and Anderson classification. Gustilo type I stable fractures due to gunshot wounds and seen within 8 hours can be treated with tetanus toxoid (if no history of immunization or booster within 5 years), surface irrigation, and casting or a hard sole shoe. Antibiotics are not required unless gross contamination is present. However, if the extent of contamination is unclear, or if a joint is penetrated, then routine antibiotic prophylaxis is recommended. Indications for surgery include: articular involvement, unstable fractures, presentation 8 or more hours after injury, tendon involvement, and superficial fragments in the palm or sole. Type I unstable fractures may be stabilized with internal or external fixation. Type II unstable fractures should be treated with external fixation and repeat debridements until clean.
A 32-year-old laborer reports left ankle pain and deformity. History reveals that he sustained a left ankle fracture 2 years ago and was treated with closed reduction and casting. Radiographs are shown in Figures 25a through 25c. What is the most appropriate management?
1) Bracing and physical therapy
2) Intra-articular injection of steroids into the ankle joint, bracing, and physical therapy
3) Intra-articular injection of hyaluronic acid product into the ankle joint, bracing, and physical therapy
4) Ankle fusion
5) Corrective osteotomy of the fibula and medial malleolus with reconstruction of the syndesmosis if unstable
Corrective osteotomy of fibular malunions, with appropriate lengthening, even in the presence of early arthritis, has been shown to decrease ankle pain and increase stability. Reduction and bone grafting of the medial malleolar nonunion is also needed. There is no evidence supporting the use of intraarticular steroids or hyaluronic acid in the ankle joint. Lateral talar displacement of even 1 mm has been reproducibly shown to decrease tibiotalar contact by 40% to 42%, causing a predisposition to arthritis.
Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The swelling has subsided by 3 weeks and the medial wound is clean. What do you tell the patient
about the likelihood of infection if a formal open reduction and internal fixation via a lateral approach is performed?
1) There is no significant difference between the infection rate for this fracture and a similar closed fracture.
2) Due to the risk of infection, open reduction and internal fixation is not recommended for this fracture.
3) The infection rate is three to five times more likely with this fracture.
4) Due to the risk of infection from a lateral approach, treatment is confined to limited internal fixation or an external fixator.
5) The patient will need to undergo 3 weeks of IV antibiotics at home.
Multiple authors have shown similar infection rates for grade 1 and 2 open medial fractures and closed fractures that have been treated with an extensile lateral approach and open reduction and internal fixation. Patients only need IV antibiotics for 2 to 3 days after surgery. Formal open reduction and internal fixation is not recommended for grade 3 medial wounds and most lateral wounds.
A 24-year-old woman was struck by a mini van in a parking lot and sustained a closed segmental tibia fracture that was treated with an intramedullary nail the following morning. Follow-up examinations reveal a slowly progressive clawing of all five toes, a progressive equinocavovarus contracture, and the patient is unable to perform a single heel rise on the affected limb. At 1 year after surgery, the patient now has a 10-degree equinus contracture that is not relieved with knee flexion. Treatment should now consist of
1) physical therapy and bracing.
2) reassurance that these problems will resolve with time.
3) posterior capsule release, Achilles tendon lengthening, and excision of the scarred muscle and tendon in the leg and foot.
4) Achilles tendon lengthening, and flexor digitorum longus and flexor hallucis longus tenotomies at the individual digits with transfer of the posterior tibial tendon to the dorsum of the foot.
5) flexor digitorum longus and flexor hallucis longus tenotomies at the individual digits with midfoot capsular release and hallux interphalangeal fusion.
This is an example of a missed deep posterior compartment syndrome that typically presents 6 months after the injury with progressive clawing due to necrosis, scarring, and contracture of the posterior tibial tendon, flexor digitorum longus, and flexor hallucis longus. Treatment consists of debridement of necrotic muscle and scar tissue with corresponding tendon excision. After debridement and posterior capsule release, if the equinus is relieved with knee flexion, a gastrocnemius slide may be performed.
Otherwise, the lengthening should be at the level of the Achilles tendon. Bracing will not address the claw toes.
Optimal management of the injury shown in Figure 31 should include which of the following?
1) Cast immobilization in equinus
2) Open reduction and internal fixation once the acute soft-tissue swelling has resolved
3) Urgent reduction and fixation
4) Arthroscopic-assisted percutaneous fixation
5) Open reduction and internal fixation with primary subtalar arthrodesis
The radiograph shows a displaced calcaneal beak fracture, a tongue-type fracture variant. The fracture fragment typically includes the insertion point of the Achilles tendon, which places marked tension on the thin overlying soft-tissue envelope and can lead to full-thickness necrosis if not acutely addressed. Cast immobilization does not adequately address the increased soft-tissue tension, as the fragment will be difficult to control. Arthroscopic-assisted techniques or primary arthrodesis are not indicated because calcaneal beak fractures are typically extra-articular.
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?
1) Surgical stabilization within 6 to 8 hours of injury
2) Extent of initial fracture displacement
3) Nicotine use
4) Posterior-to-anterior screw fixation
5) Anatomic fracture reduction
The incidence of osteonecrosis following displaced talar neck fractures is most related to the extent of initial fracture displacement. With increasing fracture displacement, the tenuous vascular supply to the talar body is more at risk for damage, thereby increasing the risk of osteonecrosis. Although displaced talar neck fractures have historically been considered a surgical emergency, recent studies have shown that the timing of surgical intervention bears no impact on the development of osteonecrosis. While nicotine use has an influence on fracture healing, it has never been shown to be a factor in osteonecrosis, nor has posterior-to-anterior screw fixation or the quality of fracture reduction.
A 32-year-old woman sustained a closed calcaneus fracture 2 years ago and was treated nonsurgically. She now reports a 6-month history of progressively worsening pain over the anterior ankle and lateral hindfoot. Climbing stairs and ascending slopes is particularly difficult for her. Bracing and intra-articular corticosteroid injections have not provided sufficient relief. Figure 36 shows a weight-bearing lateral radiograph. What is the most appropriate surgical option?
1) Subtalar arthrodesis in situ with plantar flexion osteotomy of the talar neck
2) Distraction subtalar arthrodesis with a corticocancellous bone block autograft
3) Subtalar arthrodesis in situ
4) Triple arthrodesis
5) Subtalar arthrodesis in situ with anterior ankle exostectomy
Intra-articular fractures of the calcaneus often include depression of the posterior facet of the subtalar joint. This can lead to dorsiflexion of the talus because of diminished height posteriorly. In a weight-bearing position, the dorsal surface of the talar neck can impinge against the distal tibia, causing anterior ankle pain. In addition, posttraumatic arthritis of the subtalar joint typically occurs after a calcaneus fracture. The patient’s symptoms are consistent with both anterior ankle impingement and subtalar degenerative arthritis. The Bohler angle, approximately 15 degrees, confirms depression of the posterior facet. Distraction subtalar arthrodesis with a corticocancellous bone block autograft will improve talar declination, decrease anterior impingement, and address the subtalar degenerative arthritis simultaneously.
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?
1) Reduces shrinkage of the residual limb
2) Creates a more stable platform for load transfer
3) Reduces wound healing complications by avoiding the soft-tissue dissection necessary to transect the fibula at a level proximal to the tibia
4) Connecting bone strut provides an attachment point for more effective
myodesis
5) Allows a more proximal resection level to decrease tension on the wound
The Ertl modification of a below-knee amputation has been proposed to create a more stable “platform” to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area.
Early studies have suggested that this modification may enhance the patient’s perceived functional outcome.
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
1) Irrigation and debridement of the cystic lesion and 6 weeks of IV antibiotics
2) Curettage, debridement of nonviable bone, and placement of absorbable
antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics
3) Complete resection of the infected portion of bone, placement of an external fixator to stabilize the tibia, and 6 weeks of IV antibiotics
4) Amputation
5) Local debridement of bone and the overlying skin and soft tissues, 6 weeks of IV antibiotics, and free-flap wound coverage
The patient has chronic tibial osteomyelitis that is due to low virulent bacteria. The history and studies do not suggest the need for an amputation or a free-flap procedure. This is a localized tibial infection that is in a healed bone; there is no need to resect the entire area of the tibia bone around the infection. The most appropriate treatment is curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics. Studies have shown that in cases of localized osteomyelitis that are of low virulence, as little as 1 week of IV antibiotics followed by 6 weeks of oral antibiotics is successful.
A 59-year-old woman underwent open reduction and internal fixation (ORIF) of her ankle 6 months ago, with subsequent hardware removal 3 months later. She now reports persistent, diffuse ankle pain, swelling, and limited range of motion. Figure 48 shows an oblique radiograph of the ankle. What is the next most appropriate step in management?
1) Physical therapy
2) Hardware removal
3) Repeat placement of a syndesmotic screw
4) Deltoid ligament reconstruction
5) Revision ORIF with exploration of the syndesmosis and medial ankle
The radiographs demonstrate persistent widening of the medial clear space with an ossicle. This represents soft-tissue interposition-scar tissue, the deltoid ligament, or the posterior tibialis tendon. Physical therapy will not improve the symptomatic malalignment. Hardware removal would be indicated for pain localized to the lateral fibula. Repeat syndesmotic screw fixation alone will not reduce the malalignment. Deltoid ligament repair may be necessary but will need to be combined with debridement of the medial ankle and syndesmosis, as well as repeat placement of one or more syndesmotic screws to maintain the reduction.
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight.
Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
1) Cephalosporin
2) Cephalosporin and aminoglycoside
3) Cephalosporin and penicillin
4) Cephalosporin and vancomyacin
5) Cephalosporin, aminoglycoside, and penicillin
A farm injury is automatically considered a grade III (Gustillo classification) injury regardless of size, energy, or additional soft-tissue injury due to the likelihood of substantial contamination. Antibiotic recommendations for grade III injuries include a first- or second-generation cephalosporin with an aminoglycoside or fluoroquinolone within 3 hours of injury, with penicillin added for farm injuries.
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
1) Methotrexate
2) Gold
3) Hydroxychloroquine
4) TNF-a inhibitors
5) Smoking
Clinical studies have shown that smoking cessation for 4 weeks reduces the risk of infection to the level of nonsmokers. Adverse effects on wound healing caused by chemotherapy used to treat rheumatoid arthritis has not been borne out in the literature.
Your 25-year-old patient complains of anterior knee pain after retrograde femoral nailing for a diaphyseal fracture and asks you why you didn’t perform antegrade nailing as he has seen on the internet.
You tell him that retrograde nailing is your preferred technique over antergrade nailing for diaphyseal femoral fractures because it has been shown to have which of the following?
1) Increased rate of union
2) Decreased rate of infection
3) Shorter operative time
4) Lower rates of hip pain
5) Lower rates of knee pain
Patients with retrograde femoral nails commonly have knee pain, while antegrade nails commonly have hip pain, abductor weakness and heterotopic ossification of the abductors.
Ostrum’s randomized prospective study of 100 patients with reamed femoral nails found 22% of antegrade nail patients had proximal hip pain, weak hip abductors or trendelenburg gait. No significant difference was found in set-up time, operative time, knee motion or pain, or infection rates.
Ricci performed a retrospective study of 293 fractures and found that the antegrade femoral nail group had more hip pain (10% vs 4%) and the retrograde nail group had more knee pain (36% vs 9%). There was no difference in healing, malunion, non-union or other complications.
Tornetta performed a randomized controlled comparison of 69 femur fractures and found more problems of length and rotation using a retrograde nailing.
There was no difference in time to union, operating time, blood loss, complications, size of nail or reamer, or transfusion requirements.
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
1) Zone 1 (the ala)
2) Zone 2 (the foramina)
3) Zone 3 (the central canal)
4) Zones 1 and 2
5) The sacral laminae
Denis divided the sacrum into three zones: zone 1 represents the lateral ala, zone 2 represents the foramina, and zone 3 represents the central canal. A fracture is classified according to its most medial extension. Those in zone 3
are typically bursting-type fractures or fracture-dislocations and are most prone to neurologic sequelae.
A 31-year-old male sustains the injury shown in Figure A. As compared to treatment with a simple sling, what is the primary advantage of treatment with a figure-of-eight brace?
1) Decreased sleep disturbance
2) Decreased personal care and hygiene impairment
3) Decreased rates of malunion
4) Improved long-term clinical outcomes
5) No advantage, equivalent result between a simple sling and figure-of-eight brace
Figure of eight braces have been shown to have no differences as compared to simple slings in regard to healing times, healing rates, and alignment at final follow-up.
The referenced study by Andersen et al is a Level 1 randomized controlled study showing equivalent cosmetic and clinical outcomes with sling versus figure of eight bracing despite increased sleep disturbances and increased rate of personal care impairment in those treated with a figure of eight brace.
The second referenced study by Nordqvist et al is a Level 4 case series designed to analyze the long-term outcome of mid-clavicle fractures in adults and to evaluate the clinical importance of displacement and fracture
comminution. They found a 39/225 rate of moderate shoulder pain with figure of eight bracing. Overall they concluded that few patients with fractures of the mid-part of the clavicle require operative treatment.
A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?
1) Bone grafting and revision open reduction and internal fixation
2) Hemiarthroplasty
3) Dynamic hip screw without angular correction
4) Valgus intertrochanteric osteotomy
5) Core decompression
Femoral neck fracture nonunion is a challenging problem for orthopaedic surgeons. Vertical fractures are more prone to nonunion due to shear stress rather than compressive forces across the fracture site. Several authors have suggested these fractures are more common in young adults due to injury type and bone composition. It is widely regarded that an effort should be made to salvage the femoral head if vascularity remains. The most common method to treat this complication is valgus intertrochanteric osteotomy of the femur. This functionally makes a vertical fracture more horizontal, converting shear into
compressive forces. It also helps correct the varus position of the fracture nonunion.
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?
1) Anterior column
2) Anterior wall
3) Posterior column
4) Both column
5) Transverse
The fracture pattern shown in the radiographs is a fracture of the posterior column. The only line interrupted on the AP pelvis is the ilioischial line. The obturator oblique view shows that the iliopectineal line is intact as is the outline of the posterior wall. The iliac oblique view shows an interruption of the ilioischial line and an intact anterior wall. Therefore, this fracture is a fracture of the posterior column.
Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?
1) Open reduction and internal fixation of the radial head and immobilization
2) Medial collateral ligament repair
3) Radial head replacement, ulnar nerve transposition, and external fixation
4) Coronoid repair, radial head replacement, and lateral ligamentous repair
5) Nonsurgical management in a hinged elbow brace
This elbow fracture-dislocation involves a radial head fracture, coronoid fracture, and ulnohumeral dislocation (terrible triad). Several algorithms exist for treatment; surgical treatment is indicated. The treatment should address the radial head. Studies have shown replacement to be superior to repair in comminuted fractures. The coronoid may be addressed in unstable cases at the time of radial head excision and replacement. Lateral ligamentous repair is carried out during closure of the lateral elbow capsule. Medial ligamentous repair also may be undertaken but usually in concert with bony repair. Hinged
external fixation remains an option when instability exists following bony and soft-tissue repair. Acute ulnar nerve transposition is rarely indicated.
