Diaphyseal Tibial Fractures: What You Must Know for Recovery

Key Takeaway
For anyone wondering about Diaphyseal Tibial Fractures: What You Must Know for Recovery, Diaphyseal tibial fractures are the most common long bone fracture. Diagnosis is confirmed by plain radiographs of the tibia and adjacent joints. Treatment is generally operative, primarily involving intramedullary nailing. However, external fixation or open reduction internal fixation (ORIF) may be more appropriate in rare cases, depending on the specific location and orientation of the fracture.
Diaphyseal Tibial Fractures: What You Must Know for Recovery
Diaphyseal tibial fractures represent the most common long bone fracture, posing significant challenges in management due to the tibia's subcutaneous location, variable soft tissue envelope, and high incidence of associated complications. A thorough understanding of their diagnosis, treatment, and prognosis is paramount for orthopedic surgeons.
Summary
Diagnosis is primarily confirmed by plain radiographs of the tibia, encompassing the adjacent knee and ankle joints. The prevailing treatment standard for displaced diaphyseal tibial fractures is intramedullary (IM) nailing. However, external fixation or open reduction and internal fixation (ORIF) may be more appropriate in specific scenarios, contingent on fracture morphology, location, soft tissue status, and patient factors. A meticulous pre-operative assessment and adherence to sound surgical principles are critical for optimizing outcomes and mitigating complications.
Introduction & Epidemiology
Diaphyseal tibial fractures are a frequent occurrence, accounting for approximately 17% of all lower extremity fractures and 4% of all fractures within the Medicare population. These fractures exhibit a bimodal distribution: high-energy mechanisms typically affect younger, active individuals, while falls or lower-energy mechanisms are more prevalent in older patients, often associated with osteopenia or osteoporosis. Males demonstrate a higher incidence than females across most age groups.
Etiology and Pathophysiology
Diaphyseal tibial fractures arise from a spectrum of traumatic forces. Low-energy mechanisms commonly result in spiral fracture patterns, frequently accompanied by a fibula fracture at a different level, indicative of a torsional injury. High-energy mechanisms, such as motor vehicle collisions or falls from height, typically lead to wedge or short oblique fracture patterns. These are often characterized by significant comminution, substantial displacement, and more severe concomitant soft tissue injury, reflecting greater energy dissipation at the fracture site. The extent of soft tissue compromise is a critical determinant of treatment strategy and prognosis, particularly in open fractures.
Associated Conditions
The energy imparted during injury can result in several critical associated conditions:
*
Soft Tissue Injury:
Ranging from simple abrasions to extensive degloving injuries, often complicated by local tissue necrosis or infection. Open fractures require meticulous debridement and management based on the Gustilo-Anderson classification.
*
Compartment Syndrome:
A limb-threatening condition demanding prompt recognition and emergent fasciotomy. The enclosed fascial compartments of the leg are highly susceptible, particularly after high-energy trauma or reperfusion injury.
*
Bone Loss:
Severe comminution or open injuries can result in segmental bone defects, necessitating advanced reconstructive techniques.
*
Ipsilateral Skeletal Injury:
"Floating knee" injuries (ipsilateral femoral and tibial fractures) are high-energy events associated with severe soft tissue compromise and high complication rates. Other ipsilateral injuries may include patellar fractures, ankle fractures, or fibular head dislocations.
*
Neurovascular Injury:
Direct trauma or fracture displacement can injure the superficial peroneal, deep peroneal, or tibial nerves, or the major arteries and veins of the leg. Vascular compromise is an orthopedic emergency.
*
Systemic Trauma:
In polytrauma patients, diaphyseal tibial fractures are often one component of a broader injury pattern, requiring prioritization and damage control orthopedic principles.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the leg's anatomy and the biomechanics of the tibia is fundamental to both surgical planning and execution.
Osteology
The
tibia
is the primary weight-bearing bone of the lower leg. Its diaphysis is triangular in cross-section proximally, becoming more rounded distally. Key anatomical features include:
*
Anterior Border (Tibial Crest):
A prominent, subcutaneous ridge that serves as a critical landmark but leaves the medial aspect of the tibia vulnerable to open injuries.
*
Medial Surface:
Largely subcutaneous, increasing the risk of infection and delayed healing in open fractures.
