Quadrilateral Space Syndrome: Anatomy, Diagnosis, and Surgical Decompression
Key Takeaway
Quadrilateral space syndrome (QSS) is a rare neurovascular entrapment disorder caused by compression of the axillary nerve and posterior humeral circumflex artery. Typically affecting young overhead athletes, it presents with poorly localized shoulder pain and teres minor atrophy. Surgical decompression, utilizing the Cahill and Palmer posterior approach, involves releasing fibrous bands within the quadrilateral space to restore neurovascular flow and alleviate symptoms.
INTRODUCTION TO QUADRILATERAL SPACE SYNDROME
Quadrilateral space syndrome (QSS) is an uncommon but clinically significant neurovascular entrapment neuropathy characterized by the compression of the axillary nerve and the posterior humeral circumflex artery (PHCA) within the anatomic confines of the quadrilateral space. First comprehensively described by Cahill and Palmer in 1983, this syndrome remains a diagnostic challenge due to its insidious onset and the frequently vague, poorly localized nature of the presenting symptoms.
The condition predominantly affects the dominant extremity of young, active adults—particularly athletes engaged in repetitive overhead sports such as baseball (pitchers), volleyball, tennis, and swimming. The peak demographic incidence occurs between 20 and 35 years of age. Left untreated, QSS can lead to chronic posterior shoulder pain, selective atrophy of the teres minor and deltoid musculature, and a significant decline in athletic performance and overhead functional capacity.
SURGICAL ANATOMY AND BIOMECHANICS
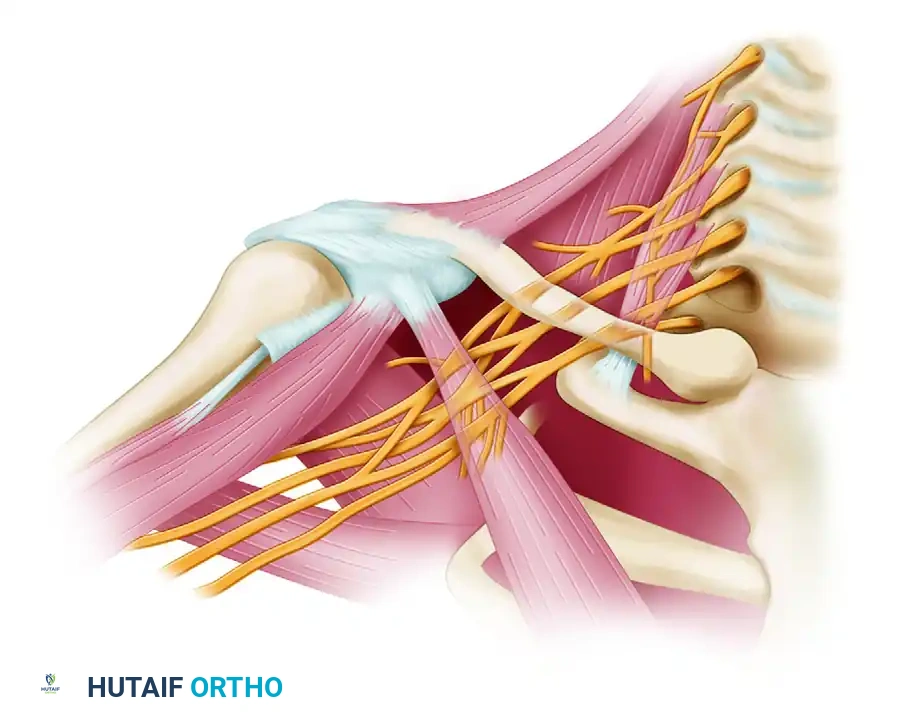
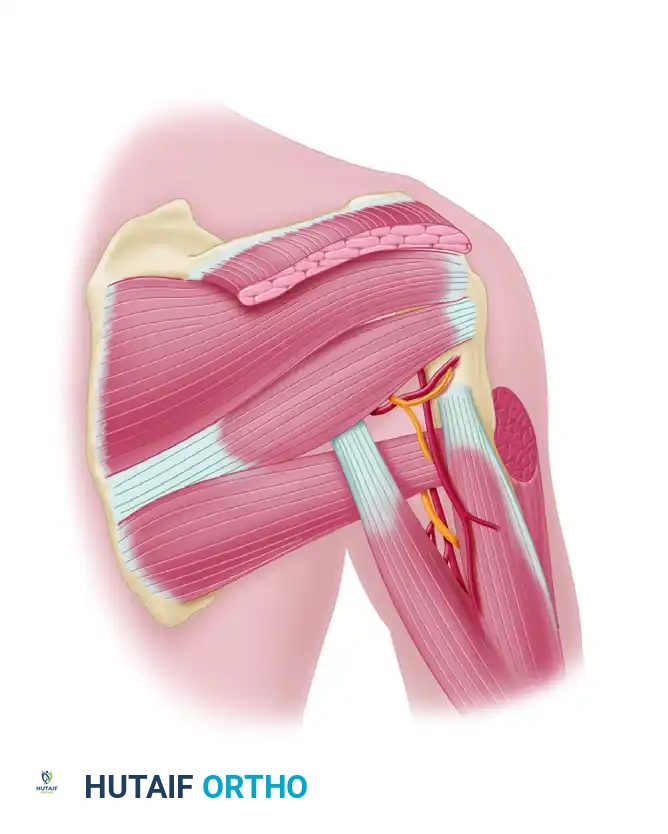
A profound understanding of the posterior shoulder anatomy is paramount for both accurate diagnosis and safe surgical decompression. The quadrilateral space is an anatomic interval in the posterior shoulder complex, acting as a primary conduit for neurovascular structures exiting the axilla to supply the posterior shoulder.
Boundaries of the Quadrilateral Space
The space is defined by four distinct anatomic borders:
* Superior Border: The inferior margin of the teres minor muscle and the inferior glenohumeral joint capsule.
* Inferior Border: The superior margin of the teres major muscle.
* Medial Border: The lateral margin of the long head of the triceps brachii muscle.
* Lateral Border: The surgical neck of the humeral shaft.
Contents of the Space
