Sternoclavicular Joint Injury: A Comprehensive Academic Review of Epidemiology, Anatomy, and Biomechanics
Key Takeaway
Sternoclavicular (SC) joint injuries are rare yet critical shoulder girdle traumas, typically resulting from high-energy incidents. The SC joint, the sole bony link between the upper limb and axial skeleton, relies primarily on complex ligamentous stabilizers. Posterior dislocations are particularly concerning due to potential mediastinal compression, necessitating precise diagnosis and meticulous management for optimal outcomes.
Sternoclavicular Joint Injury: Essential Guide to Diagnosis & Care
Introduction & Epidemiology
Injuries to the sternoclavicular (SC) joint, while often overlooked due to their rarity, represent a critical subset of shoulder girdle trauma that demands precise diagnosis and meticulous management. As the only true articulation connecting the upper extremity to the axial skeleton, the SC joint's integrity is paramount for normal shoulder function and, in specific injury patterns, for the preservation of vital mediastinal structures.
Epidemiological data underscore the infrequency of these injuries. Cave et al. notably reported that among 1,603 shoulder girdle dislocations, only 3% involved the SC joint, contrasting sharply with the 85% glenohumeral and 12% acromioclavicular (AC) dislocations observed. This low incidence rate, approximately 1% of all dislocations, often leads to delayed or missed diagnoses, particularly in polytrauma settings where more obvious injuries may overshadow subtle SC joint pathology. Despite their rarity, these injuries carry significant potential for morbidity due to their anatomical proximity to critical neurovascular and visceral structures within the thoracic inlet.
The etiology of SC joint dislocations is predominantly high-energy trauma. Approximately 80% of these injuries are attributed to either motor vehicle accidents (47%) or sports-related incidents (31%). Direct trauma to the anterior chest or shoulder can result in anterior dislocations, which are typically stable and less complex. Conversely, indirect forces, such as a blow to the posterolateral shoulder or a direct force to the anteromedial clavicle, can produce posterior dislocations. These posterior displacement injuries, while less common (occurring in about 25% of all SC joint dislocations), are of greater clinical concern given the significant risk of mediastinal compression and associated life-threatening complications. Understanding these mechanisms is crucial for anticipating injury patterns and performing a thorough clinical assessment.
Surgical Anatomy & Biomechanics
The sternoclavicular joint is a complex diarthrodial joint, classified as a saddle-type articulation, which provides the sole bony link between the upper limb and the trunk. This unique position facilitates a wide range of motion for the shoulder girdle, allowing for elevation, depression, protraction, retraction, and axial rotation of the clavicle.
Articular Surfaces:
The medial clavicle articulates with the manubrium of the sternum and the first costal cartilage. A distinctive feature is the significant incongruity of the articular surfaces: the articular surface of the clavicle is considerably larger and more convex than the smaller, reciprocally concave articular facet on the manubrium. Less than half of the medial clavicle articulates with the sternum at any given time. This inherent bony instability necessitates robust ligamentous support to maintain joint integrity, lending the SC joint the distinction of having the least amount of bony stability among the major joints of the body. Both articular surfaces are covered by fibrocartilage, contributing to shock absorption and joint mechanics.
Ligamentous Stabilizers:
The stability of the SC joint is primarily derived from its intricate ligamentous complex, rather than its bony congruity. These ligaments include:
-
Intra-articular Disc Ligament (Articular Disc): This crucial structure, composed of tough fibrocartilage, arises from the superior and posterior aspects of the medial clavicle and attaches inferiorly to the junction of the first rib and manubrium. It essentially divides the joint into two separate synovial cavities. Functionally, it acts as a hinge during clavicular motion, a vital shock absorber, and, most importantly, a primary checkrein against medial and superior displacement of the clavicle. Injuries to this disc can lead to chronic instability and pain.

-
Anterior and Posterior Sternoclavicular Ligaments: These strong, fibrous bands reinforce the joint capsule anteriorly and posteriorly, respectively. The anterior ligament is thicker and broader than the posterior, resisting anterior displacement of the clavicle. The posterior ligament is critical for preventing posterior displacement, and its integrity is paramount given the proximity of vital mediastinal structures.

-
Costoclavicular Ligament (Rhomboid Ligament): Located just lateral and inferior to the SC joint, this strong, bilaminar ligament extends from the inferior surface of the medial clavicle to the superior surface of the first rib and its costal cartilage. It serves as the primary static stabilizer of the SC joint, resisting superior and lateral displacement of the clavicle. It also limits excessive clavicular elevation and rotation. This ligament's integrity is often a key factor in determining the stability of SC joint injuries.