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
1) Irrigation and debridement, external fixation of the ankle and foot, traction and pinning of the femur, open reduction and internal fixation of the forearm
2) Irrigation and debridement, external fixation of the ankle, foot, and femur, splinting of the forearm
3) Irrigation and debridement and open reduction and internal fixation of the ankle and foot, intramedullary nailing of the femur, open reduction and internal fixation of the forearm
4) Irrigation and debridement and open reduction and internal fixation of the ankle and foot, intramedullary nailing of the femur, splinting of the forearm
5) Irrigation and debridement, external fixation of the foot and ankle, intramedullary nailing of the femur, open reduction and internal fixation of the forearm
The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable.
Which of the following is most commonly associated with an open clavicular fracture?
1) Scapulothoracic dissociation
2) Closed head injury
3) Calcaneus fracture
4) Pelvic ring injury
5) Open tibial fracture
Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.
A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of
1) closed reduction and casting.
2) external fixation and percutaneous pinning of the distal radius.
3) open reduction and internal fixation of the distal radius.
4) open reduction and internal fixation of the distal radius and open repair of the ulnar styloid.
5) nonbridging external fixation of the distal radius.
The patient has a high-energy injury with resultant comminution of the distal radius metaphysis. Cast immobilization is likely to lead to radial shortening and angulation due to the comminution. Similarly, while external fixation and pinning has been successful in the past, some loss of radial length and volar angulation is typically noted. Present plate fixation devices for the distal radius employing locking screw technology have a superior ability to resist radial shortening and dorsal angulation. Fixation of the ulnar styloid is warranted when there is distal radioulnar joint instability or significant displacement of the styloid. This is more likely to occur with a fracture at the base of the styloid. In this instance, the distal radioulnar joint does not appear to be disrupted.
Following fixation of a displaced intra-articular fracture of the distal humerus through a posterior approach, what is the expected outcome?
1) Development of arthritic changes at 1 year
2) Restoration of full elbow range of motion
3) Loss of approximately 25% of elbow flexion strength
4) Posterolateral rotatory instability
5) Olecranon nonunion
Following repair of a displaced intra-articular distal humerus fracture, the ability to regain full elbow range of motion is rare. Recent reports of olecranon osteotomy have yielded healing rates of between 95% to 100%. According to McKee and associates, patients can be expected to have residual loss of elbow flexion strength of 25%.
A 28-year-old cowgirl was injured while herding cattle 1 week ago. A radiograph and CT scans are shown in Figures 13a through 13c. What is the most appropriate management for this injury?
1) Nonsurgical management and gradual weight bearing as tolerated
2) Nonsurgical management and restricted weight bearing
3) Placement of a pelvic binder
4) Open reduction and internal fixation of the symphysis
5) Open reduction and internal fixation of the symphysis and iliosacral screws
The patient has an AP I pelvic ring disruption with minimal symphyseal widening. The best treatment is nonsurgical management and weight bearing as tolerated. This will help close the anterior pelvic ring during the healing process. Pelvic binders are excellent for acute treatment of widely displaced pelvic fractures but are not recommended for long-term use. Open reduction and internal fixation is not indicated for this injury and furthermore, the posterior ring is not injured.
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
1) AIDS
2) Polytrauma
3) Pelvic fracture
4) Pilon fracture
5) Acute myocardial infarction (AMI)
Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb “feels” different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?
1) Serial physical examinations
2) Angiography
3) Duplex ultrasound examination
4) Ankle-brachial index (ABI)
5) Measurement of compartment pressures
The patient initially has a distal third femoral fracture and a pulseless limb. The first step is to reduce the fracture and reassess the vascular status. Although the pulse returns, it feels different than the quality of the pulse in the contralateral uninjured extremity. There is a risk of a vascular injury with this fracture pattern due to tethering of the femoral vessels at the adductor hiatus; therefore, the vascular status needs further assessment since the pulses are not symmetrical. A physical examination is not very accurate in assessing whether a vascular injury is present; therefore, serial examinations are not appropriate. Angiography is very sensitive and specific but is time consuming and can cause complications secondary to the dye and the arterial puncture required to perform it. Duplex ultrasound is effective but is very operator-dependent and may not be available 24 hours a day. The ABI is easily performed and has been shown to be sensitive and specific. If the value is greater than 0.9, the negative predictive value is 99% and when the value is less than 0.9, it is 95% sensitive and 97% specific for a major arterial injury. It has been shown to be useful for blunt lower extremity injuries as well as knee dislocations.
What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?
1) Total elbow arthroplasty
2) Functional hinge bracing
3) Long arm casting
4) Crossed Kirschner wires
5) Dual column plates
This intra-articular distal humerus fracture with displacement at the joint surface is best treated with surgical fixation. The most biomechanically sound construct is two plates applied to either column 180 degrees from one another. Elbow arthroplasty is most appropriate for low demand elderly patients.
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury?
1) Inlet and outlet views of the pelvis to better delineate the injury
2) Angiography
3) Laparotomy
4) Open reduction and internal fixation of the pelvis
5) Placement of a pelvic binder around the patient
This hypotensive patient has an obvious open book injury of the pelvic ring on the AP pelvis radiograph and further radiographs are not needed prior to the
initiation of treatment. Although angiography may be indicated if he does not respond to stabilization of his pelvis and fluid/blood administration, temporary stabilization of the pelvis with a sheet or binder should be performed first because it is simple, quick, and has been shown to be effective. This patient does not need a laparotomy at this point since the FAST examination did not show any free intra-abdominal fluid and his chest radiograph was unremarkable, leaving the most likely source of bleeding the pelvic fracture.
Open reduction with internal fixation of a pelvic injury is not indicated in an acutely ill patient.
A 220-lb 20-year-old man was involved in a motor vehicle accident. His work-up reveals that he has multiple long bone fractures as well as a splenic injury that is currently being managed nonsurgically. His initial blood pressure in the trauma bay was 70/30 mm Hg. After receiving 4 liters of fluid and 3 units of packed red blood cells, his blood pressure is currently 110/70, his heart rate is 100, his urine output is 90 mL/h (normal 0.5 to 1 mL/kg/h), and his core temperature is 97.9 degrees F (36.5 degrees C). At this point, the patient’s resuscitation can be described as which of the following?
1) Complete based on the normalization of his blood pressure, urine output, and heart rate
2) Cannot be determined based on the data presented
3) Incomplete based on his fluid requirements calculated using his initial blood pressure as a measure of blood volume loss
4) Incomplete since he will need surgery on the long bone fractures and should be “tanked up” prior to losing blood in the operating room
5) Incomplete based on his heart rate
Although the end points of resuscitation are still unclear, what is known is that normalization of the standard hemodynamic parameters (blood pressure, heart rate, and urine output) is not adequate. Up to 85% of patients with normal hemodynamic parameters can still have inadequate tissue oxygenation or uncompensated shock. The initial base deficit, lactate level, or gastric pHi can be used to stratify patients for resuscitation needs, risks of death, and multiple organ failure (level 1 evidence). The time it takes to normalize the base deficit, the lactate level, or gastric pHi, can predict survival (level 2 evidence). Patients who have been in uncompensated shock (abnormal vital signs) should have their resuscitation monitored using data other than vital signs.
A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
1) Continued nonsurgical management
2) Posterior open reduction and internal fixation with tension band plating
3) Posterior iliosacral screws
4) Anterior open reduction and internal fixation
5) Anterior open reduction and internal fixation and posterior fixation
Fortunately, surgical treatment of sub-acute pelvic ring injuries is relatively uncommon as acute management has become more common. Delayed reconstruction of pelvic ring malunion and impending malunion is rare.
Nonsurgical management may have a role as long as the hemipelvis does not flex, shorten, and/or externally rotate. The AP pelvic radiograph suggests that all three motions are happening in this patient. These are just a few of the indications to repair the pelvic ring and this is best done with anterior and posterior fixation. Anterior symphyseal plating will help correct most of the deformity. Posterior fixation can and should be added to lessen the forces on the anterior ring reconstruction when repair is performed in a sub-acute or delayed fashion. Posterior fixation can help obtain a more anatomic reduction and helps decrease the risk of anterior hardware failure.
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?
1) Immobilization of the wrist in ulnar deviation for 4 weeks before starting range-of-motion exercises
2) In situ Kirschner wire fixation of the carpal bones for 6 weeks
3) Extending the volar incision used for fracture fixation and repairing the injured structures in addition to percutaneous Kirschner wire fixation
4) Performing a separate dorsal incision and repairing the injured structures in addition to percutaneous Kirschner wire fixation
5) Arthroscopic repair of the injured structures and percutaneous Kirschner wire fixation
The intraoperative radiograph reveals a scapholunate ligament disruption. Repair of the stout dorsal scapholunate interosseous ligaments is required. Interestingly, the results of scapholunate ligament injuries associated with distal radius fractures appear to be superior to those of isolated ligament injuries.
A 36-year-old woman is placed in a short arm cast for a nondisplaced extra-articular distal radius fracture. Seven weeks later she notes the sudden inability to extend her thumb. What is the most likely cause of her condition?
1) Posterior interosseous nerve palsy
2) Cervical disk herniation
3) Entrapment of the flexor pollicis longus tendon
4) Rupture of the extensor pollicis longus tendon
5) Metacarpophalangeal joint dislocation
A recent review of 200 consecutive distal radius fractures noted that the overall incidence of extensor pollicis longus rupture was 3%. The causes are believed to be mechanical irritation, attrition, and vascular impairment. The fracture is usually nondisplaced and the patient notes weeks to months after injury the sudden, painless inability to extend the thumb. Treatment involves extensor indicis proprius tendon transfer or free palmaris longus tendon grafting.
In Gustilo type III open tibial diaphyseal fractures, which of the following factors is associated with an increased risk of a poor functional outcome?
1) Soft-tissue coverage within 3 days of injury
2) Bone grafting 3 months after injury
3) Wound debridement within 6 to 24 hours from injury
4) Definitive treatment with external fixation
5) Free tissue transfer for soft-tissue coverage
According to the published outcomes analyses from the Lower Extremity Assessment Project (LEAP) study group of patients prospectively followed for 2 to 7 years, definitive fixation with an intramedullary nail has shown improved outcomes when compared to definitive external fixation. The findings showed that the timing of wound debridement (within 6 hours from injury as compared to within 6 to 24 hours), the timing of soft-tissue coverage (3 days or less from injury as compared to more than 3 days), and the timing of bone grafting after injury (within or after 3 months) did not impact the infection or union rates and had no effect on functional outcome. The LEAP study has shown at 7-year follow-up that patients who are definitively treated with external fixation have a significantly longer time to union, poorer functional outcomes, longer time to achieve full weight bearing, and more time in the hospital.
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
1) closed reduction and splinting.
2) open reduction and internal fixation through a volar approach.
3) external fixation and Kirschner wire fixation.
4) intrafocal pinning and casting.
5) acceptance of alignment and bracing.
Definitive treatment decisions for displaced distal radius fractures in the elderly are based on a number of factors related to the fracture pattern and patient demographics. The first step in any treatment algorithm is a closed reduction and splinting with reassessment of alignment parameters. This is an extra-articular fracture with dorsal angulation. Low-demand elderly patients can be treated well with accepted minor malreduction.
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome?
1) His clinical outcome will correlate closely with his initial reduction.
2) His outcome will correlate with his radiographic score on the Ankle Osteoarthritis Score.
3) He will likely require a late ankle arthrodesis.
4) He will demonstrate marked limitations with regard to recreational activities.
5) He will perceive improvements for a period of over 2 years.
Marsh and associates retrospectively reviewed 56 tibial plafond fractures and found that the patients perceived improvement in their function and pain for an average of 2.4 years. They demonstrated some limitations in recreational activities but not marked limitations. Patients were unlikely to need a late arthrodesis (13%), and their outcomes did not correlate well with assessments of reduction or arthritis scores.
The injury shown in Figure 24 was most likely caused by what mechanism of injury?
1) Anterior posterior compression
2) Lateral compression
3) Vertical shear
4) Combined mechanism
5) Flexion-rotation
The CT cut shows a fracture through the posterior portion of the iliac wing or a crescent fracture. This occurs after a laterally directed force is applied to the anterior part of the involved iliac wing.
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?
1) Functional bracing
2) Hanging long arm cast immobilization
3) Intramedullary nailing
4) Open reduction and internal fixation, radial nerve exploration
5) External bone stimulator
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated.
Which of the following is most predictive of a medial side ankle injury in the presence of a fibula fracture above the level of the joint?
1) Severe medial ankle tenderness
2) Severe medial ankle ecchymosis
3) Stress radiographs showing the medial clear space measuring 6 mm and the superior joint space measuring 3 mm
4) Inability to ambulate
5) Medial ankle swelling
Isolated Lauge-Hansen supination-external rotation-type ankle fractures comprise 20% to 40% of ankle fractures and nonsurgical management is effective for managing SER-2 ankle fractures. Tornetta and associates recently showed that medial ankle tenderness, ecchymosis, and swelling are not reliable findings when trying to determine deltoid competence. Stress radiographs showing a medial clear space of greater than 4 mm or one that is also 1 mm greater than the superior joint space, or any lateral talar subluxation are indicative of deltoid incompetence and indicative of a SER-4 ankle fracture.
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure
34/. What is the next most appropriate step in the orthopaedic management of this patient?
1) Axillary view
2) CT of the shoulder
3) Closed reduction
4) Sling and close follow-up
5) Functional brace
The next step in the management of this injury is completion of the shoulder trauma series. An axillary radiograph, which can be quickly performed in the emergency department, must be obtained to accurately assess the humeral head relationship to the glenoid. If difficulty is encountered, a “Velpeau” axillary may be substituted. If that fails to elucidate the status of the glenohumeral joint, a CT scan should be obtained.
Which of the following findings best describes the acetabular fracture shown in Figure 38?
1) Posterior column with articular impaction and a free fragment
2) Anterior column with articular impaction
3) Posterior wall with an intra-articular fragment
4) Posterior wall with articular impaction and a free intra-articular fragment
5) Posterior wall with articular impaction
The CT scan shows a posterior wall fracture with impaction of the articular surface and a free fragment within the joint. Proper treatment of this injury requires not only reduction and fixation of the posterior wall fragment but also removal of the free fragment and elevation of the depressed articular segment.
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
1) normal sexual function and normal vaginal childbirth.
2) sexual dysfunction (dyspareunia) and normal vaginal childbirth.
3) normal sexual function and caesarean section childbirth.
4) sexual dysfunction (dyspareunia) and caesarean section childbirth.
5) normal sexual function and caesarean section childbirth until hardware removal.
Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is
almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not.
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?
1) Closed treatment and casting
2) Open reduction and internal fixation
3) Primary subtalar arthrodesis
4) Percutaneous fixation
5) External fixation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures.
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
1) Radial head resection, open reduction and internal fixation of the coronoid, and medial collateral ligament repair
2) Radial head resection and lateral collateral ligament repair
3) Radial head arthroplasty alone
4) Radial head arthroplasty and lateral collateral ligament repair
5) Radial head arthroplasty, open reduction and internal fixation of the coronoid, and lateral collateral ligament repair
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region.
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal
1) Reamed intramedullary nailing
2) Traction
3) External fixation
4) Open plating
5) Mast suit
The patient has several indications that he is not ready for definitive fixation of the femoral shaft fracture at this point. He is cold with a core temperature of 93 degrees F, and hypothermia of less than 95 degrees F (35 degrees C) has been shown to be associated with an increased mortality rate in trauma patients. The patient has also not been resuscitated based on his increasing lactate levels and although controversial, it has been shown that temporary external fixation leads to a lower incidence of multiple organ failure and acute respiratory distress syndrome.