*
Interosseous Membrane:
Connects the tibia and fibula, providing stability and separating the anterior from the posterior compartments. Injury to this membrane can destabilize the tibiofibular syndesmosis.
*
Nutrient Foramen:
Typically located on the posterior surface, supplying the major blood supply to the diaphyseal cortex. Disruption of this blood supply, particularly with reaming, can impact fracture healing.
The
fibula
is a non-weight-bearing bone but is crucial for muscle attachment and ankle stability. Its integrity and relationship to the tibia should always be assessed, as isolated fibula fractures, or fibula fractures at a different level to the tibia, can influence torsional stability and reduction.

Musculature and Compartments
The leg is divided into four distinct fascial compartments by the interosseous membrane and fascial septa, each containing specific muscles, nerves, and vessels:
*
Anterior Compartment:
Tibialis anterior, extensor digitorum longus, extensor hallucis longus, fibularis (peroneus) tertius. Innervated by the deep fibular (peroneal) nerve. Contains the anterior tibial artery. Actions: dorsiflexion, toe extension.
*
Lateral Compartment:
Fibularis (peroneus) longus and brevis. Innervated by the superficial fibular (peroneal) nerve. Actions: eversion, plantarflexion.
*
Superficial Posterior Compartment:
Gastrocnemius, soleus, plantaris. Innervated by the tibial nerve. Contains the sural nerve. Actions: plantarflexion.
*
Deep Posterior Compartment:
Tibialis posterior, flexor digitorum longus, flexor hallucis longus. Innervated by the tibial nerve. Contains the posterior tibial artery and fibular artery. Actions: plantarflexion, inversion, toe flexion.
Swelling within these rigid compartments, particularly after high-energy trauma, can lead to compartment syndrome, compressing nerves and vessels.
Neurovasculature
Major neurovascular structures at risk during tibial fracture surgery include:
*
Peroneal Nerve (Common Fibular Nerve):
Wraps around the fibular neck, making it vulnerable during proximal fibular manipulation or external fixation pin placement. Divides into superficial and deep branches.
*
Tibial Nerve:
Runs through the deep posterior compartment.
*
Anterior Tibial Artery:
Travels with the deep fibular nerve in the anterior compartment.
*
Posterior Tibial Artery and Peroneal Artery:
Supply the posterior and lateral compartments, respectively.
Careful dissection and awareness of these structures are essential to prevent iatrogenic injury.
Biomechanics
The tibia is subjected to complex loading patterns including axial compression, bending, and torsion.
*
Axial Loading:
Primarily borne by the tibia, especially when the fibula is intact.
*
Torsional Forces:
Lead to spiral fracture patterns. The fibula plays a role in resisting torsional stress.
*
Bending Moments:
Result in transverse or short oblique fractures.
Intramedullary nailing transforms the tibia into a load-sharing construct, meaning the bone and the implant share the load. This promotes callus formation and secondary bone healing. In contrast, plate fixation is typically a load-bearing construct, which can lead to stress shielding. The choice of implant and fixation technique must consider these biomechanical principles to optimize healing and minimize complications.
Indications & Contraindications
The decision-making process for diaphyseal tibial fractures involves careful consideration of fracture characteristics, soft tissue status, patient comorbidities, and surgeon experience.
Operative Indications
Surgical management is generally indicated for:
*
Displaced, Unstable Fractures:
* Greater than 5-10 degrees of angulation in any plane (varus/valgus, apex anterior/posterior).
* Greater than 1-2 cm of shortening.
* Greater than 50% displacement of cortical width.
* Rotationally unstable fractures.
*
Open Fractures (Gustilo-Anderson Type I-III):
After urgent debridement and irrigation, internal fixation is typically recommended to stabilize the limb and facilitate soft tissue management.
*
Polytrauma Patients:
Early stabilization (within 24 hours) of major long bone fractures is a cornerstone of damage control orthopedics, reducing systemic inflammatory response and improving patient outcomes.
*
Segmental Fractures:
Often inherently unstable and prone to nonunion.
*
Pathologic Fractures:
Requires stabilization and often biopsy.
*
Associated Vascular Injury:
After vascular repair, internal fixation provides a stable skeletal framework.
*
Floating Knee Injuries:
Require stabilization of both femoral and tibial components.
*
Failure of Non-Operative Treatment:
Progressive displacement, persistent pain, or impending skin compromise.
