What Causes Femoral Fractures? Essential Guide & Prevention Tips
Key Takeaway
This article provides essential research regarding What Causes Femoral Fractures? Essential Guide & Prevention Tips. Femoral fractures causes typically include falls, especially in older adults with osteoporosis or other bone diseases. High-energy trauma, such as motor vehicle accidents or sports injuries, can also be a significant factor. Additionally, pathological conditions like bone tumors or infections are recognized causes of these fractures.
What Causes Femoral Fractures? Essential Guide & Prevention Tips
Introduction & Epidemiology
Proximal femoral fractures, commonly referred to as hip fractures, represent a significant orthopedic challenge, particularly within the geriatric population. These injuries involve the upper portion of the femur, encompassing the femoral head, neck, intertrochanteric region, and subtrochanteric shaft. Anatomically, these fractures are broadly categorized into intracapsular (femoral head, subcapital, transcervical, basicervical neck fractures) and extracapsular (intertrochanteric and subtrochanteric fractures), a distinction critical for understanding vascularity, healing potential, and treatment algorithms.
Epidemiologically, proximal femoral fractures are a global health concern, with an estimated 1.6 million occurrences annually worldwide, a number projected to reach 4.5 million by 2050. The incidence significantly increases with age, with the majority of fractures occurring in individuals over 65 years. Females are disproportionately affected, exhibiting a two to three times higher incidence than males, largely attributable to postmenopausal osteoporosis and longer life expectancy. The societal and economic burden is substantial, characterized by high morbidity (loss of independence, functional decline), mortality (up to 30% within one year post-fracture), and considerable healthcare costs associated with acute treatment, rehabilitation, and long-term care.
The most prevalent type of proximal femoral fracture is the intertrochanteric fracture, accounting for approximately 50% of all hip fractures, followed by femoral neck fractures (45%) and subtrochanteric fractures (5%). While falls from a standing height constitute the primary mechanism of injury in older adults with compromised bone quality (osteoporosis), high-energy trauma (e.g., motor vehicle collisions, significant falls, sports injuries) are common etiologies in younger patients. Pathological fractures, secondary to underlying conditions such as metastatic disease, primary bone tumors, or metabolic bone diseases, also contribute to the overall incidence. Additionally, periprosthetic fractures around existing hip arthroplasties are an increasingly recognized entity.
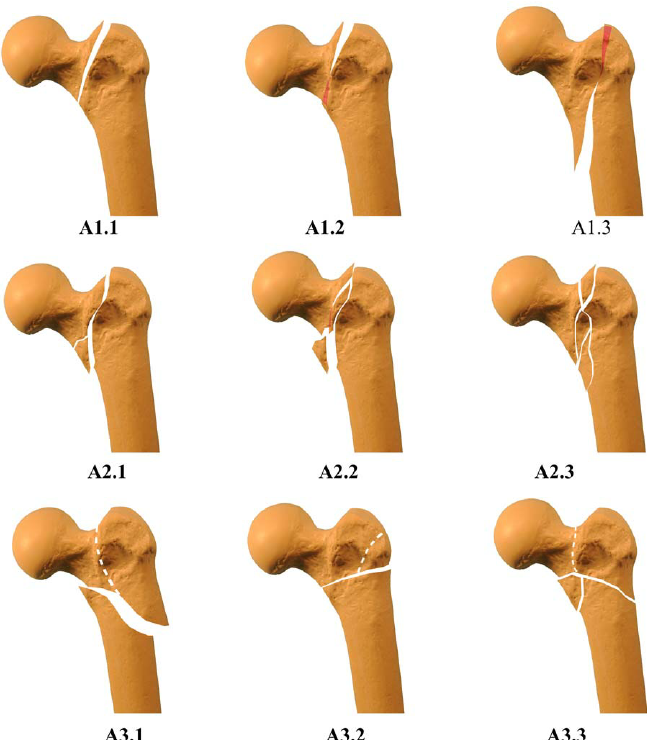
Classification systems, such as the AO/OTA (Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association) system, provide a standardized framework for describing fracture morphology, location, and severity, facilitating communication, guiding treatment, and predicting outcomes. Other specific classifications include Garden and Pauwels for femoral neck fractures, and Evans/Jensen for intertrochanteric fractures, each offering valuable insights into fracture stability and surgical planning.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the surgical anatomy and biomechanics of the proximal femur is paramount for effective fracture management.
