Terrible Triad Injury of the Elbow: Epidemiology, Anatomy, Biomechanics & Surgical Indications

Key Takeaway
A terrible triad elbow injury is a complex, highly unstable elbow pattern characterized by a radial head fracture, coronoid process fracture, and disruption of the lateral ulnar collateral ligament (LUCL). This severe injury typically results from a fall, leading to posterolateral rotatory instability and almost always requires meticulous surgical intervention for stabilization and optimal functional recovery.
Introduction & Epidemiology
The terrible triad injury (TTI) of the elbow is a complex and highly unstable injury pattern, characterized by a combination of radial head fracture, coronoid process fracture, and disruption of the lateral ulnar collateral ligament (LUCL) complex. This injury represents a severe form of posterolateral rotatory instability (PLRI) and, if not accurately diagnosed and meticulously managed, frequently leads to chronic pain, instability, and significant functional deficits, including severe stiffness and post-traumatic arthritis.
Epidemiologically, TTI typically results from a fall onto an outstretched hand with the forearm supinated, leading to an axial load, valgus stress, and external rotation moment on the elbow joint. This mechanism initiates a sequential pattern of soft tissue and bony injury, beginning with the LUCL complex, progressing to the radial head, and finally involving the coronoid. While not as common as isolated elbow fractures, the incidence of TTI is significant among complex elbow dislocations, contributing substantially to the burden of elbow pathology in orthopedic practice. It predominantly affects active adults, often with high-energy mechanisms, though falls in elderly populations can also produce this pattern due to osteoporotic bone. The inherent instability and propensity for poor outcomes underscore the critical importance of a thorough understanding of its biomechanics, diagnosis, and surgical management for every orthopedic surgeon.
Surgical Anatomy & Biomechanics
A profound understanding of the intricate anatomy and biomechanics of the elbow joint is paramount for effective management of the terrible triad injury. The elbow is a hinge joint primarily formed by the articulation of the distal humerus with the proximal ulna and radius, providing both mobility and stability.
Bony Structures
- Distal Humerus: Comprises the trochlea (articulating with the ulna) and the capitellum (articulating with the radial head). The medial and lateral epicondyles serve as origins for collateral ligaments and muscle groups.
- Proximal Ulna: The olecranon and coronoid processes form the trochlear notch, which articulates with the humeral trochlea. The coronoid process is a key anterior stabilizer, resisting posterior displacement of the ulna relative to the humerus. Fractures of the coronoid significantly compromise this inherent bony stability.
- Radial Head: Articulates with the capitellum and the radial notch of the ulna. It contributes significantly to valgus stability and resistance to axial loading. Fractures of the radial head disrupt the integrity of the radiohumeral articulation and can lead to incongruity and pain.
Ligamentous Stabilizers
The elbow's stability is heavily reliant on its robust ligamentous structures:
- Medial Collateral Ligament (MCL) Complex: Consists of the anterior bundle (primary valgus stabilizer), posterior bundle, and transverse ligament. While typically spared in a primary TTI, its integrity must always be assessed.
-
Lateral Collateral Ligament (LCL) Complex:
Critical for posterolateral rotatory stability. It comprises:
- Lateral Ulnar Collateral Ligament (LUCL): Originates from the lateral epicondyle and inserts onto the supinator crest of the ulna. It is the primary stabilizer against posterolateral rotatory subluxation and is invariably disrupted in TTI.
- Radial Collateral Ligament (RCL): Extends from the lateral epicondyle to the annular ligament.
- Annular Ligament: Encircles the radial head, maintaining its articulation with the ulna.
- Accessory Lateral Collateral Ligament (ALCL): Reinforces the annular ligament.
- Capsule: The fibrous capsule surrounds the joint, reinforced by the collateral ligaments. Disruption of the capsule accompanies severe dislocations.
Biomechanics of TTI
The "terrible triad" represents a sequential disruption of elbow stability:
- LUCL Disruption: The injury typically begins with rupture of the LUCL due to a valgus and posterolateral rotatory force. This compromises the primary restraint to posterolateral rotation.