-
Interclavicular Ligament: Extending across the jugular notch, connecting the superior aspects of the medial ends of both clavicles and the manubrium, this ligament helps to limit superior displacement of the clavicle and provides indirect stability to the SC joints, especially during shoulder depression.
Biomechanics:
The SC joint permits movements in all three planes:
*
Elevation/Depression:
Approximately 30-40 degrees of elevation and 10 degrees of depression.
*
Protraction/Retraction:
Approximately 15-20 degrees in each direction.
*
Axial Rotation:
About 30-45 degrees of posterior rotation during arm elevation.
These motions are synchronized with movements at the glenohumeral and acromioclavicular joints to achieve the full range of shoulder motion. The ligaments constrain these movements, with the costoclavicular ligament being crucial for superior and lateral stability, and the anterior/posterior SC ligaments resisting anteroposterior translation. The articular disc, acting as a fulcrum, also facilitates smooth motion and absorbs compressive forces.
Neurovascular and Visceral Proximity:
A thorough understanding of the anatomical relationships posterior to the SC joint is paramount for any intervention. The posterior aspect of the joint is immediately adjacent to numerous critical structures within the superior mediastinum and thoracic inlet, including:
*
Vascular Structures:
Brachiocephalic (innominate) artery and vein, subclavian artery and vein, common carotid artery, internal jugular vein. The right brachiocephalic artery courses directly posterior to the right SC joint.
*
Visceral Structures:
Trachea, esophagus, pleura, apex of the lung.
*
Nerve Structures:
Phrenic nerve, vagus nerve, recurrent laryngeal nerve.
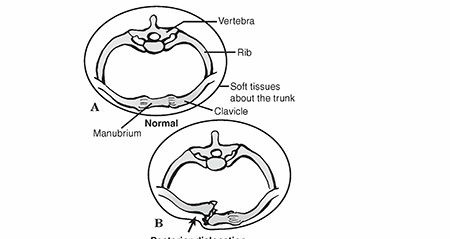
Posterior dislocation of the clavicle can directly compress or lacerate these vital structures, leading to potentially life-threatening complications such as superior vena cava syndrome, pneumothorax, tracheoesophageal injury, brachial plexus palsy, or massive hemorrhage. This intimate relationship dictates the urgency and surgical approach for posterior dislocations.
Indications & Contraindications
The decision-making process for managing sternoclavicular joint injuries hinges on the direction of dislocation, chronicity, associated injuries, and the patient's overall health status.
Non-Operative Indications
Non-operative management is the preferred initial approach for many SC joint injuries, particularly those that are stable or lack significant risk to vital structures.
- Grade I & II Sprains: These represent mild to moderate ligamentous injuries without complete dislocation. Rest, ice, sling immobilization for comfort, and gradual rehabilitation are typically effective.
-
Acute Anterior SC Joint Dislocations:
These are generally stable injuries with a low risk of neurovascular compromise. While cosmetically noticeable, they are often well-tolerated functionally. Management involves a period of sling immobilization (2-4 weeks), pain control, and a progressive rehabilitation program focusing on range of motion and strengthening. Closed reduction can be attempted but is often unstable and may not be maintained, and recurrent anterior subluxation or dislocation is common. Given the benign nature of anterior instability, operative intervention is rarely indicated unless there is persistent, debilitating pain and functional impairment refractory to conservative measures.

- Asymptomatic Chronic Instability: In cases of long-standing SC joint instability (anterior or posterior) that do not cause significant pain or functional limitation, conservative management focusing on periscapular strengthening and activity modification is appropriate.
- Patients with Significant Comorbidities: For patients with medical conditions that pose a high anesthetic or surgical risk, non-operative management may be chosen even for injuries that would typically warrant surgical intervention, provided there is no immediate life-threatening compromise.
Operative Indications
Operative intervention is reserved for specific SC joint injuries that pose risks to the patient, are irreducible, or result in persistent, debilitating symptoms after failed conservative treatment.
-
Acute Posterior SC Joint Dislocations:
This is widely considered an orthopedic emergency and an absolute indication for operative intervention (or at least an urgent attempt at closed reduction under controlled conditions). The immediate and significant risk of compression or laceration to vital mediastinal structures (trachea, esophagus, great vessels) mandates prompt reduction. While closed reduction can be attempted, it frequently fails or is unstable, necessitating open reduction.

- Irreducible Dislocations (Acute or Chronic): If closed reduction is unsuccessful, or if soft tissue interposition (e.g., intra-articular disc, posterior capsule, SCM muscle) prevents concentric reduction, open reduction is indicated. This applies to both anterior and posterior dislocations.
- Open SC Joint Dislocations: These are rare but require emergent surgical debridement and reduction to prevent infection and address associated soft tissue trauma.
