Orthopedics Hyperguide Review | Dr Hutaif General Ortho -...
14 Apr 2026
54 min read
84 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedics Hyperguide Review | Dr Hutaif Gen...
00:00
Start Quiz
Question 1High Yield
When compared with postoperative external beam radiation therapy for the treatment of soft-tissue sarcomas, preoperative radiation therapy is associated with which of the following?

Explanation
The next most appropriate step in management is to proceed with a biopsy of the most accessible site. This can be done
by the surgeon or by an interventional radiologist trained in core biopsy techniques. It is imperative to make a pathologic diagnosis prior to proceeding with any further medical, surgical, or radiation treatments. A histologic diagnosis at this point is the only way a medical oncologist can have a meaningful discussion with the patient about their disease, its natural history, and ultimately discuss treatment options and prognosis. Further imaging at this point only delays the time to histologic evaluation. Consideration of surgical stabilization can be delayed until a diagnosis is established and a multidisciplinary approach is initiated. This fracture can be treated at least temporarily with nonsurgical protected weight bearing with a walker or crutches.
Hospice may soon serve a useful role but a diagnosis must first be rendered and a limited life expectancy anticipated. Pre Res # 100 is 2
**MORE MCQS**
[ORTHO MCQS 011 FREE BANK 02](http://hutaifortho.com/878)
---
[ORTHO MCQS 011 FREE BANK](http://hutaifortho.com/877)
[Orthopedic MCQS online Hip and knee ADULT...](http://hutaifortho.com/876)
[ORTHOPEDIC MCQS OB 20 TRAUMA1](http://hutaifortho.com/875)
[ORTHOPEDIC MCQS OB 20 BASIC5](http://hutaifortho.com/874)
[ORTHOPEDIC MCQS OB 20 BASIC7](http://hutaifortho.com/873)
[ORTHOPEDIC MCQS OB 20 BASIC 6](http://hutaifortho.com/872)
[ORTHOPEDIC MCQS OB 20 BASIC 44](http://hutaifortho.com/871)
[ORTHOPEDIC MCQS OB 20 BASIC 4](http://hutaifortho.com/870)
[ORTHOPEDIC MCQS OB 20 BASIC 3](http://hutaifortho.com/869)
[ORTHOPEDIC MCQS OB 20 BASIC 2](http://hutaifortho.com/868)
[ORTHOPEDIC MCQS OB 20 BASIC 1](http://hutaifortho.com/867)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4](http://hutaifortho.com/865)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3](http://hutaifortho.com/864)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2](http://hutaifortho.com/863)
[1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW](http://hutaifortho.com/862)
[ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01](http://hutaifortho.com/861)
[ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01](http://hutaifortho.com/860)
[ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01](http://hutaifortho.com/859)
[ORTHOPEDIC MCQS BANK WITH
NATOMY 02](http://hutaifortho.com/858)
[ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02](http://hutaifortho.com/857)
[ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02](http://hutaifortho.com/856)
[ORTHOPEDIC MCQS WITH ANSWER FOOT 03](http://hutaifortho.com/855)
[ORTHOPEDIC MCQS WITH ANSWER SPINE 03](http://hutaifortho.com/854)
[ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03](http://hutaifortho.com/853)
[ORTHOPEDIC MCQS WITH ANSWER HIP 04](http://hutaifortho.com/852)
[ORTHOPEDIC MCQS WITH ANSWER PEDS 04](http://hutaifortho.com/851)
[ORTHOPEDIC MCQS WITH ANSWER SPORT 04](http://hutaifortho.com/850)
[ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05](http://hutaifortho.com/849)
[ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05](http://hutaifortho.com/848)
[ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05](http://hutaifortho.com/847)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06](http://hutaifortho.com/846)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...](http://hutaifortho.com/845)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06](http://hutaifortho.com/844)
[ORTHOPEDIC MCQS with Answers ONLINE BASIC 06](http://hutaifortho.com/843)
[ORTHOPEDIC MCQS ONLINE PEDIATRICS 07](http://hutaifortho.com/842)
[ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07](http://hutaifortho.com/841)
[ONLINE ORTHOPEDIC MCQS SPORT07](http://hutaifortho.com/840)
[ONLINE ORTHOPEDIC MCQS UPPER LIMB08](http://hutaifortho.com/839)
[ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08](http://hutaifortho.com/838)
[ONLINE ORTHOPEDIC MCQS ANATOMY08](http://hutaifortho.com/837)
[ONLINE ORTHOPEDIC MCQS FOOT0 9](http://hutaifortho.com/836)
[ONLINE ORTHOPEDIC MCQS SPINE0 9](http://hutaifortho.com/835)
[ONLINE ORTHOPEDIC MCQS TRAUMA 9](http://hutaifortho.com/834)
[Orthopedic MCQS online sports Medicine](http://hutaifortho.com/833)
[Orthopedic MCQS online Shoulder and Elbow](http://hutaifortho.com/832)
[Orthopedic MCQS online Hip and knee](http://hutaifortho.com/831)
[online orthopedic mcqs](http://hutaifortho.com/830)
[Shoulder and elbow: Mcqs AND EMQS Answers](http://hutaifortho.com/766)
[Shoulder And Elbow: Questions Mcqs AND EMQS](http://hutaifortho.com/765)
[Hand and wrist: Answers MCQS EMQS](http://hutaifortho.com/764)
[Hand and wrist: MCQ AND EMQ Questions](http://hutaifortho.com/763)
[quize](http://hutaifortho.com/729)
[KEY POINTS](http://hutaifortho.com/727)
[MIND MAP](http://hutaifortho.com/726)
[action tree](http://hutaifortho.com/725)
[action2](http://hutaifortho.com/724)
[Action](http://hutaifortho.com/723)
[patient](http://hutaifortho.com/722)
[Bop](http://hutaifortho.com/721)
[New](http://hutaifortho.com/720)
[Trial](http://hutaifortho.com/714)
[Pupup](http://hutaifortho.com/713)
[SSEE](http://hutaifortho.com/704)
[SE](http://hutaifortho.com/703)
[2021 SHOULDER AND ELBOW MCQS FREE](http://hutaifortho.com/689)
[Pediatric Orthopaedic MCQS Self-Assessment...](http://hutaifortho.com/685)
[Self-Assessment Examination 2020 Adult Spine MCQS](http://hutaifortho.com/684)
[Foot and Ankle free MCQS2020 Online](http://hutaifortho.com/681)
[UPDATED ORTHOPEDIC MCQS](http://hutaifortho.com/680)
[FREE Orthopedics MCQS 2022 1951.-2000.](http://hutaifortho.com/677)
[FREE Orthopedics MCQS 2022 1901.-1950.](http://hutaifortho.com/676)
[FREE Orthopedics MCQS 2022 1851-1900.](http://hutaifortho.com/675)
[FREE Orthopedics MCQS 2022 1751-1850..](http://hutaifortho.com/674)
[FREE Orthopedics MCQS 2022 1751-1800..](http://hutaifortho.com/673)
[Foot and Ankle FREE ORTHOPEDICS MCQS Question 11](http://hutaifortho.com/672)
[FREE Orthopedics MCQS 2022 1701-1750.](http://hutaifortho.com/668)
[FREE Orthopedics MCQS 2022 1651-1700](http://hutaifortho.com/667)
[FREE Orthopedics MCQS 2022 1601-1650.](http://hutaifortho.com/666)
[ORTHOPEDIC MCQS FREE 2023](http://hutaifortho.com/665)
[FREE Orthopedics MCQS 2022 1551-1600](http://hutaifortho.com/664)
[FREE Orthopedics MCQS 2022 1501-1550](http://hutaifortho.com/663)
[FREE Orthopedics MCQS 2022 1451-1500](http://hutaifortho.com/662)
[FREE Orthopedics MCQS 2022 1401-1450](http://hutaifortho.com/661)
[FREE Orthopedics MCQS 2022 1351 -1400](http://hutaifortho.com/660)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350](http://hutaifortho.com/659)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300](http://hutaifortho.com/658)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200](http://hutaifortho.com/656)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150](http://hutaifortho.com/655)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100](http://hutaifortho.com/654)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051](http://hutaifortho.com/653)
[ORTHOPEDICS HYPERGUIDE MCQ 951-1000](http://hutaifortho.com/652)
[ORTHOPEDICS HYPERGUIDE MCQ 901-950](http://hutaifortho.com/651)
[ORTHOPEDICS HYPERGUIDE MCQ 851-900](http://hutaifortho.com/650)
[ORTHOPEDICS HYPERGUIDE MCQ 800-850](http://hutaifortho.com/649)
[ORTHOPEDICS HYPERGUIDE MCQ 751-800](http://hutaifortho.com/647)
[ORTHOPEDICS HYPERGUIDE MCQ 701-750](http://hutaifortho.com/646)
[ORTHOPEDICS HYPERGUIDE MCQ 651-700](http://hutaifortho.com/645)
[ORTHOPEDICS HYPERGUIDE MCQ 601-650](http://hutaifortho.com/644)
[ORTHOPEDICS HYPERGUIDE MCQ 551-600](http://hutaifortho.com/643)
[ORTHOPEDICS HYPERGUIDE MCQ 501-550](http://hutaifortho.com/642)
[ORTHOPEDICS HYPERGUIDE MCQ 451-500](http://hutaifortho.com/641)
[ORTHOPEDICS HYPERGUIDE MCQ 401-450](http://hutaifortho.com/640)
[ORTHOPEDICS HYPERGUIDE MCQ 351-400](http://hutaifortho.com/639)
[ORTHOPEDICS HYPERGUIDE MCQ 301-350](http://hutaifortho.com/638)
[ORTHOPEDICS HYPERGUIDE MCQ 251-300](http://hutaifortho.com/637)
[ORTHOPEDICS HYPERGUIDE MCQ 201-250](http://hutaifortho.com/636)
[ORTHOPEDICS HYPERGUIDE MCQ 151-200](http://hutaifortho.com/635)
[ORTHOPEDICS HYPERGUIDE MCQ 101-150](http://hutaifortho.com/634)
[FREE Orthopedics MCQS 2022 51-100](http://hutaifortho.com/633)
[Orthopedics Hyperguide MCQ 1-50](http://hutaifortho.com/631)
by the surgeon or by an interventional radiologist trained in core biopsy techniques. It is imperative to make a pathologic diagnosis prior to proceeding with any further medical, surgical, or radiation treatments. A histologic diagnosis at this point is the only way a medical oncologist can have a meaningful discussion with the patient about their disease, its natural history, and ultimately discuss treatment options and prognosis. Further imaging at this point only delays the time to histologic evaluation. Consideration of surgical stabilization can be delayed until a diagnosis is established and a multidisciplinary approach is initiated. This fracture can be treated at least temporarily with nonsurgical protected weight bearing with a walker or crutches.