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?
1) MRI scan
2) Physical examination
3) Workers’ compensation status
4) Surgeon availability
5) Patient age
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
1) Consult the ethics committee before giving blood.
2) Use cell saver blood.
3) Ask the patient’s family for consent to give blood.
4) Use plasma expanders.
5) Give the patient blood.
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah’s Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah’s Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open wound is not recommended nor would there likely be enough from an open pelvic fracture to salvage. The patient’s family may be expressing their own beliefs rather than the patient’s beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability.
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and
1) talectomy.
2) reimplantation of the talus.
3) reimplantation of the talus with acute triple arthrodesis.
4) Syme amputation.
5) transtibial amputation.
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures.
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
1) Spiral
2) Oblique
3) Transverse
4) Segmental
5) Comminuted
A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism.
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?
1) Kocher-Langenbeck
2) Iliofemoral
3) Ilioinguinal
4) Extended iliofemoral
5) Triradiate approach
The fracture is an associated both column fracture. The best approach for this fracture is the ilioinguinal. The Kocher-Langenbeck is best for posterior injuries to the acetabulum and some transverse fractures. The iliofemoral alone is limited to high anterior column injuries. The extended iliofemoral and triradiate
approaches although useful for this fracture, have a higher rate of complications.
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
1) plating of the radial shaft fracture then open repair of the triangular fibrocartilage complex.
2) open reduction and internal fixation of the radius and ulna.
3) plating of the radius then closed reduction and evaluation of the distal radioulnar joint (DRUJ).
4) closed reduction of the radius and DRUJ.
5) plating of the radius then pinning of the DRUJ in pronation.
This Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction of the radial shaft and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. If not, either open or closed reduction with pinning is undertaken. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?
1) Chronic osteomyelitis
2) Planovalgus hindfoot
3) Plantar nerve entrapment
4) Wound dehiscence
5) Painful hardware
The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence.
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
1) A primed immune system with an increased risk of a systemic inflammatory response
2) Nothing since they are no longer in uncompensated shock and their vital signs have normalized
3) Higher nonunion rates after fracture fixation
4) Higher infection rates after definitive fracture fixation
5) Higher complication rates after temporizing external fixation of long bone fractures
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a “primed” immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered.
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is
intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?
1) Emergent four compartment fasciotomies
2) Emergent four compartment fasciotomies and open reduction and internal fixation of the fracture
3) Elevation of the limb overnight and four compartment fasciotomies in the morning
4) Elevation of the limb overnight and a recheck of compartment pressures in the morning
5) Emergent MRI of the knee and leg
The patient has a compartment syndrome based on the firm compartments of the leg and the elevated compartment pressures measured at the diastolic pressure reading. Muscle ischemia occurs quickly when compartment pressures are elevated, and within 6 hours irreversible damage can occur. Emergent fasciotomies permit decompression of all four compartments and reestablishment of vascular supply to the muscles. Stabilization of the fracture prevents further soft-tissue injury.
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
1) The mean arterial blood pressure is above 90 mm Hg.
2) The pulse pressure has normalized.
3) Urine output is greater than 0.5 to 1 mL/kg/h.
4) Oxygen delivery has been maximized.
5) Aerobic metabolism has been restored in all tissue beds.
Shock can be defined as inadequate tissue perfusion. Resuscitation or the resolution of shock is defined as when oxygen debt has been repaid, tissue acidosis is eliminated, and aerobic metabolism has been restored in all tissue beds. The end points for resuscitation are not clearly defined, but occult shock can still be present in the setting of normal vital signs and normal urine output due to selective perfusion of organ systems.
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
1) Infection
2) Malunion
3) Loss of forearm rotation
4) Refracture
5) Delayed union/nonunion
Healing of forearm fractures in skeletally immature patients is the usual outcome. The use of intramedullary fixation has been reported to result in a lower frequency of refractures when compared to plate osteosynthesis due to the absence of diaphyseal holes after plate removal, which are considered stress risers. Regardless of implant technique, malunion and infection are infrequent. Loss of forearm pronation and supination is a common occurrence in surgically treated fractures due to the higher degree of soft-tissue injury, and periosteal stripping leads to fracture site instability and fracture comminution.
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
1) Anterior superior iliac spine
2) Sciatic buttress
3) A column of bone running from the anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS)
4) The most superior portion of the roof of the acetabulum
5) Iliopectineal line
The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures.
A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure
62/. Based on these findings, what is the most appropriate treatment?
1) Electrical stimulation
2) Bone grafting
3) No weight bearing
4) Bone grafting and compression plating
5) Free vascularized bone transport
Nonunions after intramedullary nails are often treated with exchange reamed nailing. In a recent study, this resulted in a union rate of 53%. After failed exchange nailing, bone grafting and compression plating should be used. The other options resulted in less satisfactory results as compared to bone grafting and compression plating.
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?
1) Peroneal tendon tear
2) Lateral process talus fracture
3) Talar neck fracture
4) Lisfranc injury
5) Deltoid ligament tear
This cuboid compression fracture (“nutcracker” injury) is associated with subtle injury to the Lisfranc complex. This diagnosis must be made to ensure proper treatment.
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
1) Posterior column/posterior wall acetabular
2) Associated both column acetabular
3) Transverse plus posterior wall acetabular
4) Anterior column posterior hemitransverse acetabular
5) Anterior column acetabular
The radiographs and CT scans reveal an anterior column acetabular fracture. The fracture has quadrilateral plate extension but does not exit out the posterior column. The CT scans confirm an intact posterior column and no wall fracture. A transverse fracture is best seen on the CT scan and runs in the sagittal plane, not the coronal plane.
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture.
Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
1) Long arm cast immobilization
2) Total elbow arthroplasty
3) Open reduction and internal fixation
4) Osteoarticular allograft
5) Resection arthroplasty
Several studies have documented the satisfactory outcomes of total elbow arthroplasty when osteosynthesis is not feasible for fixation of a distal humerus fracture, particularly in the physiologically older patient with low functional demands. Total elbow arthroplasty should be considered when a comminuted intra-articular distal humerus fracture occurs in a woman older than age 65 years, particularly with such associated comorbidities as systemic steroid use, osteoporosis, or rheumatoid arthritis.
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
1) Cast removal and measurement of carpal canal pressure
2) Immediate carpal tunnel release and pinning of the fracture
3) Continued observation
4) Surgical reduction and pinning of the fracture
5) Electromyography/nerve conduction velocity studies
The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural
compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression.
A 25-year-old male polytrauma patient undergoes initial temporary external fixation for a femoral shaft fracture. He is converted to a femoral nail at 7 days. This management can be expected to result in
1) higher infection rates.
2) higher nonunion rates.
3) equal union and infection rates.
4) higher rate of ARDS.
5) higher mortality rate.
Recently Harwood and associates investigated the principles of damage control orthopaedics (DCO) as they apply to patients with femoral shaft fractures.
When they compared those who underwent initial external fixation of femoral shaft fractures with conversion to an intramedullary nail to those who underwent intramedullary nailing as their initial treatment, they found the following: overall infection rates were comparable in patients receiving DCO versus primary intramedullary fixation; open fracture was an independent risk factor for infection regardless of the treatment method; contamination rates in external fixator pin sites rose considerably when left in place more than 2 weeks and logistic regression analysis suggests that infection rates may increase when conversion to an intramedullary nail occurs after 2 weeks following external fixation; and there was no significant difference in time to union among treatment groups.
Which of the following is the most stable construct for fixation of an unstable transforaminal sacral fractures?
1) External fixation
2) Iliosacral osteosynthesis
3) Combined iliosacral and lumbopelvic fixation (triangular osteosynthesis)
4) Anterior pelvic ring plating with bilateral sacroilliac percutaenous screw fixation
5) Transiliac bars with anterior pelvic ring plating
Combined iliosacral and lumbopelvic fixation (triangular osteosynthesis) for sacral fractures has the greatest stiffness when used for an unstable sacral fracture.
The referenced article by Schildhauer et al is a cadaveric study that examined the biomechanical properties of different fixation constructs under cyclic loading and demonstrates that triangular osteosynthesis for unstable transforaminal sacral fractures provides significantly greater stability than iliosacral screw fixation under in-vitro cyclical loading.
Illustration below shows the radiographic appearance of lumbopelvic fixation. The addition of iliosacral fixation would complete triangular osteosynthesis.
The Cotton test evaluates which of the following structures?
1) Calcaneofibular ligament
2) Lateral ulnar collateral ligament of the elbow
3) Ligamentum flavum
4) Anterior talofibular ligament
5) Ankle syndesmosis
The inferior tibiofibular syndesmosis is a fibrous articulation consisting of four ligaments; the elasticity of these ligaments permits axial, vertical, anterior, posterior, and mediolateral motion at the ankle syndesmosis during weight bearing.
Of note, the Cotton test was originally described around 1910 by Frederic J. Cotton as the "talar glide test" evaluating the medial/lateral translation of the talus in the mortise. A positive result indicates disruption of the ankle syndesmosis in the face of an ankle injury.
Nielson et al reported that the level of the fibular fracture does not correlate reliably with the integrity or extent of the interosseous membrane (IOM) tears identified on MRI in operative ankle fractures. Therefore, one cannot consistently estimate the integrity of the IOM and subsequent need for transsyndesmotic fixation based solely on the level of the fibular fracture. This supports the need for intraoperative stress testing (ie, external rotation stress or Cotton test) of the ankle syndesmosis in all operative ankle fractures.
The study by Leeds et al noted a correlation between syndesmosis reduction (initial and final) and outcomes (radiographic and clinical).
The attached video shows the Cotton test during an ankle fixation procedure.
A comminuted femoral shaft fracture is treated with an intramedullary nail locked with a single distal screw. What is the most likely mode of failure of the screw?
1) Screw pulls out of the cortical shaft
2) Screw head breaks off due to bending stresses
3) Shaft of the screw fractures in the region that is inside the nail
4) Screw threads are damaged by fretting against the edges of the holes in the nail
5) Screw bends excessively
The screw is being loaded and pushed distally at the two points where it contacts the walls of the nail, and it is being pushed proximally at the two points where it contacts the cortex, ie, near the head and tip of the screw. This places the screw in four-point bending, producing tensile stresses on the
inferior side of the screw and compressive stresses on the superior side. The tensile stresses, combined with stress risers at the screw threads, eventually could lead to fatigue fracture of the screw. Because the cortices in the metaphysis are far apart, the bending moment is large and, therefore, stresses near the midshaft of the screw produced by bending are much larger than shear stresses in this case. Pullout of the screw is unlikely because the loads are not directed along the axis of the screw. There are no bending stresses at the ends of the screw. A bent screw may be difficult to remove, but this would not likely cause failure of the fixation.
A 30-year-old female presents with the injury shown in Figure A after falling on her outstretched arm. During operative treatment of the fracture, anatomic reduction of the radius is achieved. However, the surgeon is unable to reduce the distal radioulnar joint. What structure is most likely impeding the reduction?
1) Median nerve
2) Flexor carpi radialis
3) Pronator quadratus
4) Extensor carpi ulnaris
5) Flexor carpi ulnaris
Figure A shows a Galeazzi fracture (distal 1/3 radial shaft fracture with associated distal radioulnar joint dislocation). In this injury, an inability to reduce the distal radioulnar joint in a closed fashion is most commonly secondary to interposition of the extensor carpi ulnaris tendon. Early recognition of the dislocation of the ulna and ECU into the DRUJ and their significance may avoid poor results.
The referenced study by Biyani et al reports a case in which both the extensor carpi ulnaris and extensor digiti minimi tendons were displaced on either side of the ulnar head.
The referenced study by Budgen et al presents a case of a Galeazzi fracture dislocation with an irreducible distal radioulnar joint.
The referenced study by Paley et al reports two cases of distal radioulnar joint (DRUJ) disruption and diastasis secondary to distal radial fractures that were associated with displacement of the ulnar styloid and extensor carpi ulnaris (ECU) into the DRUJ. Both cases had a palpable empty ECU tendon sulcus.
What is the antibiotic of choice for gonococcal septic arthritis of the knee?
1) Erythromycin
2) Penicillin
3) Tetracycline
4) Ceftriaxone
5) Vancomycin
Gonococcal septic arthritis, caused by the gram-negative diplococcus Neisseria gonorrhoeae, typically affects two age groups: newborns and adolescents. The level of penicillin and tetracycline resistance in Neisseria gonorrhoeae is so high that it is completely ineffective in most parts of the world. A third-generation cephalosporin such as ceftriaxone is recommended in most areas. Fluoroquinolones may be an alternative treatment option if antimicrobial susceptibility can be documented by culture. In areas where co-infection with chlamydia is common, doxycycline may be used with ceftriaxone.
An above-the-knee amputation is performed 12 cm above the joint line. What is the best management of the adductor muscle group?
1) Resection of the adductors to prevent adductor contracture
2) Shortening and reattachment to the mid-femur to improve biomechanics
3) Myodesis to the distal end of the bone
4) Transfer to the quadriceps to improve hip flexion
5) Attachment to the hamstrings
The best socket fit requires resection of the wide flair of the condyles and amputation approximately 12 cm above the joint line. The adductor magnus is a very important muscle that participates in achieving a more efficient gait.
Myodesis of the bone through drill holes near the cut end of the bone has been shown to improve biomechanics.
In determining the FRAX score (fracture risk assessment tool), the World Health Organization determined that which of the following risk factors is not contributory to the clinical risk of fracture in its population cohorts?
1) BMI (body mass index)
2) Spine T-score from DEXA scan (dual-energy absorptiometry)
3) Current smoking activity
4) Parental history of hip fracture
5) Prior history of fracture before age 50
The FRAX score calculates the clinical risk of fracture using bone mineral density of the femoral neck, BMI, current smoking activity, history of parental hip fracture, and prior personal history of fracture before age 50. The World Health Organization has developed this new fracture risk assessment tool to identify individuals at high risk of osteoporotic fracture. The current standard, which bases treatment decisions largely on bone mineral density measurement, has proven to be specific, but not sensitive, for the identification of patients at high risk of fracture. Because nearly 50% of postmenopausal women in the community older than age 50 years who suffer an osteoporotic fracture do not have osteoporosis defined by a BMD test and because of the limited availability of BMD in many countries, clinical risk factors were added to BMD to identify patients at high risk for osteoporotic fractures. The site and
reference technology is DEXA at the femoral neck. T-scores are based on the National Health and Nutrition Examination Survey reference values for women aged 20 to 29 years. The same absolute values are used in men. Although the model is constructed for BMD at the femoral neck, the total hip site is thought to predict fracture equivalently in women.
Glenohumeral disarticulation often leads to which of the following changes?
1) Hiking of the shoulder girdle
2) Hypertrophy of the amputated shoulder girdle
3) Improvement in thoracic spinal deformity
4) Protraction of the shoulder
5) Winging of the scapula
Postural abnormalities are common after high upper extremity amputation. Normally the weight of the upper extremity and the shoulder girdle muscles keep the shoulder balanced. When the arm is amputated and the scapula remains, the shoulder girdle muscles are unopposed, resulting in upward movement often called "hiking" of the shoulder girdle. In a growing child, removal of the entire upper limb can result in scoliosis of the spine due to muscle imbalance. Abnormal shoulder elevation can often be minimized by corrective exercises and wearing a shoulder prosthesis.