- Associated Neurovascular or Visceral Compromise: Any evidence of vascular compromise (e.g., absent pulses, expanding hematoma), tracheal compression (stridor, dysphagia), esophageal injury, or neurological deficits warrants urgent surgical exploration and reduction, regardless of the direction of dislocation.
- Chronic, Painful SC Joint Instability (Anterior or Posterior): For patients who experience persistent, debilitating pain, functional limitation, or recurrent symptomatic subluxations/dislocations despite adequate non-operative management (typically 6-12 months of structured rehabilitation), surgical stabilization or reconstruction may be indicated.
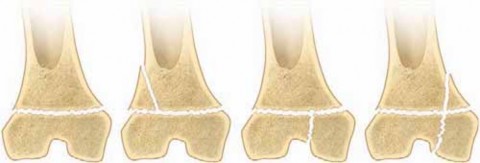
- Medial Clavicle Epiphyseal Fractures (Salter-Harris Type I or II): In adolescents, the medial clavicular physis remains open until age 20-25. These physeal injuries can mimic true SC joint dislocations but are anatomically distinct. While many are amenable to closed reduction, unstable or irreducible physeal separations often require open reduction and internal fixation, typically with bioabsorbable sutures to avoid physeal violation. Posterior displacement of the epiphysis carries the same risks as posterior dislocation of the joint.
Contraindications
Absolute contraindications to SC joint surgery are few and generally relate to the patient's inability to tolerate surgery or anesthesia.
- Acute Local Infection: Surgery through an infected field is contraindicated.
- Severe Overlying Skin Compromise: Extensive soft tissue injury, devitalized skin, or severe burns may necessitate delay or alternative strategies.
- Severe Uncontrolled Medical Comorbidities: Patients with unstable cardiac conditions, severe coagulopathies, or other life-threatening medical issues where the risk of surgery outweighs the benefits (unless immediate life-saving intervention is required).
Operative vs. Non-Operative Indications Summary
| Feature | Non-Operative Indications | Operative Indications |
|---|---|---|
| Dislocation Type | Acute Anterior SC Joint Dislocation | Acute Posterior SC Joint Dislocation (Emergency) |
| Grade I & II SC Joint Sprains | Irreducible SC Joint Dislocation (any direction) | |
| Open SC Joint Dislocation | ||
| Chronicity | Asymptomatic Chronic SC Joint Instability | Symptomatic Chronic SC Joint Instability (failed conservative) |
| Associated Factors | No associated neurovascular/visceral compromise | Associated Neurovascular/Visceral Compromise |
| Medial Clavicle Epiphyseal Fracture (unstable/irreducible/posterior) | ||
| Patient Status | Significant medical comorbidities precluding surgery (no acute threat) | Medically fit for surgery |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for SC joint surgery, particularly given the proximity to vital mediastinal structures.
Diagnosis & Imaging
-
Clinical Assessment:
A thorough history and physical examination are paramount.
- History: Mechanism of injury (direct vs. indirect force, anterior vs. posterior impact), time since injury, symptoms (pain, deformity, dyspnea, dysphagia, hoarseness, paresthesias).
- Inspection: Deformity (e.g., medial clavicle prominence anteriorly or palpable void posteriorly), swelling, ecchymosis, skin compromise.
- Palpation: Tenderness over the SC joint, displacement of the medial clavicle. For posterior dislocations, careful palpation may reveal a posterior void or, conversely, a lack of the normal bony prominence of the medial clavicle, which can be misleading due to muscle spasm and edema.
- Range of Motion: Pain with shoulder girdle movements.
- Neurovascular Assessment: Critical for posterior dislocations. Evaluate radial, ulnar, and brachial pulses bilaterally. Assess capillary refill, sensation, and motor function of the upper extremity. Look for signs of vascular compromise (pallor, coolness, decreased pulse).
- Pulmonary/Airway Assessment: Auscultate lung sounds, observe respiratory effort. Inquire about dyspnea, stridor, or dysphagia. A posterior dislocation can impinge on the trachea or esophagus.
-
Radiographic Evaluation:
- Standard Radiographs: Anteropoposterior (AP) view of the shoulder and chest may show gross displacement but can be difficult to interpret due to overlapping structures.
- Serendipity View: This specialized view, taken with the patient supine and the X-ray beam angled 40 degrees cephalad, helps differentiate between anterior and posterior dislocations by projecting the medial clavicle superior or inferior to the sternum. For a posterior dislocation, the affected clavicle will appear inferior to the contralateral clavicle on this view.
-
Oblique Views:
Can provide additional information but are often insufficient for definitive diagnosis.

-
Computed Tomography (CT) Scan with Intravenous Contrast:
This is the
gold standard
for diagnosing SC joint injuries, particularly posterior dislocations.
- Provides high-resolution axial and 3D reconstructions to precisely define the direction and degree of displacement.