Proximal Femoral Anatomy
The proximal femur comprises the femoral head, femoral neck, greater trochanter, lesser trochanter, and the subtrochanteric region.
*
Femoral Head:
Articulates with the acetabulum, forming a ball-and-socket joint. Its blood supply is critical and primarily derived from the medial and lateral circumflex femoral arteries via the retinacular vessels, with a minor contribution from the artery of the ligamentum teres (foveal artery), especially in pediatric patients. Disruption of these vessels, particularly in displaced intracapsular fractures, carries a high risk of avascular necrosis (AVN).
*
Femoral Neck:
Connects the head to the shaft, characterized by a complex trabecular pattern designed to withstand compressive and tensile forces. The angle of inclination (average 125-135 degrees) and angle of anteversion (average 10-15 degrees) are crucial for hip joint mechanics and gait. Fractures here disrupt the capsular attachment and often the retinacular vessels.
*
Greater Trochanter:
A large, quadrilateral eminence providing attachment for the gluteus medius, gluteus minimus, and piriformis muscles. Its integrity is vital for hip abductor function.
*
Lesser Trochanter:
A conical prominence on the posteromedial aspect of the femur, serving as the insertion point for the iliopsoas muscle. Displacement of this fragment indicates significant traction by the iliopsoas.
*
Intertrochanteric Region:
The area between the greater and lesser trochanters, forming the extracapsular base of the femoral neck. This region is rich in cancellous bone and has an excellent blood supply, contributing to high union rates, but often involves significant comminution.
*
Subtrochanteric Region:
Extends from the lesser trochanter distally for approximately 5 cm. This area is subjected to high stress due to significant muscle attachments (iliopsoas, glutei, adductors) and represents a stress riser, making fractures here prone to malunion and nonunion, especially with significant comminution or instability.
Neurovascular Relationships
Key neurovascular structures in proximity to the proximal femur include:
*
Femoral Artery/Vein/Nerve:
Located anteriorly, particularly vulnerable in direct anterior approaches or extensive anterior dissection.
*
Sciatic Nerve:
Courses posteriorly, at risk during posterior hip approaches or in cases of posterior fracture dislocation.
*
Lateral Femoral Cutaneous Nerve:
Superficial, susceptible to iatrogenic injury during lateral approaches, leading to meralgia paresthetica.
*
Obturator Nerve:
Medially, generally protected but relevant in pelvic reconstruction.
Biomechanics of Fracture
The biomechanics of proximal femoral fractures are dictated by bone quality, mechanism of injury, and muscle forces.
*
Bone Quality:
Osteoporosis drastically reduces bone mineral density and architectural integrity, lowering the fracture threshold. Trabecular bone in the femoral neck and intertrochanteric region is particularly vulnerable.
*
Mechanism of Injury:
*
Falls:
Low-energy falls, common in the elderly, often result in torsional or direct impact forces on the greater trochanter, leading to intertrochanteric or femoral neck fractures. The impact force combined with rotational stresses (e.g., foot fixed while body rotates) can initiate fracture.
*
High-Energy Trauma:
In younger patients, significant forces (axial load, bending, torsion) from motor vehicle accidents or direct trauma can cause complex femoral head, neck, or subtrochanteric fractures.
*
Pathological Fractures:
Result from weakened bone due to tumors (primary or metastatic), infections, or metabolic diseases, where normal physiological stresses lead to fracture.
*
Muscle Deforming Forces:
*
Iliopsoas:
Pulls the lesser trochanter fragment anteriorly and proximally.
*
Gluteus Medius/Minimus:
Abduct and externally rotate the proximal fragment.
*
Adductors:
Pull the distal fragment medially.
*
Hamstrings/Quadriceps:
Exert axial traction and rotational forces on the distal fragment.
Understanding these forces is critical for achieving and maintaining reduction.