Hospice may soon serve a useful role but a diagnosis must first be rendered and a limited life expectancy anticipated. Pre Res # 100 is 2
**MORE MCQS**
[ORTHO MCQS 011 FREE BANK 02](http://hutaifortho.com/878)
---
[ORTHO MCQS 011 FREE BANK](http://hutaifortho.com/877)
[Orthopedic MCQS online Hip and knee ADULT...](http://hutaifortho.com/876)
[ORTHOPEDIC MCQS OB 20 TRAUMA1](http://hutaifortho.com/875)
[ORTHOPEDIC MCQS OB 20 BASIC5](http://hutaifortho.com/874)
[ORTHOPEDIC MCQS OB 20 BASIC7](http://hutaifortho.com/873)
[ORTHOPEDIC MCQS OB 20 BASIC 6](http://hutaifortho.com/872)
[ORTHOPEDIC MCQS OB 20 BASIC 44](http://hutaifortho.com/871)
[ORTHOPEDIC MCQS OB 20 BASIC 4](http://hutaifortho.com/870)
[ORTHOPEDIC MCQS OB 20 BASIC 3](http://hutaifortho.com/869)
[ORTHOPEDIC MCQS OB 20 BASIC 2](http://hutaifortho.com/868)
[ORTHOPEDIC MCQS OB 20 BASIC 1](http://hutaifortho.com/867)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4](http://hutaifortho.com/865)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3](http://hutaifortho.com/864)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2](http://hutaifortho.com/863)
[1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW](http://hutaifortho.com/862)
[ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01](http://hutaifortho.com/861)
[ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01](http://hutaifortho.com/860)
[ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01](http://hutaifortho.com/859)
[ORTHOPEDIC MCQS BANK WITH
NATOMY 02](http://hutaifortho.com/858)
[ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02](http://hutaifortho.com/857)
[ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02](http://hutaifortho.com/856)
[ORTHOPEDIC MCQS WITH ANSWER FOOT 03](http://hutaifortho.com/855)
[ORTHOPEDIC MCQS WITH ANSWER SPINE 03](http://hutaifortho.com/854)
[ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03](http://hutaifortho.com/853)
[ORTHOPEDIC MCQS WITH ANSWER HIP 04](http://hutaifortho.com/852)
[ORTHOPEDIC MCQS WITH ANSWER PEDS 04](http://hutaifortho.com/851)
[ORTHOPEDIC MCQS WITH ANSWER SPORT 04](http://hutaifortho.com/850)
[ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05](http://hutaifortho.com/849)
[ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05](http://hutaifortho.com/848)
[ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05](http://hutaifortho.com/847)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06](http://hutaifortho.com/846)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...](http://hutaifortho.com/845)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06](http://hutaifortho.com/844)
[ORTHOPEDIC MCQS with Answers ONLINE BASIC 06](http://hutaifortho.com/843)
[ORTHOPEDIC MCQS ONLINE PEDIATRICS 07](http://hutaifortho.com/842)
[ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07](http://hutaifortho.com/841)
[ONLINE ORTHOPEDIC MCQS SPORT07](http://hutaifortho.com/840)
[ONLINE ORTHOPEDIC MCQS UPPER LIMB08](http://hutaifortho.com/839)
[ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08](http://hutaifortho.com/838)
[ONLINE ORTHOPEDIC MCQS ANATOMY08](http://hutaifortho.com/837)
[ONLINE ORTHOPEDIC MCQS FOOT0 9](http://hutaifortho.com/836)
[ONLINE ORTHOPEDIC MCQS SPINE0 9](http://hutaifortho.com/835)
[ONLINE ORTHOPEDIC MCQS TRAUMA 9](http://hutaifortho.com/834)
[Orthopedic MCQS online sports Medicine](http://hutaifortho.com/833)
[Orthopedic MCQS online Shoulder and Elbow](http://hutaifortho.com/832)
[Orthopedic MCQS online Hip and knee](http://hutaifortho.com/831)
[online orthopedic mcqs](http://hutaifortho.com/830)
[Shoulder and elbow: Mcqs AND EMQS Answers](http://hutaifortho.com/766)
[Shoulder And Elbow: Questions Mcqs AND EMQS](http://hutaifortho.com/765)
[Hand and wrist: Answers MCQS EMQS](http://hutaifortho.com/764)
[Hand and wrist: MCQ AND EMQ Questions](http://hutaifortho.com/763)
[quize](http://hutaifortho.com/729)
[KEY POINTS](http://hutaifortho.com/727)
[MIND MAP](http://hutaifortho.com/726)
[action tree](http://hutaifortho.com/725)
[action2](http://hutaifortho.com/724)
[Action](http://hutaifortho.com/723)
[patient](http://hutaifortho.com/722)
[Bop](http://hutaifortho.com/721)
[New](http://hutaifortho.com/720)
[Trial](http://hutaifortho.com/714)
[Pupup](http://hutaifortho.com/713)
[SSEE](http://hutaifortho.com/704)
[SE](http://hutaifortho.com/703)
[2021 SHOULDER AND ELBOW MCQS FREE](http://hutaifortho.com/689)
[Pediatric Orthopaedic MCQS Self-Assessment...](http://hutaifortho.com/685)
[Self-Assessment Examination 2020 Adult Spine MCQS](http://hutaifortho.com/684)
[Foot and Ankle free MCQS2020 Online](http://hutaifortho.com/681)
[UPDATED ORTHOPEDIC MCQS](http://hutaifortho.com/680)
[FREE Orthopedics MCQS 2022 1951.-2000.](http://hutaifortho.com/677)
[FREE Orthopedics MCQS 2022 1901.-1950.](http://hutaifortho.com/676)
[FREE Orthopedics MCQS 2022 1851-1900.](http://hutaifortho.com/675)
[FREE Orthopedics MCQS 2022 1751-1850..](http://hutaifortho.com/674)
[FREE Orthopedics MCQS 2022 1751-1800..](http://hutaifortho.com/673)
[Foot and Ankle FREE ORTHOPEDICS MCQS Question 11](http://hutaifortho.com/672)
[FREE Orthopedics MCQS 2022 1701-1750.](http://hutaifortho.com/668)
[FREE Orthopedics MCQS 2022 1651-1700](http://hutaifortho.com/667)
[FREE Orthopedics MCQS 2022 1601-1650.](http://hutaifortho.com/666)
[ORTHOPEDIC MCQS FREE 2023](http://hutaifortho.com/665)
[FREE Orthopedics MCQS 2022 1551-1600](http://hutaifortho.com/664)
[FREE Orthopedics MCQS 2022 1501-1550](http://hutaifortho.com/663)
[FREE Orthopedics MCQS 2022 1451-1500](http://hutaifortho.com/662)
[FREE Orthopedics MCQS 2022 1401-1450](http://hutaifortho.com/661)
[FREE Orthopedics MCQS 2022 1351 -1400](http://hutaifortho.com/660)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350](http://hutaifortho.com/659)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300](http://hutaifortho.com/658)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200](http://hutaifortho.com/656)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150](http://hutaifortho.com/655)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100](http://hutaifortho.com/654)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051](http://hutaifortho.com/653)
[ORTHOPEDICS HYPERGUIDE MCQ 951-1000](http://hutaifortho.com/652)
[ORTHOPEDICS HYPERGUIDE MCQ 901-950](http://hutaifortho.com/651)
[ORTHOPEDICS HYPERGUIDE MCQ 851-900](http://hutaifortho.com/650)
[ORTHOPEDICS HYPERGUIDE MCQ 800-850](http://hutaifortho.com/649)
[ORTHOPEDICS HYPERGUIDE MCQ 751-800](http://hutaifortho.com/647)
[ORTHOPEDICS HYPERGUIDE MCQ 701-750](http://hutaifortho.com/646)
[ORTHOPEDICS HYPERGUIDE MCQ 651-700](http://hutaifortho.com/645)
[ORTHOPEDICS HYPERGUIDE MCQ 601-650](http://hutaifortho.com/644)
[ORTHOPEDICS HYPERGUIDE MCQ 551-600](http://hutaifortho.com/643)
[ORTHOPEDICS HYPERGUIDE MCQ 501-550](http://hutaifortho.com/642)
[ORTHOPEDICS HYPERGUIDE MCQ 451-500](http://hutaifortho.com/641)
[ORTHOPEDICS HYPERGUIDE MCQ 401-450](http://hutaifortho.com/640)
[ORTHOPEDICS HYPERGUIDE MCQ 351-400](http://hutaifortho.com/639)
[ORTHOPEDICS HYPERGUIDE MCQ 301-350](http://hutaifortho.com/638)
[ORTHOPEDICS HYPERGUIDE MCQ 251-300](http://hutaifortho.com/637)
[ORTHOPEDICS HYPERGUIDE MCQ 201-250](http://hutaifortho.com/636)
[ORTHOPEDICS HYPERGUIDE MCQ 151-200](http://hutaifortho.com/635)
[ORTHOPEDICS HYPERGUIDE MCQ 101-150](http://hutaifortho.com/634)
[FREE Orthopedics MCQS 2022 51-100](http://hutaifortho.com/633)
[Orthopedics Hyperguide MCQ 1-50](http://hutaifortho.com/631)
Question 2High Yield
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right
groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?

Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
Question 3High Yield
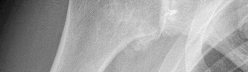
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient?
---
---
---
---


Explanation
The radiographs show severe osteoarthritis of the shoulder. The best surgical option would be an arthroplasty. The major determining factor for which type of arthroplasty to choose is the integrity of the rotator cuff tendons.
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
Question 4High Yield
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
With soft-tissue loss, local or free flap coverage may be necessary to treat exposed tendon and bone. However, a vacuum-assisted closure device is a good temporizing dressing. It prevents external contamination, reduces edema around the wound, increases oxygen tension in the wound, and promotes the formation of granulation tissue. The use of this negative pressure device has been described in both acute traumatic and in chronic wound scenarios. If sufficient granulation tissue forms, closure may be by split graft, avoiding a more complex coverage procedure. Immediate skin grafting over the exposed anterior tibial tendon and tibia would have a low likelihood of success. Dressing changes with sulfasalazine may be beneficial in a burn wound to assist with removal of skin slough; however, in a granulating wound, the material may be toxic to early epithelialization. Xenograft is a foreign body and should not be applied to an acute contaminated open wound. Historically, a cross-leg flap was a treatment alternative for lower extremity soft-tissue loss; however, its current applications are extremely limited.
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
Question 5High Yield
Slide 1 Slide 2
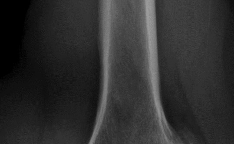
A 9-year-old boy has a history of multiple fractures. He presents with left leg pain following a minor fall. His anteroposterior
(Slide 1) and lateral (Slide 2) plain radiographs are shown. The most likely genetiCdefect would be:
A 9-year-old boy has a history of multiple fractures. He presents with left leg pain following a minor fall. His anteroposterior
(Slide 1) and lateral (Slide 2) plain radiographs are shown. The most likely genetiCdefect would be:
Explanation
The anteroposterior and lateral radiographs show thinned cortices and a gentle S-shaped curve of the tibia. The overall alignment of the tibia, as well as the physes, is normal. These are the radiographiCfeatures of osteogenesis imperfecta.
In osteogenesis imperfecta, the genetiCdefect involves type I collagen. Type I collagen is made up of two alpha-1 chains and one alpha-2 chain in a triple helix. Glycine is the smallest amino acid and is crucial for coiling of the triple helix. Mutations in the
glycine chain lead to severe forms of osteogenesis imperfecta. One should also remember the Silence classification:
Type Inheritance Sclera Severity
I AD Blue Mild form, normal teeth
II AR Blue Lethal form, die early
III AR Normal Severe, progressively deforming
IV AD Normal Moderately severe
Biphosphonate therapy can be used to slow bone remodeling and increase bone mass. With regard to the incorrect choices:
FGF receptor 3 is associated with achondroplasia. Fibrillin is associated with Marfan's syndrome.
Type II collagen is associated with spondyloepiphyseal dsyplasia.
Cartilage oligomeriCmatrix protein is associated with pseudoachondroplasia. Correct Answer: Type I collagen
In osteogenesis imperfecta, the genetiCdefect involves type I collagen. Type I collagen is made up of two alpha-1 chains and one alpha-2 chain in a triple helix. Glycine is the smallest amino acid and is crucial for coiling of the triple helix. Mutations in the
glycine chain lead to severe forms of osteogenesis imperfecta. One should also remember the Silence classification:
Type Inheritance Sclera Severity
I AD Blue Mild form, normal teeth
II AR Blue Lethal form, die early
III AR Normal Severe, progressively deforming
IV AD Normal Moderately severe
Biphosphonate therapy can be used to slow bone remodeling and increase bone mass. With regard to the incorrect choices:
FGF receptor 3 is associated with achondroplasia. Fibrillin is associated with Marfan's syndrome.
Type II collagen is associated with spondyloepiphyseal dsyplasia.
Cartilage oligomeriCmatrix protein is associated with pseudoachondroplasia. Correct Answer: Type I collagen
Question 6High Yield
Figure 1 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?

Explanation
■
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-α, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-β, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-α, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-β, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
Question 7High Yield
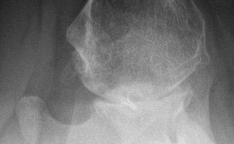
Figure below shows the radiograph obtained from a 76-year-old woman who has sharp pain in her groin,
thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best
to proceed. What is the best next step?
thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best
to proceed. What is the best next step?

Explanation
The next best course of action is total hip arthroplasty. The patient is an otherwise healthy woman requesting pain relief and expresses a desire to be dancing in 4 months. She has had more than 6 months of symptoms that are classic hip osteoarthritis symptoms, with pain in the groin and thigh. Severe osteoarthritis is seen in the radiograph as well. NSAIDs are no longer working. Given the objective findings, the subjective reports, and the duration of symptoms, this patient merits surgery. Consideration for steroid injection is reasonable, but given her desire to be dancing in 4 months, an injection would increase her risk of infection if total hip arthroplasty were to be performed within 3 months of the
injection.
injection.
Question 8High Yield
What is the most appropriate next step?
Explanation
- Nonsteroidal anti-inflammatory drugs and physical therapy_
Question 9High Yield
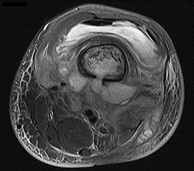
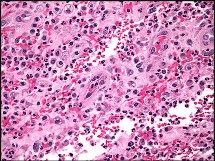
Figures 89a through 89g are the radiographs, MR images, and biopsy specimen of a 32-year-old man who has chronic left thigh and knee pain and recent knee swelling with no specific trauma or injury. The pain is exacerbated with activity but is also present at rest and at night. What is the most appropriate treatment?







Explanation
The radiographs show a lytic, destructive, poorly marginated femur lesion. MR imaging confirms the infiltrative nature of the lesion, a communication with the joint, and a substantial nonenhancing joint effusion. Biopsy confirms numerous polymorphonuclear neutrophils consistent with osteomyelitis with septic arthritis. The treatment of femur osteomyelitis with a septic knee includes aggressive debridement of all nonviable tissue, placement of antibiotic beads, and IV antibiotics. Surgical wide resection and endoprosthetic reconstruction would be considered only if the lesion were a low-grade malignancy. Aggressive curettage with allograft placement would be considered for benign tumors. Allograft placement is not appropriate in the setting of an infection. Chemotherapy followed by wide surgical resection and reconstruction is only appropriate for a high-grade malignancy.
RECOMMENDED READINGS
82. [Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004 Jul 24-30;364(9431):369-79. Review. PubMed PMID: 15276398.](http://www.ncbi.nlm.nih.gov/pubmed/15276398)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15276398)
83. [Tetsworth K, Cierny G 3rd. Osteomyelitis debridement techniques. Clin Orthop Relat Res. 1999 Mar;(360):87-96. Review. PubMed PMID: 10101313.](http://www.ncbi.nlm.nih.gov/pubmed/10101313)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10101313)
84. [Karchevsky M, Schweitzer ME, Morrison WB, Parellada JA. MRI findings of septic arthritis and associated osteomyelitis in adults. AJR Am J Roentgenol. 2004 Jan;182(1):119-22. PubMed PMID: 14684523.](http://www.ncbi.nlm.nih.gov/pubmed/14684523)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14684523)
CLINICAL SITUATION FOR QUESTIONS 90 AND 91
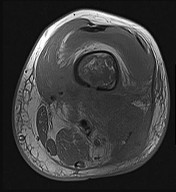
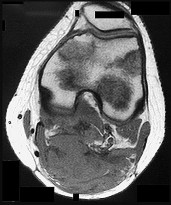
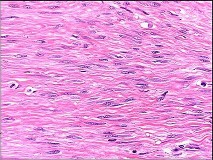
Figures 90a and 90b are the axial MR image and histology of a 27-year-old woman who has a firm lesion in the popliteal fossa. Figure 90c is the gross specimen after resection.