A 10-day-old girl has decreased active motion of the left upper extremity. The mother reports a difficult vaginal delivery with presumed shoulder dystocia. Examination shows full passive range of motion of the shoulder, elbow, and wrist but only active flexion of the fingers and wrist. Factors predictive of a good outcome include which of the following?
1) Breech delivery
2) Absence of an ipsilateral clavicle fracture
3) Horner's sign and an APGAR score of 10 at 1 minute
4) Return of active biceps before 3 months and preservation of full passive shoulder range of motion
5) Absent Moro and Babinski reflexes
Return of active biceps before 3 months and preservation of full passive shoulder range of motion are predictors of a good outcome. Breech delivery is usually associated with preganglionic injury. Preganglionic injury can result in a Horner's sign, which includes ptosis, myosis, and anhydrosis. Preganglionic injuries are unlikely to recover. The Moro reflex is elicited by dropping a baby's head a short distance and observing active elbow extension and fanning of the fingers, followed by elbow flexion and crying. Absence of the Moro reflex suggests a poor prognosis.
An 18-month-old child was involved in a motor vehicle accident and sustained an isolated injury to the left upper extremity. A radiograph is shown in Figure 33. What is the most appropriate management for this injury?
1) Hanging arm cast
2) Closed reduction with flexible intramedullary nail fixation
3) Coaptation splinting and bandaging the arm to the thorax
4) Closed reduction and external fixation
5) Locking plate fixation
Humeral shaft fractures in infants and young children heal rapidly and have excellent remodeling potential. Appropriate treatment in this age group is immobilization with a coaptation splint and bandaging the arm to the thorax for comfort. Internal fixation is appropriate in multiple trauma, and external fixation may be useful when soft-tissue injury is extensive.
If a percutaneous iliosacral screw is placed too anteriorly, and the screw exits anterior to the sacral ala before re-entering the sacral body, what will be the most likely finding postoperatively?
1) Lack of ankle dorsiflexion
2) Lack of ankle plantarflexion
3) Lack of knee extension
4) Loss of bowel and/or bladder control
5) Lack of great toe extension
This question is a simple review of anatomy and nerve innervation. The L5 root is at risk with an "in-out-in" screw, as described in the question, as the nerve root is just anterior to the sacral ala as it enters the true pelvis. L5 is primarily evaluated by extensor hallucis longus function. L4 is tested with tibialis anterior function and S1 by gastroc-soleus function (ankle plantarflexion).
A 10-year-old boy is struck by a car and sustains open left tibia and fibula fractures with bone protruding through a 7-cm laceration, multiple deep and superficial abrasions over the anterior leg, and road gravel is present in the wounds. His foot is warm and well-perfused with normal sensation and he has no pain with passive range of motion of the toes. Optimal treatment should consist of
1) irrigation and debridement of the fractures and application of an external fixator.
2) irrigation and debridement of the fractures and a reamed intramedullary nail.
3) irrigation and debridement of the fracture and percutaneous Kirschner wire fixation.
4) submuscular plating.
5) reduction and a short leg cast.
The patient has a grade 2 open fracture and therefore needs wound debridement as a first step, followed by fracture stabilization preferably with an external fixator. A reamed intramedullary nail is not indicated in a 10-year-old child with open growth plates. Submuscular plating is not needed in an open fracture and there is no mention of fracture debridement. Percutaneous Kirschner wires will not provide adequate fracture stabilization, nor will a short leg cast. Flexible nailing should be considered as another form of fixation.
Figures 5a and 5b show the radiographs of a 21-year-old wrestler who reports that his leg was rolled over while wrestling. The patient has decreased sensation and function in the distribution of the peroneal nerve, and he has absent pulses. What is the most appropriate initial management at this time?
1) Acute reconstruction of all ligamentous structures
2) Emergency MRI and reconstruction of all ligamentous structures
3) Emergency arteriogram followed by MRI
4) Emergency surgery with open reduction and repair of all torn structures with vascular surgery available
5) Closed reduction in the emergency room and reevaluation of the vascular status
The patient has an acute traumatic anteromedial dislocation of the knee with occlusion of the popliteal artery with a possible tear. Treatment should include reduction and reevaluation of the vascular status. At this time, if pulses are symmetric, observation may be appropriate without surgical intervention of the artery, but documentation with studies would be appropriate. Delayed reconstruction of injured structures is appropriate.
A 26-year-old male presents after a motor vehicle accident. Work-up reveals a closed left femoral shaft fracture, and an ipsilateral posterior wall fracture. He undergoes intramedullary nailing of the femur, and open reduction internal fixation of the posterior wall. He is treated with 25 mg of indomethacin three times daily for 6 weeks following an initial dose on the evening of surgery for heterotopic ossification prophylaxis. Which of the following is true regarding this post-operative treatment protocol?
1) It is associated with an increased rate of femoral shaft nonunion
2) It has no effect on the healing time of the posterior wall fracture
3) It is associated with a faster time to union
4) Indomethacin is superior to radiation treatment in the prevention of heterotopic ossification
5) There is a decreased rate of revision surgery needed when indomethacin is administered post-operatively
Heterotopic ossification (HO) prophylaxis with indomethacin has been shown to increase the risk of long-bone nonunion.
Indomethacin therapy has been shown to be an effective means of preventing HO formation, however literature has shown that it increases the risk of long bone and acetabular nonunion. Indomethacin works primarily by inhibiting IGF-1, which is a different mechanism from other NSAID's which typically inhibit the COX enzymes. IGF-1 is important for bone healing, and its inhibition may be a risk factor for delayed bone healing.
Burd et al performed a study to determine if patients with an acetabular fracture, who received indomethacin for prophylaxis against HO, were at risk of delayed healing or nonunion of any associated fractures of long bones. The study group consisted of 112 patients who had sustained at least one concomitant fracture of a long bone; of which 36 needed no prophylaxis, 38 received focal radiation and 38 received indomethacin. When comparing patients who received indomethacin with those who did not, a significant difference was noted in the rate of long bone nonunion (26% vs 7%).
Jordan et al performed a study to document the efficacy of variable treatment durations with indomethacin prophylaxis for HO and its effect on union of the posterior wall (PW) in operatively treated acetabular fractures. Patients were randomly assigned to one of four treatment groups: (1) placebo for 6 weeks,
(2) 3 days of indomethacin followed by placebo for a total of 6 weeks, (3) 1
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Krajbich reviews the management of pediatric patients with lower-limb deficiences and amputations. He advocates disarticulation as opposed to transosseous amputation when possible as bone overgrowth has not been observed in bone ends covered by articular cartilage.
O'neal et al retrospectively reviewed their rates of surgical revision for bone overgrowth in pediatric and adolescent amputees. The highest rates of revision were seen with metaphyseal-level amputations (50%) and with traumatic amputations (43%).
Benevenia et al reviewed their rates of overgrowth in skeletally immature transosseous amputees using an autogenous epiphyseal transplant from the amputated limb to cap the medullary canal. They found that only 1 of 10 patients undergoing amputation with this technique had complications due to bone overgrowth, compared with 6 of 7 patients undergoing traditional transosseous amputation.
Illustration A is a clinical photo of bone overgrowth eroding through the soft tissue in a transhumeral amputee. Illustration B demonstrates the radiographic appearance of bone overgrowth in a transtibial amputation.
Incorrect Answers:
. Neurogenic pain is a concern for adults, but rarely occurs in children.
Answer 3. Flexion contracture is not a common complication following amputation in pediatric patients.
Answer 4. Adduction contracture is not a common complication following amputation in this patient population.
Answer 5. The proximal tibial physis, important for longitudinal growth of the limb, would be sacrificed with a knee disarticulation, meaning the residual limb will be shorter than if the patient had a transtibial amputation.
A 52-year-old woman reports mild pain localized to the left sternoclavicular joint. History is notable for chronic renal failure requiring dialysis for the last 5 years. A clinical photograph, chest radiograph, and bone scan are shown in Figures 58a through 58c. What is the most likely diagnosis?
1) Pseudogout
2) Spontaneous subluxation
3) Postmenopausal arthritis
4) Chronic osteomyelitis
5) Friedreich’s disease
Spontaneous swelling with the appearance of joint subluxation may be associated with an acute, subacute, or chronic bacterial infection of the sternoclavicular joint. Common causes of infection include bacteremia, rheumatoid arthritis, alcoholism, intravenous drug use, and chronic debilitating diseases. Subclavian vein catheterization and renal dialysis can predispose patients to sepsis and osteomyelitis of the sternoclavicular joint.
A 19-year-old man was struck by a car and is seen in the emergency department with a grade IIIC open distal tibia and fibula fracture. Examination reveals that the toes are cool and dusky with a sluggish capillary refill. Angiography reveals a lesion in the posterior tibial artery amenable to repair. There is no sensation on the plantar aspect of the foot, and he is unable to flex his toes. A clinical photograph and radiograph are shown in Figures 2a and 2b. What is the next most appropriate step in management?
1) Irrigation and debridement with immediate intramedullary fixation, vascular repair, and primary closure
2) Irrigation and debridement with external fixation, vascular repair, and delayed closure
3) Irrigation and debridement with external fixation, vascular repair, exploration of the tibial nerve, and delayed closure
4) Guillotine amputation at the fracture site with delayed closure
5) Immediate below-knee amputation
In the past, loss of plantar sensation in this grade IIIC tibial fracture would have been an indication for below-knee amputation regardless of the potential for vascular repair. However the 2002 LEAP study divided 55 patients with loss of plantar sensation into two groups, the insensate amputation group and the insensate limb salvage group, with 55% of patients in the insensate salvage group regaining normal sensation 2 years after injury. Furthermore, those in
the salvage group who remained insensate after 2 years had equivalent outcomes to those in the amputation group. Because of these findings, limb salvage with vascular repair and external stabilization with delayed closure is deemed appropriate treatment. Immediate intramedullary fixation is not indicated. Because ischemia, contusion, and stretch can adversely affect the tibial nerve, the additional insult of exploration of the nerve is also not advisable given the soft-tissue compromise.
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?
1) Anterior tibialis tendon transfer to the dorsolateral midfoot
2) Posterior tibialis tendon transfer to the dorsolateral midfoot
3) Peroneus longus tendon transfer to the dorsolateral midfoot
4) Peroneus brevis tendon transfer to the dorsolateral midfoot
5) Flexor hallucis longus tendon transfer to the peroneus brevis
Compartment syndrome of the anterior and deep posterior compartments results in anterior tibialis and posterior tibialis tendon weakness, respectively. Furthermore, the long flexors to the hallux and lesser toes will be weak as well. The intact peroneus longus overpowers the weak anterior tibialis tendon, resulting in plantar flexion of the first metatarsal, cavus, and hindfoot varus.
Therefore, transferring the peroneus longus to the dorsolateral midfoot reduces the first metatarsal plantar flexion torque, and possibly augments ankle dorsiflexion torque.
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the
ankle is obtained. This test is designed to evaluate the integrity of what structure?
1) Posterior talofibular ligament
2) Distal tibiofibular syndesmosis
3) Anterior talofibular ligament
4) Deltoid ligament
5) Calcaneofibular ligament
In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used.
A 29-year-old patient sustains a closed, displaced joint depression intra-articular calcaneus fracture. In discussing potential complications of surgical intervention through an extensile lateral approach, which of the following is considered the most common complication following surgery?
1) Nonunion
2) Deep infection
3) Delayed wound healing
4) Peroneal tendinitis
5) Posttraumatic arthritis
Delayed wound healing and wound dehiscence is the most common complication of surgical management of calcaneal fractures through an extensile lateral approach, occurring in up to 25% of patients. Most wounds ultimately heal with local treatment; the deep infection rate is approximately 1% to 4% in closed fractures. Posttraumatic arthritis may develop despite open reduction and internal fixation, but the percentages remain low. Peroneal tendinitis may occur from adhesions within the tendon sheath or from prominent hardware but is relatively uncommon. Nonunion of a calcaneal fracture is rare.
Twelve months after open reduction and internal fixation of a comminuted distal radius fracture as seen in Figure A and B, which of the following tendons is at greatest risk of rupture?
1) Abductor Pollicis Longus
2) Extensor Pollicis Brevis
3) Extensor Indicis Proprius
4) Flexor Pollicis Brevis
5) Flexor Pollicis Longus
Figure A shows a distal radius fracture treated with a volar locked plate. Historically, distal radius fractures treated with dorsal plates were notorious for extensor tendon irritation with some cited rates as high as 50%.
In the reference by Drobetz et al, they reviewed 50 fractures treated with a volar locked plate. They noted that in 6 (12%) of cases that there was rupture of the flexor pollicis longus (FPL) at a mean of 10 months post operatively.
The second reference by Douthit is a retrospective review of 46 fractures treated with a volar locked plate. Excellent initial and maintenance of reduction was noted in 85% of cases, but FPL rupture occurred in 2 patients. Prominent plates and sharp screws were cited as reasons for tendon rupture.
Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?
1) MRI of the ankle
2) CT of the ankle
3) Technetium bone scan
4) Radiographs of the tibia and fibula
5) Repeat radiographs of the ankle in 5 to 7 days
The radiographs show an isolated posterior malleolus fracture which, given the injury mechanism, is highly suspicious for a Maisonneuve injury. As with any suspected extremity injury, radiographs including the joints above and below the level of injury are acutely indicated. Although MRI may reveal a ligamentous injury to the ankle and CT may show asymmetry of the ankle mortise or syndesmosis, both studies are considerably more costly and are not indicated in the absence of a complete radiographic work-up. Technetium bone scan is nonspecific and would be of limited value in this instance, as would repeat radiographs of the ankle.
A 25-year-old woman with a healed proximal tibiofibular fracture treated with an intramedullary nail 2 years ago is currently wearing an ankle-foot orthosis (AFO) and reports a persistent foot drop. She is unhappy with the AFO and has not seen any functional improvement despite months of physical therapy. Serial electromyograms (EMG) show no recent change over the past year. Examination and EMG findings are consistent with a tibialis anterior 1/5, extensor hallucis longus 2/5, extensor digitorum longus 2/5, posterior tibial tendon (PTT) 5/5, peroneals 3/5, flexor hallucis longus 5/5, and gastrocsoleus 5/5. No discrete nerve lesion was identified. The patient has a flexible equinovarus contracture. What is the most appropriate management?
1) Continued AFO bracing and therapy
2) Ankle fusion
3) Exploration and release of the common peroneal nerve
4) Transfer of the PTT through the interosseous membrane with attachment to the tibialis anterior and peroneus tertius above the level of the ankle, debridement of the anterior compartment, and Achilles tendon lengthening
5) Transfer of the peroneus longus to the dorsum of the foot and Achilles tendon lengthening
This pattern of injury is consistent with an unrecognized compartment syndrome of the anterior and lateral compartments. Transfer of the PTT through a long incision in the interosseous membrane corrects the foot drop deformity, and allows adequate dorsiflexion provided that the tendon to be transferred has a strength of 5/5. Muscles/tendons typically lose one grade of strength after transfer. Transfer into the tendons at the level of the ankle prevents overtensioning or pullout of a PTT tendon that is not long enough.