Indications & Contraindications
Management of proximal femoral fractures varies significantly based on fracture location, displacement, patient age, bone quality, and physiological status. Surgical intervention is the standard of care for the vast majority of these fractures, with non-operative management reserved for specific circumstances.
Operative Indications
-
Displaced Femoral Neck Fractures:
- Younger Patients (<60-65 years): Urgent anatomical reduction and internal fixation to preserve the femoral head (cannulated screws, dynamic hip screw). Risk of AVN is high, but head preservation is prioritized.
- Elderly, Active Patients: Hemiarthroplasty (unipolar/bipolar) or total hip arthroplasty (THA) for displaced fractures, offering predictable outcomes and early mobilization. THA is preferred in active, low-demand patients with pre-existing degenerative hip disease.
- Non-Displaced or Minimally Displaced Femoral Neck Fractures: Often treated with internal fixation (cannulated screws) across all age groups to prevent displacement and achieve healing. Close monitoring for AVN and nonunion is essential.
- Intertrochanteric Fractures (All types): Nearly universally managed operatively due to the inherent instability, significant deforming muscle forces, and need for early weight-bearing. Fixation options include dynamic hip screws (DHS) for stable patterns or cephalomedullary nails (IMN) for unstable patterns (reverse obliquity, subtrochanteric extension, comminution).
- Subtrochanteric Fractures: Operative stabilization is mandatory due to high biomechanical stress, strong deforming muscle forces, and high rates of nonunion and malunion with non-operative treatment. Long cephalomedullary nails are the preferred implant.
- Pathological Fractures (e.g., Metastatic Disease): Often require prophylactic fixation or reconstruction with IMN or arthroplasty to prevent impending fracture or stabilize existing fracture, aiming for pain relief and functional restoration.
- Femoral Head Fractures: Typically occur with hip dislocations. Management depends on Pipkin classification (e.g., fragments needing excision, open reduction and internal fixation for large displaced fragments, THA in selected cases).
Contraindications to Surgery
Absolute contraindications are rare and typically relate to the patient's immediate physiological status.
*
Moribund Patient:
Anesthetic and surgical risks outweigh potential benefits. Palliative care with pain management is prioritized.
*
Uncontrolled Medical Comorbidities:
Severe, uncompensated cardiac, pulmonary, or neurological conditions where general or regional anesthesia poses an unacceptable risk. Aggressive medical optimization is attempted first.
*
Active Sepsis or Systemic Infection:
Increases the risk of surgical site infection and implant failure. Infection must be controlled before elective surgery.
*
Non-Ambulatory Status with Minimal Pain:
In rare cases of non-displaced or stable fractures in non-ambulatory patients with minimal pain, non-operative management might be considered after careful multidisciplinary evaluation.
Operative vs. Non-Operative Indications Summary
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Femoral Neck Fractures | Displaced (all ages), Non-displaced (all ages) | Non-ambulatory, minimal pain, extreme medical comorbidities |
| Intertrochanteric Fractures | All patterns (stable/unstable) | Extreme medical comorbidities, non-ambulatory, palliative |
| Subtrochanteric Fractures | All patterns | Extreme medical comorbidities, non-ambulatory, palliative |
| Pathological Fractures | Prophylactic fixation, pain, functional restoration | Limited life expectancy, pain well-controlled, no functional need |
| Patient Status | Medically stable, ambulatory potential, desire for function | Moribund, uncontrolled systemic infection, severe comorbidities |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for minimizing complications and optimizing surgical outcomes.
Diagnostic Imaging
- Plain Radiographs: Anteroposterior (AP) pelvis, true lateral view of the affected hip, and sometimes a contralateral hip view for templating or comparison. These define fracture location, pattern, displacement, and comminution.
- Computed Tomography (CT) Scan: Indicated for complex fracture patterns, articular involvement (femoral head fractures), occult fractures not seen on plain films, or for precise assessment of comminution and fragment rotation in subtrochanteric fractures. Useful for preoperative 3D reconstruction.
- Magnetic Resonance Imaging (MRI): Gold standard for detecting occult fractures (e.g., stress fractures of the femoral neck in athletes) when plain radiographs are negative, or for assessing AVN.