- Radial Head Fracture: As the posterolateral rotatory force continues, the radial head impacts the capitellum, leading to fracture. The radial head's contribution to axial and valgus stability is lost.
- Coronoid Process Fracture: With loss of the LUCL and radial head stability, the elbow becomes highly susceptible to posterior displacement. The coronoid process, now acting as a fulcrum, fractures as the olecranon is driven posteriorly against the distal humerus. The size and type of coronoid fracture are directly proportional to the degree of instability.
This sequence creates a vicious circle of instability. Failure to reconstruct all three components (LUCL, radial head, coronoid) leads to persistent instability, especially in posterolateral rotation, and a high risk of redislocation and progressive arthrosis.
Indications & Contraindications
Indications for Operative vs. Non-Operative Management
Given the inherent instability of the terrible triad injury, surgical intervention is almost universally indicated. Non-operative management is rarely successful and typically reserved for highly select cases, often with poor functional outcomes.
Operative Indications:
- All terrible triad injuries: By definition, the combination of radial head fracture, coronoid fracture, and LUCL disruption leads to gross elbow instability, necessitating surgical stabilization.
- Unstable elbow joint: Inability to achieve or maintain a stable, concentric reduction through a full range of motion (typically 30-130 degrees) post-reduction, especially with gentle valgus and rotational stress, is a definitive indication for surgery.
-
Radial Head Fractures:
- Mason type II, III, or IV with mechanical block, significant displacement (>2mm), angulation, or comminution, particularly if associated with coronoid fracture and LUCL injury.
- Displaced or comminuted fractures preventing stable reduction of the elbow.
-
Coronoid Fractures:
- O'Driscoll Type I (>2mm fragment), Type II, or Type III fractures, especially if >10-15% of the coronoid height or articular surface is involved. These significantly compromise the primary anterior buttress.
- Any coronoid fracture contributing to persistent instability.
- LUCL Disruption: The presence of this injury is a core component of the TTI, and its surgical repair or reconstruction is essential for restoring posterolateral rotatory stability.
Non-Operative Indications:
- Extremely rare for true TTI: Non-operative management typically leads to chronic instability, stiffness, and poor outcomes.
- Medically unstable patient: Patients with severe comorbidities precluding safe anesthesia and surgery. In these extreme cases, judicious non-operative management with a brace and early controlled range of motion may be considered, but with guarded prognosis.
- Minimally displaced stable fractures (non-TTI scenario): In isolated radial head or coronoid fractures without concomitant ligamentous injury or dislocation, non-operative treatment may be appropriate. However, this is not a terrible triad injury.
- Patient refusal for surgery: Despite clear indications, a patient's informed refusal necessitates non-operative management, with thorough documentation of potential consequences.
Contraindications
Absolute Contraindications:
- Active infection: Local or systemic infection that would preclude safe surgical intervention.
- Lack of suitable soft tissue envelope: Severe open injuries or extensive soft tissue damage precluding wound closure or increasing infection risk.
Relative Contraindications:
- Severe medical comorbidities: Patients with significant cardiac, pulmonary, or neurological conditions where the risks of anesthesia and surgery outweigh the potential benefits. Careful multidisciplinary assessment is crucial.
- Extensive local tissue damage or bone loss: While not always a contraindication, it may necessitate alternative reconstructive strategies (e.g., bone grafting, external fixation).
- Patient's inability to comply with post-operative rehabilitation: This is a relative contraindication as successful outcomes heavily rely on diligent adherence to rehab protocols.