Debridement of the scarred muscle in the anterior compartment decreases the risk of scarring down to the tendon transfer. Transfer of the peroneus longus is not preferred given its relative lack of strength and line of pull. Continued therapy and bracing are unlikely to lead to further improvement at 2 years after injury. An ankle fusion would correct the foot drop but would not address the tendon imbalances between the tibialis anterior and the peroneus longus, and the PTT and the peroneus brevis.
When using a two-incision approach for open reduction and internal fixation of a Hawkins III talar fracture-dislocation involving
the talar neck and body, what anatomic structure must be preserved to optimize outcome?
1) Deltoid branch of the artery of the tarsal canal
2) Dorsalis pedis artery
3) Tarsal sinus artery
4) Perforating peroneal artery
5) Navicular artery
A Hawkins III fracture-dislocation generally presents with posteromedial displacement with the deltoid ligament intact. Therefore, the only remaining blood supply is the deltoid branch of the artery of the tarsal canal originating from the posterior tibial artery. Often, the medial malleolus is fractured, assisting in reduction and visualization of fracture reduction. If the medial malleolus is intact, a medial malleolus osteotomy allows visualization of the reduction without compromising the last remaining blood supply to the talus.
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort.
Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?
1) Short leg cast for 6 weeks
2) Splinting with early range of motion at 3 weeks
3) Immediate open reduction and internal fixation through a medial approach
4) Delayed open reduction and internal fixation
5) Fusion
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended.
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management?
1) Triple antibiotic coverage
2) Transfer to the ICU and a consult with infectious disease
3) Urgent irrigation and debridement with gentle skin closure
4) Urgent hyperbaric oxygen treatments and immunoglobulin
5) Urgent aggressive debridement of skin, subcutaneous fat, and fascia
The patient has necrotizing fasciitis, a rare and sometimes fatal disease that has many different etiologies. Signs that this is not a normal infection are the worsening clinical symptoms despite IV antibiotics and the systemic symptoms. He needs urgent surgical care before he becomes completely septic and unstable. He needs very aggressive debridement of his tissues. Hyperbaric oxygen and immunoglobulins are only anecdotally helpful, and would only be used after surgery.
Figures 17a through 17c show the radiographs of a 38-year-old man following a motorcycle accident. The posterior portion of the talus extruded through a posterolateral wound. The extruded talar body is visible in the wound along with some road debris. Management should now consist of surgical irrigation, debridement, and
1) removal of the extruded talus and placement of an external fixator.
2) immediate tibiocalcaneal fusion.
3) reimplantation of the talus, external fixation, and/or open reduction and internal fixation of the talar neck fracture.
4) reimplantation followed by primary tibiotalar arthrodesis.
5) Syme amputation.
The extruded talus should be placed in sterile bacitracin solution, irrigated thoroughly, gently debrided, and immediately replanted in the OR. Open reduction and internal fixation of the talar fracture may be attempted immediately depending on the soft-tissue envelope, or delayed after soft-tissue
stabilization with an external fixator. A retrospective study of 19 patients with an extruded talus reported that 12 patients had no subsequent surgery after definitive fixation, 7 had subsequent procedures, and 2 patients developed infections that were treated successfully at an average of 42-month follow-up. Successful outcome in this series was attributed to multiple debridements, soft-tissue stabilization, and primary wound closure.
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?
1) CT scan
2) Repeat period of immobilization
3) Referral to pain management for sympathetic blocks
4) Continued observation and physical therapy
5) Acupuncture
Persistent pain at the fracture site in the absence of infection is most likely due to a nonunion, best detected by CT. Walsh and DiGiovanni reported on a series of closed rotational fibular fractures in which nonunions were detected by CT in the absence of standard ankle radiographic findings. Repeat immobilization would not be appropriate at this late date. Pain management/sympathetic blocks would be considered if the patient displayed pain with light touch and disproportionate pain consistent with a complex mediated pain syndrome.
Acupuncture would be expected to be of limited benefit.
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?
1) Talectomy
2) Revision open reduction and internal fixation (ORIF) with bone grafting
3) Ankle arthrodesis
4) Tibiotalocalcaneal arthrodesis
5) Triple arthrodesis
The radiographs reveal nonunion of a talar neck fracture. There is no radiographic evidence of osteonecrosis or significant degenerative arthritis. The results of talectomy are suboptimal. Arthrodesis would be indicated for degenerative arthritis. Revision ORIF is feasible and preserves motion. A vascularized graft should be considered whenever osteonecrosis is present, but the talar body appears viable in this case.
A 27-year-old man was struck by a taxi cab and sustained comminuted right distal third tibia and fibula fractures; treatment consisted of placement of an intramedullary nail in the tibia the following morning. At his 6-month follow-up, he has clawing of all five toes. Examination reveals flexion deformities of the distal and proximal interphalangeal joints that are flexible with plantar flexion and rigid with dorsiflexion. Calluses are present on the dorsum and tip of the toes. Single heel rise is normal. He has a mild equinus contracture (relative to the left leg) that is not relieved with knee flexion. What is the most appropriate treatment option?
1) Physical therapy and bracing
2) Reassurance that the deformity will resolve with time
3) Achilles tendon lengthening, and release or retromalleolar lengthening of the flexor digitorum longus (FDL) and flexor hallucis longus (FHL)
4) FDL and FHL tenotomies at the individual digits with transfer of the posterior tibial tendon to the dorsum of the foot
5) FDL and FHL tenotomies at the individual digits with midfoot capsular release and hallux interphalangeal fusion
This is an example of tethering of the flexor hallucis longus/flexor digitorum longus (FHL/FDL) to the fracture site. Additional time and/or physical therapy and bracing would not be expected to be of benefit. Release of the FHL and FDL from the fracture site or retromalleolar lengthening will address the posttraumatic claw toe deformity and Achilles tendon lengthening will address the mild equinus. Posterior tibial tendon transfer is not appropriate as the patient demonstrates a normal heel rise. Midfoot releases and hallux fusion are also not indicated.
A 24-year-old man reports the development of a foot drop following a knee dislocation 1 year ago. The common peroneal nerve was found to be in continuity at the time of surgical reconstruction of the posterolateral corner of the knee joint. He would like to eliminate the need for an ankle-foot orthosis. What is the best option to achieve elimination of the orthosis?
1) Repeat neurolysis of the common peroneal nerve at the knee level
2) Repeat neurolysis of the common peroneal nerve with cable grafting
3) Extensor hallucis longus transfer to the distal first metatarsal
4) Anterior transfer of the tibialis posterior tendon through the interosseous membrane
5) Ankle fusion
The ankle dorsiflexor muscles have been denervated for too long a period to expect reinnervation to be successful. Even if the extensor hallucis longus tendon was functional, it is unlikely to have sufficient strength to achieve dynamic ankle dorsiflexion. The tibialis posterior tendon transfer has been shown to predictably achieve these goals in a high percentage of patients.
Successful ankle fusion is likely to fail with time due to the development of forefoot equinus.
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
1) Quicker return to activities
2) Quicker return to work
3) Increased subtalar joint range of motion
4) Decreased risk of nonunion
5) Decreased risk of posttraumatic arthritis
The radiographs and CT scans show a displaced intra-articular calcaneal fracture, with loss of calcaneal height and length. Recent multicenter, randomized, prospective studies suggest that surgical treatment of displaced intra-articular calcaneal fractures is associated with an almost six-fold decrease
in the risk of posttraumatic subtalar arthritis (necessitating subtalar arthrodesis) compared to nonsurgical treatment. Despite ongoing controversy, surgical treatment has not been shown to be advantageous with respect to activity, time to return to work, or subtalar joint range of motion. A nonunion of a calcaneal fracture is exceedingly rare regardless of the treatment method.
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments.
Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
1) surface irrigation, sterile dressing, and a short leg cast.
2) surface irrigation, sterile dressing, a short leg cast, and oral antibiotics.
3) surface irrigation, sterile dressing, a short leg cast, and IV antibiotics.
4) surgical debridement, a short leg cast, and IV antibiotics.
5) surgical debridement, external or internal fixation, and IV antibiotics.
The patient sustained a type I unstable fracture that requires debridement of superficial fragments from the sole and surgical stabilization. Low-velocity wounds less than 8 hours old are considered type I open fractures. In contrast, gunshot wounds with associated fractures more than 8 hours old are considered type II open fractures using the Gustilo and Anderson classification. Gustilo type I stable fractures due to gunshot wounds and seen within 8 hours can be treated with tetanus toxoid (if no history of immunization or booster within 5 years), surface irrigation, and casting or a hard sole shoe. Antibiotics are not required unless gross contamination is present. However, if the extent of contamination is unclear, or if a joint is penetrated, then routine antibiotic prophylaxis is recommended. Indications for surgery include: articular involvement, unstable fractures, presentation 8 or more hours after injury, tendon involvement, and superficial fragments in the palm or sole. Type I unstable fractures may be stabilized with internal or external fixation. Type II unstable fractures should be treated with external fixation and repeat debridements until clean.
A 32-year-old laborer reports left ankle pain and deformity. History reveals that he sustained a left ankle fracture 2 years ago and was treated with closed reduction and casting. Radiographs are shown in Figures 25a through 25c. What is the most appropriate management?
1) Bracing and physical therapy
2) Intra-articular injection of steroids into the ankle joint, bracing, and physical therapy
3) Intra-articular injection of hyaluronic acid product into the ankle joint, bracing, and physical therapy
4) Ankle fusion
5) Corrective osteotomy of the fibula and medial malleolus with reconstruction of the syndesmosis if unstable
Corrective osteotomy of fibular malunions, with appropriate lengthening, even in the presence of early arthritis, has been shown to decrease ankle pain and increase stability. Reduction and bone grafting of the medial malleolar nonunion is also needed. There is no evidence supporting the use of intraarticular steroids or hyaluronic acid in the ankle joint. Lateral talar displacement of even 1 mm has been reproducibly shown to decrease tibiotalar contact by 40% to 42%, causing a predisposition to arthritis.
Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The swelling has subsided by 3 weeks and the medial wound is clean. What do you tell the patient
about the likelihood of infection if a formal open reduction and internal fixation via a lateral approach is performed?
1) There is no significant difference between the infection rate for this fracture and a similar closed fracture.
2) Due to the risk of infection, open reduction and internal fixation is not recommended for this fracture.
3) The infection rate is three to five times more likely with this fracture.
4) Due to the risk of infection from a lateral approach, treatment is confined to limited internal fixation or an external fixator.
5) The patient will need to undergo 3 weeks of IV antibiotics at home.
Multiple authors have shown similar infection rates for grade 1 and 2 open medial fractures and closed fractures that have been treated with an extensile lateral approach and open reduction and internal fixation. Patients only need IV antibiotics for 2 to 3 days after surgery. Formal open reduction and internal fixation is not recommended for grade 3 medial wounds and most lateral wounds.
A 24-year-old woman was struck by a mini van in a parking lot and sustained a closed segmental tibia fracture that was treated with an intramedullary nail the following morning. Follow-up examinations reveal a slowly progressive clawing of all five toes, a progressive equinocavovarus contracture, and the patient is unable to perform a single heel rise on the affected limb. At 1 year after surgery, the patient now has a 10-degree equinus contracture that is not relieved with knee flexion. Treatment should now consist of
1) physical therapy and bracing.
2) reassurance that these problems will resolve with time.
3) posterior capsule release, Achilles tendon lengthening, and excision of the scarred muscle and tendon in the leg and foot.
4) Achilles tendon lengthening, and flexor digitorum longus and flexor hallucis longus tenotomies at the individual digits with transfer of the posterior tibial tendon to the dorsum of the foot.
5) flexor digitorum longus and flexor hallucis longus tenotomies at the individual digits with midfoot capsular release and hallux interphalangeal fusion.
This is an example of a missed deep posterior compartment syndrome that typically presents 6 months after the injury with progressive clawing due to necrosis, scarring, and contracture of the posterior tibial tendon, flexor digitorum longus, and flexor hallucis longus. Treatment consists of debridement of necrotic muscle and scar tissue with corresponding tendon excision. After debridement and posterior capsule release, if the equinus is relieved with knee flexion, a gastrocnemius slide may be performed.
Otherwise, the lengthening should be at the level of the Achilles tendon. Bracing will not address the claw toes.
Optimal management of the injury shown in Figure 31 should include which of the following?
1) Cast immobilization in equinus
2) Open reduction and internal fixation once the acute soft-tissue swelling has resolved
3) Urgent reduction and fixation
4) Arthroscopic-assisted percutaneous fixation
5) Open reduction and internal fixation with primary subtalar arthrodesis
The radiograph shows a displaced calcaneal beak fracture, a tongue-type fracture variant. The fracture fragment typically includes the insertion point of the Achilles tendon, which places marked tension on the thin overlying soft-tissue envelope and can lead to full-thickness necrosis if not acutely addressed. Cast immobilization does not adequately address the increased soft-tissue tension, as the fragment will be difficult to control. Arthroscopic-assisted techniques or primary arthrodesis are not indicated because calcaneal beak fractures are typically extra-articular.
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?
1) Surgical stabilization within 6 to 8 hours of injury
2) Extent of initial fracture displacement
3) Nicotine use
4) Posterior-to-anterior screw fixation
5) Anatomic fracture reduction
The incidence of osteonecrosis following displaced talar neck fractures is most related to the extent of initial fracture displacement. With increasing fracture displacement, the tenuous vascular supply to the talar body is more at risk for damage, thereby increasing the risk of osteonecrosis. Although displaced talar neck fractures have historically been considered a surgical emergency, recent studies have shown that the timing of surgical intervention bears no impact on the development of osteonecrosis. While nicotine use has an influence on fracture healing, it has never been shown to be a factor in osteonecrosis, nor has posterior-to-anterior screw fixation or the quality of fracture reduction.
A 32-year-old woman sustained a closed calcaneus fracture 2 years ago and was treated nonsurgically. She now reports a 6-month history of progressively worsening pain over the anterior ankle and lateral hindfoot. Climbing stairs and ascending slopes is particularly difficult for her. Bracing and intra-articular corticosteroid injections have not provided sufficient relief. Figure 36 shows a weight-bearing lateral radiograph. What is the most appropriate surgical option?
1) Subtalar arthrodesis in situ with plantar flexion osteotomy of the talar neck
2) Distraction subtalar arthrodesis with a corticocancellous bone block autograft
3) Subtalar arthrodesis in situ
4) Triple arthrodesis
5) Subtalar arthrodesis in situ with anterior ankle exostectomy
Intra-articular fractures of the calcaneus often include depression of the posterior facet of the subtalar joint. This can lead to dorsiflexion of the talus because of diminished height posteriorly. In a weight-bearing position, the dorsal surface of the talar neck can impinge against the distal tibia, causing anterior ankle pain. In addition, posttraumatic arthritis of the subtalar joint typically occurs after a calcaneus fracture. The patient’s symptoms are consistent with both anterior ankle impingement and subtalar degenerative arthritis. The Bohler angle, approximately 15 degrees, confirms depression of the posterior facet. Distraction subtalar arthrodesis with a corticocancellous bone block autograft will improve talar declination, decrease anterior impingement, and address the subtalar degenerative arthritis simultaneously.
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?