- Axillary Nerve: Arising from the posterior cord of the brachial plexus (C5, C6), the axillary nerve traverses the quadrilateral space and divides into anterior and posterior branches. The posterior branch provides motor innervation to the teres minor and the posterior head of the deltoid, and sensory innervation to the lateral shoulder via the superior lateral cutaneous nerve of the arm.
- Posterior Humeral Circumflex Artery (PHCA): A branch of the third part of the axillary artery, the PHCA travels alongside the axillary nerve to supply the deltoid, teres minor, and the glenohumeral joint capsule.
Clinical Pearl: Dynamic Compression
The quadrilateral space is not static. During abduction and external rotation (ABER) of the upper extremity, the teres minor and teres major muscles undergo a "scissoring" effect, significantly reducing the cross-sectional area of the space. This dynamic narrowing is the primary biomechanical driver of neurovascular compression in overhead athletes.
PATHOPHYSIOLOGY AND ETIOLOGY
The exact etiology of QSS is often multifactorial, but the primary pathological mechanism is the formation of anomalous fibrous bands within the quadrilateral space. These transverse or oblique fascial bands tether the axillary nerve and PHCA against the muscular borders or the humeral shaft.
Other contributing factors include:
* Muscular Hypertrophy: Hypertrophy of the teres minor, teres major, or the long head of the triceps in elite athletes can decrease the baseline volume of the space.
* Trauma: Direct blunt trauma to the posterior shoulder or a history of glenohumeral dislocation can lead to localized hematoma, subsequent fibrosis, and scarring within the space.
* Anatomic Variants: Aberrant muscular slips or variations in the origin of the long head of the triceps.
* Paralabral Cysts: Inferior glenohumeral joint cysts extending into the quadrilateral space (often associated with posterior labral tears).
CLINICAL PRESENTATION AND DIAGNOSIS
Diagnosing QSS requires a high index of suspicion, as the symptoms frequently mimic other common shoulder pathologies, such as rotator cuff tendinopathy, internal impingement, or cervical radiculopathy.
Subjective Symptoms
Patients typically report poorly localized, aching pain in the anterior, lateral, or posterior aspect of the shoulder. The pain is exacerbated by overhead activities and is often accompanied by non-dermatomal paresthesias or a feeling of "heaviness" in the arm. Unlike cervical radiculopathy, the pain rarely radiates distal to the elbow.