*
Soft Tissue Compromise:
When casts or splints are intolerable or risk further skin breakdown (e.g., severe burns).
Non-Operative Indications
Non-operative management may be considered for:
*
Minimally Displaced, Stable Closed Fractures:
Especially non-displaced spiral or transverse fractures with good alignment maintained in a cast or brace. Regular radiographic follow-up is crucial.
*
Medically Unstable Patients:
If the patient's comorbidities preclude safe surgical intervention, non-operative management (e.g., external fixator as a temporizing measure, or casting) may be chosen until medical optimization.
*
Pilon Extension:
Significant articular extension into the ankle joint (pilon fracture component) is generally a relative contraindication for primary IM nailing without addressing the articular component.
Contraindications to Intramedullary Nailing
- Active Local Infection: A relative contraindication. Aggressive debridement and antibiotics, potentially followed by external fixation, may be necessary before considering IM nailing.
- Significant Articular Extension: Fractures extending substantially into the knee or ankle joint often require adjunctive fixation (e.g., plates and screws) for precise articular reduction, or a different primary implant if the articular component is dominant. IM nailing primarily addresses the diaphysis.
- Extremely Narrow Medullary Canal: If the canal is too small to accommodate even the smallest available nail, or if reaming is considered unsafe.
- Skeletal Immaturity with Open Physes: A relative contraindication due to risk of physeal arrest. Smaller diameter nails or alternative fixation (plates, external fixators) may be used.
- Uncontrolled Soft Tissue Compromise: In certain open fractures with extensive contamination or devitalized tissue, initial external fixation may be preferred prior to definitive IM nailing.
Table: Operative vs. Non-Operative Indications for Diaphyseal Tibial Fractures
| Feature | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | >5-10° angulation, >1-2 cm shortening, >50% cortical disp. | Minimally displaced, stable, good alignment on films |
| Fracture Pattern | Comminuted, segmental, highly unstable | Non-displaced spiral, stable transverse |
| Soft Tissue Status | Open fractures (Gustilo-Anderson I-III), Compartment Syndrome | Closed, intact skin, minimal swelling (suitable for cast) |
| Associated Injuries | Polytrauma, vascular injury, floating knee | Isolated, non-displaced fracture in stable patient |
| Patient Factors | Young, active patient, high functional demands | Medically frail, non-ambulatory, low functional demands |
| Failure of Conservative | Progressive displacement, pain, skin compromise | Initial successful non-operative trial |
| Specific Contraindications to IMN | Active infection, significant articular extension, narrow canal | N/A (IMN is the operative choice) |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to anticipating challenges and ensuring a successful outcome.
Pre-Operative Planning
-
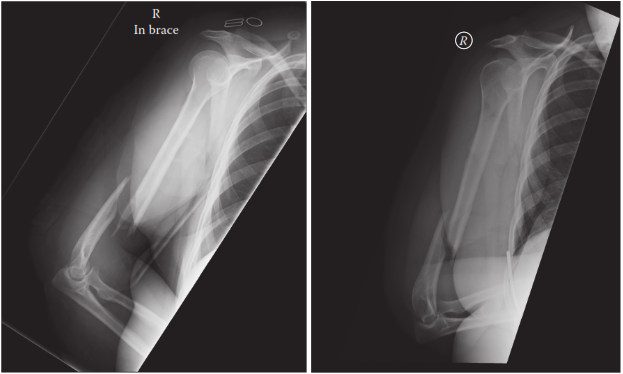
Imaging Review:
- Plain Radiographs: AP and lateral views of the entire tibia, including the knee and ankle joints, are essential to assess fracture morphology, displacement, comminution, and articular involvement. Views of the contralateral leg can aid in templating nail length and diameter.
- Computed Tomography (CT) Scan: Indicated for complex fracture patterns, articular extension, or when assessing comminution and bone loss. It helps delineate entry points and identify blocking screw placements.
- Angiography: Performed if vascular injury is suspected.
- Gustilo-Anderson Classification: For open fractures, a precise classification guides debridement timing, antibiotic choice, and initial wound management.
-
Timing of Surgery:
- Emergent: Open fractures (within 6 hours ideal), compartment syndrome, acute vascular compromise.