RECOMMENDED READINGS
82. [Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004 Jul 24-30;364(9431):369-79. Review. PubMed PMID: 15276398.](http://www.ncbi.nlm.nih.gov/pubmed/15276398)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15276398)
83. [Tetsworth K, Cierny G 3rd. Osteomyelitis debridement techniques. Clin Orthop Relat Res. 1999 Mar;(360):87-96. Review. PubMed PMID: 10101313.](http://www.ncbi.nlm.nih.gov/pubmed/10101313)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10101313)
84. [Karchevsky M, Schweitzer ME, Morrison WB, Parellada JA. MRI findings of septic arthritis and associated osteomyelitis in adults. AJR Am J Roentgenol. 2004 Jan;182(1):119-22. PubMed PMID: 14684523.](http://www.ncbi.nlm.nih.gov/pubmed/14684523)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14684523)
CLINICAL SITUATION FOR QUESTIONS 90 AND 91
Figures 90a and 90b are the axial MR image and histology of a 27-year-old woman who has a firm lesion in the popliteal fossa. Figure 90c is the gross specimen after resection.
Question 10High Yield
Nerve conduction velocity is slowed by
Explanation
A number of factors affect nerve conduction velocity; for example, increased body temperature increases nerve conduction velocity. Nerve conduction velocity is slowed by advancing age, compression, decreased blood flow, and fibrosis (from large imprecise sutures used for nerve repair). There is no _association between hand dominance and nerve conduction velocity._
Question 11High Yield
Which of the following is not a complication of macrodactyly surgery:
Explanation
C omplications of macrodactyly surgery include poor healing of flaps secondary to devascularization or undue tension, nerve injury or decreased sensation, infection, stiffness, bony nonunion or malunion, and failure of the epiphysiodesis.
Question 12High Yield
What is the best approach to reduce and stabilize a displaced volar lunate facet fracture of the wrist?
Explanation
A volar lunate fragment of a distal radial fracture is considered a critical component to overall joint stability and function. Obtaining a reduction is difficult through a standard volar approach to the radius between the flexor carpi radialis and radial artery. Visualization and reduction of the ulnar volar facet is not possible from this approach. An extended carpal tunnel incision provides access to the entire articular surface, except for the distal radial styloid component.
REFERENCES: Hanel DP, Jones MD, Trumble TE: Wrist fractures. Orthop Clin North Am 2002;33:35-57.
Trumble TE, Culp RW, Hanel DP, et al: Intra-articular fractures of the distal aspect of the radius. Instr Course Lect 1999;48:465-480.
REFERENCES: Hanel DP, Jones MD, Trumble TE: Wrist fractures. Orthop Clin North Am 2002;33:35-57.
Trumble TE, Culp RW, Hanel DP, et al: Intra-articular fractures of the distal aspect of the radius. Instr Course Lect 1999;48:465-480.
Question 13High Yield
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Explanation
Based on these findings, the most likely diagnosis is a rotator cuff injury and probable tear; therefore, MRI is the study of choice. CT is preferred for articular fractures. A bone scan is nonspecific and can identify inflammation or occult fracture. Joint aspiration is not likely to identify an effusion. Physical therapy and a functional capacity examination are used to identify weakness during recovery prior to a return to work or sports.
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 14High Yield
..Complete transection of the ulnar nerve at the elbow will result in
Explanation
- weakness with finger abduction.
Question 15High Yield
The best treatment is
Explanation
- chemotherapy and wide surgical resection._
Question 16High Yield
A 2-year-old child is brought to your office for evaluation of a "big hand." Upon examination, you notice that the child has mildly enlarged ring and small fingers. There is full range of motion without instability. The childâs parents inform you that they would like you to amputate the affected digits as soon as possible. You should:
Explanation
Although amputation may be necessary in some patients with macrodactyly, it is too early in the course of this case to begin entertaining such a drastic measure. A debulking procedure is not recommended for a 2-year-old child. Radiation therapy is not an option in uncomplicated cases of macrodactyly. The surgeon must educate the parents about the disease process and order additional testing.
Question 17High Yield
The plain radiographs and MR image shown in Figures 37a through 37c indicate which condition?
Explanation
- Cam-type femoroacetabular impingement with an acetabular labral tear
Question 18High Yield
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be**
Explanation
Isolated palsy of the infraspinatus portion of the suprascapular nerve is common in volleyball players and is seen frequently in the throwing arm of baseball players. The exact cause is not known, but it may be the result of either tethering or traction on the nerve at the spinoglenoid notch. Synovial cysts in the spinoglenoid notch also can be a cause, but the patient’s negative MRI findings rule out that entity. Because many isolated nerve palsies of the infraspinatus branch are asymptomatic, initial management should always be nonsurgical. Surprisingly, many athletes with this injury can participate fully in sports. Surgical treatment with decompression at the notch is unpredictable and generally is indicated only if nonsurgical management fails.
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Martin SD, Warren RF, Martin TL, Kennedy K, O’Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Martin SD, Warren RF, Martin TL, Kennedy K, O’Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 19High Yield
Figure 6 shows the radiograph of a 72-year-old woman who underwent a primary total hip arthroplasty
17 years ago. She now reports groin pain. Optimal surgical management should consist of which of the following?
17 years ago. She now reports groin pain. Optimal surgical management should consist of which of the following?
Explanation
Polyethylene wear is evident due to the superiorly eccentric position of the femoral head within the acetabulum. Despite proximal femoral osteolysis, the component appears well fixed, as does the acetabulum. The acetabular component appears to be well positioned. Therefore, an isolated synovectomy and polyethylene liner exchange is indicated. If the hip is stable, there is no need for more extensive revision work.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 521-528.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 521-528.
Question 20High Yield
A patient with Pott’s disease, tuberculosis of the spine, is more likely to have which of the following early findings?


Explanation
DISCUSSION: Tuberculosis of the spine typically has an indolent presentation. Unlike pyogenic infections of the spine, the disk space is usually preserved. Most commonly, the thoracic and lumbar spine are affected. Laboratory studies may be nonspecific. Delayed presentation usually results in neurologic compromise and a kyphotic deformity. Treatment includes a multidrug regimen. Surgery is indicated for deformity correction or failure of medical treatment.
REFERENCES: Rajasekaran S: Buckling collapse of the spine in childhood spinal tuberculosis. Clin Orthop Relat Res 2007;460:86-92.
_TAL-MaeKXCpy I_ Hu SS: Spinal infections. J Am Acad Orthop Surg 2002; 10:188-197fcUa-MJ ^
Figure 71a Figure 71b Figure 71c Figure 71 d Question 71
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain
during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 71 d show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
1. ##### Bracing with a thoracolumbosacral orthosis (TLSO)
2. ##### Observation with repeat radiographs of the scoliosis in 3 months and nonsteroidal antiinflammatory drugs for the pain
3. ##### MRI of the neuro-axis
4. ##### Surgical removal
5. ##### Radiofrequency ablation
PREFERRED RESPONSE: 4
DISCUSSION: The history, examination findings, and studies are consistent with an osteoid osteoma. The CT scan shows a classic “target” lesion, and the bone scan has intense uptake at the site of the osteoid osteoma. The child has had a 2-year history of pain that even wakes her from sleep, so
obs _A_ e _L_ rv _-M_ at _a_ io _de_ n _na_ a _C_ n _o_ d _py_ anti-inflammatory drugs is not a preferred treatment. Bracing will not help with the
58 • American Academy of Orthopaedic Surgeons
discomfort because the pain is not mechanical in nature. MRI would not be needed in addition to the studies already completed. The osteoid osteoma is close to the spinal cord so radiofrequency ablation is not preferred. Surgical removal and biopsy is the treatment of choice.
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
574/. Cantwell CP, Obyme J, Eustace S: Current trends in treatment of osteoid osteoma with an emphasis on radiofirequency ablation. Eur Radiol 2004;14:607-617.
Figure 72
REFERENCES: Rajasekaran S: Buckling collapse of the spine in childhood spinal tuberculosis. Clin Orthop Relat Res 2007;460:86-92.
_TAL-MaeKXCpy I_ Hu SS: Spinal infections. J Am Acad Orthop Surg 2002; 10:188-197fcUa-MJ ^
Figure 71a Figure 71b Figure 71c Figure 71 d Question 71
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain
during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 71 d show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
1. ##### Bracing with a thoracolumbosacral orthosis (TLSO)
2. ##### Observation with repeat radiographs of the scoliosis in 3 months and nonsteroidal antiinflammatory drugs for the pain
3. ##### MRI of the neuro-axis
4. ##### Surgical removal
5. ##### Radiofrequency ablation
PREFERRED RESPONSE: 4
DISCUSSION: The history, examination findings, and studies are consistent with an osteoid osteoma. The CT scan shows a classic “target” lesion, and the bone scan has intense uptake at the site of the osteoid osteoma. The child has had a 2-year history of pain that even wakes her from sleep, so
obs _A_ e _L_ rv _-M_ at _a_ io _de_ n _na_ a _C_ n _o_ d _py_ anti-inflammatory drugs is not a preferred treatment. Bracing will not help with the
58 • American Academy of Orthopaedic Surgeons
discomfort because the pain is not mechanical in nature. MRI would not be needed in addition to the studies already completed. The osteoid osteoma is close to the spinal cord so radiofrequency ablation is not preferred. Surgical removal and biopsy is the treatment of choice.