Objective Physical Examination
- Point Tenderness: The hallmark physical finding is exquisite point tenderness over the quadrilateral space, located posteriorly, just inferior to the teres minor insertion and lateral to the long head of the triceps.
- Provocative Testing (ABER Test): Symptoms are reliably reproduced by placing the patient's arm in 90 degrees of abduction and maximal external rotation for 1 minute. This position dynamically compresses the neurovascular bundle.
- Motor Evaluation: Weakness and atrophy are notoriously difficult to detect clinically in the early stages unless significant deltoid involvement is present. The teres minor is a relatively small muscle, and its weakness in external rotation is often masked by a robust infraspinatus.
Diagnostic Imaging Modalities
- Magnetic Resonance Imaging (MRI): MRI is the gold standard non-invasive diagnostic tool. The classic finding is selective fatty infiltration, edema, or atrophy of the teres minor muscle (and occasionally the deltoid). This denervation pattern, isolated to the axillary nerve distribution, is highly suggestive of QSS.
- MR Angiography (MRA) or Conventional Arteriography: Arteriography performed with the arm in the provocative ABER position will demonstrate dynamic occlusion or focal stenosis of the posterior humeral circumflex artery. While historically considered the definitive test, it is now often reserved for complex or equivocal cases due to its invasive nature.
- Electromyography and Nerve Conduction Studies (EMG/NCS): EMG/NCS are frequently normal or inconclusive in QSS. The compression is often dynamic and positional, meaning resting nerve conduction may remain unimpaired until late-stage, irreversible axonal damage has occurred.
INDICATIONS FOR SURGICAL INTERVENTION
Surgical decompression is indicated for patients who have failed a comprehensive trial of conservative management (typically 3 to 6 months). Conservative measures include activity modification, cessation of overhead sports, non-steroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy (focusing on posterior capsule stretching and periscapular stabilization), and ultrasound-guided corticosteroid injections into the quadrilateral space.
Absolute Indications for Surgery:
* Refractory, debilitating pain precluding activities of daily living or athletic participation.
* Progressive, MRI-confirmed atrophy of the teres minor or deltoid musculature.
* Demonstrable dynamic occlusion of the PHCA with corresponding severe ischemic symptoms.
SURGICAL TECHNIQUE: POSTERIOR DECOMPRESSION (CAHILL AND PALMER)
The posterior approach described by Cahill and Palmer remains the gold standard for direct visualization and decompression of the quadrilateral space.
1. Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia, often supplemented with an interscalene regional nerve block for postoperative pain control. The patient is positioned in the lateral decubitus position with the operative arm draped free to allow for intraoperative manipulation and provocative testing. Alternatively, the prone position can be utilized based on surgeon preference.
2. Incision and Superficial Dissection
- Identify the spine of the scapula and the posterior border of the deltoid.
- Make a curvilinear incision parallel and just inferior to the spine of the scapula. Curve the incision inferiorly over the posterior aspect of the humerus to allow for adequate inferior and lateral dissection.
- Develop a full-thickness skin flap, including all subcutaneous tissue down to the deep deltoid fascia.
🚨 Surgical Warning: Meticulous Hemostasis
Control bleeding, which may be moderately severe, with electrocautery immediately upon raising the flaps. If hemostasis is not achieved before the deep fascia is opened, blood will dissect rapidly into the loose areolar tissue planes. This markedly hinders the visualization of the delicate neurovascular bundle and increases the risk of iatrogenic injury.
3. Deep Dissection and Deltoid Reflection
- Incise the deep fascia at the inferior border of the deltoid muscle. Begin the dissection inferolaterally and proceed superiorly and medially.
- Carefully elevate and detach the posterior deltoid from the spine of the scapula using electrocautery.
- Crucial Step: Leave a sufficient border (cuff) of the musculotendinous origin attached to the scapular spine to facilitate robust resuture and repair during closure.
4. Teres Minor Takedown
- Identify the teres minor muscle belly and trace it laterally to its insertion on the inferior facet of the greater tuberosity and the posterior rotator cuff.
- Detach the teres minor at its tendinous insertion.