- Urgent (24-72 hours): Most closed fractures, especially in polytrauma patients (damage control orthopedics). Delaying surgery can allow for soft tissue swelling resolution but prolonged delay increases risk of nonunion.
- Antibiotics & Tetanus Prophylaxis: Standard for all open fractures, prophylactic for closed.
- Tourniquet: Optional. Can reduce blood loss and improve visualization, but has potential for nerve injury and reperfusion issues.
- Implant Selection: Determine nail diameter and length based on templating and intraoperative measurements. Consider reamed vs. unreamed nailing, static vs. dynamic locking.
- Reduction Strategy: Pre-plan how the fracture will be reduced (e.g., traction, manipulation, external fixator as a reduction tool, blocking screws).
Patient Positioning
The patient is typically positioned supine on a radiolucent operating table, allowing for fluoroscopic imaging in both AP and lateral planes.
*
Fracture Table:
Provides continuous longitudinal traction, which can aid in reduction and maintain length. The knee can be flexed to 90 degrees (for infrapatellar entry) or maintained in a semi-extended position (for suprapatellar entry).
*
Free-Leg Technique:
The uninjured leg is placed in a well-padded leg holder, while the injured leg is draped free. This allows for manual traction and manipulation, and easier adjustment of knee flexion. A bump under the ipsilateral buttock may be used to internally rotate the leg and aid in infrapatellar entry.
*
Image Intensifier (C-arm) Setup:
The C-arm must be positioned to allow unobstructed AP and lateral views of the entire tibia and the entry point without repositioning the patient or the injured limb.
Detailed Surgical Approach / Technique: Reamed Intramedullary Nailing
Intramedullary nailing is the gold standard for most diaphyseal tibial fractures. This section outlines the general technique for reamed IM nailing.
1. Debridement (for Open Fractures)
For open fractures, meticulous debridement of all devitalized tissue and thorough irrigation are performed prior to internal fixation. This may involve serial debridements.
2. Incisions and Entry Point
The choice of entry point and incision depends on surgeon preference and fracture characteristics (e.g., very proximal or distal fractures may favor suprapatellar).
Infrapatellar Entry (Standard Technique)
- Incision: A 3-5 cm longitudinal incision is made over the patellar tendon, slightly medial or lateral to the midline. Alternatively, a medial parapatellar incision can be used.
- Approach: The patellar tendon is either split longitudinally, or a medial parapatellar approach is utilized to expose the intercondylar notch. Care is taken to avoid damage to the patellar tendon and fat pad.
- Entry Portal: The entry portal is created in the intercondylar notch, slightly medial to the lateral tibial spine, in line with the intramedullary canal on both AP and lateral views. It should be centered anterior-posteriorly, just anterior to the articular cartilage. An awl or drill is used to open the cortex.
Suprapatellar Entry
- Incision: A small longitudinal incision (2-3 cm) is made superior to the patella, either in the midline or slightly medial.
- Approach: A specific suprapatellar portal is used, passing through the quadriceps tendon and into the intercondylar notch. A guide sleeve and trocar protect the patellofemoral joint cartilage.
- Entry Portal: Similar to infrapatellar, aiming to align with the medullary canal.
- Advantages: Allows for a semi-extended knee position, which can aid in reduction of proximal and distal fractures, potentially reduces knee pain compared to infrapatellar approaches.
- Disadvantages: Requires specialized instrumentation, potential for chondral injury to the patella or trochlea.
3. Guidewire Placement
- A ball-tipped guidewire is carefully inserted through the entry portal and advanced down the medullary canal, across the fracture site, and into the distal metaphysis.
- Reduction: During guidewire insertion, the fracture must be reduced. This may require manual traction, manipulation, or temporary external fixation. Fluoroscopy is used to confirm reduction and guidewire position in both AP and lateral planes.
- Central Position: The guidewire should be centrally located within the canal in both views at all times to prevent iatrogenic malalignment (e.g., apex anterior/posterior angulation or valgus/varus) and cortical impingement.
4. Reaming
- A flexible reamer is advanced over the guidewire. Sequential reaming is performed with increasing reamer sizes, typically in 0.5 or 1.0 mm increments.
- Reaming Diameter: The canal is typically over-reamed by 1.0-1.5 mm beyond the chosen nail diameter. This creates space for the nail, increases cortical contact, and allows for larger diameter nails, which are biomechanically stronger.