- Crucially visualizes the relationship of the medial clavicle to the adjacent neurovascular structures (brachiocephalic vessels, subclavian vessels, carotid artery) and visceral structures (trachea, esophagus). This is essential for assessing the risk of compromise and planning surgical approach.
-
Helps identify associated fractures (clavicle, sternum, rib, first rib).


-
Magnetic Resonance Imaging (MRI):
While less frequently used for acute bony assessment, MRI is valuable for:
- Evaluating ligamentous and capsular integrity (e.g., articular disc tears, costoclavicular ligament injury).
- Assessing chronic SC joint pain or stress injuries.
- Differentiating between true SC joint dislocation and medial clavicular physeal injury in adolescents, which can appear similar on radiographs.
Pre-operative Workup
- Consultations: For posterior dislocations or suspected neurovascular compromise, consultation with vascular surgery, cardiothoracic surgery, or general surgery is imperative. Anesthesiology consultation is critical to discuss potential airway challenges and monitoring requirements.
- Blood Products: Type and cross-match blood should be readily available, especially for posterior dislocations, due to the risk of significant hemorrhage.
- Informed Consent: Detailed discussion with the patient regarding the nature of the injury, operative risks (including damage to vital structures, recurrent instability, chronic pain, infection), potential need for sternotomy or vascular repair, and expected recovery.
- Emergency Planning: For posterior dislocations, the operating room should be prepared for potential emergent thoracotomy or sternotomy.
Patient Positioning
- Supine Position: The patient is positioned supine on a radiolucent operating table.
- Shoulder Roll: A rolled blanket or specialty bolster is placed longitudinally between the scapulae, allowing the shoulders to fall back and the thoracic inlet to hyperextend. This improves exposure of the SC joint and provides counter-traction for reduction maneuvers.
- Arm Positioning: The ipsilateral arm should be draped free to allow for manipulation during reduction.
- Head Position: The head is typically turned slightly away from the operative side.
- C-arm Access: Ensure unrestricted fluoroscopy access for intraoperative imaging to confirm reduction and fixation.
- Surgical Prep: Wide sterile preparation from the jaw to the umbilicus, extending laterally to the mid-axillary lines, anticipating potential extension of the incision or need for sternotomy/thoracotomy. Both sides of the chest should be prepped and draped for potential access to the contralateral subclavian vein for central line placement, if needed.
- Pressure Monitoring: Arterial line placement is often prudent for continuous blood pressure monitoring, especially when vascular compromise is a concern.
Detailed Surgical Approach / Technique
The surgical management of SC joint injuries is primarily dictated by the direction of dislocation, its chronicity, and the presence of associated neurovascular compromise. Acute posterior dislocations represent an orthopedic emergency requiring immediate attention.
Surgical Approach
-
Incision:
A curvilinear or transverse skin incision is made directly over the affected sternoclavicular joint, centered on the deformity. The incision typically extends 5-8 cm, medial to the midline of the sternum and lateral along the clavicle. A transverse incision provides excellent cosmetic results and can be extended if necessary.

- Subplatysmal Flaps: Subcutaneous dissection proceeds, raising superior and inferior subplatysmal flaps to provide adequate exposure. Care must be taken to identify and protect the supraclavicular nerves to avoid post-operative dysesthesia.
- Muscle Dissection: The sternal head of the sternocleidomastoid (SCM) muscle may be partially detached from its sternal origin or retracted laterally to expose the joint capsule. Complete detachment should be avoided if possible, but if necessary, it must be meticulously repaired at closure. The pectoralis major muscle may also require partial detachment for inferior exposure.
- Joint Capsule Exposure: The anterior sternoclavicular ligament and joint capsule are visualized. For posterior dislocations, the medial clavicle will be displaced posteriorly, often creating a palpable void anteriorly.
-
Protection of Posterior Structures:
This is the single most critical step, especially for posterior dislocations. Blunt dissection is carefully performed along the posterior aspect of the clavicle and sternum to the retrosternal space. A vascular surgeon or cardiothoracic surgeon should be available. A finger or a blunt instrument (e.g., a curved malleable retractor or a right-angle clamp) is gently passed behind the medial clavicle and into the mediastinum to protect the great vessels, trachea, and esophagus during reduction maneuvers. This maneuver must be performed with extreme caution.

Reduction (Acute Posterior Dislocation)
-
Closed Reduction Maneuvers: For acute posterior dislocations, a trial of closed reduction under general anesthesia is often performed first.
- Traction-Extension Technique: With the patient supine and a shoulder roll in place, an assistant provides counter-traction to the trunk. The surgeon or assistant grasps the ipsilateral arm and applies longitudinal traction and abduction/extension of the shoulder. A sterile towel clip or a sterile, wrapped hand can be used to grasp the posterior aspect of the medial clavicle to lever it anteriorly. The adduction and external rotation of the humerus can also provide a levering force.