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
574/. Cantwell CP, Obyme J, Eustace S: Current trends in treatment of osteoid osteoma with an emphasis on radiofirequency ablation. Eur Radiol 2004;14:607-617.
Figure 72
Question 21High Yield
The examination finding shown in Video 1 is consistent with which defect?
Explanation
The video shows the lack of tenodesis caused by the incompetence of the FDP tendon to the ring finger, which can be attributable to a laceration, tendon rupture, or avulsion. Note how the ring finger stays extended (compared to the other digits) when the extensor tendons are tightened during wrist extension. The other fingers are pulled into flexion by the FDP tendons when the extensor tendons are relaxed during wrist extension. With the wrist flexed, the extensor mechanism to all fingers appears to be functioning normally. Findings indicating a trigger finger would be locking in flexion of the proximal interphalangeal joint. FDS incompetence can only be detected by blocking FDP function of the other fingers and actively flexing the examined finger.
Question 22High Yield
Figure 77 shows the CT scan of a 65-year-old Asian man who has been experiencing increasing difficulty using his hands. His handwriting has changed and he feels off balance. What is the most likely cause of his symptoms?

Explanation
This patient has cervical myelopathy caused by both congenital stenosis and an ossified posterior longitudinal ligament (OPLL). OPLL typically is seen in populations of Asian people and appears more frequently in males. The pathogenesis is unclear, but the posterior longitudinal ligament that connects the posterior vertebral body becomes ossified, making it visible on CT scan.
A herniated disk may be difficult to see on a CT scan and is not typically calcified This patient has degenerative spondylosis and likely some ligamentum hypertrophy, but the OPLL is fairly prominent and thick in the upper cervical spine. The ligamentum flavum is located dorsal to the dural sac, and the ossification is ventral to the dural sac.
RECOMMENDED READINGS
22. [An HS, Al-Shihabi L, Kurd M. Surgical treatment for ossification of the posterior longitudinal ligament in the cervical spine. J Am Acad Orthop Surg. 2014 Jul;22(7):420-9. doi: 10.5435/JAAOS-22-07-420. Review. PubMed PMID: 24966248.](http://www.ncbi.nlm.nih.gov/pubmed/24966248)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24966248)
23. [Mizuno J, Nakagawa H. Ossified posterior longitudinal ligament: management strategies and outcomes. Spine J. 2006 Nov-Dec;6(6 Suppl):282S-288S. Review. PubMed PMID: 17097548. ](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[View](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17097548)
A herniated disk may be difficult to see on a CT scan and is not typically calcified This patient has degenerative spondylosis and likely some ligamentum hypertrophy, but the OPLL is fairly prominent and thick in the upper cervical spine. The ligamentum flavum is located dorsal to the dural sac, and the ossification is ventral to the dural sac.
RECOMMENDED READINGS
22. [An HS, Al-Shihabi L, Kurd M. Surgical treatment for ossification of the posterior longitudinal ligament in the cervical spine. J Am Acad Orthop Surg. 2014 Jul;22(7):420-9. doi: 10.5435/JAAOS-22-07-420. Review. PubMed PMID: 24966248.](http://www.ncbi.nlm.nih.gov/pubmed/24966248)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24966248)
23. [Mizuno J, Nakagawa H. Ossified posterior longitudinal ligament: management strategies and outcomes. Spine J. 2006 Nov-Dec;6(6 Suppl):282S-288S. Review. PubMed PMID: 17097548. ](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[View](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17097548)
Question 23High Yield
A 50-year-old man sustained an external rotation traction injury to his right arm. He felt a pop in the anterior aspect of his shoulder associated with immediate pain and swelling. The MRI scan shows a tear of the subscapularis tendon, as shown in Figures 1 and
Explanation
The anatomic structure labeled is the biceps tendon, which has subluxated medially from the intertubercular groove as a result of disruption of the biceps pulley that occurs with subscapularis tears. The anterior labrum is adjacent to the glenoid and is not normally torn with subscapularis pathology. The middle glenohumeral ligament may appear cord-like, but is shown more medial to the subluxated biceps tendon. The rotator interval tissue, or "comma" tissue, is generally along the upper border of the subscapularis and is pulled toward the coracoid base in subscapularis tears.
Question 24High Yield
Figure 1 shows the radiograph obtained from a 54-year-old woman with rheumatoid arthritis who has thumb pain and dysfunction. Nonsurgical treatment, including splinting, oral NSAIDs, activity modification, and steroid injections, has failed. What is the most appropriate surgical intervention?
---
---

Explanation
Various options exist to treat thumb CMC arthritis: trapezial resection alone, trapezial resection with ligament suspensionplasty or tendon interposition, trapezial resection with both ligament suspensionplasty and tendon interposition, CMC fusion, and CMC replacement. MCP hyperextension can develop in long-standing CMC arthritis, contributing to CMC instability as well as thumb pain and weakness. In patients with concomitant MCP hyperextension that exceeds 30°,
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
Question 25High Yield
Back injuries occur in approximately 2% of the work force every year,
resulting in workers’ compensation costs of more than $20 billion. What percentage of workers, with symptoms severe enough to require work absence, return to work within 12 weeks?
resulting in workers’ compensation costs of more than $20 billion. What percentage of workers, with symptoms severe enough to require work absence, return to work within 12 weeks?
Explanation
In adults, 70% to 85% will experience an episode of low back pain at some period during their life. Most recover quickly and without residual functional deficits. Of those patients with symptoms severe enough to require absence from work, 60% to 70% return within 6 weeks and 80% to 90% return within 12 weeks. After 12 weeks of symptoms, return to work is much slower.
Question 26High Yield
Figure 1 shows the radiograph obtained from a 67-year-old man recently diagnosed with osteoarthritis, 8
years after receiving a left metal-on-metal total hip arthroplasty (THA). The acetabular component has a modular cobalt alloy acetabular liner. The patient states that he did very well postoperatively, but for the last 6 months has noted worsening pain and swelling in his left hip. Serum metal ion testing reveals a chromium level of 12.4 ng/mL, compared with a normal level of less than 0.3 ng/mL, and a cobalt level of 11.8 ng/mL, compared with a normal level less than 0.7 ng/mL. An MRI with metal artefact reduction sequence (MARS) was performed and is shown in Figure
years after receiving a left metal-on-metal total hip arthroplasty (THA). The acetabular component has a modular cobalt alloy acetabular liner. The patient states that he did very well postoperatively, but for the last 6 months has noted worsening pain and swelling in his left hip. Serum metal ion testing reveals a chromium level of 12.4 ng/mL, compared with a normal level of less than 0.3 ng/mL, and a cobalt level of 11.8 ng/mL, compared with a normal level less than 0.7 ng/mL. An MRI with metal artefact reduction sequence (MARS) was performed and is shown in Figure

Explanation
Metal-on-metal THA was initially introduced in the 1990s, with the proposed advantages of decreased wear and improved stability. However, catastrophic adverse local tissue reactions associated with their use has raised numerous concerns. The work-up of a patient with a prior metal-on-metal total hip arthroplasty involves a thorough history and physical examination; blood analysis, including the erythrocyte sedimentation rate, C-reactive protein, and metal ion levels; and secondary imaging, including ultrasonography, CT, and MRI. In a patient with clinical symptoms, elevated metal ion levels, and a large fluid collection seen on MRI, the most appropriate treatment would be removal of the metal-on-metal bearing. Given the presence of an adverse reaction involving cobalt and chromium, a revision ceramic head may be most appropriate to avoid the potential of trunnion-associated corrosion.
Question 27High Yield
A 6-year-old child is seen in the emergency department after falling from the monkey bars. Examination reveals tenderness of the right humerus and an inability to dorsiflex the wrist. No other injuries are identified. Radiographs show a minimally displaced and angulated (10 degrees of varus angulation) fracture of the distal one third of the humeral shaft. Initial management should consist of which of the following?
Explanation
2010 Pediatric Orthopaedic Examination
ook • 69
3. ##### Immediate exploration of the radial nerve with open reduction and plate fixation
4. ##### Monitoring of radial nerve function and application of a sling and swathe
5. ##### Monitoring of radial nerve function and external fixation PREFERRED RESPONSE: 4
DISCUSSION: Humeral shaft fractures in children rarely require open reduction. Shoulder and elbow function does not appear to be affected by up to 40 degrees of angulation in this patient population. Because of the high rate of remodeling in pediatric patients, the standard treatment is immobilization in a sling and swathe, a hanging arm cast, or a compressive dressing. Surgical fixation of humeral shaft fractures is usually only necessary in open injuries, multitrauma, or severely displaced fractures. Most radial nerve injuries associated with humerus fractures are secondary to contusion. Almost all associated radial nerve injuries in pediatric patients can be treated with observation.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 304.