- Bone Scan: Less commonly used now but can identify occult fractures or metastatic lesions.
Medical Optimization
A multidisciplinary approach is crucial, especially for elderly patients.
*
Geriatric Co-management:
Improves outcomes, reduces complications (delirium, pressure ulcers), and facilitates earlier mobilization.
*
Anesthesia Consultation:
Assessment of patient comorbidities (ASA classification), choice of anesthesia (general vs. regional), and pain management strategies.
*
Internal Medicine/Cardiology/Pulmonology:
Optimization of chronic medical conditions (e.g., hypertension, diabetes, cardiac disease, COPD) to reduce perioperative risks.
*
Nutritional Assessment:
Malnutrition is common in elderly hip fracture patients and needs to be addressed pre- and post-operatively.
*
DVT Prophylaxis:
Initiation of chemical and/or mechanical prophylaxis as soon as safely possible.
Templating
Preoperative templating involves using radiographic images (AP pelvis) and manufacturer templates to determine appropriate implant size, length, and offset. This is critical for:
*
Internal Fixation (DHS/IMN):
Determining screw/nail length, diameter, angle (in DHS), and ensuring appropriate distal fixation.
*
Arthroplasty (Hemi/THA):
Sizing the femoral stem, head diameter, offset, and leg length assessment.
Patient Positioning
Correct patient positioning is critical for surgical access, fracture reduction, and fluoroscopic imaging.
*
Supine on a Fracture Table:
Most common for intertrochanteric and subtrochanteric fractures treated with intramedullary nailing (IMN) or dynamic hip screw (DHS), and for cannulated screw fixation of femoral neck fractures.
*
Advantages:
Allows for controlled traction, internal/external rotation, and adduction/abduction via boot traction. Facilitates fluoroscopic imaging in multiple planes.
*
Disadvantages:
Requires careful padding to prevent pressure injuries. Perineal post can cause pressure necrosis.
*
Setup:
Unaffected leg is abducted and flexed to allow C-arm access. Affected leg is in line with the body.
*
Supine on a Radioducent Table:
Used for total hip arthroplasty (THA) or hemiarthroplasty when a direct anterior (DAA) approach is chosen. Allows for full limb mobilization during surgery.
*
Lateral Decubitus Position:
Used for posterior approaches to the hip (e.g., for THA, hemiarthroplasty, or Pipkin fracture fixation), or occasionally for highly comminuted subtrochanteric fractures where direct lateral exposure is preferred for plating.
*
Setup:
Patient is placed on the unaffected side, stabilized with bean bag and kidney rests. Careful padding of dependent arm and leg.
*
Considerations:
All positions require careful attention to nerve protection (e.g., common peroneal nerve at fibular head, ulnar nerve at elbow), adequate padding of bony prominences, and secure strapping.
Detailed Surgical Approach / Technique
The choice of surgical technique depends heavily on the fracture classification, patient age, bone quality, and surgeon preference.
Femoral Neck Fractures
Intracapsular fractures (subcapital, transcervical, basicervical)
A. Internal Fixation (Cannulated Screws):
*
Indications:
Non-displaced fractures (Garden I/II), displaced fractures in younger patients (<60-65 years) where head preservation is paramount, or physiologically young/active elderly patients.
*
Positioning:
Supine on fracture table.
*
Approach:
Minimally invasive, involving small stab incisions for guidewire placement.
*
Reduction:
Essential for displaced fractures. Techniques include the Leadbetter maneuver (traction, internal rotation, abduction, then gentle internal rotation) or external rotation/abduction/traction. Intraoperative fluoroscopy (AP/Lateral) confirms reduction.
*
Technique:
1. Place guidewires (typically 2 or 3) from the lateral femoral cortex, aiming into the femoral head. A common configuration is an inverted triangle for stability, with one inferior and two superior screws. The inferior screw should be parallel to the calcar femorale.
2. Wires should be parallel in the AP view and diverging anteriorly/posteriorly in the lateral view to maximize bone purchase.