1) Reduces shrinkage of the residual limb
2) Creates a more stable platform for load transfer
3) Reduces wound healing complications by avoiding the soft-tissue dissection necessary to transect the fibula at a level proximal to the tibia
4) Connecting bone strut provides an attachment point for more effective
myodesis
5) Allows a more proximal resection level to decrease tension on the wound
The Ertl modification of a below-knee amputation has been proposed to create a more stable “platform” to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area.
Early studies have suggested that this modification may enhance the patient’s perceived functional outcome.
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
1) Irrigation and debridement of the cystic lesion and 6 weeks of IV antibiotics
2) Curettage, debridement of nonviable bone, and placement of absorbable
antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics
3) Complete resection of the infected portion of bone, placement of an external fixator to stabilize the tibia, and 6 weeks of IV antibiotics
4) Amputation
5) Local debridement of bone and the overlying skin and soft tissues, 6 weeks of IV antibiotics, and free-flap wound coverage
The patient has chronic tibial osteomyelitis that is due to low virulent bacteria. The history and studies do not suggest the need for an amputation or a free-flap procedure. This is a localized tibial infection that is in a healed bone; there is no need to resect the entire area of the tibia bone around the infection. The most appropriate treatment is curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics. Studies have shown that in cases of localized osteomyelitis that are of low virulence, as little as 1 week of IV antibiotics followed by 6 weeks of oral antibiotics is successful.
A 59-year-old woman underwent open reduction and internal fixation (ORIF) of her ankle 6 months ago, with subsequent hardware removal 3 months later. She now reports persistent, diffuse ankle pain, swelling, and limited range of motion. Figure 48 shows an oblique radiograph of the ankle. What is the next most appropriate step in management?
1) Physical therapy
2) Hardware removal
3) Repeat placement of a syndesmotic screw
4) Deltoid ligament reconstruction
5) Revision ORIF with exploration of the syndesmosis and medial ankle
The radiographs demonstrate persistent widening of the medial clear space with an ossicle. This represents soft-tissue interposition-scar tissue, the deltoid ligament, or the posterior tibialis tendon. Physical therapy will not improve the symptomatic malalignment. Hardware removal would be indicated for pain localized to the lateral fibula. Repeat syndesmotic screw fixation alone will not reduce the malalignment. Deltoid ligament repair may be necessary but will need to be combined with debridement of the medial ankle and syndesmosis, as well as repeat placement of one or more syndesmotic screws to maintain the reduction.
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight.
Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
1) Cephalosporin
2) Cephalosporin and aminoglycoside
3) Cephalosporin and penicillin
4) Cephalosporin and vancomyacin
5) Cephalosporin, aminoglycoside, and penicillin
A farm injury is automatically considered a grade III (Gustillo classification) injury regardless of size, energy, or additional soft-tissue injury due to the likelihood of substantial contamination. Antibiotic recommendations for grade III injuries include a first- or second-generation cephalosporin with an aminoglycoside or fluoroquinolone within 3 hours of injury, with penicillin added for farm injuries.
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
1) Methotrexate
2) Gold
3) Hydroxychloroquine
4) TNF-a inhibitors
5) Smoking
Clinical studies have shown that smoking cessation for 4 weeks reduces the risk of infection to the level of nonsmokers. Adverse effects on wound healing caused by chemotherapy used to treat rheumatoid arthritis has not been borne out in the literature.
Your 25-year-old patient complains of anterior knee pain after retrograde femoral nailing for a diaphyseal fracture and asks you why you didn’t perform antegrade nailing as he has seen on the internet.
You tell him that retrograde nailing is your preferred technique over antergrade nailing for diaphyseal femoral fractures because it has been shown to have which of the following?
1) Increased rate of union
2) Decreased rate of infection
3) Shorter operative time
4) Lower rates of hip pain
5) Lower rates of knee pain
Patients with retrograde femoral nails commonly have knee pain, while antegrade nails commonly have hip pain, abductor weakness and heterotopic ossification of the abductors.
Ostrum’s randomized prospective study of 100 patients with reamed femoral nails found 22% of antegrade nail patients had proximal hip pain, weak hip abductors or trendelenburg gait. No significant difference was found in set-up time, operative time, knee motion or pain, or infection rates.
Ricci performed a retrospective study of 293 fractures and found that the antegrade femoral nail group had more hip pain (10% vs 4%) and the retrograde nail group had more knee pain (36% vs 9%). There was no difference in healing, malunion, non-union or other complications.
Tornetta performed a randomized controlled comparison of 69 femur fractures and found more problems of length and rotation using a retrograde nailing.
There was no difference in time to union, operating time, blood loss, complications, size of nail or reamer, or transfusion requirements.
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
1) Zone 1 (the ala)
2) Zone 2 (the foramina)
3) Zone 3 (the central canal)
4) Zones 1 and 2
5) The sacral laminae
Denis divided the sacrum into three zones: zone 1 represents the lateral ala, zone 2 represents the foramina, and zone 3 represents the central canal. A fracture is classified according to its most medial extension. Those in zone 3
are typically bursting-type fractures or fracture-dislocations and are most prone to neurologic sequelae.
A 31-year-old male sustains the injury shown in Figure A. As compared to treatment with a simple sling, what is the primary advantage of treatment with a figure-of-eight brace?
1) Decreased sleep disturbance
2) Decreased personal care and hygiene impairment
3) Decreased rates of malunion
4) Improved long-term clinical outcomes
5) No advantage, equivalent result between a simple sling and figure-of-eight brace
Figure of eight braces have been shown to have no differences as compared to simple slings in regard to healing times, healing rates, and alignment at final follow-up.
The referenced study by Andersen et al is a Level 1 randomized controlled study showing equivalent cosmetic and clinical outcomes with sling versus figure of eight bracing despite increased sleep disturbances and increased rate of personal care impairment in those treated with a figure of eight brace.
The second referenced study by Nordqvist et al is a Level 4 case series designed to analyze the long-term outcome of mid-clavicle fractures in adults and to evaluate the clinical importance of displacement and fracture
comminution. They found a 39/225 rate of moderate shoulder pain with figure of eight bracing. Overall they concluded that few patients with fractures of the mid-part of the clavicle require operative treatment.
A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?
1) Bone grafting and revision open reduction and internal fixation
2) Hemiarthroplasty
3) Dynamic hip screw without angular correction
4) Valgus intertrochanteric osteotomy
5) Core decompression
Femoral neck fracture nonunion is a challenging problem for orthopaedic surgeons. Vertical fractures are more prone to nonunion due to shear stress rather than compressive forces across the fracture site. Several authors have suggested these fractures are more common in young adults due to injury type and bone composition. It is widely regarded that an effort should be made to salvage the femoral head if vascularity remains. The most common method to treat this complication is valgus intertrochanteric osteotomy of the femur. This functionally makes a vertical fracture more horizontal, converting shear into
compressive forces. It also helps correct the varus position of the fracture nonunion.
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?
1) Anterior column
2) Anterior wall
3) Posterior column
4) Both column
5) Transverse
The fracture pattern shown in the radiographs is a fracture of the posterior column. The only line interrupted on the AP pelvis is the ilioischial line. The obturator oblique view shows that the iliopectineal line is intact as is the outline of the posterior wall. The iliac oblique view shows an interruption of the ilioischial line and an intact anterior wall. Therefore, this fracture is a fracture of the posterior column.
Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?
1) Open reduction and internal fixation of the radial head and immobilization
2) Medial collateral ligament repair
3) Radial head replacement, ulnar nerve transposition, and external fixation
4) Coronoid repair, radial head replacement, and lateral ligamentous repair
5) Nonsurgical management in a hinged elbow brace
This elbow fracture-dislocation involves a radial head fracture, coronoid fracture, and ulnohumeral dislocation (terrible triad). Several algorithms exist for treatment; surgical treatment is indicated. The treatment should address the radial head. Studies have shown replacement to be superior to repair in comminuted fractures. The coronoid may be addressed in unstable cases at the time of radial head excision and replacement. Lateral ligamentous repair is carried out during closure of the lateral elbow capsule. Medial ligamentous repair also may be undertaken but usually in concert with bony repair. Hinged
external fixation remains an option when instability exists following bony and soft-tissue repair. Acute ulnar nerve transposition is rarely indicated.
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
1) Irrigation and debridement, external fixation of the ankle and foot, traction and pinning of the femur, open reduction and internal fixation of the forearm
2) Irrigation and debridement, external fixation of the ankle, foot, and femur, splinting of the forearm
3) Irrigation and debridement and open reduction and internal fixation of the ankle and foot, intramedullary nailing of the femur, open reduction and internal fixation of the forearm
4) Irrigation and debridement and open reduction and internal fixation of the ankle and foot, intramedullary nailing of the femur, splinting of the forearm
5) Irrigation and debridement, external fixation of the foot and ankle, intramedullary nailing of the femur, open reduction and internal fixation of the forearm
The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable.
Which of the following is most commonly associated with an open clavicular fracture?
1) Scapulothoracic dissociation
2) Closed head injury
3) Calcaneus fracture
4) Pelvic ring injury
5) Open tibial fracture
Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.
A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of
1) closed reduction and casting.
2) external fixation and percutaneous pinning of the distal radius.
3) open reduction and internal fixation of the distal radius.
4) open reduction and internal fixation of the distal radius and open repair of the ulnar styloid.
5) nonbridging external fixation of the distal radius.
The patient has a high-energy injury with resultant comminution of the distal radius metaphysis. Cast immobilization is likely to lead to radial shortening and angulation due to the comminution. Similarly, while external fixation and pinning has been successful in the past, some loss of radial length and volar angulation is typically noted. Present plate fixation devices for the distal radius employing locking screw technology have a superior ability to resist radial shortening and dorsal angulation. Fixation of the ulnar styloid is warranted when there is distal radioulnar joint instability or significant displacement of the styloid. This is more likely to occur with a fracture at the base of the styloid. In this instance, the distal radioulnar joint does not appear to be disrupted.
Following fixation of a displaced intra-articular fracture of the distal humerus through a posterior approach, what is the expected outcome?
1) Development of arthritic changes at 1 year
2) Restoration of full elbow range of motion
3) Loss of approximately 25% of elbow flexion strength
4) Posterolateral rotatory instability
5) Olecranon nonunion
Following repair of a displaced intra-articular distal humerus fracture, the ability to regain full elbow range of motion is rare. Recent reports of olecranon osteotomy have yielded healing rates of between 95% to 100%. According to McKee and associates, patients can be expected to have residual loss of elbow flexion strength of 25%.
A 28-year-old cowgirl was injured while herding cattle 1 week ago. A radiograph and CT scans are shown in Figures 13a through 13c. What is the most appropriate management for this injury?
1) Nonsurgical management and gradual weight bearing as tolerated
2) Nonsurgical management and restricted weight bearing
3) Placement of a pelvic binder
4) Open reduction and internal fixation of the symphysis
5) Open reduction and internal fixation of the symphysis and iliosacral screws
The patient has an AP I pelvic ring disruption with minimal symphyseal widening. The best treatment is nonsurgical management and weight bearing as tolerated. This will help close the anterior pelvic ring during the healing process. Pelvic binders are excellent for acute treatment of widely displaced pelvic fractures but are not recommended for long-term use. Open reduction and internal fixation is not indicated for this injury and furthermore, the posterior ring is not injured.
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
1) AIDS
2) Polytrauma
3) Pelvic fracture
4) Pilon fracture
5) Acute myocardial infarction (AMI)
Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb “feels” different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?
1) Serial physical examinations
2) Angiography
3) Duplex ultrasound examination
4) Ankle-brachial index (ABI)
5) Measurement of compartment pressures
The patient initially has a distal third femoral fracture and a pulseless limb. The first step is to reduce the fracture and reassess the vascular status. Although the pulse returns, it feels different than the quality of the pulse in the contralateral uninjured extremity. There is a risk of a vascular injury with this fracture pattern due to tethering of the femoral vessels at the adductor hiatus; therefore, the vascular status needs further assessment since the pulses are not symmetrical. A physical examination is not very accurate in assessing whether a vascular injury is present; therefore, serial examinations are not appropriate. Angiography is very sensitive and specific but is time consuming and can cause complications secondary to the dye and the arterial puncture required to perform it. Duplex ultrasound is effective but is very operator-dependent and may not be available 24 hours a day. The ABI is easily performed and has been shown to be sensitive and specific. If the value is greater than 0.9, the negative predictive value is 99% and when the value is less than 0.9, it is 95% sensitive and 97% specific for a major arterial injury. It has been shown to be useful for blunt lower extremity injuries as well as knee dislocations.
What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?
1) Total elbow arthroplasty
2) Functional hinge bracing
3) Long arm casting
4) Crossed Kirschner wires
5) Dual column plates
This intra-articular distal humerus fracture with displacement at the joint surface is best treated with surgical fixation. The most biomechanically sound construct is two plates applied to either column 180 degrees from one another. Elbow arthroplasty is most appropriate for low demand elderly patients.
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury?
1) Inlet and outlet views of the pelvis to better delineate the injury
2) Angiography
3) Laparotomy
4) Open reduction and internal fixation of the pelvis
5) Placement of a pelvic binder around the patient
This hypotensive patient has an obvious open book injury of the pelvic ring on the AP pelvis radiograph and further radiographs are not needed prior to the
initiation of treatment. Although angiography may be indicated if he does not respond to stabilization of his pelvis and fluid/blood administration, temporary stabilization of the pelvis with a sheet or binder should be performed first because it is simple, quick, and has been shown to be effective. This patient does not need a laparotomy at this point since the FAST examination did not show any free intra-abdominal fluid and his chest radiograph was unremarkable, leaving the most likely source of bleeding the pelvic fracture.
Open reduction with internal fixation of a pelvic injury is not indicated in an acutely ill patient.
A 220-lb 20-year-old man was involved in a motor vehicle accident. His work-up reveals that he has multiple long bone fractures as well as a splenic injury that is currently being managed nonsurgically. His initial blood pressure in the trauma bay was 70/30 mm Hg. After receiving 4 liters of fluid and 3 units of packed red blood cells, his blood pressure is currently 110/70, his heart rate is 100, his urine output is 90 mL/h (normal 0.5 to 1 mL/kg/h), and his core temperature is 97.9 degrees F (36.5 degrees C). At this point, the patient’s resuscitation can be described as which of the following?
1) Complete based on the normalization of his blood pressure, urine output, and heart rate
2) Cannot be determined based on the data presented
3) Incomplete based on his fluid requirements calculated using his initial blood pressure as a measure of blood volume loss
4) Incomplete since he will need surgery on the long bone fractures and should be “tanked up” prior to losing blood in the operating room
5) Incomplete based on his heart rate
Although the end points of resuscitation are still unclear, what is known is that normalization of the standard hemodynamic parameters (blood pressure, heart rate, and urine output) is not adequate. Up to 85% of patients with normal hemodynamic parameters can still have inadequate tissue oxygenation or uncompensated shock. The initial base deficit, lactate level, or gastric pHi can be used to stratify patients for resuscitation needs, risks of death, and multiple organ failure (level 1 evidence). The time it takes to normalize the base deficit, the lactate level, or gastric pHi, can predict survival (level 2 evidence). Patients who have been in uncompensated shock (abnormal vital signs) should have their resuscitation monitored using data other than vital signs.