- Reflect the teres minor medially. This maneuver will expose the underlying quadrilateral space and leave a small opening in the posterior glenohumeral capsule.
Clinical Pearl: Teres Minor Management
Extensive biomechanical and clinical follow-up studies have demonstrated that no clinically significant weakness of external rotation of the humerus is detected postoperatively if the teres minor is left detached. The infraspinatus provides overwhelming compensatory power for external rotation.
5. Decompression of the Quadrilateral Space
- With the teres minor reflected, the quadrilateral space is brought into direct view.
- Decompress the space utilizing a combination of blunt and sharp dissection.
- A finger inserted into this space and directed anteriorly will typically feel tethered and meet distinct resistance. This resistance is caused by the pathological fibrous bands traversing the space.
- Carefully resect all fibrous bands, adhesions, and scar tissue compressing the axillary nerve and the PHCA.
6. Neurovascular Management and Verification
- Identify the axillary nerve and the posterior humeral circumflex artery.
- Follow the neurovascular bundle anteriorly toward its origin from the main axillary vessels to ensure complete release of any proximal tethering.
- Pitfall Avoidance: Exercise extreme caution to avoid injuring the accompanying venae comitantes (veins). These vessels are thin-walled, highly prone to tearing, and can cause troublesome bleeding that obscures the surgical field.
- Dynamic Verification: After decompression is visually complete, place a palpating finger directly on the posterior circumflex artery. Abduct and externally rotate the arm (ABER position) and test the arterial pulse. A strong, bounding pulse in the provocative position confirms adequate decompression.
7. Closure
- Irrigate the surgical bed copiously.
- Do not reattach the teres minor to the capsule or greater tuberosity. Allow it to retract medially.
- Anatomically approximate and repair the posterior deltoid to the musculotendinous cuff left on the spine of the scapula using heavy, non-absorbable sutures (e.g., #2 FiberWire or Ethibond).
- Close the subcutaneous tissue and skin in a standard layered fashion.
POSTOPERATIVE CARE AND REHABILITATION
A structured, phased rehabilitation protocol is essential to optimize outcomes and prevent postoperative complications such as adhesive capsulitis.
Phase I: Protection and Early Motion (Weeks 0-2)
- Immobilization: A standard shoulder sling is worn primarily for comfort and to protect the deltoid repair. The sling can be discontinued as soon as the patient feels comfortable, usually within 1 to 2 weeks.
- Range of Motion (ROM): Early, gentle passive range of motion (PROM) and active-assisted range of motion (AAROM) are highly encouraged immediately postoperatively to avoid superimposed adhesive capsulitis. Pendulum exercises and supine forward elevation are initiated.
- Precautions: Avoid active extension and active horizontal abduction to protect the posterior deltoid repair.
Phase II: Active Motion and Early Strengthening (Weeks 3-6)
- Transition to full active range of motion (AROM) in all planes.
- Initiate submaximal, pain-free isometric strengthening for the rotator cuff and periscapular stabilizers.
- Begin gentle posterior capsular stretching if any internal rotation deficit is noted.
Phase III: Advanced Strengthening and Return to Play (Weeks 6-12+)
- Progressive isotonic strengthening of the rotator cuff, deltoid, and periscapular musculature.
- Incorporate sport-specific kinetic chain exercises.
- Overhead athletes may begin a structured, interval return-to-throwing or return-to-play program around 10 to 12 weeks postoperatively, contingent upon the restoration of full, painless ROM and symmetrical shoulder strength.
COMPLICATIONS
While surgical decompression is generally highly successful, potential complications include:
* Iatrogenic Nerve Injury: Direct injury to the axillary nerve or its branches during dissection.
* Vascular Injury: Tearing of the PHCA or its accompanying veins, leading to hematoma formation.
* Deltoid Dehiscence: Failure of the posterior deltoid repair, resulting in weakness and cosmetic deformity. Strict adherence to leaving a robust fascial cuff during the approach mitigates this risk.
* Adhesive Capsulitis: Postoperative stiffness is the most common complication, underscoring the critical need for early, supervised range of motion.
* Incomplete Decompression: Failure to release all fibrous bands, leading to persistent symptoms and the potential need for revision surgery. Dynamic intraoperative pulse palpation is the best preventative measure against this outcome.
You Might Also Like