Open Capsular Shift for Multidirectional and Posterior Shoulder Instability
Key Takeaway
The open capsular shift remains a foundational procedure for managing multidirectional and complex posterior shoulder instability. This comprehensive surgical guide details the biomechanical rationale, precise step-by-step operative techniques—including humeral and glenoid-based T-incisions—and rigorous postoperative rehabilitation protocols. Designed for orthopedic surgeons, it provides critical insights into managing concurrent Hill-Sachs lesions, optimizing capsular tensioning, and ensuring long-term glenohumeral stability while preserving functional range of motion.
INTRODUCTION TO THE CAPSULAR SHIFT
The open capsular shift, originally popularized by Neer and Foster, remains a cornerstone in the surgical armamentarium for the treatment of multidirectional instability (MDI) and complex posterior shoulder instability. While arthroscopic techniques have advanced significantly, the open capsular shift provides unparalleled access for volumetric reduction of the redundant capsule, direct management of severe capsular laxity, and robust tissue imbrication.
The fundamental biomechanical goal of the capsular shift is to eliminate the redundant inferior capsular pouch and address posterior capsular laxity by advancing the inferior glenohumeral ligament (IGHL) complex superiorly and laterally (or medially, depending on the approach). This effectively restores the "hammock" effect of the IGHL, providing a dynamic checkrein against inferior and anteroposterior translation without over-constraining the glenohumeral joint.
💡 Clinical Pearl
The success of a capsular shift relies heavily on precise preoperative clinical examination. The surgeon must definitively determine the primary direction of instability (anterior, posterior, or inferior) under anesthesia, as this dictates the orientation of the capsulotomy and the vector of the capsular shift.
PREOPERATIVE EVALUATION AND IMAGING
Clinical Assessment
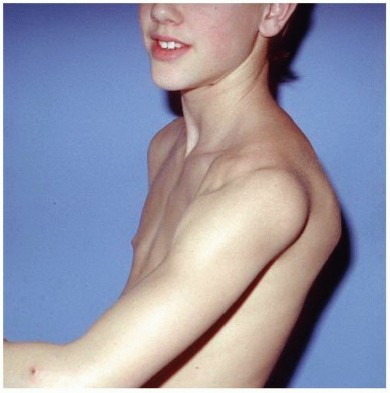
A meticulous history and physical examination are paramount. Patients with atraumatic MDI often present with generalized ligamentous laxity (Beighton score >4). The examination must include the sulcus sign (assessed in neutral and external rotation to evaluate the rotator interval), the apprehension/relocation test, the jerk test, and the shift-and-load test.
Advanced Imaging
Standard radiographs (True AP, Scapular Y, and Axillary lateral) are mandatory to assess for glenoid version, bone loss, and humeral head defects.
For complex instability, a T2-weighted axial Magnetic Resonance Arthrography (MRA) with intra-articular contrast is the gold standard. MRA allows for the precise evaluation of:
* Capsular Volume: Quantifying the degree of redundancy.
* Rotator Interval: Identifying a gap greater than 1 cm between the superior glenohumeral ligament (SGHL) and middle glenohumeral ligament (MGHL).
* Labral Pathology: Specifically evaluating for loss of chondrolabral containment.
* The Kim Lesion: As described by Kim et al., this is a concealed, incomplete avulsion of the posteroinferior labrum. MRA often reveals a chondrolabral cavity with erosion, cracking, or partial detachment posteriorly and inferiorly in over 80% of posterior instability cases.
MANAGEMENT OF CONCURRENT BONY DEFECTS
Addressing humeral head bone loss (Hill-Sachs lesions) is critical to preventing recurrent instability. The management algorithm is dictated by the size of the defect relative to the humeral head articular surface:
- 20% to 30% Defect: In the acute setting, these engaging lesions may be treated by disimpaction and bone grafting. In the chronic setting, an arthroscopic remplissage (transfer of the infraspinatus tendon and posterior capsule into the defect) is highly effective. Wolf et al. demonstrated excellent outcomes utilizing suture anchors to secure the infraspinatus into the defect, effectively converting an intra-articular lesion to an extra-articular one.
- 30% to 40% Defect: These larger defects are best managed indirectly via a Latarjet procedure. By extending the glenoid articular arc with the coracoid bone block, the Hill-Sachs lesion is prevented from engaging the anterior glenoid rim. Alternatively, direct filling of the defect using structural osteoarticular allografts can yield satisfactory results, though hardware removal may be required later. The use of focal metallic resurfacing implants (e.g., HemiCap) or humeral rotational osteotomies combined with capsular imbrication are viable, albeit less common, alternatives.