A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
1) Continued nonsurgical management
2) Posterior open reduction and internal fixation with tension band plating
3) Posterior iliosacral screws
4) Anterior open reduction and internal fixation
5) Anterior open reduction and internal fixation and posterior fixation
Fortunately, surgical treatment of sub-acute pelvic ring injuries is relatively uncommon as acute management has become more common. Delayed reconstruction of pelvic ring malunion and impending malunion is rare.
Nonsurgical management may have a role as long as the hemipelvis does not flex, shorten, and/or externally rotate. The AP pelvic radiograph suggests that all three motions are happening in this patient. These are just a few of the indications to repair the pelvic ring and this is best done with anterior and posterior fixation. Anterior symphyseal plating will help correct most of the deformity. Posterior fixation can and should be added to lessen the forces on the anterior ring reconstruction when repair is performed in a sub-acute or delayed fashion. Posterior fixation can help obtain a more anatomic reduction and helps decrease the risk of anterior hardware failure.
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?
1) Immobilization of the wrist in ulnar deviation for 4 weeks before starting range-of-motion exercises
2) In situ Kirschner wire fixation of the carpal bones for 6 weeks
3) Extending the volar incision used for fracture fixation and repairing the injured structures in addition to percutaneous Kirschner wire fixation
4) Performing a separate dorsal incision and repairing the injured structures in addition to percutaneous Kirschner wire fixation
5) Arthroscopic repair of the injured structures and percutaneous Kirschner wire fixation
The intraoperative radiograph reveals a scapholunate ligament disruption. Repair of the stout dorsal scapholunate interosseous ligaments is required. Interestingly, the results of scapholunate ligament injuries associated with distal radius fractures appear to be superior to those of isolated ligament injuries.
A 36-year-old woman is placed in a short arm cast for a nondisplaced extra-articular distal radius fracture. Seven weeks later she notes the sudden inability to extend her thumb. What is the most likely cause of her condition?
1) Posterior interosseous nerve palsy
2) Cervical disk herniation
3) Entrapment of the flexor pollicis longus tendon
4) Rupture of the extensor pollicis longus tendon
5) Metacarpophalangeal joint dislocation
A recent review of 200 consecutive distal radius fractures noted that the overall incidence of extensor pollicis longus rupture was 3%. The causes are believed to be mechanical irritation, attrition, and vascular impairment. The fracture is usually nondisplaced and the patient notes weeks to months after injury the sudden, painless inability to extend the thumb. Treatment involves extensor indicis proprius tendon transfer or free palmaris longus tendon grafting.
In Gustilo type III open tibial diaphyseal fractures, which of the following factors is associated with an increased risk of a poor functional outcome?
1) Soft-tissue coverage within 3 days of injury
2) Bone grafting 3 months after injury
3) Wound debridement within 6 to 24 hours from injury
4) Definitive treatment with external fixation
5) Free tissue transfer for soft-tissue coverage
According to the published outcomes analyses from the Lower Extremity Assessment Project (LEAP) study group of patients prospectively followed for 2 to 7 years, definitive fixation with an intramedullary nail has shown improved outcomes when compared to definitive external fixation. The findings showed that the timing of wound debridement (within 6 hours from injury as compared to within 6 to 24 hours), the timing of soft-tissue coverage (3 days or less from injury as compared to more than 3 days), and the timing of bone grafting after injury (within or after 3 months) did not impact the infection or union rates and had no effect on functional outcome. The LEAP study has shown at 7-year follow-up that patients who are definitively treated with external fixation have a significantly longer time to union, poorer functional outcomes, longer time to achieve full weight bearing, and more time in the hospital.
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
1) closed reduction and splinting.
2) open reduction and internal fixation through a volar approach.
3) external fixation and Kirschner wire fixation.
4) intrafocal pinning and casting.
5) acceptance of alignment and bracing.
Definitive treatment decisions for displaced distal radius fractures in the elderly are based on a number of factors related to the fracture pattern and patient demographics. The first step in any treatment algorithm is a closed reduction and splinting with reassessment of alignment parameters. This is an extra-articular fracture with dorsal angulation. Low-demand elderly patients can be treated well with accepted minor malreduction.
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome?
1) His clinical outcome will correlate closely with his initial reduction.
2) His outcome will correlate with his radiographic score on the Ankle Osteoarthritis Score.
3) He will likely require a late ankle arthrodesis.
4) He will demonstrate marked limitations with regard to recreational activities.
5) He will perceive improvements for a period of over 2 years.
Marsh and associates retrospectively reviewed 56 tibial plafond fractures and found that the patients perceived improvement in their function and pain for an average of 2.4 years. They demonstrated some limitations in recreational activities but not marked limitations. Patients were unlikely to need a late arthrodesis (13%), and their outcomes did not correlate well with assessments of reduction or arthritis scores.
The injury shown in Figure 24 was most likely caused by what mechanism of injury?
1) Anterior posterior compression
2) Lateral compression
3) Vertical shear
4) Combined mechanism
5) Flexion-rotation
The CT cut shows a fracture through the posterior portion of the iliac wing or a crescent fracture. This occurs after a laterally directed force is applied to the anterior part of the involved iliac wing.
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?
1) Functional bracing
2) Hanging long arm cast immobilization
3) Intramedullary nailing
4) Open reduction and internal fixation, radial nerve exploration
5) External bone stimulator
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated.
Which of the following is most predictive of a medial side ankle injury in the presence of a fibula fracture above the level of the joint?
1) Severe medial ankle tenderness
2) Severe medial ankle ecchymosis
3) Stress radiographs showing the medial clear space measuring 6 mm and the superior joint space measuring 3 mm
4) Inability to ambulate
5) Medial ankle swelling
Isolated Lauge-Hansen supination-external rotation-type ankle fractures comprise 20% to 40% of ankle fractures and nonsurgical management is effective for managing SER-2 ankle fractures. Tornetta and associates recently showed that medial ankle tenderness, ecchymosis, and swelling are not reliable findings when trying to determine deltoid competence. Stress radiographs showing a medial clear space of greater than 4 mm or one that is also 1 mm greater than the superior joint space, or any lateral talar subluxation are indicative of deltoid incompetence and indicative of a SER-4 ankle fracture.
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure
34/. What is the next most appropriate step in the orthopaedic management of this patient?
1) Axillary view
2) CT of the shoulder
3) Closed reduction
4) Sling and close follow-up
5) Functional brace
The next step in the management of this injury is completion of the shoulder trauma series. An axillary radiograph, which can be quickly performed in the emergency department, must be obtained to accurately assess the humeral head relationship to the glenoid. If difficulty is encountered, a “Velpeau” axillary may be substituted. If that fails to elucidate the status of the glenohumeral joint, a CT scan should be obtained.
Which of the following findings best describes the acetabular fracture shown in Figure 38?
1) Posterior column with articular impaction and a free fragment
2) Anterior column with articular impaction
3) Posterior wall with an intra-articular fragment
4) Posterior wall with articular impaction and a free intra-articular fragment
5) Posterior wall with articular impaction
The CT scan shows a posterior wall fracture with impaction of the articular surface and a free fragment within the joint. Proper treatment of this injury requires not only reduction and fixation of the posterior wall fragment but also removal of the free fragment and elevation of the depressed articular segment.
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
1) normal sexual function and normal vaginal childbirth.
2) sexual dysfunction (dyspareunia) and normal vaginal childbirth.
3) normal sexual function and caesarean section childbirth.
4) sexual dysfunction (dyspareunia) and caesarean section childbirth.
5) normal sexual function and caesarean section childbirth until hardware removal.
Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is
almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not.
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?
1) Closed treatment and casting
2) Open reduction and internal fixation
3) Primary subtalar arthrodesis
4) Percutaneous fixation
5) External fixation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures.
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
1) Radial head resection, open reduction and internal fixation of the coronoid, and medial collateral ligament repair
2) Radial head resection and lateral collateral ligament repair
3) Radial head arthroplasty alone
4) Radial head arthroplasty and lateral collateral ligament repair
5) Radial head arthroplasty, open reduction and internal fixation of the coronoid, and lateral collateral ligament repair
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region.
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal
1) Reamed intramedullary nailing
2) Traction
3) External fixation
4) Open plating
5) Mast suit
The patient has several indications that he is not ready for definitive fixation of the femoral shaft fracture at this point. He is cold with a core temperature of 93 degrees F, and hypothermia of less than 95 degrees F (35 degrees C) has been shown to be associated with an increased mortality rate in trauma patients. The patient has also not been resuscitated based on his increasing lactate levels and although controversial, it has been shown that temporary external fixation leads to a lower incidence of multiple organ failure and acute respiratory distress syndrome.
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?
1) MRI scan
2) Physical examination
3) Workers’ compensation status
4) Surgeon availability
5) Patient age
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
1) Consult the ethics committee before giving blood.
2) Use cell saver blood.
3) Ask the patient’s family for consent to give blood.
4) Use plasma expanders.
5) Give the patient blood.
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah’s Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah’s Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open wound is not recommended nor would there likely be enough from an open pelvic fracture to salvage. The patient’s family may be expressing their own beliefs rather than the patient’s beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability.
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and
1) talectomy.
2) reimplantation of the talus.
3) reimplantation of the talus with acute triple arthrodesis.
4) Syme amputation.
5) transtibial amputation.
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures.
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
1) Spiral
2) Oblique
3) Transverse
4) Segmental
5) Comminuted
A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism.
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?
1) Kocher-Langenbeck
2) Iliofemoral
3) Ilioinguinal
4) Extended iliofemoral
5) Triradiate approach
The fracture is an associated both column fracture. The best approach for this fracture is the ilioinguinal. The Kocher-Langenbeck is best for posterior injuries to the acetabulum and some transverse fractures. The iliofemoral alone is limited to high anterior column injuries. The extended iliofemoral and triradiate
approaches although useful for this fracture, have a higher rate of complications.
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
1) plating of the radial shaft fracture then open repair of the triangular fibrocartilage complex.
2) open reduction and internal fixation of the radius and ulna.
3) plating of the radius then closed reduction and evaluation of the distal radioulnar joint (DRUJ).
4) closed reduction of the radius and DRUJ.
5) plating of the radius then pinning of the DRUJ in pronation.
This Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction of the radial shaft and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. If not, either open or closed reduction with pinning is undertaken. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?
1) Chronic osteomyelitis
2) Planovalgus hindfoot
3) Plantar nerve entrapment
4) Wound dehiscence
5) Painful hardware
The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence.
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
1) A primed immune system with an increased risk of a systemic inflammatory response
2) Nothing since they are no longer in uncompensated shock and their vital signs have normalized
3) Higher nonunion rates after fracture fixation
4) Higher infection rates after definitive fracture fixation
5) Higher complication rates after temporizing external fixation of long bone fractures
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a “primed” immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered.
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is
intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?
1) Emergent four compartment fasciotomies
2) Emergent four compartment fasciotomies and open reduction and internal fixation of the fracture
3) Elevation of the limb overnight and four compartment fasciotomies in the morning
4) Elevation of the limb overnight and a recheck of compartment pressures in the morning
5) Emergent MRI of the knee and leg
The patient has a compartment syndrome based on the firm compartments of the leg and the elevated compartment pressures measured at the diastolic pressure reading. Muscle ischemia occurs quickly when compartment pressures are elevated, and within 6 hours irreversible damage can occur. Emergent fasciotomies permit decompression of all four compartments and reestablishment of vascular supply to the muscles. Stabilization of the fracture prevents further soft-tissue injury.
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
1) The mean arterial blood pressure is above 90 mm Hg.
2) The pulse pressure has normalized.
3) Urine output is greater than 0.5 to 1 mL/kg/h.
4) Oxygen delivery has been maximized.
5) Aerobic metabolism has been restored in all tissue beds.
Shock can be defined as inadequate tissue perfusion. Resuscitation or the resolution of shock is defined as when oxygen debt has been repaid, tissue acidosis is eliminated, and aerobic metabolism has been restored in all tissue beds. The end points for resuscitation are not clearly defined, but occult shock can still be present in the setting of normal vital signs and normal urine output due to selective perfusion of organ systems.
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
1) Infection
2) Malunion
3) Loss of forearm rotation
4) Refracture
5) Delayed union/nonunion
Healing of forearm fractures in skeletally immature patients is the usual outcome. The use of intramedullary fixation has been reported to result in a lower frequency of refractures when compared to plate osteosynthesis due to the absence of diaphyseal holes after plate removal, which are considered stress risers. Regardless of implant technique, malunion and infection are infrequent. Loss of forearm pronation and supination is a common occurrence in surgically treated fractures due to the higher degree of soft-tissue injury, and periosteal stripping leads to fracture site instability and fracture comminution.
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
1) Anterior superior iliac spine
2) Sciatic buttress
3) A column of bone running from the anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS)
4) The most superior portion of the roof of the acetabulum
5) Iliopectineal line
The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures.
A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure
62/. Based on these findings, what is the most appropriate treatment?
1) Electrical stimulation
2) Bone grafting
3) No weight bearing
4) Bone grafting and compression plating
5) Free vascularized bone transport
Nonunions after intramedullary nails are often treated with exchange reamed nailing. In a recent study, this resulted in a union rate of 53%. After failed exchange nailing, bone grafting and compression plating should be used. The other options resulted in less satisfactory results as compared to bone grafting and compression plating.
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?
1) Peroneal tendon tear
2) Lateral process talus fracture
3) Talar neck fracture
4) Lisfranc injury
5) Deltoid ligament tear
This cuboid compression fracture (“nutcracker” injury) is associated with subtle injury to the Lisfranc complex. This diagnosis must be made to ensure proper treatment.
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
1) Posterior column/posterior wall acetabular
2) Associated both column acetabular
3) Transverse plus posterior wall acetabular
4) Anterior column posterior hemitransverse acetabular
5) Anterior column acetabular
The radiographs and CT scans reveal an anterior column acetabular fracture. The fracture has quadrilateral plate extension but does not exit out the posterior column. The CT scans confirm an intact posterior column and no wall fracture. A transverse fracture is best seen on the CT scan and runs in the sagittal plane, not the coronal plane.
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture.
Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
1) Long arm cast immobilization
2) Total elbow arthroplasty
3) Open reduction and internal fixation
4) Osteoarticular allograft
5) Resection arthroplasty
Several studies have documented the satisfactory outcomes of total elbow arthroplasty when osteosynthesis is not feasible for fixation of a distal humerus fracture, particularly in the physiologically older patient with low functional demands. Total elbow arthroplasty should be considered when a comminuted intra-articular distal humerus fracture occurs in a woman older than age 65 years, particularly with such associated comorbidities as systemic steroid use, osteoporosis, or rheumatoid arthritis.
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
1) Cast removal and measurement of carpal canal pressure
2) Immediate carpal tunnel release and pinning of the fracture
3) Continued observation
4) Surgical reduction and pinning of the fracture
5) Electromyography/nerve conduction velocity studies
The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural
compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression.
A 25-year-old male polytrauma patient undergoes initial temporary external fixation for a femoral shaft fracture. He is converted to a femoral nail at 7 days. This management can be expected to result in
1) higher infection rates.
2) higher nonunion rates.
3) equal union and infection rates.
4) higher rate of ARDS.
5) higher mortality rate.
Recently Harwood and associates investigated the principles of damage control orthopaedics (DCO) as they apply to patients with femoral shaft fractures.