- Benefits of Reaming: Increased nail-bone contact, improved secondary stability, biological stimulation of healing by introducing bone marrow elements and growth factors.
- Risks of Reaming: Heat necrosis, potential for fat embolism, iatrogenic comminution, increased blood loss. Unreamed nailing may be considered in cases of severe soft tissue injury or significant systemic compromise to minimize these risks.
5. Nail Insertion
- After adequate reaming, the selected intramedullary nail is attached to the insertion handle/jig.
- The nail is carefully inserted over the guidewire, through the entry portal, and slowly advanced down the medullary canal.
- Careful Insertion: Forceful insertion should be avoided to prevent iatrogenic fracture or propagation. Rotational alignment should be continuously assessed.
- Final Position: The nail should be inserted so that its proximal end is flush with or slightly below the articular surface, minimizing hardware prominence. Its distal tip should be adequately seated in the distal metaphysis but not impinging on the ankle joint.
6. Proximal Locking
- Using a dedicated jig attached to the insertion handle, proximal locking screws are inserted bicortically.
- Static vs. Dynamic Locking: Two screws provide static locking, preventing both rotation and shortening. One screw provides dynamic locking, allowing for controlled axial micromotion which can stimulate healing, but provides less rotational stability. Static locking is preferred initially for most diaphyseal fractures.
- Verification: Fluoroscopy confirms screw position and bicortical purchase.
7. Distal Locking
- Distal locking is crucial for preventing rotational instability and maintaining length. This is often the most challenging step.
-
Techniques:
- Jig-assisted: Some nail systems offer distal locking jigs, but these are often less accurate than proximal jigs due to the length of the nail.
- Freehand Technique (Perfect Circle Technique): The C-arm is positioned perpendicular to the nail and rotated until a perfect circle (end-on view) of the screw hole is visualized. A drill is then advanced through a small incision down the center of the circle to achieve bicortical purchase.
- Number of Screws: Typically, two distal screws are used for static locking.
- Verification: AP and lateral fluoroscopic views confirm screw length and bicortical purchase.
8. Reduction Aids
For difficult reductions, various techniques can be employed:
*
Manual Traction and Manipulation:
Performed by an assistant or utilizing the fracture table.
*
External Fixator:
A temporary external fixator can be applied to aid in length restoration, de-rotation, and alignment before nail insertion.
*
Blocking Screws (Poller Screws):
Small-diameter screws placed eccentrically in the metaphysis adjacent to the entry point or distal to the fracture, used to "steer" the guidewire and nail into a desired position, particularly useful for reducing apex anterior/posterior or valgus/varus malalignment in metaphyseal extensions or difficult reductions.
*
Lag Screws Through Nail:
For long oblique or spiral fractures, a lag screw can be placed through the nail itself, after reduction, to achieve interfragmentary compression, providing additional stability.
9. Wound Closure
Once satisfactory fixation is confirmed, the incisions are irrigated, and layered closure is performed. Skin staples or sutures are used for the skin.
Complications & Management
Diaphyseal tibial fractures are associated with a relatively high rate of complications, even with optimal surgical management. Proactive anticipation and prompt management are crucial.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|
Nonunion/Delayed Union
| 5-30% | Dynamization (if fixed locked), exchange nailing, bone grafting (autograft/allograft with rhBMP-2), plate augmentation, fibular osteotomy, pulsed electromagnetic field (PEMF) stimulation. |
|
Malunion
| 5-15% | Corrective osteotomy (if symptomatic and significant angulation/rotation). |
|
Infection
| 1-5% (closed), 10-30% (open)| Debridement, irrigation, targeted antibiotics, implant retention (if stable union) vs. removal and external fixation (if unstable/persistent infection), soft tissue coverage. |
|
Compartment Syndrome
| 1-5% | Emergency fasciotomy. |
|
Hardware Irritation/Prominence
| 10-20% | Hardware removal (after fracture union). |
|
Vascular/Nerve Injury
| <1% | Exploration, repair (vascular), nerve grafting/repair (if indicated), rehabilitation. |
|
Knee Pain
| 10-50% (post-IMN) | Physical therapy, hardware removal (especially proximal screws or prominent nail entry site), steroid injection. |
|
Refracture
| 1-5% (after hardware removal) | Re-fixation with IMN or plate. |
Detailed Management Strategies
Nonunion
Defined as lack of radiographic healing after 6-9 months or progression to nonunion at any stage.