3. Confirm placement with fluoroscopy; avoid penetrating the articular cartilage.
4. Measure screw lengths, drill, tap (if needed), and insert cannulated screws. Ensure proper compression across the fracture site.
5. Check for limb length and rotation.
*
Pearls:
Anatomic reduction is crucial for vascularity and healing. Varus malreduction or posterior comminution is associated with higher failure rates.
B. Arthroplasty (Hemiarthroplasty or Total Hip Arthroplasty - THA):
*
Indications:
Displaced femoral neck fractures (Garden III/IV) in elderly patients (>65 years) or those with significant comorbidities, particularly for hemiarthroplasty. THA is preferred for active elderly patients with pre-existing symptomatic osteoarthritis or high functional demands.
*
Positioning:
Supine on a standard radiolucent table (for DAA) or lateral decubitus (for posterior/anterolateral approaches).
*
Approaches:
*
Posterior (Kocher-Langenbeck):
Most common, internervous plane between gluteus maximus (superior gluteal nerve) and piriformis/obturator internus (sacral plexus). Dissection involves releasing external rotators.
*
Anterolateral (Hardinge/Watson-Jones):
Internervous plane between tensor fascia latae (superior gluteal nerve) and gluteus medius (superior gluteal nerve). Involves splitting the gluteus medius/vastus lateralis.
*
Direct Anterior (DAA):
Internervous plane between tensor fascia latae (superior gluteal nerve) and sartorius (femoral nerve). Does not detach muscles from the greater trochanter. Requires specialized instrumentation and expertise.
*
Technique:
1. Access the hip joint via the chosen approach.
2. Dislocate the femoral head and excise it.
3. Prepare the femoral canal (reaming/broaching) to accept the stem. Bone quality determines cemented vs. uncemented stem.
4. Size the femoral stem and trial reduce.
5. For hemiarthroplasty, implant a unipolar or bipolar femoral head. For THA, ream and prepare the acetabulum for acetabular cup insertion (often uncemented with screw fixation), then implant the prosthetic femoral head.
6. Perform trial reduction and assess stability, leg length, and offset.
7. Definitive implant insertion.
8. Layered wound closure.
*
Pearls:
Meticulous soft tissue handling, precise component positioning for stability and longevity, and appropriate leg length restoration.
Intertrochanteric Fractures
Extracapsular fractures
A. Dynamic Hip Screw (DHS) with Side Plate:
*
Indications:
Stable intertrochanteric fractures (e.g., 2-part, AO/OTA 31-A1) where the posteromedial cortex is intact or can be reconstructed. Less commonly used for unstable patterns due to high failure rates.
*
Positioning:
Supine on a fracture table with traction.
*
Approach:
Lateral incision, centered on the greater trochanter. Dissect down to the vastus lateralis, incise its fascia, and elevate it anteriorly.
*
Reduction:
Restore length, alignment, and rotation. Use traction, internal rotation, and sometimes direct manipulation (joystick/pointed reduction clamp). Confirm with fluoroscopy (AP/Lateral).
*
Technique:
1. Place a guide wire for the lag screw into the femoral head, centered on the calcar femorale and in the inferior quadrant on the lateral view. Ensure optimal tip-apex distance (TAD <25mm).
2. Ream for the lag screw barrel and tap.
3. Insert the lag screw.
4. Slide the side plate barrel over the lag screw, align the plate with the femoral shaft, and fix it with cortical screws.
5. Insert the compression screw to achieve controlled impaction.
6. Check for limb length and rotation.
7. Layered wound closure.
*
Pearls:
TAD is a critical predictor of cutout. Proper reduction is paramount. Maintain slight valgus to resist varus collapse.
B. Cephalomedullary Nail (IMN):
*
Indications:
Unstable intertrochanteric fractures (e.g., 3-part, 4-part, reverse obliquity, AO/OTA 31-A2/A3), and those with subtrochanteric extension. Also preferred for osteoporotic bone.
*
Positioning:
Supine on a fracture table with traction.
*
Approach:
Small incision at the tip of the greater trochanter or slightly medial for appropriate nail entry point.