Table: Operative vs. Non-Operative Indications for Terrible Triad Injury
| Feature | Operative Indications | Non-Operative Indications (Rare for True TTI) | Patient Stability (for surgery) | Conscious, Cooperative patient requiring stabilization for radial head or radial head and coronoid and torn LUCL for stabilization. | Medically unstable patient, moribund, refusing surgery, or severe local infection/tissue viability issues preventing definitive stabilization. |
|---|---|---|
|
Radial Head Fracture:
|
| Mason Classification | - Type I (No displacement)
-
Type II (Partial articulation, mild displacement, small step-off)
-
Type III (Comminuted, displaced)
-
Type IV (Associated with elbow dislocation)
| Mason type I (non-displaced, stable) in isolated cases
without
TTI. |
|
Coronoid Fracture:
|
| O'Driscoll Classification | -
Type I (>2mm fragment, base fracture)
-
Type II (Tip fracture, <10% height)
-
Type III (Body fracture, >10% height)
| Minimal non-displaced tip fractures in isolation
without
other TTI components and stable elbow range of motion. |
|
Ligamentous Instability:
|
| LUCL Disruption |
Always indicates operative intervention
due to profound posterolateral rotatory instability. | None. By definition of TTI, LUCL is disrupted and requires repair. |
|
Elbow Stability:
|
| After Reduction |
Gross instability
with inability to maintain concentric reduction through full arc of motion (30-130 degrees), especially with valgus and rotational stress. | Exceptionally stable elbow after reduction (rare with TTI), full pain-free stable range of motion (often aided by external fixator). |
|
Associated Injuries:
|
| Neurovascular Compromise |
Requires urgent surgical intervention
to address the underlying cause (e.g., compartment syndrome, vascular injury, nerve impingement). | None. |
| Open Fracture/Dislocation |
Requires urgent surgical debridement and stabilization.
| None. |
|
Patient Factors:
|
| Medical Status | Medically fit for surgery and anesthesia. | Medically unstable, contraindicating general anesthesia. |
| Compliance | Capable and willing to comply with rigorous post-operative rehabilitation. | Unwilling or unable to comply with demanding rehabilitation. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for successful outcomes in terrible triad injuries, encompassing comprehensive diagnostic evaluation, surgical strategy, and logistics.
Diagnostic Workup
-
Clinical Examination:
- Neurovascular Status: Thorough assessment of radial, ulnar, and median nerve function and distal perfusion. Document pre-operatively.
- Soft Tissue Envelope: Evaluate for open wounds, abrasions, or swelling, which may influence surgical timing or approach.
- Elbow Stability: After initial reduction (if dislocated), assess stability by gently ranging the elbow from full extension to flexion, applying valgus/varus and rotational stress. Most TTIs will be grossly unstable.
-
Imaging:
- Plain Radiographs: Anteroposterior (AP) and lateral views are essential to confirm dislocation (if present), identify obvious fractures (radial head, coronoid), and rule out other bony injuries. Oblique views (radial head view) can better delineate radial head fracture patterns.
-
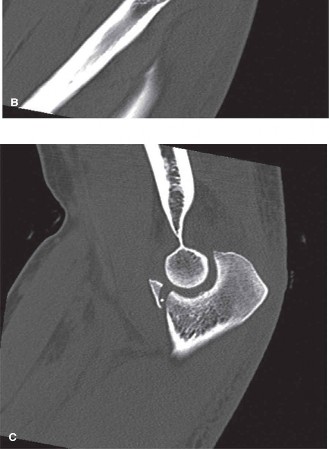
Computed Tomography (CT) Scan:
Absolutely essential.
A high-resolution CT scan with 3D reconstructions provides invaluable information regarding:
- Coronoid fracture morphology: Size, comminution, displacement, and involvement of the sublime tubercle (critical for MCL attachment).
- Radial head fracture pattern: Number of fragments, displacement, articular step-off, and associated impaction.
- Humerus and ulna integrity: Rule out associated fractures.
- Congruity of reduction: Confirm concentric reduction if performed before CT.
- Magnetic Resonance Imaging (MRI): While not routinely required acutely, MRI can provide detailed information about ligamentous injuries (LUCL, MCL) and capsular disruption. In cases of equivocal plain radiographs or CT findings regarding ligamentous stability, MRI can be supplementary. Its primary role is often for chronic instability or occult soft tissue injuries.

Illustrative pre-operative imaging of a terrible triad injury, demonstrating radial head fracture, coronoid fracture, and associated dislocation. A comprehensive CT scan is crucial for detailed fracture assessment.