Shrader MW: Proximal humerus and humeral shaft fractures in children. Hand Clin 2007;23:431-435. Caviglia H, Garrido CP, Palazzi FF, et al: Pediatric fractures of the humerus. Clin Orthop Relat Res 2005;432:49-56.
2010 Pediatric Orthopaedic Examination
ook • 69
3. ##### Immediate exploration of the radial nerve with open reduction and plate fixation
4. ##### Monitoring of radial nerve function and application of a sling and swathe
5. ##### Monitoring of radial nerve function and external fixation PREFERRED RESPONSE: 4
DISCUSSION: Humeral shaft fractures in children rarely require open reduction. Shoulder and elbow function does not appear to be affected by up to 40 degrees of angulation in this patient population. Because of the high rate of remodeling in pediatric patients, the standard treatment is immobilization in a sling and swathe, a hanging arm cast, or a compressive dressing. Surgical fixation of humeral shaft fractures is usually only necessary in open injuries, multitrauma, or severely displaced fractures. Most radial nerve injuries associated with humerus fractures are secondary to contusion. Almost all associated radial nerve injuries in pediatric patients can be treated with observation.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 304.
Shrader MW: Proximal humerus and humeral shaft fractures in children. Hand Clin 2007;23:431-435. Caviglia H, Garrido CP, Palazzi FF, et al: Pediatric fractures of the humerus. Clin Orthop Relat Res 2005;432:49-56.
Question 28High Yield
Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?
Explanation
Minimally displaced fractures of the proximal humerus have a good outcome if physical therapy is initiated within 2 weeks of the injury. Results are not affected by age, open reduction and internal fixation, or involvement of the greater tuberosity. Immobilization for longer than 3 weeks will often result in stiffness.
REFERENCES: Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Hodgson SA, Mawson SJ, Stanley D: Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 2003;85:419-422.
REFERENCES: Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Hodgson SA, Mawson SJ, Stanley D: Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 2003;85:419-422.
Question 29High Yield
What is the most cost-effective implant indicated for the injury shown in Figures A and B, assuming the hospital purchases the implants at-cost from the manufacturer?



Explanation
In the intertrochanteric hip fracture displayed, a sliding hip screw (SHS) or cephalomedullary nail (CMN) would be indicated; the SHS is the cheaper implant.
In a standard obliquity intertrochanteric fracture without lateral wall comminution, an SHS is a cost-effective option. In reverse obliquity fractures or those with lateral wall comminution (unstable), there is an increased failure rate with this implant and an CMN should be considered. There is some controversy in terms of short and intermediate nail indications, which are attractive because they do not require reaming. SHS implants are contraindicated in subtrochanteric fractures. Although some hospitals receive discounts on implants, in general, intramedullary nail options are more expensive than SHS.
Swart et al. examined the cost-effectiveness of different fixation options for intertrochanteric hip fractures. They compared SHS and CMN implants using an expected-value decision-analysis model, taking into account fracture patterns, failure rates, and revision costs. In their study, the average cost of a SHS was
$2,000 compared to $3,200 for a standard CMN. They concluded that the SHS was likely more cost-effective for stable and questionably stable fractures compared to CMN fixation; CMN was more cost-effective for reverse obliquity patterns.
Kaplan et al. provided a review article on the surgical management of intertrochanteric fractures. Factors to determine treatment should include the patient's medical co-morbidities, pre-existing arthritis, bone quality, and fracture morphology. Their study did not find an appreciable difference in patient outcomes using either CMN or SHS for stable intertrochanteric fractures; surgeon experience and implant costs should, therefore, drive the decision making process for implant selection.
Figures A and B are AP and lateral right hip radiographs, respectively, demonstrating a standard obliquity intertrochanteric hip fracture. Illustration A is an AP post-operative radiograph showing a hip fracture treated with a SHS.
Incorrect Answers:
Answers 1 and 2: Both of these options are appropriate for this fracture but more costly than a SHS.
Answer 4: Arthroplasty is not indicated for this patient with an intertrochanteric fracture and preserved joint space.
Answer 5: Cannulated screws are not indicated for an intertrochanteric fracture.
In a standard obliquity intertrochanteric fracture without lateral wall comminution, an SHS is a cost-effective option. In reverse obliquity fractures or those with lateral wall comminution (unstable), there is an increased failure rate with this implant and an CMN should be considered. There is some controversy in terms of short and intermediate nail indications, which are attractive because they do not require reaming. SHS implants are contraindicated in subtrochanteric fractures. Although some hospitals receive discounts on implants, in general, intramedullary nail options are more expensive than SHS.
Swart et al. examined the cost-effectiveness of different fixation options for intertrochanteric hip fractures. They compared SHS and CMN implants using an expected-value decision-analysis model, taking into account fracture patterns, failure rates, and revision costs. In their study, the average cost of a SHS was
$2,000 compared to $3,200 for a standard CMN. They concluded that the SHS was likely more cost-effective for stable and questionably stable fractures compared to CMN fixation; CMN was more cost-effective for reverse obliquity patterns.
Kaplan et al. provided a review article on the surgical management of intertrochanteric fractures. Factors to determine treatment should include the patient's medical co-morbidities, pre-existing arthritis, bone quality, and fracture morphology. Their study did not find an appreciable difference in patient outcomes using either CMN or SHS for stable intertrochanteric fractures; surgeon experience and implant costs should, therefore, drive the decision making process for implant selection.
Figures A and B are AP and lateral right hip radiographs, respectively, demonstrating a standard obliquity intertrochanteric hip fracture. Illustration A is an AP post-operative radiograph showing a hip fracture treated with a SHS.
Incorrect Answers:
Answers 1 and 2: Both of these options are appropriate for this fracture but more costly than a SHS.
Answer 4: Arthroplasty is not indicated for this patient with an intertrochanteric fracture and preserved joint space.
Answer 5: Cannulated screws are not indicated for an intertrochanteric fracture.
Question 30High Yield
The examination suggests a neurologic deficit of which nerve?
Explanation
- Common peroneal nerve
Question 31High Yield
What would be the expected outcome following appropriate management of the injury revealed in Figures 1 and 2?
Explanation
■
The images reveal a displaced tibial eminence fracture in a skeletally immature patient. These represent anterior cruciate ligament (ACL)-equivalent injuries in children. Though the ACL elongates as part of the injury process, when the bony fragment is replaced and heals, the knee is usually functionally stable, and patients return to preinjury levels of activity without difficulty.
No long-term injury is expected, so there is no reason to expect inability to return to sports or strenuous activity. This injury heals with normal bone and does not predispose to reinjury. There is no evidence that a stable knee, which is expected after this injury, will lead to premature osteoarthritis.
■
The images reveal a displaced tibial eminence fracture in a skeletally immature patient. These represent anterior cruciate ligament (ACL)-equivalent injuries in children. Though the ACL elongates as part of the injury process, when the bony fragment is replaced and heals, the knee is usually functionally stable, and patients return to preinjury levels of activity without difficulty.
No long-term injury is expected, so there is no reason to expect inability to return to sports or strenuous activity. This injury heals with normal bone and does not predispose to reinjury. There is no evidence that a stable knee, which is expected after this injury, will lead to premature osteoarthritis.
Question 32High Yield
A 77-year-old man with a history of mild renal insufficiency and atrial fibrillation on warfarin therapy is scheduled to undergo a left total hip arthroplasty. He previously underwent a right total hip arthroplasty with development of significant heterotopic bone that resulted in limitation of motion. What is the most appropriate form of prophylactic treatment to minimize the formation of heterotopic bone on his left hip?

Explanation
DISCUSSION: This question centers on the prophylactic treatment to reduce the risk of heterotopic bone formation. Prophylaxis is indicated because he has already demonstrated bone formation with his prior hip arthroplasty, which places him at increased risk for developing heterotopic bone on the contralateral side. He is on warfarin and has renal insufficiency, which makes the use of NSAIDs contraindicated. The recommended dose is 600 to 800 centigrey of radiation given within 24 hours of surgery preoperatively or 72 hours postoperatively.
REFERENCES: Kolbl O, Knelles D, Barthel T, et al: Preoperative irradiation versus the use of nonsteroidal anti-inflammatory drugs for prevention of heterotopic ossification following total hip replacement: The results of a randomized trial. Int J Radiat Oncol Biol Phys 1998;42:397-401.
Pakos EE, Ioannidis JP: Radiotherapy vs nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip surgery: A meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys 2004;60:888-895.
Seegenschmiedt MH, Makoski HB, Micke O, et al: Radiation prophylaxis for heterotopic ossification about the hip joint: A multicenter study. Int J Radiat Oncol Biol Phys 2001 ;51:756-765.
Figure 23 a Figure 23b
DISCUSSION: This question centers on the prophylactic treatment to reduce the risk of heterotopic bone formation. Prophylaxis is indicated because he has already demonstrated bone formation with his prior hip arthroplasty, which places him at increased risk for developing heterotopic bone on the contralateral side. He is on warfarin and has renal insufficiency, which makes the use of NSAIDs contraindicated. The recommended dose is 600 to 800 centigrey of radiation given within 24 hours of surgery preoperatively or 72 hours postoperatively.