- "Figure-of-Four" Maneuver: This involves the surgeon placing their knee or fist in the patient's ipsilateral axilla for leverage, while simultaneously applying downward and backward pressure on the shoulder to lift the clavicle anteriorly.
- Anesthesiologist Awareness: The anesthesiologist must monitor for any signs of airway compromise (e.g., stridor, desaturation) during reduction attempts, as the dislocated clavicle may momentarily or persistently impinge the trachea.
-
Open Reduction: If closed reduction fails, or for complex/chronic cases, open reduction is performed.
- The medial clavicle is directly visualized.
- Any soft tissue interposition (e.g., posterior capsule, intra-articular disc, SCM muscle) preventing reduction is identified and carefully removed or repositioned.
- Using bone hooks, reduction clamps, or a towel clamp placed anteriorly on the medial clavicle (with posterior protection), the clavicle is levered anteriorly into its anatomical position. Care must be taken to ensure the posterior wall of the capsule is not incarcerated in the joint.
Stabilization/Reconstruction
Once reduced, the SC joint often requires stabilization, particularly for posterior dislocations, chronic instability, or if the primary stabilizers are severely compromised. Direct repair of the anterior and posterior capsules and ligaments is attempted whenever possible.

-
Suture-Based Reconstruction (Ligamentous Repair/Augmentation): This is the most common and biomechanically sound method, aiming to recreate the function of the costoclavicular ligament.
- Graft Options: Autografts (e.g., semitendinosus, palmaris longus) or allografts are commonly used.
-
Technique (e.g., "Figure-of-Eight" Reconstruction):
- Tunnels are drilled in the medial clavicle (typically two, from anterior to posterior, avoiding the physis in adolescents).
- A tunnel is drilled in the first rib (or adjacent sternum), medial and inferior to the SC joint.
- The graft is passed through these tunnels in a figure-of-eight or double-bundle configuration to reconstruct the costoclavicular ligament and/or reinforce the sternoclavicular ligaments.
-
The graft is then tensioned with the arm in a neutral position (or slight abduction/extension) to restore normal joint kinematics and stability, then secured with sutures, interference screws, or buttons.


- Intra-articular Disc Repair: If the articular disc is torn or avulsed and still viable, it can be repaired back to the capsule or periosteum. However, severe disc damage often necessitates partial or complete resection if it impedes reduction or contributes to chronic pain.
-
Internal Bracing: The use of high-strength sutures or tapes (e.g., FiberTape®) to augment primary ligament repair has gained traction. These tapes provide immediate strength and allow for earlier, more aggressive rehabilitation, acting as an internal brace while biological healing occurs.
-
K-wires/Pins: Traditionally, transarticular K-wire or Steinman pin fixation was used but is now largely contraindicated as a sole fixation method due to a high risk of catastrophic migration into the mediastinum, heart, or great vessels. If used, they must be supplemented with robust soft tissue repair and removed early. They may be acceptable for temporary stabilization during surgery or for open physeal injuries with strict caveats.
-
Plate Fixation: Rarely used for pure dislocations due to poor bone quality at the sternal attachment point. May be considered for associated sternal or clavicular fractures that contribute to instability, but careful consideration of hardware prominence and irritation is needed.
Specific Considerations for Medial Clavicle Physeal Injuries
In adolescents, medial clavicle physeal fractures (Salter-Harris type I or II) are more common than true SC joint dislocations, often misdiagnosed as posterior dislocations.
*
Imaging:
CT scan is crucial to differentiate.
*
Reduction:
Most can be reduced closed. If closed reduction fails or for unstable posterior displacement, open reduction is indicated.
*
Fixation:
Physeal-sparing techniques are paramount. Suture repair of the periosteal sleeve (which often remains attached to the sternum) is usually sufficient. K-wires across the physis should be avoided unless absolutely necessary, and if used, should be smooth, placed in a non-compressing fashion, and removed as early as possible.
Closure
After reduction and stabilization, the SCM muscle (if detached) is repaired. The platysma is closed in layers, followed by meticulous skin closure. A drain may be placed if significant dead space or bleeding is encountered.
Complications & Management
Sternoclavicular joint injuries and their surgical management are associated with a range of potential complications, some of which can be life-threatening. A thorough understanding of these risks and their management is crucial.