Pre-operative Considerations
- Timing of Surgery: Early definitive fixation (within 1-2 weeks) is generally recommended to prevent contracture formation and facilitate early rehabilitation. Delayed surgery can make soft tissue dissection more challenging and increase the risk of stiffness.
- Anesthesia: General anesthesia is standard. Regional blocks (e.g., supraclavicular or interscalene brachial plexus block) can provide excellent post-operative pain control and improve patient comfort.
-
Implants and Equipment:
Ensure availability of:
- Radial head fracture fixation kits (low-profile plates, headless screws).
- Radial head arthroplasty implants (multiple sizes, stems, heads) if replacement is anticipated.
- Coronoid fixation options (suture anchors, cannulated screws, small fragment plates, suture lasso kits).
- Suture anchors for LUCL repair.
- Appropriate retractors, osteotomes, drills, and fluoroscopy.
- Bone graft (autograft or allograft) may be needed for bone loss.
-
Surgical Plan:
Based on imaging, formulate a clear step-by-step plan:
- Sequence of repair (typically coronoid, radial head, LUCL).
- Specific fixation techniques for each component.
- Contingency plans (e.g., if radial head repair is not feasible, plan for replacement).
Patient Positioning
- Supine Position with Arm on Hand Table: This is the most common position. The patient is placed supine on the operating table, and the affected arm is abducted onto a sterile hand table. This allows excellent access to both lateral and medial aspects of the elbow by rotating the arm. A padded arm holder can secure the humerus.
- Lateral Decubitus Position: Some surgeons prefer this for easier gravity-assisted access to the posterior and lateral elbow. The patient is positioned on their side, and the arm draped free.
- Tourniquet: A pneumatic tourniquet is applied to the upper arm to provide a bloodless field, crucial for visualization and precise dissection.
- Sterile Preparation and Draping: The arm, shoulder, and axilla are meticulously prepared with an antiseptic solution and draped to allow full range of motion of the elbow during the procedure and provide access for potential graft harvest if needed.
Detailed Surgical Approach / Technique
The surgical management of terrible triad injuries demands a systematic approach to address all components of the injury. The general principle is to restore the bony architecture first, followed by ligamentous stability. The typical sequence is coronoid repair, then radial head fixation/replacement, and finally, LUCL repair.
General Principles
- Systematic Exposure: Gain adequate exposure to all injured structures without excessive soft tissue stripping.
- Anatomic Reduction: Aim for anatomic reduction of all fracture fragments and ligamentous insertions.
- Stable Fixation: Achieve rigid internal fixation where possible to permit early controlled motion.
- Sequential Reconstruction: Address the most critical stabilizers first, assessing stability after each step.
- Intra-operative Assessment: Confirm stability and range of motion under fluoroscopy or direct visualization at the conclusion of the procedure.
Surgical Approach
The primary approach for terrible triad injuries is typically a posterolateral approach , which can be extended.
-
Skin Incision: A curvilinear incision is made starting proximally, 4-5 cm above the lateral epicondyle, extending distally over the epicondyle and continuing distally along the ulnar border of the forearm for 6-8 cm. This allows wide exposure.
-
Dissection to Internervous Plane (Kocher Approach):
- Subcutaneous tissues are incised, and full-thickness flaps are raised. The interval between the anconeus posteriorly and the extensor carpi ulnaris (ECU) anteriorly is identified.
- The Kocher interval is developed. This internervous plane is between the extensor carpi ulnaris (innervated by the radial nerve) and the anconeus (innervated by the radial nerve, but a separate branch, allowing dissection without injury to primary nerve branches).
- Care is taken to protect the posterior cutaneous nerve of the forearm (a branch of the radial nerve) and its branches crossing the field.
- The common extensor origin is released partially from the lateral epicondyle (anteriorly) or elevated carefully. The posterior aspect of the joint capsule and LUCL complex is visualized. The LUCL is typically avulsed from its humeral origin.
- The radial head and neck are exposed by splitting the anconeus-ECU interval and retracting the muscle bellies.