- >45% Defect: Massive defects compromising nearly half of the articular surface generally necessitate prosthetic replacement (hemiarthroplasty or total shoulder arthroplasty) to restore joint congruity and stability.
SURGICAL TECHNIQUE: ANTERIOR CAPSULAR SHIFT
Approach and Incision Selection
The procedure is performed via a standard deltopectoral approach. The cephalic vein is typically retracted laterally with the deltoid. The clavipectoral fascia is incised, and the conjoined tendon is retracted medially.
Two primary techniques exist for the capsulotomy, each with specific indications:
- Glenoid-Based T-Incision (O’Brien, Warren, Schwartz): The vertical limb of the "T" is made adjacent to the glenoid. This approach is highly advantageous if there is a concomitant detached anterior glenoid labrum (Bankart lesion) that requires direct repair.
- Humeral-Based T-Incision (Neer Technique): The vertical limb is made adjacent to the humeral neck. This is the preferred technique for profound inferior instability without a labral tear. It allows the surgeon to extend the posterior portion of the capsular flap further around the humerus (facilitated by external rotation), enabling maximal posterior and inferior capsular tightening.
⚠️ Surgical Warning
When developing the inferior capsular flap, the axillary nerve is at extreme risk as it courses immediately inferior to the capsule. A flat blunt elevator (e.g., a Fukuda or Darrach retractor) must be placed between the inferior capsule and the axillary nerve to protect it during capsular release.
Step-by-Step Neer Humeral-Based Shift
- Subscapularis Management: The subscapularis tendon is divided approximately 1 cm medial to its insertion on the lesser tuberosity. It is critical to leave the inferior-most portion of the subscapularis tendon intact and free so that the muscle's excursion is not tethered postoperatively.
- Rotator Interval Closure: Inspect the rotator interval. Close the cleft between the MGHL and the SGHL using robust, nonabsorbable sutures to eliminate superior capsular laxity.
- Capsulotomy: Make a T-shaped opening by incising horizontally between the MGHL and the IGHL.
- Flap Mobilization: With the arm in external rotation and the axillary nerve strictly protected, develop the inferior capsular flap. Detach the reinforced portion of the capsule (containing the IGHL) from the inferior aspect of the humeral neck, extending around to the posterior aspect of the neck.
- Intra-articular Inspection: Inspect the joint meticulously. Remove any osteochondral loose bodies or degenerative labral tags.
- Trial Reduction and Tensioning: Test for posterior instability by applying forward traction on the inferior capsular flap. This allows the surgeon to estimate the precise new location for the flap insertion that will eliminate the inferior pouch and posterior redundancy.
- Humeral Preparation: Using curettes and a small gouge, create a shallow bleeding bone slot at the anterior and inferior sulcus of the humeral neck.
- Capsular Fixation: Suture anchors are the modern gold standard for securing the capsule to the humeral neck. Suture the inferior capsular flap to the prepared bone slot and the subscapularis stump.
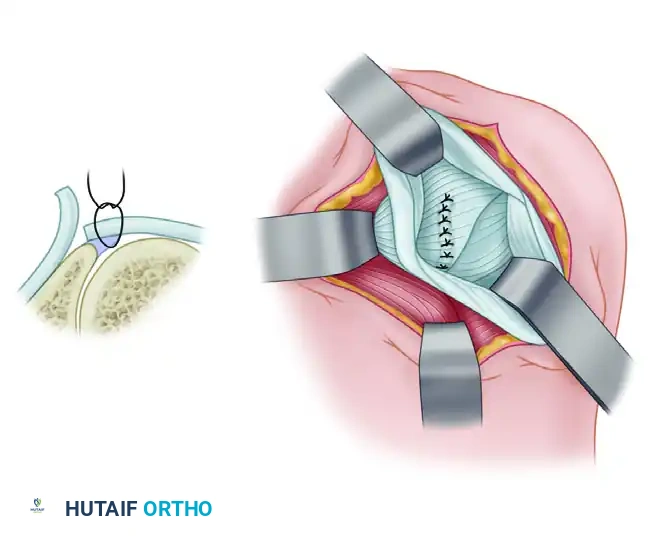
- The "Shift": The tension applied must completely obliterate the inferior pouch. Suture the inferior flap first, drawing it superiorly and laterally. Next, draw the superior flap down over the inferior flap and suture it in place. This imbrication causes the MGHL to reinforce the anterior capsule, acting as a dynamic sling against inferior subluxation.
- Arm Positioning During Fixation: The arm must be held in slight flexion and approximately 10 degrees of external rotation during capsular reattachment.
- Modification for Athletes: Bigliani et al. recommend repairing the capsule with the arm in 25 degrees of external rotation and 20 degrees of abduction. For overhead throwing athletes, even greater abduction and external rotation are required to prevent postoperative loss of functional range of motion.