*
Reduction:
Traction, internal rotation. Use fluoroscopy. Reduction can be challenging for unstable patterns; percutaneous clamps, joysticks, or indirect reduction techniques may be needed.
*
Technique:
1.
Entry Point:
Critical. Lateral aspect of the greater trochanter, at or slightly medial to the tip, in line with the femoral canal on both AP and lateral views. Improper entry can lead to varus malalignment or fracture of the greater trochanter.
2. Open the femoral canal with an awl/reamer.
3. Ream the femoral canal to appropriate size (if non-cannulated).
4. Insert the cephalomedullary nail.
5. Insert the lag screw(s) into the femoral head, aiming for optimal TAD (<25mm). For some nails, a second screw (cervical/trochanteric) may be used.
6. Distal locking screws are inserted to prevent rotation and maintain length. Dynamic vs. static locking depends on fracture stability and surgeon preference.
7. Check for limb length and rotation.
8. Layered wound closure.
*
Pearls:
Proper entry point is crucial. Maintaining reduction during nail insertion can be challenging. Lag screw position and TAD are vital for preventing cutout.
Subtrochanteric Fractures
A. Long Cephalomedullary Nail (IMN):
*
Indications:
Preferred treatment for most subtrochanteric fractures due to superior biomechanical stability in this high-stress region.
*
Positioning:
Supine on a fracture table with strong traction.
*
Approach:
Small incision at the tip of the greater trochanter, as for intertrochanteric nailing, or slightly more proximal and medial depending on specific nail design.
*
Reduction:
Often the most challenging aspect due to strong muscle deforming forces (iliopsoas, glutei, adductors).
*
Proximal fragment:
Often flexed, abducted, and externally rotated.
*
Distal fragment:
Often adducted and internally rotated.
* Techniques: Traction, counter-traction, manual manipulation, fracture table maneuvers, external fixation outriggers, cerclage wires (open reduction), or specialized reduction clamps.
*
Technique:
1.
Entry Point:
Crucial, as for intertrochanteric nailing, to avoid varus malreduction.
2. Open the canal, ream.
3. Insert the long cephalomedullary nail. This often requires significant force and careful manipulation to pass the fracture site.
4. Insert the lag screw(s) into the femoral head, ensuring optimal TAD.
5. Insert multiple distal locking screws (typically two) to control rotation and prevent shortening.
6. Confirm length, rotation, and alignment with fluoroscopy.
7. Layered wound closure.
*
Pearls:
Achieving and maintaining reduction during nail insertion is paramount. Beware of iatrogenic comminution during reduction attempts. Use of blocking screws may aid in reduction.
B. Plate Osteosynthesis (e.g., Locking Plates):
*
Indications:
Less common now for primary subtrochanteric fractures, generally reserved for specific fracture patterns not amenable to IMN (e.g., very distal subtrochanteric fractures approaching the condyles, very proximal comminution not allowing good IMN fixation, or failed IMN).
*
Positioning:
Lateral decubitus or supine on a radiolucent table.
*
Approach:
Direct lateral approach, elevating the vastus lateralis from the lateral femoral shaft.
*
Technique:
1. Achieve reduction (often open reduction is required due to complex comminution).
2. Contour a long locking plate to the lateral aspect of the femur.
3. Secure the plate with locking screws proximally and distally, ensuring adequate bone purchase in both fragments.
4. Consider adjunctive cerclage wires for highly comminuted patterns.
5. Layered wound closure.
*
Pearls:
Requires more extensive soft tissue dissection, which may compromise vascularity. Biomechanically less stiff than IMN for high-energy subtrochanteric fractures.
General Intraoperative Principles
- Fluoroscopy: Essential for all proximal femoral fracture fixation to confirm reduction, guidewire placement, implant position, and overall alignment.
- Sterile Technique: Meticulous adherence to sterile protocols to minimize infection risk.
- Blood Loss Management: Prophylactic measures (e.g., tranexamic acid), careful hemostasis, and readiness for transfusion.
- Soft Tissue Protection: Minimize stripping, use careful retraction to protect muscle, nerve, and vascular structures.