Intra-operative view of a lateral approach to the elbow, showcasing the exposure of the radial head and lateral epicondyle, crucial for addressing the radial head fracture and LUCL repair.
Step-by-Step Repair / Technique
1. Coronoid Fracture Management
The coronoid fracture is a key stabilizer. Its repair should precede radial head fixation or replacement, as restoration of the coronoid buttress is fundamental to elbow stability.
*
Exposure:
For Type I and some Type II fractures (tip or anteromedial facet fractures), the fragment can often be visualized and addressed through the lateral approach, especially if the elbow is dislocated or unstable. For larger or significantly displaced Type III fractures (basal or body fractures), an additional medial approach or a transolecranon osteotomy (controversial, often avoided if possible) might be necessary.
*
Techniques:
*
Suture Lasso/Lariat Technique:
For small to medium-sized fragments (O'Driscoll Type I/II), sutures are passed through drill holes in the proximal ulna, lassoing the coronoid fragment and tying it down, restoring its position. This is performed using an anterior capsulotomy if required to retrieve the fragment.
*
Lag Screw Fixation:
For larger, non-comminuted fragments, a small lag screw can provide stable fixation. This often requires an anterior-to-posterior trajectory from the ulna, or through a separate medial incision.
*
Small Plate Fixation:
For comminuted or larger basal fractures (O'Driscoll Type III), small fragment plates (e.g., 1/4 tubular plate or specific coronoid plates) can be applied. This often requires a separate medial incision for direct visualization and reduction.
*
Suture Anchors:
Small fragments can sometimes be secured using suture anchors inserted into the ulnar metaphysis.
2. Radial Head Fracture Management
The goal is to restore articular congruity and maintain stability.
*
Classification:
Mason-Hotchkiss classification guides treatment.
*
Options:
*
Open Reduction Internal Fixation (ORIF):
For Mason Type II fractures (displaced, two-part, or three-part non-comminuted) and some Type III fractures with reconstructible fragments. Small, low-profile screws (e.g., headless compression screws) or mini-plates are used. The fixation should be below the articular surface to avoid impingement during pronation/supination.
*
Radial Head Excision:
Historically performed, but largely abandoned in TTI due to profound loss of valgus and axial stability, leading to increased risk of instability, valgus deformity, and late degenerative changes.
Generally contraindicated in TTI.
*
Radial Head Arthroplasty (Replacement):
The preferred option for severely comminuted or unreconstructible Mason Type III or IV fractures. Implants can be metal (cobalt-chrome, titanium) or pyrocarbon. The goal is to restore the correct radial length and provide a buttress against valgus stress. The implant should be sized carefully to avoid overstuffing the radiocapitellar joint.
*
Selection:
* Reconstructible: ORIF.
* Unreconstructible comminution or large defect: Radial head replacement.
3. Lateral Ulnar Collateral Ligament (LUCL) Repair/Reconstruction
This is crucial for restoring posterolateral rotatory stability. The LUCL is typically avulsed from its humeral origin at the lateral epicondyle.
*
Identification:
The avulsed LUCL complex (often with a cuff of periosteum or common extensor origin) is identified.
*
Repair:
*
Direct Repair:
If the tissue quality is good and the ligament can be reapproximated to its anatomic origin on the lateral epicondyle, suture anchors (typically 2-3) are placed into the epicondyle. Non-absorbable sutures are passed through the avulsed ligamentous tissue and tied down with the forearm in pronation and the elbow flexed to 60-90 degrees to tension the LUCL appropriately.
*
Reconstruction:
If the LUCL tissue is severely damaged or chronic, a graft reconstruction may be necessary. Autografts (e.g., palmaris longus, gracilis, triceps fascia) or allografts can be used. Tunnels are drilled in the lateral epicondyle and ulna (supinator crest) to recreate the isometric course of the LUCL, and the graft is passed and secured.