Intraoperative Complications
| Complication | Incidence / Risk Factors | Salvage Strategies / Management |
|---|---|---|
| Neurovascular Injury | Primarily with posterior dislocations; up to 25% of cases. Risk to brachiocephalic vessels, subclavian vessels, common carotid, internal jugular vein, phrenic/vagus nerve, recurrent laryngeal nerve. | Immediate recognition, direct compression to control bleeding. Emergent vascular/thoracic surgery consultation and repair (e.g., vessel repair/ligation, nerve repair if possible). Intraoperative imaging (angiography). |
| Tracheal/Esophageal Injury | Rare, but highly morbid with posterior dislocations. | Immediate recognition (air/fluid leak, aspiration). Emergent cardiothoracic/general surgery consultation for repair. Airway management (intubation, tracheostomy). Nasogastric tube insertion. |
| Pneumothorax | Risk during posterior dissection or trauma to lung apex. | Immediate chest tube insertion. Intraoperative vigilance (anesthesiologist monitoring airway pressures, breath sounds). |
| Airway Compromise during Reduction | Due to direct tracheal compression by dislocated clavicle. | Prompt recognition by anesthesiologist (stridor, difficulty ventilating, desaturation). Immediate cessation of reduction attempt. If persistent, open reduction or emergent airway intervention (intubation, possibly tracheostomy). |
| Fracture (Clavicle, Sternum, Rib) | Result of trauma or iatrogenic during reduction/fixation. | Intraoperative imaging to confirm. Address associated fracture (e.g., small plate, tension band, non-operative for stable rib fracture). May necessitate changes in stabilization strategy. |
| Irreducible Dislocation | Due to soft tissue interposition (e.g., disc, SCM, capsule). | Identify and release entrapped structures. Careful open reduction with protection of posterior structures. Consider alternative reduction techniques or fixation methods. |
Early Postoperative Complications
| Complication | Incidence / Risk Factors | Salvage Strategies / Management |
|---|---|---|
| Infection | General surgical risk (~1-5%). Increased risk with open injuries or compromised tissues. | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics, irrigation, possible hardware removal (after soft tissue healing, if stable). |
| Hematoma/Seroma | Risk of bleeding into dead space; lymph accumulation. | Small: Observation, compression. Large/Symptomatic: Aspiration (sterile, guided) or surgical drainage. |
| Persistent Instability/Redislocation | Inadequate reduction, insufficient fixation, premature rehabilitation, severe ligamentous damage. | Assess clinically and with imaging (CT). Revision surgery with more robust reconstruction (e.g., stronger graft, different technique), prolonged immobilization. |
| Pneumothorax (delayed) | Can present hours to days post-op from iatrogenic injury. | Clinical signs (dyspnea, chest pain, decreased breath sounds) and chest X-ray. Chest tube insertion. |
| Wound Dehiscence | Poor wound healing, excessive tension, infection. | Local wound care, possible re-closure, management of underlying infection. |
Late Postoperative Complications
| Complication | Incidence / Risk Factors | Salvage Strategies / Management |
|---|---|---|
| Chronic Pain | Often due to residual instability, post-traumatic arthritis, nerve irritation, or failed reconstruction. | Comprehensive pain management (physical therapy, NSAIDs, injections). Revision surgery if instability is a primary driver. Consider medial clavicle resection arthroplasty for isolated painful post-traumatic arthritis (uncommon due to non-weight bearing nature). |
| Stiffness/Limited ROM | Prolonged immobilization, capsular fibrosis, inadequate rehabilitation. | Intensive physical therapy (passive/active ROM). Manipulation under anesthesia. Capsular release in severe, refractory cases. |
| Post-Traumatic Osteoarthritis | Common sequela, especially after intra-articular disc injury or chronic instability. | Conservative management (pain relief, activity modification). Medial clavicle resection arthroplasty (for severe, localized, debilitating pain after non-operative failures). |
| Hardware Failure/Migration | Applicable if pins/wires or other hardware are used. K-wire migration into mediastinum is well-documented and potentially fatal. | Immediate surgical removal of migrating hardware. For other hardware, removal if symptomatic. If instability recurs, revision with soft tissue reconstruction. Emphasize avoidance of transarticular K-wires. |
| Recurrent Instability | Similar to persistent instability; more common with anterior dislocations. | Comprehensive re-evaluation (clinical, CT, MRI). Revision surgery with robust ligament reconstruction (autograft/allograft) is often indicated if symptomatic. |
| Nonunion/Malunion (if associated fracture) | Inadequate fixation, biological factors. | Nonunion: Revision surgery with internal fixation and bone grafting. Malunion: Potentially symptomatic, requiring osteotomy or joint remodeling if function is significantly impaired. |
| Cosmetic Deformity | More common with anterior dislocations, even after reduction. | Counseling patients pre-operatively. May require plastic surgery consultation, but often well-tolerated if asymptomatic. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following sternoclavicular joint surgery is critical for optimizing outcomes, restoring function, and minimizing the risk of recurrence. Protocols must be tailored to the specific surgical procedure, the extent of the injury, and the patient's individual healing capacity and goals. The primary goals are to protect the repair, gradually restore range of motion, regain strength, and facilitate a safe return to activity.