Complications & Management
Proximal femoral fractures carry a significant risk of complications, both surgical and medical, demanding vigilant monitoring and proactive management.
Common Complications & Salvage Strategies
| Complication | Incidence | Management / Salvage Strategy |
|
Mortality
| Approx. 5-10% (in-hospital), 20-30% (1-year) | Aggressive medical optimization, early surgery, DVT/PE prophylaxis, geriatric co-management. |
|
Infection (SSI)
| 1-5% | Prophylactic antibiotics, meticulous sterile technique, minimize surgical time, wound care. Salvage: Debridement, irrigation, suppressive antibiotics; explantation & two-stage revision arthroplasty (for periprosthetic infection). |
|
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE)
| DVT: 40-60% (untreated), PE: 1-10% | Early mobilization, chemical prophylaxis (LMWH, fondaparinux, aspirin), mechanical prophylaxis (compression stockings, SCDs). Salvage: Anticoagulation for DVT/PE, IVC filter for recurrent PE with contraindications to anticoagulation. |
|
Malunion
| Varies (5-20%) | For symptomatic malunion (pain, gait disturbance, LLD): Corrective osteotomy. Non-symptomatic may be observed. |
|
Nonunion
| Femoral Neck: 10-30%; Subtrochanteric: 5-15% | Femoral Neck: Revision internal fixation with bone graft, valgus osteotomy, or conversion to hemiarthroplasty/THA. Inter/Subtrochanteric: Revision nailing/plating, bone graft (autograft/allograft), stimulating devices (electrical/ultrasound). ### Patient
Early Post-Op (0-2 weeks):
*
Pain Management:
Multimodal analgesia.
*
Weight Bearing (WB):
Determined by fracture stability and fixation.
*
Stable Fixation (e.g., non-displaced femoral neck fixation, stable intertrochanteric IMN):
Often weight-bearing as tolerated (WBAT) or touch-bearing weight (TDWBAT).
*
Unstable Fixation/Fractures (e.g., comminuted subtrochanteric, poor bone quality):
Protected weight-bearing (PWB) or non-weight-bearing (NWB) for 6-12 weeks.
*
Arthroplasty:
Typically WBAT.
*
Range of Motion (ROM):
Initiate gentle, active-assisted and passive ROM exercises within pain limits. Avoid hip precautions (if indicated for arthroplasty) – typically for posterior approach (avoid flexion >90, adduction, internal rotation).
*
Strengthening:
Gentle isometric exercises (quad sets, glute sets).
*
Mobility:
Bed mobility, transfer training, short-distance ambulation with appropriate assistive devices (walker, crutches).
*
DVT Prophylaxis:
Continue chemical and mechanical prophylaxis.
*
Wound Care:
Monitor incision site for signs of infection.
Intermediate Phase (2-12 weeks):
*
Weight Bearing:
Progress as tolerated, based on radiographic signs of healing and fracture stability.
*
ROM:
Continue to increase active and passive ROM.
*
Strengthening:
Progressive resistive exercises for hip abductors, adductors, flexors, and extensors. Core strengthening.
*
Gait Training:
Focus on normal gait mechanics, balance, and endurance. Progress from walker to crutches to cane.
*
Scar Management:
Initiate scar massage.
Advanced Phase (>12 weeks):
*
Functional Training:
Progress to functional activities, stairs, uneven surfaces.
*
Return to Activity:
Gradually return to recreational and work-related activities. High-impact sports may be restricted depending on fracture type and fixation.
*
Strength and Endurance:
Continue advanced strengthening and cardiovascular conditioning.
*
Fall Prevention:
Ongoing assessment and intervention for fall risk (balance training, home modification, medication review).
*
Bone Health:
Address underlying osteoporosis with medication (bisphosphonates, PTH analogs, denosumab), calcium, and Vitamin D.
Specific Considerations
-
Femoral Neck Fractures:
- Internal Fixation: Protected WB for 6-12 weeks due to risk of nonunion/AVN. Close radiographic follow-up for signs of failure or complications.
- Arthroplasty: Early WBAT, focus on hip precautions if posterior approach.