*Radiographic image, likely post-operative, demonstrating internal fixation of the radial head and the presence of suture anchors or tunnels for ligamentous repair/reconstruction, reflecting a successfully treated terrible triad injury.*
4. Medial Collateral Ligament (MCL) Assessment
- Though less commonly injured primarily in TTI, the MCL should be dynamically stressed after the lateral structures are stabilized. If gross valgus instability persists after LUCL, coronoid, and radial head stabilization, an acute repair of the MCL (typically the anterior bundle) is indicated. This is performed via a separate medial incision, usually with suture anchors.
5. Capsular Repair
- The capsule, if extensively torn, should be meticulously repaired to further enhance stability and provide a barrier to heterotopic ossification.
6. Stability Assessment
- After all components are addressed, the elbow's stability is dynamically assessed through a full range of motion (from approximately 30° to 130° flexion, and with pronation/supination). Fluoroscopy can confirm concentric reduction throughout the arc. The elbow should remain stable under gentle valgus, varus, and rotational stress. If instability persists, further evaluation and potentially external fixation or supplementary repair are considered.
Closure
- The wound is irrigated thoroughly.
- The deep fascia is closed.
- Subcutaneous tissues are approximated, and the skin is closed with sutures or staples.
- A sterile dressing is applied, followed by a posterior splint with the elbow flexed to approximately 90 degrees and the forearm in neutral rotation to protect the repairs.
Complications & Management
Despite meticulous surgical technique, terrible triad injuries are associated with a high rate of complications due to their complex nature. Vigilant post-operative monitoring and timely intervention are critical.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Typical Incidence (Approximate) | Salvage Strategies / Management |
|---|---|---|
| Elbow Stiffness / Loss of Motion | 20-50% (most common) |
- Aggressive physical therapy, dynamic splinting.
- Manipulation under anesthesia (MUA) for acute stiffness. - Surgical arthrolysis (open or arthroscopic) for persistent stiffness after 6-12 months. - Removal of hardware if symptomatic and not contributing to stability. |
| Persistent Instability / Redislocation | 5-20% |
- Revision LUCL reconstruction.
- Revision coronoid fixation/reconstruction. - Revision radial head arthroplasty. - Dynamic external fixation. - Total elbow arthroplasty (TEA) in severe, recurrent, or chronic cases with poor bone stock. |
| Heterotopic Ossification (HO) | 10-30% |
- Prophylaxis: Indomethacin (for 3-6 weeks post-op) or radiation therapy (single dose within 24-72 hours).
- Surgical excision after maturation (typically 6-12 months post-onset) if functionally limiting. |
| Post-traumatic Arthritis | 10-25% (long-term) |
- Non-operative management (NSAIDs, activity modification, injections).
- Arthroscopic debridement. - Interposition arthroplasty. - Distraction arthroplasty. - Total elbow arthroplasty for severe end-stage disease. |
| Ulnar Neuropathy | 5-15% |
- Initial non-operative management (padding, observation).
- Nerve decompression (in situ release or anterior transposition) if symptoms persist or worsen. Prophylactic transposition may be considered if a medial approach was used or the nerve is at risk. |
| Infection | 1-5% |
- Superficial: Oral antibiotics, local wound care.
- Deep: Surgical debridement, intravenous antibiotics (typically 6 weeks), implant retention vs. removal (if stable or non-union). - Two-stage revision if infection persists. |
| Nonunion / Malunion |
Radial Head: 2-5%
Coronoid: Rare |
- Radial Head: Revision ORIF, radial head arthroplasty.
- Coronoid: Revision fixation, bone grafting. |
| Implant-Related Issues | 5-10% |
- Symptomatic hardware (e.g., prominence, loosening): Removal after bone healing and stability are achieved.
- Radial head implant subsidence or loosening: Revision arthroplasty. |
| Compartment Syndrome | <1% | - Urgent fasciotomy. |
| Neurovascular Injury (Acute) | <1% | - Immediate surgical exploration and repair of injured vessels/nerves. |
General Management Principles for Complications
- Early Detection: Regular clinical follow-up and radiographic assessment are crucial to identify complications promptly.