Phase I: Protection and Early Motion (Weeks 0-6)
-
Goals:
- Protect the surgical repair/reconstruction.
- Control pain and swelling.
- Prevent stiffness in uninvolved joints.
- Initiate gentle scapular mobility.
-
Immobilization:
- Sling: The arm is typically immobilized in a sling for 2-4 weeks, or longer (up to 6 weeks) for more extensive reconstructions or high-risk patients. The sling provides comfort and prevents unwanted movements.
- Avoidance: Strict avoidance of active or passive shoulder abduction and external rotation beyond neutral, and horizontal extension, which can place stress on the healing SC joint.
-
Exercises:
- Elbow, Wrist, Hand ROM: Active range of motion exercises for the elbow, wrist, and hand are initiated immediately to prevent stiffness and maintain circulation.
- Gentle Passive/Assisted Shoulder ROM (pendulums): Pendulum exercises can be started as early as day 1 post-op, emphasizing gravity-assisted motion without active muscle contraction of the shoulder girdle.
- Scapular Mobilization: Gentle scapular retraction and protraction exercises (e.g., "scapular clocks") are started, ensuring these movements are controlled and do not stress the SC joint.
- Isometric Exercises (Submaximal): Light, submaximal isometric contractions of the shoulder muscles (e.g., deltoid, rotator cuff) can be initiated cautiously, only if pain-free and without stressing the SC joint.
-
Activity Restrictions:
- No lifting, pushing, or pulling with the affected arm.
- No weight-bearing on the affected arm.
- Avoidance of activities that stress the SC joint (e.g., reaching overhead, reaching across the body).
- Maintain good posture.
Phase II: Progressive Strengthening and Range of Motion (Weeks 6-12)
-
Goals:
- Gradually restore full, pain-free range of motion.
- Initiate progressive strengthening of the shoulder girdle.
- Improve neuromuscular control.
-
Immobilization:
- Sling is discontinued as comfort and control allow, typically around 4-6 weeks post-op.
-
Exercises:
- Active Assisted Range of Motion (AAROM) to Active Range of Motion (AROM): Progress from AAROM (e.g., using a wand or pulley system) to full AROM as tolerated, gradually increasing the arcs of motion. Emphasis on elevation, flexion, and rotation.
-
Isotonic Strengthening (Light Resistance):
Begin with light resistance exercises using elastic bands or very light weights. Focus on rotator cuff, deltoid, and scapular stabilizer muscles.
- Internal/external rotation with arm adducted.
- Scapular retraction (e.g., rows).
- Shoulder flexion and abduction in pain-free ranges.
- Core Stability: Continue and advance core strengthening exercises to provide a stable base for upper extremity movements.
- Proprioceptive Exercises: Initiate balance and proprioception drills for the shoulder.
-
Activity Restrictions:
- Continue to avoid heavy lifting and vigorous activities.
- No contact sports or activities involving forceful impact.
- Listen to pain and avoid movements that cause sharp discomfort.
Phase III: Advanced Strengthening and Return to Activity (Weeks 12+)
-
Goals:
- Maximize strength, power, and endurance.
- Refine neuromuscular control and proprioception.
- Gradual and safe return to sport-specific or activity-specific demands.
-
Exercises:
- Progressive Resistance Training: Advance to heavier weights and more challenging resistance exercises.
-
Functional and Sport-Specific Training:
- Plyometric exercises for the upper extremity (e.g., medicine ball throws).
- Throwing programs (for athletes).
- Overhead drills.
- Gradual simulation of work or sport activities.
- High-Intensity Proprioception: Incorporate unstable surface training and reaction drills.
- Endurance Training: Continue general cardiovascular fitness.
-
Return to Activity:
- A gradual return to full, unrestricted activities, including contact sports, is typically allowed no earlier than 4-6 months post-surgery, and often longer (6-9 months) for high-demand athletes or those with extensive reconstructions.
- Return criteria include full, pain-free range of motion, near-normal strength, excellent neuromuscular control, and absence of apprehension or instability.
- The decision to return to sport should be individualized and based on objective functional testing.
Important Considerations:
*
Patient Compliance:
Adherence to the protocol is crucial. Overaggressive rehabilitation can jeopardize the repair, while under-activity can lead to stiffness.
*
Pain as a Guide:
Pain should always be respected as a warning sign.
*
Individualization:
Protocols must be adapted based on surgical findings (e.g., extent of ligament damage, graft used), patient age, and activity level.
*
Long-Term Follow-up:
Continued monitoring for signs of chronic instability or post-traumatic arthritis.