- Intertrochanteric Fractures: Often WBAT or TDWBAT from early post-op due to good cancellous bone healing, unless fixation is unstable or fracture highly comminuted.
- Subtrochanteric Fractures: Often require protected WB for longer periods (3-6 months) due to high stress and risk of nonunion/implant failure.
Summary of Key Literature / Guidelines
The management of proximal femoral fractures is guided by robust clinical evidence and international consensus.
Classification Systems
-
AO/OTA Classification:
The universally accepted system for all fractures. For proximal femur:
- 31-A: Peritrochanteric fractures (intertrochanteric, subtrochanteric). Subdivided by number of fragments and stability.
- 31-B: Femoral neck fractures. Subdivided by location (subcapital, transcervical, basicervical).
- 31-C: Femoral head fractures. Subdivided by Pipkin classification.
-
Garden Classification (Femoral Neck):
Based on displacement and trabecular alignment, correlates with blood supply disruption.
- Type I: Incomplete fracture, valgus impacted.
- Type II: Complete fracture, non-displaced.
- Type III: Complete fracture, partially displaced (varus angulation).
- Type IV: Complete fracture, completely displaced.
-
Pauwels Classification (Femoral Neck):
Based on the angle of the fracture line relative to the horizontal, predicting shear forces and stability.
- Type I: <30 degrees (low shear, more stable).
- Type II: 30-50 degrees.
- Type III: >50 degrees (high shear, very unstable).
- Evans-Jensen Classification (Intertrochanteric): Based on fracture pattern, comminution, and stability. Differentiates stable from unstable patterns, which guides implant choice (DHS vs. IMN).
Key Guidelines and Recommendations
-
AAOS (American Academy of Orthopaedic Surgeons) Clinical Practice Guidelines:
Provide evidence-based recommendations for hip fracture management, addressing timing of surgery, choice of implant (internal fixation vs. arthroplasty), pain management, DVT prophylaxis, and geriatric co-management. Key recommendations include:
- Surgery within 48 hours for most patients to reduce morbidity and mortality.
- Hemiarthroplasty for displaced femoral neck fractures in active elderly patients.
- THA for active, physiologically younger patients with displaced femoral neck fractures and pre-existing hip arthritis.
- Cephalomedullary nails for unstable intertrochanteric fractures.
- Multidisciplinary care, including orthogeriatric co-management.
- NICE (National Institute for Health and Care Excellence) Guidelines (UK): Echo many AAOS recommendations, emphasizing early surgery, rehabilitation, and secondary prevention of fragility fractures.
Landmark Literature & Trials
- FAITH Trial (Fixation of Ankle Fractures in the Elderly): While focused on ankle fractures, it underscores the importance of proper fixation in osteoporotic bone. A similar trial for hip fractures (e.g., comparing different femoral neck fixation strategies) would be impactful.
- HEALTH Trial (Hip fracture Evaluation AT Home vs. Hospital): Investigating the impact of post-operative care settings on outcomes.
- Studies on Intramedullary Nailing vs. Dynamic Hip Screw: Numerous meta-analyses consistently demonstrate that cephalomedullary nails are superior for unstable intertrochanteric fractures, particularly reverse obliquity and those with subtrochanteric extension, due to better biomechanical control and lower rates of implant failure. DHS remains a viable option for truly stable 2-part fractures.
- Studies on Arthroplasty vs. Internal Fixation for Displaced Femoral Neck Fractures: Systematic reviews and randomized controlled trials consistently show that arthroplasty (hemi or THA) leads to lower reoperation rates compared to internal fixation in elderly patients with displaced femoral neck fractures, albeit with a higher initial surgical risk. The choice between hemiarthroplasty and THA in suitable patients is often debated, with THA offering better long-term function but higher dislocation risk.
- Role of Geriatric Co-management: Studies consistently show that orthopedic-geriatric co-management models lead to reduced hospital length of stay, lower rates of delirium, improved functional outcomes, and reduced one-year mortality.
The continuous evolution of surgical techniques, implant design, and perioperative care protocols necessitates ongoing engagement with current literature and adherence to evidence-based guidelines for optimal patient care.
You Might Also Like