REFERENCES: Kolbl O, Knelles D, Barthel T, et al: Preoperative irradiation versus the use of nonsteroidal anti-inflammatory drugs for prevention of heterotopic ossification following total hip replacement: The results of a randomized trial. Int J Radiat Oncol Biol Phys 1998;42:397-401.
Pakos EE, Ioannidis JP: Radiotherapy vs nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip surgery: A meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys 2004;60:888-895.
Seegenschmiedt MH, Makoski HB, Micke O, et al: Radiation prophylaxis for heterotopic ossification about the hip joint: A multicenter study. Int J Radiat Oncol Biol Phys 2001 ;51:756-765.
Figure 23 a Figure 23b
Question 33High Yield
With a full-thickness articular cartilage injury, the body’s healing response produces cartilage mainly composed of what type of collagen?
Explanation
With a full-thickness articular cartilage injury, a healing response is initiated with hematoma, stem cell migration, and vascular ingrowth. This response produces type I collagen and resultant fibrous cartilage rather than desired hyaline cartilage as produced by chondrocytes. This repair cartilage has diminished resiliency, stiffness, poor wear characteristics, and the predilection for arthritis. Type I collagen is also found in the annulus of intervertebral disks, tendon, bone, meniscus, and skin. Type II is found in articular cartilage and nucleus pulposus of intervertebral disks. Type III is found in skin and blood vessels, type IV is found in basement membranes, and type X is found in the calcified layer of cartilage.
REFERENCES: Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Brinker M: Basic Science in Review of Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2000.
REFERENCES: Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Brinker M: Basic Science in Review of Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2000.
Question 34High Yield
..A 45-year-old woman with diabetes has a 3-month history of left shoulder pain and motion loss unrelated to trauma. She previously underwent treatment with nonsteroidal anti-inflammatory medication and a home stretching program, experiencing minimal relief of her symptoms. Examination reveals loss of passive external rotation, abduction, and forward elevation without reduction in strength. Radiograph findings are normal. What is the most appropriate next step?
Explanation
- Cortisone injection therapy with continued physical therapy (PT)
Question 35High Yield
..A 25-year-old man is planning to have an elbow contracture release. His elbow range of motion is 40 degrees to 90 degrees of flexion. He has no heterotopic ossification. His ring and small fingers become numb as his elbow approaches his flexion endpoint. There is no evidence of instability of the ulna-humeral or radioulnar joints. To achieve the best possible outcome, the surgeon should
Explanation
- decompress the ulnar nerve.
Question 36High Yield
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?
Explanation
The primary action of the posterior tibialis tendon is inversion of the foot; secondarily, it plantar flexes the ankle. The anterior tibialis tendon also inverts the foot and only partially antagonizes the posterior tibialis tendon. The primary action of the peroneus longus is plantar flexion of the first ray. It secondarily everts the posterior tibialis tendon. The action of the flexor digitorum longus tendon is synergistic with the posterior tibialis tendon. The primary action of the peroneus brevis tendon is eversion; therefore, it is the primary antagonist of the posterior tibialis tendon.
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Mann RA: Biomechanics of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 2-36.
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Mann RA: Biomechanics of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 2-36.
Question 37High Yield
Which combination of muscle weakness is typically associated with hereditary sensory motor neuropathy:
Explanation
The peroneus brevis is usually the first muscle to atrophy. Varying patterns of loss of the other muscles of the lower extremity include the anterior tibial and, in particular, the intrinsic foot muscles. Weakness in these muscles accounts for the cavus and the claw foot deformities noted in patients with hereditary sensory motor neuropathy.
Question 38High Yield
A 45-year-old woman diagnosed with lateral epicondylitis undergoes an open debridement of the extensor carpi radialis brevis. During surgery, resection extends posterior to the equator of the radiocapitellar joint. Postoperatively, she complains of persistent pain, despite appropriate rehabilitation. What other physical examination finding is she likely to have?
Explanation
Excessive resection of the common extensor origin posterior to the equator of the radiocapitellar joint may lead to iatrogenic lateral collateral ligament (LCL) injury, causing posterior lateral rotatory instability (PLRI). Patients may present with lateral elbow pain, a positive lateral pivot shift test, or mechanical symptoms/subjective instability when pushing up from a chair (positive chair rise test). PLRI is often provoked with combined elbow extension and forearm supination, as the posterior support for the radiocapitellar joint has been lost. Therefore, placing the forearm in pronation during elbow extension places the radiocapitellar joint in a more stable position and is less likely to induce pain or mechanical symptoms. Valgus instability and MCL tenderness would be associated with an MCL injury.
Question 39High Yield
On the morning of surgery the patient reports in the preop area that she has experienced skin breakdown over the second toe for 10 days. The extensor tendon is disrupted with an exposed proximal interphalangeal joint. She has been applying antibiotic ointment to the wound and denies fever or chills. What is the best plan of care?
Explanation
The clinical photograph shows a hallux valgus and a crossover toe deformity. The plantar plate must be damaged for a crossover toe deformity to develop. A moderately severe hallux valgus deformity without arthritic change is best treated with a bunionectomy with a proximal metatarsal osteotomy. The surgeon must assume that the open joint is at least colonized and at significant risk for postsurgical infection; consequently, it is best to cancel elective surgery, and surgical debridement of soft tissue and bone with deep cultures is recommended.
RECOMMENDED READINGS
[Kaz AJ, Coughlin MJ. Crossover second toe: demographics, etiology, and radiographic assessment. Foot Ankle Int. 2007 Dec;28(12):1223-37. doi: 10.3113/FAI.2007.1223. PubMed PMID: 18173985. ](http://www.ncbi.nlm.nih.gov/pubmed/18173985)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18173985)
[Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/ 1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23774466)
[Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. ](http://www.ncbi.nlm.nih.gov/pubmed/2613128)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2613128)
RECOMMENDED READINGS
[Kaz AJ, Coughlin MJ. Crossover second toe: demographics, etiology, and radiographic assessment. Foot Ankle Int. 2007 Dec;28(12):1223-37. doi: 10.3113/FAI.2007.1223. PubMed PMID: 18173985. ](http://www.ncbi.nlm.nih.gov/pubmed/18173985)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18173985)
[Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/ 1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23774466)
[Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. ](http://www.ncbi.nlm.nih.gov/pubmed/2613128)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2613128)
Question 40High Yield
Stemless shoulder arthroplasty prostheses have recently been suggested as an alternative to traditional stemmed replacement. Advantages of the stemless surgical technique would include
Explanation
DISCUSSION
Glenoid exposure, while better than with surface replacements, is not improved over traditional stemmed replacements. Metaphyseal comminution would make it unlikely that a stemless implant could be used in most four-part fractures. Stemless replacement does have the unique advantage of allowing placement of a prosthesis with a malunion without an osteotomy, as the prosthesis is not constrained by the position of the stem. While early results are encouraging, there is no long-term data to suggest that survivorship is increased
with stemless arthroplasty.
DISCUSSION
Glenoid exposure, while better than with surface replacements, is not improved over traditional stemmed replacements. Metaphyseal comminution would make it unlikely that a stemless implant could be used in most four-part fractures. Stemless replacement does have the unique advantage of allowing placement of a prosthesis with a malunion without an osteotomy, as the prosthesis is not constrained by the position of the stem. While early results are encouraging, there is no long-term data to suggest that survivorship is increased
with stemless arthroplasty.
Question 41High Yield
A 4-year-old boy has had an isolated painful limp for the past month. He is diagnosed with Legg-Calve-Perthes disease (LCPD) that involves nearly all of his capital femoral epiphysis. Which of the following best describes his prognosis?
Explanation
This young child with total head involvement LCPD is at some risk of a poor outcome due to the extent of his disease. Most children of this age will recover well with a good outcome. He is more likely to end up with a spherical femoral head than an older child with the same extent of involvement.
_AL-Madena Copy_
REFERENCES: Schoenecker PL, Stone JW, Capelli AM: Legg-Perthes disease in children under 6 years old. Orthop Rev 1993;22:201-208.
Rosenfeld SB, Herring JA, Chao JC: Legg-Calve-Perthes disease: A review of cases with onset before six years of age. J Bone Joint Surg Am 2007;89:2712-2722.
Figure 78
_AL-Madena Copy_
REFERENCES: Schoenecker PL, Stone JW, Capelli AM: Legg-Perthes disease in children under 6 years old. Orthop Rev 1993;22:201-208.
Rosenfeld SB, Herring JA, Chao JC: Legg-Calve-Perthes disease: A review of cases with onset before six years of age. J Bone Joint Surg Am 2007;89:2712-2722.
Figure 78
Question 42High Yield
What is the most appropriate diagnosis?
Explanation
- Charcot foot
Question 43High Yield
Figure 1 and 2 are the radiographs of a 5-year-old girl who is being evaluated for back pain and intermittent headaches. Her parents deny any injury, changes in bowel or bladder function, or significant family history. Her neurological exam is normal. What is the best next step in her management?