When they compared those who underwent initial external fixation of femoral shaft fractures with conversion to an intramedullary nail to those who underwent intramedullary nailing as their initial treatment, they found the following: overall infection rates were comparable in patients receiving DCO versus primary intramedullary fixation; open fracture was an independent risk factor for infection regardless of the treatment method; contamination rates in external fixator pin sites rose considerably when left in place more than 2 weeks and logistic regression analysis suggests that infection rates may increase when conversion to an intramedullary nail occurs after 2 weeks following external fixation; and there was no significant difference in time to union among treatment groups.
Which of the following is the most stable construct for fixation of an unstable transforaminal sacral fractures?
1) External fixation
2) Iliosacral osteosynthesis
3) Combined iliosacral and lumbopelvic fixation (triangular osteosynthesis)
4) Anterior pelvic ring plating with bilateral sacroilliac percutaenous screw fixation
5) Transiliac bars with anterior pelvic ring plating
Combined iliosacral and lumbopelvic fixation (triangular osteosynthesis) for sacral fractures has the greatest stiffness when used for an unstable sacral fracture.
The referenced article by Schildhauer et al is a cadaveric study that examined the biomechanical properties of different fixation constructs under cyclic loading and demonstrates that triangular osteosynthesis for unstable transforaminal sacral fractures provides significantly greater stability than iliosacral screw fixation under in-vitro cyclical loading.
Illustration below shows the radiographic appearance of lumbopelvic fixation. The addition of iliosacral fixation would complete triangular osteosynthesis.
The Cotton test evaluates which of the following structures?
1) Calcaneofibular ligament
2) Lateral ulnar collateral ligament of the elbow
3) Ligamentum flavum
4) Anterior talofibular ligament
5) Ankle syndesmosis
The inferior tibiofibular syndesmosis is a fibrous articulation consisting of four ligaments; the elasticity of these ligaments permits axial, vertical, anterior, posterior, and mediolateral motion at the ankle syndesmosis during weight bearing.
Of note, the Cotton test was originally described around 1910 by Frederic J. Cotton as the "talar glide test" evaluating the medial/lateral translation of the talus in the mortise. A positive result indicates disruption of the ankle syndesmosis in the face of an ankle injury.
Nielson et al reported that the level of the fibular fracture does not correlate reliably with the integrity or extent of the interosseous membrane (IOM) tears identified on MRI in operative ankle fractures. Therefore, one cannot consistently estimate the integrity of the IOM and subsequent need for transsyndesmotic fixation based solely on the level of the fibular fracture. This supports the need for intraoperative stress testing (ie, external rotation stress or Cotton test) of the ankle syndesmosis in all operative ankle fractures.
The study by Leeds et al noted a correlation between syndesmosis reduction (initial and final) and outcomes (radiographic and clinical).
The attached video shows the Cotton test during an ankle fixation procedure.
A comminuted femoral shaft fracture is treated with an intramedullary nail locked with a single distal screw. What is the most likely mode of failure of the screw?
1) Screw pulls out of the cortical shaft
2) Screw head breaks off due to bending stresses
3) Shaft of the screw fractures in the region that is inside the nail
4) Screw threads are damaged by fretting against the edges of the holes in the nail
5) Screw bends excessively
The screw is being loaded and pushed distally at the two points where it contacts the walls of the nail, and it is being pushed proximally at the two points where it contacts the cortex, ie, near the head and tip of the screw. This places the screw in four-point bending, producing tensile stresses on the
inferior side of the screw and compressive stresses on the superior side. The tensile stresses, combined with stress risers at the screw threads, eventually could lead to fatigue fracture of the screw. Because the cortices in the metaphysis are far apart, the bending moment is large and, therefore, stresses near the midshaft of the screw produced by bending are much larger than shear stresses in this case. Pullout of the screw is unlikely because the loads are not directed along the axis of the screw. There are no bending stresses at the ends of the screw. A bent screw may be difficult to remove, but this would not likely cause failure of the fixation.
A 30-year-old female presents with the injury shown in Figure A after falling on her outstretched arm. During operative treatment of the fracture, anatomic reduction of the radius is achieved. However, the surgeon is unable to reduce the distal radioulnar joint. What structure is most likely impeding the reduction?
1) Median nerve
2) Flexor carpi radialis
3) Pronator quadratus
4) Extensor carpi ulnaris
5) Flexor carpi ulnaris
Figure A shows a Galeazzi fracture (distal 1/3 radial shaft fracture with associated distal radioulnar joint dislocation). In this injury, an inability to reduce the distal radioulnar joint in a closed fashion is most commonly secondary to interposition of the extensor carpi ulnaris tendon. Early recognition of the dislocation of the ulna and ECU into the DRUJ and their significance may avoid poor results.
The referenced study by Biyani et al reports a case in which both the extensor carpi ulnaris and extensor digiti minimi tendons were displaced on either side of the ulnar head.
The referenced study by Budgen et al presents a case of a Galeazzi fracture dislocation with an irreducible distal radioulnar joint.
The referenced study by Paley et al reports two cases of distal radioulnar joint (DRUJ) disruption and diastasis secondary to distal radial fractures that were associated with displacement of the ulnar styloid and extensor carpi ulnaris (ECU) into the DRUJ. Both cases had a palpable empty ECU tendon sulcus.
What is the antibiotic of choice for gonococcal septic arthritis of the knee?
1) Erythromycin
2) Penicillin
3) Tetracycline
4) Ceftriaxone
5) Vancomycin
Gonococcal septic arthritis, caused by the gram-negative diplococcus Neisseria gonorrhoeae, typically affects two age groups: newborns and adolescents. The level of penicillin and tetracycline resistance in Neisseria gonorrhoeae is so high that it is completely ineffective in most parts of the world. A third-generation cephalosporin such as ceftriaxone is recommended in most areas. Fluoroquinolones may be an alternative treatment option if antimicrobial susceptibility can be documented by culture. In areas where co-infection with chlamydia is common, doxycycline may be used with ceftriaxone.
An above-the-knee amputation is performed 12 cm above the joint line. What is the best management of the adductor muscle group?
1) Resection of the adductors to prevent adductor contracture
2) Shortening and reattachment to the mid-femur to improve biomechanics
3) Myodesis to the distal end of the bone
4) Transfer to the quadriceps to improve hip flexion
5) Attachment to the hamstrings
The best socket fit requires resection of the wide flair of the condyles and amputation approximately 12 cm above the joint line. The adductor magnus is a very important muscle that participates in achieving a more efficient gait.
Myodesis of the bone through drill holes near the cut end of the bone has been shown to improve biomechanics.
In determining the FRAX score (fracture risk assessment tool), the World Health Organization determined that which of the following risk factors is not contributory to the clinical risk of fracture in its population cohorts?
1) BMI (body mass index)
2) Spine T-score from DEXA scan (dual-energy absorptiometry)
3) Current smoking activity
4) Parental history of hip fracture
5) Prior history of fracture before age 50
The FRAX score calculates the clinical risk of fracture using bone mineral density of the femoral neck, BMI, current smoking activity, history of parental hip fracture, and prior personal history of fracture before age 50. The World Health Organization has developed this new fracture risk assessment tool to identify individuals at high risk of osteoporotic fracture. The current standard, which bases treatment decisions largely on bone mineral density measurement, has proven to be specific, but not sensitive, for the identification of patients at high risk of fracture. Because nearly 50% of postmenopausal women in the community older than age 50 years who suffer an osteoporotic fracture do not have osteoporosis defined by a BMD test and because of the limited availability of BMD in many countries, clinical risk factors were added to BMD to identify patients at high risk for osteoporotic fractures. The site and
reference technology is DEXA at the femoral neck. T-scores are based on the National Health and Nutrition Examination Survey reference values for women aged 20 to 29 years. The same absolute values are used in men. Although the model is constructed for BMD at the femoral neck, the total hip site is thought to predict fracture equivalently in women.
Glenohumeral disarticulation often leads to which of the following changes?
1) Hiking of the shoulder girdle
2) Hypertrophy of the amputated shoulder girdle
3) Improvement in thoracic spinal deformity
4) Protraction of the shoulder
5) Winging of the scapula
Postural abnormalities are common after high upper extremity amputation. Normally the weight of the upper extremity and the shoulder girdle muscles keep the shoulder balanced. When the arm is amputated and the scapula remains, the shoulder girdle muscles are unopposed, resulting in upward movement often called "hiking" of the shoulder girdle. In a growing child, removal of the entire upper limb can result in scoliosis of the spine due to muscle imbalance. Abnormal shoulder elevation can often be minimized by corrective exercises and wearing a shoulder prosthesis.
A 10-day-old girl has decreased active motion of the left upper extremity. The mother reports a difficult vaginal delivery with presumed shoulder dystocia. Examination shows full passive range of motion of the shoulder, elbow, and wrist but only active flexion of the fingers and wrist. Factors predictive of a good outcome include which of the following?
1) Breech delivery
2) Absence of an ipsilateral clavicle fracture
3) Horner's sign and an APGAR score of 10 at 1 minute
4) Return of active biceps before 3 months and preservation of full passive shoulder range of motion
5) Absent Moro and Babinski reflexes
Return of active biceps before 3 months and preservation of full passive shoulder range of motion are predictors of a good outcome. Breech delivery is usually associated with preganglionic injury. Preganglionic injury can result in a Horner's sign, which includes ptosis, myosis, and anhydrosis. Preganglionic injuries are unlikely to recover. The Moro reflex is elicited by dropping a baby's head a short distance and observing active elbow extension and fanning of the fingers, followed by elbow flexion and crying. Absence of the Moro reflex suggests a poor prognosis.
An 18-month-old child was involved in a motor vehicle accident and sustained an isolated injury to the left upper extremity. A radiograph is shown in Figure 33. What is the most appropriate management for this injury?
1) Hanging arm cast
2) Closed reduction with flexible intramedullary nail fixation
3) Coaptation splinting and bandaging the arm to the thorax
4) Closed reduction and external fixation
5) Locking plate fixation
Humeral shaft fractures in infants and young children heal rapidly and have excellent remodeling potential. Appropriate treatment in this age group is immobilization with a coaptation splint and bandaging the arm to the thorax for comfort. Internal fixation is appropriate in multiple trauma, and external fixation may be useful when soft-tissue injury is extensive.
If a percutaneous iliosacral screw is placed too anteriorly, and the screw exits anterior to the sacral ala before re-entering the sacral body, what will be the most likely finding postoperatively?
1) Lack of ankle dorsiflexion
2) Lack of ankle plantarflexion
3) Lack of knee extension
4) Loss of bowel and/or bladder control
5) Lack of great toe extension
This question is a simple review of anatomy and nerve innervation. The L5 root is at risk with an "in-out-in" screw, as described in the question, as the nerve root is just anterior to the sacral ala as it enters the true pelvis. L5 is primarily evaluated by extensor hallucis longus function. L4 is tested with tibialis anterior function and S1 by gastroc-soleus function (ankle plantarflexion).
A 10-year-old boy is struck by a car and sustains open left tibia and fibula fractures with bone protruding through a 7-cm laceration, multiple deep and superficial abrasions over the anterior leg, and road gravel is present in the wounds. His foot is warm and well-perfused with normal sensation and he has no pain with passive range of motion of the toes. Optimal treatment should consist of
1) irrigation and debridement of the fractures and application of an external fixator.
2) irrigation and debridement of the fractures and a reamed intramedullary nail.
3) irrigation and debridement of the fracture and percutaneous Kirschner wire fixation.
4) submuscular plating.
5) reduction and a short leg cast.
The patient has a grade 2 open fracture and therefore needs wound debridement as a first step, followed by fracture stabilization preferably with an external fixator. A reamed intramedullary nail is not indicated in a 10-year-old child with open growth plates. Submuscular plating is not needed in an open fracture and there is no mention of fracture debridement. Percutaneous Kirschner wires will not provide adequate fracture stabilization, nor will a short leg cast. Flexible nailing should be considered as another form of fixation.
Figures 5a and 5b show the radiographs of a 21-year-old wrestler who reports that his leg was rolled over while wrestling. The patient has decreased sensation and function in the distribution of the peroneal nerve, and he has absent pulses. What is the most appropriate initial management at this time?
1) Acute reconstruction of all ligamentous structures
2) Emergency MRI and reconstruction of all ligamentous structures
3) Emergency arteriogram followed by MRI
4) Emergency surgery with open reduction and repair of all torn structures with vascular surgery available
5) Closed reduction in the emergency room and reevaluation of the vascular status
The patient has an acute traumatic anteromedial dislocation of the knee with occlusion of the popliteal artery with a possible tear. Treatment should include reduction and reevaluation of the vascular status. At this time, if pulses are symmetric, observation may be appropriate without surgical intervention of the artery, but documentation with studies would be appropriate. Delayed reconstruction of injured structures is appropriate.
A 26-year-old male presents after a motor vehicle accident. Work-up reveals a closed left femoral shaft fracture, and an ipsilateral posterior wall fracture. He undergoes intramedullary nailing of the femur, and open reduction internal fixation of the posterior wall. He is treated with 25 mg of indomethacin three times daily for 6 weeks following an initial dose on the evening of surgery for heterotopic ossification prophylaxis. Which of the following is true regarding this post-operative treatment protocol?
1) It is associated with an increased rate of femoral shaft nonunion
2) It has no effect on the healing time of the posterior wall fracture
3) It is associated with a faster time to union
4) Indomethacin is superior to radiation treatment in the prevention of heterotopic ossification
5) There is a decreased rate of revision surgery needed when indomethacin is administered post-operatively
Heterotopic ossification (HO) prophylaxis with indomethacin has been shown to increase the risk of long-bone nonunion.
Indomethacin therapy has been shown to be an effective means of preventing HO formation, however literature has shown that it increases the risk of long bone and acetabular nonunion. Indomethacin works primarily by inhibiting IGF-1, which is a different mechanism from other NSAID's which typically inhibit the COX enzymes. IGF-1 is important for bone healing, and its inhibition may be a risk factor for delayed bone healing.
Burd et al performed a study to determine if patients with an acetabular fracture, who received indomethacin for prophylaxis against HO, were at risk of delayed healing or nonunion of any associated fractures of long bones. The study group consisted of 112 patients who had sustained at least one concomitant fracture of a long bone; of which 36 needed no prophylaxis, 38 received focal radiation and 38 received indomethacin. When comparing patients who received indomethacin with those who did not, a significant difference was noted in the rate of long bone nonunion (26% vs 7%).
Jordan et al performed a study to document the efficacy of variable treatment durations with indomethacin prophylaxis for HO and its effect on union of the posterior wall (PW) in operatively treated acetabular fractures. Patients were randomly assigned to one of four treatment groups: (1) placebo for 6 weeks,
(2) 3 days of indomethacin followed by placebo for a total of 6 weeks, (3) 1
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 50High Yield
-A 27-year-old woman who was an unrestrained driver in a head-on collision sustained the following injuries: bilateral supracondylar femur fractures, a left talus fracture, multiple left metatarsal fractures, a right distal radius fracture, and a left open elbow fracture-dislocation. Which of the following serologic inflammatory markers drawn in this patient has been shown to be a reliable measure of systemic inflammatory response, correlating with injury severity and outcome?
Explanation
No detailed explanation provided for this question.
You Might Also Like


Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon