Pelvic Ring Fractures: Your Guide to Diagnosis, Treatment & Recovery
Key Takeaway
This topic focuses on Pelvic Ring Fractures: Your Guide to Diagnosis, Treatment & Recovery, Pelvic ring fractures are high-energy injuries to the pelvic ring, typically occurring due to blunt trauma. Diagnosis is made radiographically with pelvic X-rays and further characterized by CT scans. Treatment usually involves operative fixation, depending on the degree of pelvic instability, fracture displacement, and patient activity demands.
Introduction & Epidemiology
Pelvic ring fractures are severe, high-energy injuries typically resulting from blunt trauma. They represent a significant challenge in orthopedic trauma due to their association with severe systemic injuries, high morbidity, and mortality. Understanding the biomechanics, classification, and management principles is paramount for optimal patient outcomes.
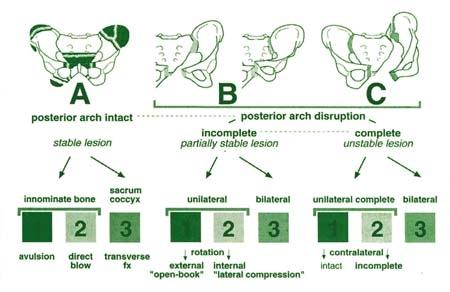
Historically, pelvic ring fractures have been categorized to guide management and prognostication. The Tile classification (Type A: stable, Type B: rotationally unstable but vertically stable, Type C: rotationally and vertically unstable) focuses on the mechanical stability of the posterior pelvic ring. The Young-Burgess classification is mechanism-based, dividing fractures into Lateral Compression (LC), Anteroposterior Compression (APC), Vertical Shear (VS), and Combined Mechanical (CM) types, each with subtypes reflecting increasing instability and injury severity. The AO/OTA classification provides a comprehensive alphanumeric system for detailed injury description, often utilized in research and comprehensive trauma centers. The choice of classification system can influence treatment algorithms and communication among specialists.
Epidemiologically, pelvic ring fractures are relatively uncommon, accounting for approximately 1-3% of all skeletal fractures. However, the associated mortality rates range from 5-20% in hemodynamically stable patients to over 50% in patients with severe hemorrhagic shock. The incidence demonstrates a bimodal distribution: predominantly young males involved in high-energy trauma (e.g., motor vehicle collisions, falls from height) and elderly individuals sustaining low-energy falls, often complicated by osteoporotic bone quality.
Associated injuries are a hallmark of pelvic ring fractures and significantly impact management. As identified in the initial assessment, orthopedic injuries commonly include long bone fractures (up to 50%), chest injuries (up to 63%), and spine fractures (up to 25%). Non-orthopedic injuries are equally critical: genitourinary system injuries (urethral tears, bladder ruptures) occur in 5-20%, with subsequent sexual dysfunction reported in up to 50% of male patients. Head and abdominal injuries are also prevalent in approximately 40% of cases. The significant concurrent trauma necessitates a multidisciplinary approach, adhering strictly to Advanced Trauma Life Support (ATLS) protocols for initial resuscitation and comprehensive evaluation.
Pediatric pelvic ring fractures present unique considerations. Due to the presence of open triradiate cartilage and greater elasticity of the immature skeleton, fracture patterns differ. These typically involve the pubic rami and iliac wings, and rarely disrupt the robust sacroiliac ligaments, resulting in inherently more stable injury patterns. Consequently, pediatric pelvic ring fractures usually respond well to non-operative management and rarely require surgical intervention, unless significant displacement or instability exists after skeletal maturation.
Surgical Anatomy & Biomechanics
The pelvic ring is a closed, osseo-ligamentous structure designed for force transmission, weight-bearing, and protection of pelvic viscera. Its integrity is critical for bipedal locomotion and stability.
Osteology: The pelvic ring comprises three main bones: the sacrum posteriorly and two paired innominate bones laterally and anteriorly. Each innominate bone is formed by the fusion of the ilium, ischium, and pubis, uniting at the acetabulum. The sacrum articulates with the ilia at the sacroiliac (SI) joints, forming the posterior arch. Anteriorly, the two pubic bones articulate at the pubic symphysis. This ring structure dictates that displacement can only occur with disruption in at least two places, a fundamental concept in understanding pelvic instability.
Ligamentous Structures:
The stability of the pelvic ring is primarily dependent on its strong surrounding ligamentous structures, particularly those of the posterior pelvic ring.
*
Posterior Pelvic Ligaments:
These are the most critical for stability.
*
Sacroiliac Ligaments:
Comprising anterior, posterior, and interosseous components. The interosseous and posterior sacroiliac ligaments are exceptionally strong, resisting both translational and rotational forces. Injury to these ligaments is a hallmark of unstable pelvic ring fractures.
*
Sacrotuberous Ligament:
Extends from the sacrum/coccyx to the ischial tuberosity, providing vertical stability and resisting external rotation.
*
Sacrospinous Ligament:
Connects the sacrum to the ischial spine, contributing to vertical stability and dividing the greater and lesser sciatic foramina.
*
Anterior Pelvic Ligaments:
*
Pubic Symphysis Ligaments:
Superior, inferior (arcuate), anterior, and posterior pubic ligaments. The inferior arcuate ligament is the thickest. While contributing to symphyseal integrity, these are less critical for overall pelvic stability compared to the posterior ligaments.
Biomechanics of the Pelvic Ring: The pelvis functions as a force transducer, transmitting axial loads from the spine to the lower extremities and vice-versa. During normal gait, significant shear and rotational forces are generated across the SI joints. The "two-point rule" or "Maissoneuve concept" states that a single break in the pelvic ring typically does not lead to displacement because the opposing intact side of the ring prevents significant motion. Therefore, an unstable pelvic ring fracture implies disruption of the ring in at least two locations (e.g., pubic symphysis diastasis and ipsilateral posterior SI ligamentous disruption). The specific pattern of these disruptions determines the type and degree of instability (rotational, vertical, or combined).
Neurovascular Structures:
Neurovascular structures are intimately associated with the posterior pelvic ligaments and bony anatomy, rendering them highly vulnerable in pelvic ring injuries and during surgical approaches.
*
Nerves:
The
lumbosacral plexus
(L4-S4) lies on the anterior surface of the sacrum, immediately adjacent to the SI joints. Specific branches at risk include:
*
Sciatic nerve:
Emerging from the greater sciatic foramen.
*
Femoral nerve:
In the iliac fossa.
*
Obturator nerve:
Exiting the obturator foramen.
*
Superior and inferior gluteal nerves:
Exiting above and below the piriformis muscle.
*
Pudendal nerve:
Often injured with sacral fractures, running near the sacrospinous ligament.
* Specific sacral nerve roots (S1, S2, S3) are particularly vulnerable to injury from sacral fractures (especially Denis Zone II and III) or iatrogenic damage during iliosacral screw placement.
*
Vessels:
The
internal iliac artery and its branches
(superior and inferior gluteal, internal pudendal, obturator) are closely associated with the posterior pelvic structures. The
presacral venous plexus
is extensive and highly fragile, making venous hemorrhage the most common and often devastating source of bleeding in pelvic trauma. Arterial injuries, though less common, are associated with higher mortality due to rapid blood loss. The proximity of the superior gluteal artery to the SI joint and greater sciatic notch makes it susceptible to injury with posterior displacement or errant screw placement.
Understanding these intricate relationships is crucial for accurate diagnosis, meticulous pre-operative planning, and safe surgical execution to minimize iatrogenic complications.
Indications & Contraindications
The decision for operative versus non-operative management of pelvic ring fractures is complex, balancing hemodynamic stability, fracture pattern, mechanical stability, associated injuries, and patient factors. The overarching principle for unstable pelvic ring injuries is early stabilization to control hemorrhage, prevent further neurovascular damage, and facilitate rehabilitation.
General Principles:
Initial management adheres to ATLS guidelines, prioritizing airway, breathing, circulation. Hemodynamic instability due to pelvic hemorrhage necessitates immediate stabilization, often involving external fixation, pelvic binders, resuscitative endovascular balloon occlusion of the aorta (REBOA), pre-peritoneal packing, and/or angioembolization, irrespective of definitive fracture fixation. Damage control orthopedics principles often dictate initial temporary stabilization followed by definitive fixation once the patient is physiologically optimized.
Operative Indications:
- Hemodynamic Instability: While not a direct indication for definitive fixation, persistent hemodynamic instability attributable to pelvic hemorrhage (after non-operative measures like external compression and fluid resuscitation) often mandates rapid external fixation, pre-peritoneal packing, and/or angiographic embolization.
- Mechanical Instability: Fractures classified as rotationally unstable (Tile B, Young-Burgess APC II/III, LC II/III) or rotationally and vertically unstable (Tile C, Young-Burgess VS) require surgical stabilization to restore the integrity of the weight-bearing axis.
-
Significant Fracture Displacement:
- Pubic Symphysis Diastasis: Typically >2.5 cm or recurrent displacement after closed reduction.
- Sacroiliac Joint Diastasis/Dislocation: >1 cm displacement or significant rotation.
- Sacral Fractures: Displacement of the sacral body >1 cm, especially in the sagittal plane, or significant comminution compromising the SI joint.
- Vertical displacement: Any significant vertical translation of the hemipelvis (e.g., >0.5-1 cm) indicates complete posterior ligamentous disruption (Vertical Shear injury).
- Open Fractures: Require urgent surgical debridement, washout, and often external fixation or delayed definitive fixation once soft tissues allow.
- Neurological Deficit: New or progressive neurological deficit directly attributable to fracture displacement (e.g., sacral nerve root impingement from a displaced sacral fracture) warrants operative decompression and stabilization.
- Entrapment of Soft Tissues: Including nerve roots, vessels, or bowel within the fracture site.
- Irreducible Dislocations: Of the pubic symphysis or sacroiliac joint.
- Patient Activity Demands: Active patients typically benefit from anatomical reduction and rigid fixation to facilitate early mobilization and return to function.
Non-Operative Indications:
- Hemodynamically Stable Patients: Without evidence of ongoing pelvic hemorrhage.
- Mechanically Stable Fractures: Fractures classified as stable (Tile A, Young-Burgess LC I, APC I). These include isolated avulsion fractures, undisplaced pubic rami fractures, or stable iliac wing fractures.
- Minimally Displaced Fractures: Where the posterior pelvic ring remains intact or minimally disrupted, and stability is maintained under physiological stress.
- Specific Pediatric Patterns: As discussed, most pediatric pelvic ring fractures are stable and heal with non-operative management.
- Severe Comorbidities: Patients with severe, uncontrolled medical comorbidities (e.g., end-stage cardiac disease, severe coagulopathy, uncontrolled sepsis) who are unable to tolerate surgery. In these cases, prolonged bed rest or temporary external fixation may be the only option.
- Extensive Soft Tissue Compromise: Where open definitive fixation is temporarily contraindicated due to extensive degloving injuries or severe wound contamination, requiring delayed fixation after soft tissue healing.
Contraindications:
- Absolute: Uncontrolled sepsis, severe irreversible coagulopathy, extreme physiological derangement where the risks of surgery far outweigh the potential benefits. These are usually temporary and indicate a need for patient optimization rather than a permanent contraindication to fixation.
- Relative: Active local infection, extensive skin loss, severe burns overlying the surgical site, pre-existing neurological deficits where surgical intervention offers no anticipated improvement.
Summary Table: Operative vs. Non-Operative Indications
| Factor | Operative Indication | Non-Operative Indication |
|---|---|---|
| Hemodynamics | Unstable due to pelvic hemorrhage (initial stabilization) | Stable, no ongoing hemorrhage |
| Mechanical Stability | Unstable (Tile B/C, Young-Burgess VS, APC II/III, LC II/III) | Stable (Tile A, Young-Burgess LC I, APC I) |
| Displacement | Significant (>2.5cm symphysis, >1cm SI joint, >1cm sacral) | Minimally displaced, stable under stress |
| Open Fracture | Present (requires debridement + fixation) | Absent |
| Neurologic Deficit | New/progressive, sacral fracture-related | Absent or non-progressive, not surgical amenable |
| Entrapment | Nerves, vessels, soft tissue entrapment | No entrapment |
| Irreducibility | Irreducible symphysis or SI joint dislocations | Reducible or stable non-displaced |
| Age/Comorbidities | Physiologically fit for surgery | Severe comorbidities precluding surgery |
| Soft Tissue | Manageable | Severe compromise preventing immediate ORIF (relative) |
| Pediatric | Rare, severe instability, significant displacement (post-closure) | Most pediatric cases, stable fracture patterns |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for successful outcomes in pelvic ring fracture surgery, minimizing complications, and optimizing the surgical approach.
Initial Resuscitation & Assessment:
Following ATLS protocols, the initial focus is on life-saving interventions. Hemodynamic instability due to pelvic hemorrhage is addressed with a multidisciplinary approach:
*
Pelvic Binder/Sheet:
Applied circumferentially at the level of the greater trochanters to reduce pelvic volume and tamponade bleeding.
*
External Fixation:
Often applied emergently in the trauma bay or operating room for rapid provisional stabilization, hemorrhage control, and reduction of pelvic volume. Supra-acetabular pins are preferred for rigidity and avoiding neurovascular structures.
*
Angioembolization:
Indicated for arterial hemorrhage identified on angiography in hemodynamically unstable patients or those with persistent bleeding despite mechanical stabilization.
*
Pre-peritoneal Packing:
A rapid, surgical technique to pack the retroperitoneal space to control venous bleeding, often used in conjunction with external fixation.
*
REBOA:
Used in severely unstable patients as a bridge to definitive hemorrhage control.
Imaging:
*
Initial Radiographs:
AP pelvis, inlet, and outlet views are standard. The AP view assesses symphyseal diastasis and vertical displacement. The inlet view (45-60 degrees caudal tilt) evaluates posterior translation, sacral body fractures, and anterior-posterior compression. The outlet view (45 degrees cranial tilt) assesses vertical displacement of the hemipelvis and sacral foramen involvement.
*
Computed Tomography (CT) Scan:
The definitive imaging modality for characterization. A full pelvic CT with thin cuts and 3D reconstructions is essential. It precisely delineates fracture morphology, sacral fracture patterns (Denis zones), SI joint disruption (diastasis, impaction, subluxation), internal rotation (LC injuries), and subtle posterior displacement. CT also identifies potential nerve root impingement, intra-articular fragments, and associated visceral injuries.
*
Magnetic Resonance Imaging (MRI):
Indicated if persistent or new neurological deficits are present, to evaluate for nerve root compression from disc herniation, hematoma, or soft tissue injury to the lumbosacral plexus that may not be evident on CT. It can also detect purely ligamentous posterior disruptions not seen on CT.
*
Angiography:
Performed in conjunction with embolization for persistent arterial hemorrhage.
Timing of Surgery:
The optimal timing of definitive fixation depends on the patient's physiological status and fracture pattern.
*
Damage Control Orthopedics (DCO):
For critically ill or physiologically deranged patients, initial temporary external fixation or posterior stabilization (e.g., percutaneous iliosacral screws) is performed, followed by definitive fixation once the patient is stable (typically within 3-10 days).
*
Early Definitive Fixation:
In stable patients, definitive fixation within the first few days (ideally 24-72 hours) can reduce complications like DVT, ARDS, and improve long-term outcomes. Delaying definitive fixation beyond 1-2 weeks can make reduction more challenging due to early callus formation and muscle spasm.
Pre-operative Considerations:
*
Blood Products:
Ensure adequate cross-matched blood is available.
*
DVT Prophylaxis:
Initiate pharmacological (heparin, LMWH) and mechanical (sequential compression devices) prophylaxis early.
*
Antibiotics:
Administer pre-operative broad-spectrum antibiotics, especially for open fractures.
*
Urinary Catheter:
Insert a Foley catheter. Crucially, a retrograde urethrogram (RUG) must be performed in male patients with suspected urethral injury (e.g., blood at the meatus, scrotal hematoma, high-riding prostate) before catheter insertion.
*
Neurological Assessment:
Thorough baseline neurological exam, especially of the lower extremities and perineum, is critical.
Patient Positioning:
Accurate positioning on a radiolucent table is paramount for intraoperative fluoroscopy and surgical access.
*
Supine Position:
Standard for anterior approaches (pubic symphysis plating, ilioinguinal approach) and percutaneous iliosacral screw placement. A bump or bolster under the contralateral SI joint can aid in achieving optimal inlet/outlet fluoroscopic views for posterior fixation.
*
Prone Position:
Required for open posterior approaches (e.g., for SI joint disruption, sacral fractures, posterior iliac wing fractures). Care must be taken to pad all pressure points and ensure abdominal free-hang to prevent increased intra-abdominal pressure and epidural venous bleeding. The use of a specialized spinal table or bolsters can facilitate this.
*
Lateral Decubitus:
Rarely used for primary pelvic ring fixation, but may be combined with anterior/posterior approaches for complex acetabular or posterior column fractures.
*
Traction:
Skeletal traction (e.g., distal femoral or proximal tibial pin) may be applied pre-operatively for vertical shear injuries to aid in reduction, and can be maintained intra-operatively.
Adequate fluoroscopic C-arm access and a clear understanding of optimal projections (AP, Inlet, Outlet, and often a lateral sacral view for sacral screws) are indispensable for all percutaneous and many open approaches.
Detailed Surgical Approach / Technique
Surgical fixation of pelvic ring fractures aims to restore anatomical alignment, provide stable fixation, and allow for early mobilization. The specific approach and technique depend heavily on the fracture classification, associated injuries, and surgeon preference.
General Principles of Fixation:
1.
Resuscitation First:
Ensure hemodynamic stability.
2.
Restore Posterior Stability First:
For unstable fractures (Tile B/C, Young-Burgess VS/APC II/III), posterior ring fixation is generally prioritized as it is the primary load-bearing structure and crucial for overall pelvic stability.
3.
Anatomical Reduction:
Achieve as anatomical a reduction as possible, especially for weight-bearing joints.
4.
Stable Fixation:
Provide fixation robust enough to allow protected weight-bearing.
1. External Fixation:
*
Indications:
Temporary stabilization for hemorrhage control, provisional fixation for open fractures, damage control orthopedics, or definitive fixation for specific stable patterns in medically compromised patients.
*
Technique:
*
Supra-acetabular Pin Placement (Anterior Frame):
This is the most common external fixator configuration.
*
Patient Positioning:
Supine on a radiolucent table.
*
Landmarks:
Anterior superior iliac spine (ASIS).
*
Incision:
A small transverse incision (approx. 2-3 cm) 2 cm superior and 2 cm posterior to the ASIS.
*
Dissection:
Blunt dissection to the outer cortex of the ilium.
*
Pin Insertion:
A specialized supra-acetabular targeting device or freehand technique. Pins are directed medially, inferiorly, and posteriorly towards the sciatic notch, remaining within the "safe corridor" of the ilium. Fluoroscopy (inlet/outlet views) confirms intraosseous placement and avoids intrapelvic penetration. Two 5.0 mm or 6.0 mm Schanz pins are placed per side, aiming for bicortical purchase.
*
Frame Assembly:
Pins are connected anteriorly with carbon fiber rods, creating a rigid triangular frame. This compresses the anterior pelvis and indirectly helps stabilize the posterior ring.
*
C-clamp (Ganz Clamp):
Less commonly used now due to high complication rates if misapplied, but can provide rapid posterior compression. Requires fluoroscopic guidance to ensure correct iliac wing application and avoid sacral nerve root impingement. Its use is largely superseded by percutaneous iliosacral screws.
2. Anterior Internal Fixation:
*
Pubic Symphysis Diastasis:
*
Approach:
Pfannenstiel incision (bikini incision) or a lower midline infraumbilical incision.
*
Dissection:
Incise subcutaneous tissue, identify and split the linea alba. Retract the rectus abdominis muscles laterally to expose the superior aspect of the pubic symphysis. Take care to identify and ligate the superficial epigastric vessels. The bladder is often adherent posteriorly and must be protected.
*
Reduction:
Direct visualization and palpation. Reduction forceps (e.g., Farabeuf clamp) are used to compress the symphysis.
*
Fixation:
A 3.5 mm reconstruction plate or a more robust 3.5 mm symphyseal plate (e.g., a two-hole, four-hole, or six-hole plate). For highly unstable injuries or comminuted rami, two plates (superior and anterior) may be used. Screws (typically 3.5 mm cortical screws) are placed bicortically, angled slightly superiorly to avoid bladder penetration, or in an anterior-posterior direction.
*
Anterior Column / Ramus Fractures:
*
Approach:
Ilioinguinal approach for fractures involving the iliac wing, anterior column, and pubic rami.
*
Technique:
Open reduction and plate fixation along the iliopectineal line. Percutaneous screw fixation is an option for certain ramus fractures.
3. Posterior Internal Fixation:
This is the cornerstone of definitive stabilization for unstable pelvic ring fractures.
-
Iliosacral Screw Fixation (Percutaneous):
- Indications: Most common method for unstable SI joint disruption (ligamentous or avulsion), sacral fractures (Denis Zone I, II, some III), and often used in conjunction with anterior plating.
- Patient Positioning: Supine on a radiolucent table. Place a firm bolster under the ipsilateral SI joint to facilitate true inlet and outlet views, ensuring the contralateral anterior pelvic ring is not obscured.
-
Technique:
Highly reliant on precise fluoroscopic guidance.
- Entry Point: Typically starts just superior to the PSIS, lateral to the S1 foramen.
-
Guide Wire Placement:
Using multiple fluoroscopic views:
- Inlet View: Ensures the wire is not projecting anteriorly into the pelvis or posteriorly into the soft tissue. A "teardrop" view confirms depth into the sacral body.
- Outlet View: Confirms cephalad/caudal trajectory, avoiding the S1 and S2 nerve root foramina. The wire should be parallel to the S1 and S2 nerve root canals.
- AP View: Checks medial-lateral trajectory and length.
- Lateral Sacral View: Crucial for confirming depth and trajectory within the S1 or S2 vertebral body. The wire should be centered within the sacral ala.
- Screw Selection: Typically 7.0 mm or 8.0 mm partially threaded cannulated lag screws, or fully threaded cancellous screws.
-
Pathways:
- S1 Pathway: Through the ilium, across the SI joint, into the S1 vertebral body. The most common and safest.
- S2 Pathway: Through the ilium, across the SI joint, into the S2 vertebral body. Requires more caudal trajectory, higher risk of S2 nerve root injury.
- Trans-Sacral Bar/Screw: For bilateral sacral fractures, screws can cross the sacrum from one ilium to the other.
-
Safety Considerations:
Meticulous technique is essential to avoid neurological (L5, S1, S2 nerve roots) and vascular (superior gluteal artery) injury. Neuro-monitoring may be used.

-
Open Reduction and Internal Fixation (ORIF) of SI Joint:
- Indications: Primarily for irreducible SI joint dislocations, large unstable posterior iliac wing fractures, comminuted SI joint fractures, or when percutaneous fixation is not feasible/successful.
- Approach: Posterior approach (e.g., modified Gibson or Kocher-Langenbeck). Involves splitting the gluteus maximus, reflecting it to expose the posterior ilium, and dissecting down to the SI joint. Care is taken to identify and protect the superior gluteal neurovascular bundle.
- Reduction: Direct visualization, use of clamps, bone hooks, or a Schanz pin in the ilium as a joystick.
- Fixation: Tension band plating (e.g., a 3.5 mm reconstruction plate spanning the posterior ilium and sacrum) or lag screws placed under direct visualization.
-
Sacral Fractures (ORIF):
- Indications: Displaced Denis Zone II (foraminal) or Zone III (central canal) sacral fractures, U-type or H-type sacral fractures, especially with neurological deficits.
- Approach: Posterior midline incision, often extending to expose the entire sacrum.
- Dissection: Incise through the lumbodorsal fascia, reflect paraspinal muscles. Careful identification of the sacral anatomy and neurological structures.
- Reduction: Often challenging due to comminution and muscle spasm. Direct manipulation, traction.
-
Fixation:
Various constructs:
- Transverse Plating: For H-type or U-type fractures, plates are applied horizontally across the sacral ala, connecting to the ilium.
- Sacral Bars: Connect posterior iliac crests, providing compression.
- Lag Screws: For specific fracture patterns.
-
Lumbopelvic Fixation:
For highly unstable sacral fractures with spinopelvic dissociation (e.g., Young-Burgess VS or Denis Zone III with L5-S1 involvement), instrumentation from L4/L5 pedicles to the posterior ilium via S2-alar-iliac (S2AI) screws may be required. This provides rigid spinopelvic stabilization.

-
Iliac Wing Fractures:
- Approach: Depends on location and displacement. Anterior approaches (ilioinguinal) or posterior approaches (Kocher-Langenbeck or modified Gibson).
- Fixation: Plate and screw fixation, typically with 3.5 mm reconstruction plates or larger profiles if necessary.
4. Combined Anterior and Posterior Fixation:
Many unstable pelvic ring fractures (especially Tile C, Young-Burgess VS or APC III) require both anterior and posterior fixation to achieve adequate stability. The sequence is typically posterior fixation first, followed by anterior fixation, as posterior stability is paramount.
Complications & Management
Pelvic ring fractures are associated with a high rate of severe complications, both early and late, reflecting the high energy of the injury and the complex anatomy of the region.
Early Complications:
-
Hemorrhage:
- Incidence: The leading cause of mortality (up to 20%), occurring in a significant percentage of unstable pelvic ring injuries. Primarily venous (80-90%) from the presacral venous plexus, but arterial injury (10-20%, often superior gluteal, obturator, internal pudendal arteries) carries higher immediate mortality.
-
Management:
- ATLS resuscitation: Aggressive fluid and blood product replacement.
- Mechanical stabilization: Pelvic binder, external fixator (supra-acetabular) for volume reduction and tamponade.
- Angioembolization: For arterial bleeding, performed by interventional radiology.
- Pre-peritoneal packing: Surgical approach to tamponade venous bleeding in the retroperitoneum.
- REBOA: As a temporary measure in profound shock.
-
Neurological Injury:
- Incidence: 10-50%, most commonly involving the lumbosacral plexus (L5, S1-S4 nerve roots). Etiology includes direct trauma (fracture fragment impingement), stretch injury, hematoma, or iatrogenic injury during screw placement or retraction.
-
Management:
- Meticulous reduction: Restore anatomical alignment to decompress neural structures.
- Careful surgical technique: Precise screw placement under fluoroscopic or navigated guidance, avoiding nerve roots.
- Nerve exploration/decompression: If a specific nerve root is clearly entrapped or lacerated.
- Post-operative monitoring: Serial neurological exams.
-
Urogenital Injury:
- Incidence: 5-20%. Urethral disruption (more common in males with APC injuries), bladder rupture (intraperitoneal with full bladder at impact, extraperitoneal with direct bony fragment injury), vaginal lacerations, rectal tears.
-
Management:
- Pre-operative diagnosis: Retrograde urethrogram (RUG) for suspected urethral injury; cystogram for suspected bladder injury.
- Urology/Colorectal surgery consult: For definitive repair (e.g., suprapubic cystostomy for urethral tears, bladder repair, colostomy for rectal injuries).
-
Infection:
- Incidence: 2-10% (higher in open fractures, up to 50%).
- Management: Aggressive debridement, thorough irrigation, intravenous antibiotics, negative pressure wound therapy (VAC), staged closure, removal of hardware if persistent.
-
Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: DVT 10-20%, PE 1-5%. High risk due to hypercoagulability of trauma, immobility, and pelvic venous plexus injury.
- Management: Aggressive prophylactic measures: pharmacologic (low molecular weight heparin, fondaparinux) and mechanical (sequential compression devices). Early mobilization.
-
Malunion / Nonunion:
- Incidence: 5-15%, higher with inadequate reduction or unstable fixation.
- Management: Revision surgery, osteotomy with bone grafting, or chronic pain management depending on symptoms.
Late Complications:
-
Chronic Pelvic Pain:
- Incidence: 20-50%, debilitating for many patients. Multifactorial: malunion, SI joint arthritis, nerve injury, psychological factors.
- Management: Multidisciplinary approach involving pain specialists, physical therapists, pharmacological management, nerve blocks, psychological support.
-
Sexual Dysfunction:
- Incidence: Up to 50% in males (erectile dysfunction, ejaculatory difficulties), less reported in females. Due to pudendal nerve injury, vascular compromise, psychological trauma.
- Management: Urology consultation, counseling, pharmacological interventions.
-
Sacroiliac Arthrosis / Post-traumatic Arthritis:
- Incidence: 10-30% after SI joint disruption or fracture.
- Management: Conservative (NSAIDs, injections), physical therapy. In refractory cases, SI joint fusion may be considered, but it is rare.
-
Heterotopic Ossification (HO):
- Incidence: 5-15%, more common after extensive anterior approaches (e.g., ilioinguinal).
- Management: Prophylaxis (NSAIDs, radiation therapy) in high-risk patients. Surgical excision if symptomatic and mature.
-
Leg Length Discrepancy (LLD):
- Incidence: Can occur with significant vertical displacement malunion.
- Management: Shoe lifts for minor LLD, surgical correction (e.g., femoral shortening/lengthening) for severe cases.
-
Chronic Instability:
- Incidence: Rare if initially adequately fixed, but can occur with hardware failure or nonunion.
- Management: Revision surgery, re-fixation, bone grafting.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (approx.) | Management / Salvage Strategy |
|---|---|---|
| Hemorrhage | High (Mortality up to 20%) | ATLS, Binder, Ex-Fix, Angioembolization, Pre-peritoneal packing |
| Neurological Injury | 10-50% (Sacral roots) | Meticulous reduction, decompression, precise screw placement, neurolysis, post-op monitoring |
| Urogenital Injury | 5-20% | RUG, Cystogram, Urology/Colorectal consult, primary repair, diversion |
| Infection | 2-10% (Higher in open) | Debridement, IV antibiotics, wound VAC, staged closure, hardware removal |
| DVT/PE | 10-20% / 1-5% | Pharmacologic & mechanical prophylaxis, early mobilization |
| Malunion/Nonunion | 5-15% | Revision ORIF, osteotomy, bone grafting, chronic pain management |
| Chronic Pelvic Pain | 20-50% | Multidisciplinary pain management, PT, nerve blocks, psychological support |
| Sexual Dysfunction | 20-50% (Males) | Urology consult, counseling, pharmacological agents |
| SI Joint Arthrosis | 10-30% | NSAIDs, injections, PT, fusion (rare) |
| Heterotopic Ossification | 5-15% (Anterior) | Prophylaxis (NSAIDs/radiation), surgical excision (if symptomatic) |
| Leg Length Discrepancy | Variable, with malunion | Shoe lift, surgical correction (osteotomy) |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to maximizing functional outcomes and mitigating long-term disability following pelvic ring fracture fixation. Protocols are individualized based on the stability of the fixation, the nature of the injury, bone quality, and patient comorbidities.
General Goals:
* Control pain and swelling.
* Prevent complications (DVT, skin breakdown, stiffness).
* Protect the surgical repair while promoting fracture healing.
* Restore muscle strength, range of motion, and endurance.
* Facilitate a safe return to pre-injury function and activities.
Weight-Bearing Status:
This is the most critical component of post-operative management and is strictly dictated by the surgeon based on the stability of fixation.
*
Stable Fractures (Non-Operative or Minimally Fixed Tile A/Young-Burgess LC I/APC I):
Generally progressive weight-bearing as tolerated.
*
Operatively Fixed Stable Fractures (e.g., Pubic Symphysis Plating for APC I/II):
Often toe-touch weight-bearing (TTWB) or partial weight-bearing (PWB) on the affected side for 6-8 weeks, progressing to full weight-bearing (FWB) once radiographic signs of healing are evident.
*
Unstable Fractures with Definitive Fixation (Tile B/C, Young-Burgess VS/APC III/LC II/III):
Typically non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) on the injured side for 8-12 weeks. This extended period allows for sufficient bony or ligamentous healing at the posterior pelvic ring, which bears significant load. Progression to PWB and then FWB is determined by radiographic evidence of healing and clinical stability.
*
High-Risk Fixation (e.g., osteoporotic bone, comminuted fractures):
May require extended NWB protocols (up to 3-4 months).
*
Lumbopelvic Fixation:
Usually allows for earlier protected weight-bearing due to the rigidity of the construct.
Physical Therapy Phases:
Phase I: Acute/Protection Phase (Weeks 0-6/8)
*
Focus:
Pain control, wound care, basic mobility, complication prevention.
*
Activities:
*
Bed mobility:
Log rolling, proper transfer techniques (supine to sit).
*
Positioning:
Frequent position changes to prevent pressure sores.
*
Range of Motion (ROM):
Gentle, active-assisted or passive ROM of hips and knees within pain limits, avoiding extremes of motion that stress the pelvic ring. Emphasis on non-weight-bearing hip flexion, abduction, and rotation.
*
Strengthening:
Gentle isometric contractions of gluteal muscles, quadriceps, and abdominal muscles, without causing pain or strain to the pelvic ring.
*
Respiratory care:
Deep breathing exercises, incentive spirometry.
*
Weight-Bearing:
Strict adherence to surgeon-prescribed NWB/TDWB/TTWB. Gait training with assistive devices (walker, crutches) on flat surfaces, emphasizing proper technique.
*
Patient Education:
Reinforce weight-bearing restrictions, warning signs of infection or DVT, proper use of assistive devices.
Phase II: Transition/Early Strengthening Phase (Weeks 6/8-12)
*
Focus:
Gradual increase in weight-bearing, controlled strengthening, improved balance.
*
Activities:
*
Weight-Bearing:
Progress from TDWB/TTWB to PWB, gradually increasing load as tolerated and as per surgeon's protocol, often using bathroom scales to gauge weight.
*
Gait Training:
Progress from walker to crutches, focusing on normalized gait pattern.
*
Strengthening:
* Initiate light closed-chain exercises (e.g., wall slides, mini-squats with support) if PWB.
* Open-chain hip and knee strengthening (hip abduction, extension, knee flexion/extension) with light resistance.
* Core stability exercises (e.g., pelvic tilts, abdominal bracing) to support the spine and pelvis.
* Stationary cycling with minimal resistance.
*
Balance and Proprioception:
Standing balance exercises with support.
*
Scar Massage:
To improve tissue mobility and reduce adhesions.
Phase III: Advanced Strengthening/Functional Phase (Weeks 12+)
*
Focus:
Restoration of full strength, endurance, agility, and return to specific activities.
*
Activities:
*
Weight-Bearing:
Progression to FWB if cleared by surgeon based on radiographic healing.
*
Strengthening:
Advanced progressive resistance exercises for hip, knee, and core musculature. Integration of multi-planar movements.
*
Functional Training:
Agility drills, plyometrics (if appropriate), sport-specific exercises for athletes.
*
Endurance Training:
Increased duration and intensity of cardiovascular exercises.
*
Balance:
Advanced balance exercises, single-leg stance.