- Individualized Approach: Treatment must be tailored to the specific complication, its severity, patient factors, and functional demands.
- Multidisciplinary Care: Involvement of physical therapists, pain management specialists, and potentially neurologists can optimize outcomes.
- Patient Counseling: Patients should be thoroughly informed pre-operatively about the potential for complications and the prolonged recovery associated with terrible triad injuries.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a cornerstone of successful terrible triad injury management. It is a carefully phased process, balancing protection of the surgical repairs with early, controlled motion to prevent stiffness and restore function. Collaboration with an experienced hand and elbow therapist is essential.
General Principles
- Protection: Safeguard the surgical repairs from excessive stress or uncontrolled movements.
- Early Motion: Initiate controlled range of motion as soon as possible to prevent adhesion formation and stiffness.
- Gradual Progression: Systematically increase the intensity of exercises and activities based on healing and stability.
- Pain Management: Optimize pain control to facilitate participation in therapy.
Phases of Rehabilitation
Phase 1: Protective Phase (Weeks 0-6)
Goals:
* Control pain and swelling.
* Protect surgical repairs.
* Initiate gentle, controlled range of motion.
Protocol:
*
Immobilization:
* Initially, a hinged elbow brace or posterior splint is applied, locking the elbow at 90 degrees of flexion with the forearm in neutral or pronation (to protect the LUCL repair). The duration of initial immobilization varies (typically 1-2 weeks), depending on intra-operative stability.
* Transition to a hinged elbow brace within 1-2 weeks, which allows controlled motion while providing protection against varus/valgus and rotational stresses.
*
Range of Motion (ROM):
*
Active-assisted and gentle passive ROM:
Initiated within the first few days to a week. The brace's range of motion is progressively increased, typically advancing 10-15 degrees per week, aiming for a stable arc of motion (e.g., 30-130 degrees flexion/extension).
*
Forearm Rotation:
Gentle pronation/supination within comfort and stability limits, often favoring pronation initially to protect the LUCL.
*
Avoidance:
Absolutely no sudden or uncontrolled movements, no lifting, pushing, or pulling, especially overhead or with heavy loads. Avoid passive overpressure, particularly into extension or varus/valgus stress.
*
Non-weight-bearing:
The affected extremity remains non-weight-bearing.
*
Hand/Wrist/Shoulder ROM:
Encourage active range of motion for these joints to prevent stiffness.
*
Modalities:
Ice, elevation, gentle massage for swelling.
Phase 2: Intermediate Phase (Weeks 6-12)
Goals:
* Gradually increase elbow ROM.
* Begin gentle strengthening.
* Improve muscle endurance.
Protocol:
*
Brace Weaning:
* Continue hinged brace, but progressively unlock ROM to full tolerance.
* Gradual weaning from the brace for activities of daily living (ADLs) as stability improves, usually around 8-10 weeks. May continue to wear the brace for heavier activities or sleep.
*
Range of Motion:
* Continue active and active-assisted ROM exercises, working towards full flexion and extension.
* Gentle self-stretching techniques are introduced (e.g., sustained passive stretches).
*
Strengthening:
* Initiate gentle isometric exercises for elbow flexors, extensors, pronators, and supinators.
* Progress to light resistance exercises with elastic bands or light weights (e.g., 1-2 lbs).
* Focus on control and smooth movements, avoiding ballistic motions.
*
Functional Activities:
Begin light, non-impact ADLs.
Phase 3: Advanced Strengthening & Return to Activity (Weeks 12-24+)
Goals:
* Restore full strength, endurance, and power.
* Regain full functional use of the arm.
* Prepare for return to sport or demanding work activities.
Protocol:
*
Strengthening:
* Progress to moderate to heavy resistance exercises, including concentric and eccentric training.
* Incorporate functional and sport-specific exercises (e.g., throwing mechanics, overhead activities, lifting simulations).
* Proprioceptive and neuromuscular control drills.
*
Endurance:
Increase repetitions and duration of activities.
*
Return to Activity:
* Gradual return to light recreational activities.