- Closure: Bring the subscapularis tendon over the shifted capsule and repair it anatomically to its stump using heavy nonabsorbable sutures. Close the deltopectoral interval and skin standardly.
SURGICAL TREATMENT OF POSTERIOR INSTABILITY
Posterior instability is predominantly treated non-operatively. Traumatic posterior dislocations (common in football linemen and hockey players) respond poorly to conservative care compared to atraumatic MDI. However, if 4 to 6 months of rigorous, scapular-stabilizing rehabilitation fails, and the patient is emotionally stable without habitual (voluntary) dislocation, surgery is indicated.
If an open procedure is selected for disabling posterior subluxation, the posterior inferior capsular shift is the procedure of choice.
Arthroscopic Integration
Prior to an open posterior shift, a diagnostic arthroscopy is highly recommended. This allows the surgeon to:
* Evaluate and arthroscopically close a patulous rotator interval anteriorly.
* Identify and repair Kim lesions or chondrolabral retroversion.
* Address any posterior bony Bankart lesions (which may require arthroscopic or open screw fixation depending on size).
Once the anterior interval is closed arthroscopically, the patient is repositioned, and an open posterior approach is utilized to perform a humeral-based posterior-inferior capsular shift, tensioning the capsule superiorly and laterally to eliminate the posterior recess.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of a capsular shift is inextricably linked to strict adherence to a phased rehabilitation protocol. The capsule and ligaments function only as a checkrein; complete recovery of the dynamic stabilizers (rotator cuff and deltoid) is mandatory to protect the surgical repair.
Phase I: Immediate Postoperative (Weeks 0–4)
- Immobilization: The extremity is placed in a commercial shoulder immobilizer with the arm in 30 to 40 degrees of abduction and slight external rotation. Light plastic splints may be used to maintain neutral flexion-extension and 20 degrees of internal rotation depending on the specific shift performed.
- Immediate Motion: Active range of motion (ROM) for the elbow, wrist, and hand is initiated on postoperative day one.
- Day 3: Pendulum (Codman’s) exercises are introduced.
- Day 10: Passive and active-assisted external rotation is permitted up to 10 degrees. Forward elevation is permitted up to 90 degrees. Submaximal isometric exercises for the deltoid and rotator cuff begin.
- Weeks 2 to 4: Isometric strengthening continues. External rotation is gradually increased to 30 degrees, and forward elevation is progressed to 140 degrees.
Phase II: Intermediate Motion (Weeks 4–6)
- ROM Progression: External rotation is increased to 40 degrees. Forward elevation is increased to 160 degrees.
- Strengthening: Isotonic resistive exercises are initiated, focusing on the internal and external rotators (to curb anteroposterior displacement) and the supraspinatus/middle deltoid (to curb inferior displacement).
Phase III: Advanced Strengthening (Weeks 6–12)
- Week 6: External rotation is pushed to 50 degrees, and full forward elevation (180 degrees) is targeted.
- Month 3: External rotation is progressed to full functional limits.
- Thrower's Modification: In the dominant shoulder of throwing athletes, external rotation is progressed more rapidly to prevent stiffness. However, extreme caution is required in late adolescents, as overly aggressive stretching can stretch out the repair and lead to recurrent instability.
Phase IV: Return to Play (Months 3–12)
- Months 3 to 9: Progressive functional strengthening. Lifting weights greater than 9 kg (20 lbs) and participation in any sports are strictly prohibited for a minimum of 9 months. Return to sport is only permitted when manual muscle testing demonstrates strength equal to the contralateral, uninjured side.
- 1 Year: Ligamentous healing is considered biologically mature at 12 months. Until this milestone is reached, patients are strictly advised against heavy overhead use, contact sports, and specific swimming strokes that place extreme stress on the capsule (e.g., butterfly stroke, backstroke).
💡 Clinical Pearl
The most common cause of failure following an open capsular shift is non-compliance with the postoperative rehabilitation protocol, specifically premature return to heavy lifting or overhead sports before dynamic muscular stability has been fully restored.
📚 Medical References
- capsular shift procedure for glenohumeral instability, Am J Sports Med 27:162, 1999.
- Hayes PRL, Flatow EL: Technical note: attrition sign in impingement syndrome, Arthroscopy 18:E44, 2002.
- Hecht P, Hayashi K, Cooley AJ, et al: The thermal effect of monopolar radiofrequency energy on the properties of joint capsule: an in vivo histologic study using a sheep model, Am J Sports Med 26:808, 1998.
- Helbig B, Wagner P, Dohler R: Mobilization of frozen shoulder under general anesthesia, Acta Orthop Belg 49:267, 1983.