*
Return to Activity:
Gradual return to work, recreational activities, and sports, typically 6-12 months post-injury, depending on the severity of the fracture and patient progress. Impact activities are generally restricted until complete healing and full strength are achieved.
Monitoring and Adjustments:
Regular clinical follow-up with the orthopedic surgeon is essential, including serial radiographs to monitor fracture healing. The rehabilitation protocol is adjusted based on pain levels, clinical stability, radiographic progress, and individual patient tolerance. A multidisciplinary approach involving physical therapists, occupational therapists, and pain management specialists optimizes long-term outcomes.
Summary of Key Literature / Guidelines
The management of pelvic ring fractures has evolved significantly with advancements in imaging, surgical techniques, and a deeper understanding of pelvic biomechanics. Current guidelines and literature emphasize a structured, multidisciplinary approach to optimize patient outcomes.
1. Classification Systems and Decision-Making:
The utility of classification systems such as
Tile (stability-based)
,
Young-Burgess (mechanism-based)
, and
AO/OTA (comprehensive)
is well-established. These systems provide a common language for describing injuries, guiding prognostic discussions, and informing treatment algorithms. Consensus guidelines, particularly from the Orthopaedic Trauma Association (OTA), reinforce the importance of these classifications in determining mechanical stability and, consequently, the need for operative fixation. For instance, Young-Burgess classifications of APC II/III, LC II/III, and VS are consistently linked to mechanical instability requiring surgical intervention.
2. Hemorrhage Control:
Prompt control of hemorrhage remains paramount in reducing mortality. A landmark study by Hauser et al. (2006) highlighted that uncontrolled hemorrhage is the leading cause of death in severe pelvic trauma. The "pelvic resuscitation" paradigm, involving early application of a
pelvic binder
,
external fixation
(supra-acetabular pins), and adjunctive
angioembolization
or
pre-peritoneal packing
, is supported by numerous studies and adopted by ATLS protocols. Cothren et al. (2007) demonstrated improved survival with selective angioembolization in hemodynamically unstable patients. The Eastern Association for the Surgery of Trauma (EAST) guidelines strongly recommend pelvic binders and early angiography for persistent instability.
3. Timing of Definitive Fixation (Damage Control Orthopedics - DCO):
The concept of DCO, where initial temporary stabilization is followed by definitive fixation once the patient is physiologically optimized, is critical for severely injured patients. Pape et al. (2009) demonstrated that delayed definitive fixation (within 3-10 days) in polytraumatized patients, after resolution of the "second hit" inflammatory response, can reduce complications like ARDS and multi-organ failure. For stable patients, early definitive fixation within 24-72 hours is often preferred to facilitate earlier mobilization and potentially reduce complications like DVT.
4. Importance of Posterior Ring Fixation:
Consistently, literature emphasizes that the posterior pelvic ring is the primary weight-bearing structure. Unstable fractures require robust posterior fixation to restore stability. Routt et al. (1995, 2011) extensively published on the technique and safety of
percutaneous iliosacral screw fixation
, which has become the gold standard for many unstable posterior injuries due to its minimally invasive nature and high biomechanical stability. Biomechanical studies (e.g., Kim et al., 2005) confirm that proper iliosacral screw placement provides superior stability compared to anterior plating alone for vertically unstable injuries. Open reduction and internal fixation (ORIF) for the posterior ring (e.g., SI joint plating or lumbopelvic fixation) are reserved for cases of irreducible displacement, complex sacral fractures, or spinopelvic dissociation where percutaneous techniques are insufficient.
5. Role of Anterior Fixation:
Anterior fixation, typically via
pubic symphysis plating
, is crucial for rotational stability in APC II/III injuries and to anatomically restore the anterior ring. While anterior fixation alone does not provide vertical stability, it is often complementary to posterior fixation in combined unstable patterns.
6. Outcomes and Complications:
Long-term outcomes following pelvic ring fractures are variable. Studies consistently report a high incidence of
chronic pelvic pain
(up to 50%) and
sexual dysfunction
(up to 50% in males) even after anatomically successful fixation (Gill et al., 2006; Bircher et al., 2007). Neurological deficits, particularly involving the lumbosacral plexus, are a persistent concern, with rates varying widely depending on the injury pattern (Denis Zone II/III sacral fractures carry highest risk). The importance of detailed pre-operative CT imaging and meticulous surgical technique to prevent iatrogenic nerve injury is repeatedly stressed. Post-traumatic arthritis of the SI joint is also a recognized long-term sequela.
7. Rehabilitation:
Evidence supports early, controlled mobilization within the limits of fixation stability. Protocols emphasizing protected weight-bearing (often NWB or TDWB for 8-12 weeks for unstable patterns) and progressive strengthening are crucial for functional recovery and reducing secondary complications like DVT and stiffness.
Future Directions:
Ongoing research focuses on refining surgical techniques, including computer navigation and robotic assistance for more precise screw placement, and optimizing individualized rehabilitation protocols. Advances in non-invasive imaging and monitoring may further enhance early diagnosis and management of associated injuries. The continued emphasis on a multidisciplinary team approach remains a cornerstone of best practice.
You Might Also Like