*
Aseptic Nonunion:
*
Hypertrophic:
Often due to insufficient stability. Management typically involves
exchange nailing
with a larger diameter reamed nail, which improves stability and provides a biological stimulus.
*
Atrophic:
Often due to both instability and biological deficiency. Requires
exchange nailing
and
bone grafting
(autogenous iliac crest bone graft is gold standard, or allograft/rhBMP-2). Plate augmentation may also be considered in recalcitrant cases. Fibular osteotomy can be performed to allow compression across the tibial nonunion.
*
Septic Nonunion:
Requires aggressive surgical debridement, antibiotic treatment based on culture sensitivities, and stabilization. This may involve staged procedures: initial debridement and external fixation, followed by definitive internal fixation after infection control.
Malunion
Rotation, angulation, or shortening can lead to functional impairment, pain, or arthrosis.
*
Rotational Malunion:
Clinically assessed by foot progression angle or comparison to the contralateral limb. Significant malrotation (>10-15 degrees) may require
corrective osteotomy
after union.
*
Angular Malunion:
If symptomatic and functional deficit, a
corrective osteotomy
can be performed.
*
Shortening:
Less than 1.5-2 cm is often tolerated. More significant shortening can be addressed with
lengthening osteotomy
, although this is a complex procedure.
Infection
- Superficial Infection: Managed with oral antibiotics and local wound care.
- Deep Infection: Requires urgent surgical debridement, thorough irrigation, and intravenous antibiotics. The implant may be retained if the fracture is stable, but if unstable or persistent infection, implant removal and temporary external fixation may be necessary, followed by staged reimplantation. Soft tissue coverage procedures may be required.
Compartment Syndrome
A true orthopedic emergency. Requires immediate four-compartment fasciotomy to relieve pressure and prevent irreversible muscle and nerve ischemia. Diagnosis is primarily clinical, but intracompartmental pressure monitoring can confirm suspicion.
Hardware Irritation/Prominence
Common, especially at the proximal nail entry site or with prominent distal locking screws. Removal of symptomatic hardware is indicated once the fracture is fully healed (typically 12-18 months post-op), but not earlier to prevent refracture.
Knee Pain
A frequent complaint after IM nailing, particularly with infrapatellar entry. Causes include hardware prominence, patellofemoral irritation, and adhesions. Management includes physical therapy, anti-inflammatory medications, steroid injections, and ultimately hardware removal after union.
Post-Operative Rehabilitation Protocols
Rehabilitation begins immediately post-operatively, tailored to fracture stability, fixation type, and individual patient factors. The primary goals are to preserve joint range of motion, prevent muscle atrophy, and progress to full weight-bearing and functional activity safely.
1. Weight-Bearing Progression
- Stable IM Nailing: For most stable, closed diaphyseal tibial fractures fixed with a well-locked IM nail, immediate weight-bearing as tolerated (WBAT) is often initiated. This promotes controlled axial micromotion, which is believed to stimulate fracture healing (Wolff's Law).
- Comminuted/Unstable Fractures, Open Fractures, or Specific Fixation: In cases of extensive comminution, bone loss, or an unreamed nail (less stable), a period of toe-touch weight bearing (TTWB) or partial weight bearing (PWB) may be prescribed, progressing based on radiographic signs of healing and clinical comfort.
- Duration: Full weight-bearing without assistive devices is typically achieved once there is clinical and radiographic evidence of progressive union.
2. Range of Motion (ROM)
-
Early Mobilization:
As soon as pain allows, early active and passive range of motion exercises for the knee and ankle joints are initiated.
- Knee: Flexion and extension exercises to prevent quadriceps stiffness and patellofemoral pain.
- Ankle: Dorsiflexion, plantarflexion, inversion, and eversion exercises to prevent ankle stiffness and maintain subtalar motion.
- Continuous Passive Motion (CPM): May be used for patients at high risk for stiffness, although its routine use is debated.
3. Strengthening
- Isometric Exercises: Initial focus on gentle isometric contractions of quadriceps, hamstrings, and calf muscles.
- Progressive Resistance Exercises: As healing progresses, resistance exercises are introduced to strengthen the muscles of the thigh and leg.