* Return to sport or heavy labor is individualized and typically not before 6 months, often longer, contingent upon objective strength and functional assessments (e.g., isokinetic testing). Full return to contact sports or heavy overhead work may take 9-12 months.
*
Long-term Monitoring:
Patients should be advised that full recovery can take up to 1-2 years, and they may experience some residual stiffness or intermittent pain, particularly with weather changes or overuse.
Key Considerations for Rehabilitation
- Individualization: Each patient's protocol must be individualized based on the specific injury, surgical repairs, intra-operative stability, and patient's progress.
- Pain as a Guide: Pain should generally not be pushed through. Any sharp increase in pain, swelling, or loss of ROM should prompt re-evaluation.
- Communication: Close communication between the surgeon, therapist, and patient is paramount to prevent complications and optimize recovery.
- Risk of HO: Monitor for signs of heterotopic ossification and implement appropriate management if detected.
Summary of Key Literature / Guidelines
The terrible triad injury remains a challenging entity in orthopedic surgery, with ongoing research refining diagnostic and treatment paradigms. Key literature and guidelines emphasize the principles of anatomic reduction, stable fixation, and early motion.
1. Anatomic Reduction and Stable Fixation of All Three Components:
* Early studies by
Hotchkiss, Morrey, and Jupiter
highlighted the importance of addressing the radial head and coronoid fractures, alongside ligamentous repair, for stable elbow function. The concept of the "circulus vitiosus" emphasizes that failure to stabilize one component compromises the entire construct.
* The
O'Driscoll classification
for coronoid fractures (tip, anteromedial, basal) and
Mason-Hotchkiss classification
for radial head fractures guide surgical decision-making regarding fragment fixation or replacement. Anteromedial coronoid fractures, even small, are increasingly recognized as critically important for stability due to their role as an anterior buttress and attachment site for the MCL.
*
Radial head replacement
has largely supplanted excision for unreconstructible fractures in TTI, as it restores important axial and valgus stability, reducing the risk of late instability and arthrosis. Monoblock metal implants or pyrocarbon implants are commonly used.
2. Surgical Sequence:
* Consensus generally supports a sequential approach:
Coronoid first, then radial head, then LUCL.
This order rebuilds the primary bony buttress, restores radial length and stability, and finally reconstructs the lateral soft tissue restraints. Some surgeons advocate for LUCL repair immediately after coronoid stabilization, followed by radial head.
* The need for
MCL repair
in TTI is debated. While typically not primarily injured, if gross valgus instability persists after all lateral structures and the coronoid are addressed, then MCL repair through a separate medial incision is indicated.
3. Rehabilitation:
*
Early, controlled range of motion
is universally advocated to prevent stiffness, but always balanced against the stability achieved intra-operatively. Protocols vary in the exact timing of brace unlocking and motion limits, but the principle of gradual progression is constant.
* Concerns regarding the impact of early motion on LUCL repair have led to strategies like initial pronation and limited early extension, or even the use of an external fixator as a temporary "internal brace" in very unstable cases, though the latter is less common for routine TTI.
4. Complication Rates:
* Literature consistently reports high complication rates, with
stiffness and heterotopic ossification (HO)
being the most common. Prophylaxis for HO (NSAIDs or radiation) is often recommended.
* Persistent instability and post-traumatic arthritis remain significant long-term challenges, underscoring the need for meticulous surgical technique and comprehensive rehabilitation.
5. Future Directions:
* Ongoing research focuses on improved implant designs for radial head and coronoid fractures, advanced techniques for ligamentous reconstruction, better methods for assessing intra-operative stability, and refined rehabilitation protocols to minimize complications and optimize long-term functional outcomes. The role of arthroscopy in acute TTI management is also an evolving area.
In summary, the terrible triad injury demands a high level of surgical expertise and a systematic, comprehensive approach. Adherence to established principles of anatomic reduction, stable fixation of all injured components, and a structured rehabilitation protocol provides the best chance for a favorable outcome, though the potential for complications remains substantial. Continued vigilance and patient education throughout the recovery journey are paramount.
You Might Also Like