Summary of Key Literature / Guidelines
The body of literature on sternoclavicular joint injuries, while not as extensive as for other shoulder girdle pathologies, provides critical insights and guiding principles for contemporary management.
-
Rarity and Diagnostic Challenges: The seminal work by Cave et al. (1987) on the epidemiology of shoulder girdle dislocations highlighted the rarity of SC joint injuries (3%), setting the stage for understanding their diagnostic challenges. Subsequent studies consistently confirm this low incidence, emphasizing the need for a high index of suspicion. Current guidelines advocate for CT imaging as the diagnostic gold standard for evaluating SC joint injuries, particularly for posterior dislocations, to accurately assess displacement and relation to mediastinal structures. MRI is increasingly utilized for soft tissue and ligamentous assessment, especially in chronic cases or for differentiating physeal injuries in adolescents.
-
Posterior Dislocations: An Emergency: There is a strong consensus across orthopedic literature that acute posterior sternoclavicular dislocations represent a true orthopedic emergency . Studies consistently report the potential for life-threatening complications, including compression or laceration of the trachea, esophagus, and great vessels (e.g., brachiocephalic artery/vein, subclavian artery/vein). Prompt closed or open reduction is paramount. The presence of vascular or thoracic surgeons for posterior dislocation reduction and potential repair is a widely accepted recommendation. While closed reduction techniques are often attempted first, the literature indicates a high failure rate or instability, often necessitating open reduction.
-
Treatment of Anterior Dislocations: For acute anterior SC joint dislocations, non-operative management with sling immobilization and rehabilitation is generally considered the first-line treatment. Surgical intervention for acute anterior dislocations is rarely indicated unless there is significant pain, persistent instability interfering with function, or failure of conservative management. The literature reports high rates of recurrent anterior subluxation or dislocation after closed reduction, but most patients remain functionally asymptomatic.
-
Surgical Stabilization Techniques:
- Transarticular K-wires/Pins: Historical literature frequently described the use of transarticular K-wires or pins for stabilization. However, there are numerous case reports and systematic reviews documenting catastrophic complications, including pin migration into the heart, aorta, or mediastinum, leading to death or severe morbidity. Consequently, the use of transarticular K-wires as sole fixation is now widely contraindicated in adult SC joint reconstruction, except in very specific, highly controlled temporary situations or for physeal injuries with strict caveats.
- Ligamentous Reconstruction: Current literature strongly supports suture-based techniques, often utilizing autograft (e.g., semitendinosus, palmaris longus) or allograft, for robust ligamentous reconstruction. The aim is to reconstruct the damaged costoclavicular and sternoclavicular ligaments, recreating the joint's intrinsic stability. Biomechanical studies have demonstrated the superior strength and stability afforded by these techniques, particularly when mimicking the anatomical course of the costoclavicular ligament. Techniques like the figure-of-eight or double-bundle reconstruction are commonly reported with good long-term outcomes for both acute and chronic instability.
- Medial Clavicle Physeal Fractures: In adolescents (under 25 years old), injuries mimicking SC joint dislocations are often Salter-Harris type I or II physeal separations. The literature emphasizes physeal-sparing open reduction and suture-based repair of the periosteal sleeve as the preferred method for unstable or irreducible cases. This avoids disrupting the growth plate and minimizing the risk of growth arrest.
-
Outcomes and Complications:
- Outcomes: Good to excellent outcomes are reported for both anterior and posterior dislocations treated appropriately. Functional outcomes after surgical reconstruction for posterior dislocations tend to be favorable, although some patients may experience residual stiffness or mild pain. For anterior dislocations, persistent instability is common but often asymptomatic.
- Complications: Beyond the immediate life-threatening complications of posterior dislocations, other documented complications include chronic pain, post-traumatic osteoarthritis, recurrent instability, infection, and hardware-related issues. The overall complication rate for SC joint surgery is not insignificant, underscoring the need for careful patient selection and meticulous surgical technique.
-
Rehabilitation: While specific detailed protocols vary, the overarching theme in the literature is a structured, progressive rehabilitation program emphasizing protection in the early phase, followed by gradual restoration of range of motion and progressive strengthening. Return to high-impact activities or sports is typically delayed for 4-6 months or more, depending on the severity of the injury and reconstruction method, to allow for adequate biological healing and graft maturation.
In conclusion, the management of sternoclavicular joint injuries has evolved significantly, with a clear shift towards aggressive management of posterior dislocations and a focus on anatomical soft tissue reconstruction techniques. Continued vigilance in diagnosis, precise surgical execution, and adherence to structured rehabilitation protocols remain the cornerstones for optimizing patient outcomes in these challenging cases.
Clinical & Radiographic Imaging



You Might Also Like