- Core Strengthening: Important for overall stability and balance.
4. Gait Training
- Initiated with assistive devices (walker, crutches) as weight-bearing status permits.
- Focus on achieving a normal, pain-free gait pattern.
5. Imaging Follow-up
- Regular radiographs (AP and lateral views) are obtained at intervals (e.g., 2 weeks, 6 weeks, 3 months, 6 months, 9-12 months) to monitor fracture healing, alignment, and implant integrity.
- Clinical assessment for pain, swelling, and tenderness at the fracture site correlates with radiographic findings.
6. Return to Activity
- Gradual return to recreational activities and sports is permitted once there is complete clinical and radiographic union, full strength, and restored range of motion.
- High-impact activities may be restricted for an extended period, especially after complex fractures.
7. Hardware Removal
- Hardware removal is generally elective and typically considered 12-18 months after fracture union, once the bone has fully remodeled and regained strength.
- Indications for removal include symptomatic hardware (prominence, pain), refracture through locking screw holes, or patient request.
- Risks of hardware removal include infection, nerve injury, and refracture, particularly if removed prematurely or without adequate cortical healing.
Summary of Key Literature / Guidelines
The management of diaphyseal tibial fractures has evolved with advances in surgical techniques and understanding of fracture biology.
- Intramedullary Nailing as Gold Standard: Numerous studies and meta-analyses consistently support reamed intramedullary nailing as the preferred treatment for most displaced diaphyseal tibial fractures. It offers superior union rates, lower rates of malunion, and earlier weight-bearing compared to non-operative management or plate fixation in most settings. The Arbeitsgemeinschaft für Osteosynthesefragen (AO Foundation) principles heavily advocate for IM nailing in these fractures.
- Reamed vs. Unreamed Nailing: While unreamed nailing was initially proposed to preserve periosteal blood supply, especially in open fractures, meta-analyses and large trials (e.g., the Canadian Orthopaedic Trauma Society studies) have largely demonstrated comparable union rates between reamed and unreamed techniques in closed fractures. Reamed nailing often permits a larger diameter nail, potentially providing greater mechanical stability and increasing union rates in certain complex fracture patterns, albeit with a theoretical increased risk of thermal necrosis or fat embolism. Current consensus suggests reamed nailing for most closed fractures, with unreamed reserved for specific indications like severe open fractures with extensive soft tissue damage or patients with compromised physiology.
- Open Fractures: The management of open tibial fractures is guided by the Gustilo-Anderson classification. Urgent debridement and irrigation are paramount. Early stabilization with IM nailing (often unreamed initially) or external fixation is recommended to facilitate wound care and reduce infection risk. Soft tissue coverage procedures are often necessary.
- Delayed Union and Nonunion: These remain significant challenges. Exchange nailing is a well-established and effective strategy for hypertrophic nonunions, often achieving union rates of 70-90%. For atrophic nonunions, bone grafting (autograft or allograft with biologics like rhBMP-2) in conjunction with stable fixation is often required. Dynamization (removing a single locking screw to allow axial micromotion) can be considered for delayed unions but its efficacy in established nonunion is debated.
- Knee Pain after Tibial Nailing: Studies consistently report a high incidence of anterior knee pain (10-50%) following tibial IM nailing. While many causes are multifactorial, hardware prominence and irritation of the patellar tendon or infrapatellar fat pad are common. Suprapatellar nailing techniques have shown promise in reducing knee pain in some studies, but further research is ongoing.
- Blocking Screws (Poller Screws): Evidence supports the use of blocking screws, particularly in juxta-articular or difficult-to-reduce diaphyseal fractures, to optimize alignment and reduce malunion rates by converting a wide metaphysis into a narrow one that guides the nail.
- Role of External Fixation: External fixation remains invaluable as a temporary stabilization method for complex open fractures, highly contaminated wounds, or in damage control orthopedics for polytrauma patients. It can also be used as a definitive treatment for select cases, particularly when IM nailing is contraindicated, but generally carries higher risks of pin tract infection and nonunion compared to IM nailing.
Continued research focuses on improving bone healing, reducing complications, and optimizing patient-reported outcomes following diaphyseal tibial fracture fixation. Understanding and applying these evidence-based principles are essential for contemporary orthopedic practice.
You Might Also Like