- Henkus JE, Cobben LP, Coerkamp EG, et al: The accuracy of subacromial injections: a prospective randomized magnetic resonance imaging study, Arthroscopy 22:277, 2006.
- Holtby R, Razmjou H: Accuracy of the Speed’s and Yergason’s tests in detecting biceps pathology and SLAP lesions: comparison with arthroscopic fi ndings, Arthroscopy 20:231, 2004.
- Holtby R, Razmjou H: Validity of the supraspinatus test as a single clinical test in diagnosing patients with rotator cuff pathology, J Orthop Sports Phys Ther 34:194, 2004.
- Holzknecht G: Über Bursitis mit Knochenverbildung, Wien Med Wochenschr 43:2757, 1911.
- Howell SM, Imobersteg AM, Segar DH, et al: Clarifi cation of the role of the supraspinatus muscle in shoulder function, J Bone Joint Surg 68A:398, 1986.
- Hurt G, Baker CL Jr: Calcifi c tendinitis of the shoulder, Orthop Clin North Am 34:567, 2003.
- Iannotti JP, Ciccone J, Buss DD, et al: Accuracy of offi ce-based ultrasonography of the shoulder for the diagnosis of rotator cuff tears, J Bone Joint Surg 87A:1305, 2005.
- Iannotti JP, Codsi JM, Kwon YW, et al: Porcine small intestine submucosa augmentation of surgical repair of chronic twotendon rotator cuff tears: a randomized, controlled trial, J Bone Joint Surg 88A:1238, 2006.
- Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi transfer for irreparable posterosuperior rotator cuff tears: factors affecting outcome, J Bone Joint Surg 88A:342, 2006.
- Iannotti JP, Swiotkowski M, Esterhai J, et al: Intraoperative assessment of rotator cuff vascularity using laser Doppler fl owmetry. Abstract presented at the annual meeting of the American Academy of Orthopaedic Surgeons, Las Vegas, Feb 1989.
- Iannotti JP, Zlatkin MB, Esterhai JL, et al: Magnetic resonance imaging of the shoulder, J Bone Joint Surg 73A:17, 1991.
- Inman VT, Saunders JB, Abbott LC: Observations in the function of the shoulder joint, J Bone Joint Surg 26A:1, 1944.
- Jarjavay JF: Sur la luxation du tendon de la longue portion du muscle biceps huméral; sur la luxation des tendons des muscles péroniers latéraux, Gazette Hebdomadaire de Médecine et de Chirurgie 21:325, 1867.
- Jerosch J, Strauss JM, Schmiel S: Arthroscopic treatment of calcifi c tendinitis of the shoulder, J Shoulder Elbow Surg 7:30, 1998.
- Jobe CM: Gross anatomy of the shoulder. In Rockwood CA Jr, Matsen FA III, eds: The shoulder, Philadelphia, 1990, Saunders. Jobe FW: Symposium: shoulder problems in overhead-overuse sports—thrower problems, Am J Sports Med 7:139, 1979.
- Jobe FW: Painful athletic injuries of the shoulder, Clin Orthop Relat Res 173:117, 1983.
- Jobe FW: Impingement problems in the athlete, Instr Course Lect 38:205, 1989.
- Jobe FW, Kvitne RS: Shoulder pain in the overhand or throwing athlete: the relationship of anterior instability and rotator cuff impingement, Orthop Rev 18:963, 1989.
- Jobe FW, Tibone JE, Perry J, et al: An EMG analysis of the shoulder in throwing and pitching: a preliminary report, Am J Sports Med 11:3, 1983.
- Jozsa L, Baliut BJ, Reffy A: Calcifying tendinopathy, Arch Orthop Trauma Surg 97:305, 1980.
- Kaplan PE, Kernahan WT Jr: Rotator cuff rupture management with suprascapular neuropathy, Arch Phys Med Rehabil 65:273, 1984.
- Karzel R, Nuber G, Lautenschlager E: Contact stresses during compression loading of the glenohumeral joint: the role of the glenoid labrum, Proc Inst Med Chicago 42:64, 1989.
- Kernwein GA, Roseberg, Sneed WR Jr: Arthrographic studies of the shoulder joint, J Bone Joint Surg 39A:1267, 1957.
- Kessel L, Bayley I, Young A: The frozen shoulder, Br J Hosp Med 25:334, 1981.
- Klepps SJ, Galatz LM: The treatment of anterior-superior instability with the pectoralis major muscle transfer, Oper Tech Orthop 13:228, 2003.
- Kronberg M, Wahlstrom P, Brostrom LA: Shoulder function after surgical repair of rotator cuff tears, J Shoulder Elbow Surg 6:125, 1997.
- Kurtz CA, Humble BJ, Rodosky MW, et al: Symptomatic
You Might Also Like