Explanation
■
This is a 5-year-old girl with a new diagnosis of scoliosis, having an isolated right thoracic curve. This is considered juvenile onset idiopathic scoliosis, which presents between the ages of 3-9 years old. The initial radiographs show a curve measuring 41°. Any curve >20° in a patient with early onset scoliosis should undergo MRI of the entire spine to assess for intraspinal pathology, with an average of 20% of patients having underlying diagnoses, i.e. Arnold-Chiari, syringomyelia. Observation or TLSO bracing may be indicated; however, an MRI is still the first line of management in this patient. Physical therapy may be useful for adjunct treatment, but the MRI is still required at this stage of evaluation and diagnosis.
■
This is a 5-year-old girl with a new diagnosis of scoliosis, having an isolated right thoracic curve. This is considered juvenile onset idiopathic scoliosis, which presents between the ages of 3-9 years old. The initial radiographs show a curve measuring 41°. Any curve >20° in a patient with early onset scoliosis should undergo MRI of the entire spine to assess for intraspinal pathology, with an average of 20% of patients having underlying diagnoses, i.e. Arnold-Chiari, syringomyelia. Observation or TLSO bracing may be indicated; however, an MRI is still the first line of management in this patient. Physical therapy may be useful for adjunct treatment, but the MRI is still required at this stage of evaluation and diagnosis.
Question 44High Yield
A 51-year-old male 2-pack per day smoker presents with a hyperkeratotic light brown plaque on the dorsum of his left ring finger that has been present for 7 years. It measures 14 mm by 13 mm. Initially, it responded to topical wart treatments, but has failed to do so recently so he sought evaluation by a dermatologist who biopsied the lesion. The results revealed squamous cell carcinoma (SCC) in situ, and he was referred for further surgical management. He has no other skin lesions, no history of SCC and no axillary lymphadenopathy. What is the next step in management?
Explanation
SCC in situ is a low-grade malignancy that typically presents as painless lesions on areas of high sun exposure such as the dorsum of the hand and fingers. The recommended treatment for lesions smaller than 100 mm is wide excision with 4 mm margins to a depth 1 layer below the tumor, along with any adjacent area of induration. Sentinel lymph node biopsy is typically not indicated in the setting of a low-grade tumor such as this one and in the absence of axillary lymphadenopathy.
Question 45High Yield
A 56-year-old man is brought to the emergency department by paramedics following a high-speed motor vehicle collision. He has obvious head trauma as seen by bilateral periorbital ecchymoses, substantial facial swelling, and a large bitemporal scalp laceration. He is not alert, but he is responsive to painful stimuli, and he moves all four extremities. What radiographic test would you order first to assess his cervical spine for potential injury?
Explanation
■
CT of the cervical spine is fast and readily available in most centers. The reported sensitivity of CT is greater than 95%, whereas specificity is almost 100%. In contrast, plain radiographs have a sensitivity of 70% and a missed injury rate of 15% to 30%. CT also has been found to be as cost effective or more cost effective compared with plain radiographs in diagnosing cervical injuries. MRI is expensive, not always readily available, and inferior to CT in diagnosing bony injuries. In this patient, dynamic imaging in the form of flexion-extension views is contraindicated as a first line radiographic test. The patient may have an unstable cervical injury which could be exacerbated with motion. The patient's mental status also does not allow voluntary motion. The maneuver would have to be done by the physician or radiology technician.
CT of the cervical spine is fast and readily available in most centers. The reported sensitivity of CT is greater than 95%, whereas specificity is almost 100%. In contrast, plain radiographs have a sensitivity of 70% and a missed injury rate of 15% to 30%. CT also has been found to be as cost effective or more cost effective compared with plain radiographs in diagnosing cervical injuries. MRI is expensive, not always readily available, and inferior to CT in diagnosing bony injuries. In this patient, dynamic imaging in the form of flexion-extension views is contraindicated as a first line radiographic test. The patient may have an unstable cervical injury which could be exacerbated with motion. The patient's mental status also does not allow voluntary motion. The maneuver would have to be done by the physician or radiology technician.
Question 46High Yield
Intraoperative frozen section analysis reveals 10 neutrophils per high-power field and a positive gram stain result. What is the best next step?
Explanation
The radiograph reveals a rotator cuff dysfunction secondary to malpositioning of the humeral stem and a nonanatomic humeral head. Glenohumeral kinematics have been altered, resulting in damage to the rotator cuff, which in turn has led to impingement with the coracoacromial arch. This single radiograph reveals excessive humeral head height, “overstuffing” of the joint, and severe narrowing of the acromiohumeral interval. Osteolysis and implant loosening are not radiographically apparent. An orthogonal view (axillary lateral) would be necessary to evaluate for shoulder instability. A CT arthrogram is the most appropriate advanced imaging test in the setting of a retained shoulder arthroplasty to evaluate the integrity of the rotator cuff. An MRI evaluation would be obfuscated by artifact. Three-phase and indium-tagged white blood cell scans may be appropriate in the setting of an occult infection evaluation, but not as a test to evaluate rotator cuff injury.
In the absence of infection with rotator cuff compromise, the most appropriate procedure(s) during revision would involve humeral component explantation and conversion to rTSA Revision anatomic hemiarthroplasty may provide pain relief, but function may not appreciably change because of the unbalanced forced couples of the rotator cuff complex. Placement of a glenoid component in the setting of an irreparable rotator cuff tear is contraindicated because rapid glenoid loosening will occur due to eccentric loading during active shoulder motion. Resection arthroplasty should be reserved for recalcitrant cases of infection because this procedure does not provide functional improvement.
In the event that frozen section analysis and positive gram stain results indicate an infection, the treating surgeon should remove all components, perform a thorough debridement and irrigation of suspect tissue, implant an antibiotic spacer, and perform a second-stage reconstruction when deemed appropriate (in light of laboratory studies, repeat shoulder aspiration, frozen section analysis, and arthroscopic soft-tissue biopsy findings). Irrigation and debridement with primary exchange/conversion of components remains inferior to 2-stage reconstruction for infection eradication. Resection arthroplasty remains a salvage procedure for resistant cases that preclude reimplantation and generally is performed for symptom control and sepsis prevention.
RECOMMENDED READINGS
1. [Bohsali KI, Wirth MA, Rockwood CA Jr. Complications of total shoulder arthroplasty. J Bone Joint Surg Am. 2006 Oct;88(10):2279-92. Review. PubMed PMID: 17015609. ](http://www.ncbi.nlm.nih.gov/pubmed/17015609)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17015609)
2. [Florschütz AV, Lane PD, Crosby LA. Infection after primary anatomic versus primary reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2015 Aug;24(8):1296-301. doi: 10.1016/j.jse.2014.12.036. Epub 2015 Feb 19. PubMed PMID: 25704211. ](http://www.ncbi.nlm.nih.gov/pubmed/25704211)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25704211)
3. [Padegimas EM, Maltenfort M, Ramsey ML, Williams GR, Parvizi J, Namdari S. Periprosthetic shoulder infection in the United States: incidence and economic burden. J Shoulder Elbow Surg. 2015 May;24(5):741-6. doi: 10.1016/j.jse.2014.11.044. Epub 2015 Jan 13. ](http://www.ncbi.nlm.nih.gov/pubmed/25595360)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25595360)
4. [Leung B, Horodyski M, Struk AM, Wright TW. Functional outcome of hemiarthroplasty compared with reverse total shoulder arthroplasty in the treatment of rotator cuff tear arthropathy. J Shoulder Elbow Surg. 2012 Mar;21(3):319-23. doi: 10.1016/j.jse.2011.05.023. Epub 2011 Aug 26. PubMed PMID: 21872496. ](http://www.ncbi.nlm.nih.gov/pubmed/21872496)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21872496)
5. [Iannotti JP, Spencer EE, Winter U, Deffenbaugh D, Williams G. Prosthetic positioning in total shoulder arthroplasty. J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):111S-121S. PubMed PMID: 15726070. ](http://www.ncbi.nlm.nih.gov/pubmed/15726070)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15726070)
6. [Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992 Apr;74(4):491-500. PubMed PMID: 1583043.](http://www.ncbi.nlm.nih.gov/pubmed/1583043)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1583043)
7. [Grosso MJ, Frangiamore SJ, Ricchetti ET, Bauer TW, Iannotti JP. Sensitivity of frozen section histology for identifying Propionibacterium acnes infections in revision shoulder arthroplasty. J Bone Joint Surg Am. 2014 Mar 19;96(6):442-7. doi: 10.2106/JBJS.M.00258. ](http://www.ncbi.nlm.nih.gov/pubmed/24647499)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24647499)
In the absence of infection with rotator cuff compromise, the most appropriate procedure(s) during revision would involve humeral component explantation and conversion to rTSA Revision anatomic hemiarthroplasty may provide pain relief, but function may not appreciably change because of the unbalanced forced couples of the rotator cuff complex. Placement of a glenoid component in the setting of an irreparable rotator cuff tear is contraindicated because rapid glenoid loosening will occur due to eccentric loading during active shoulder motion. Resection arthroplasty should be reserved for recalcitrant cases of infection because this procedure does not provide functional improvement.
In the event that frozen section analysis and positive gram stain results indicate an infection, the treating surgeon should remove all components, perform a thorough debridement and irrigation of suspect tissue, implant an antibiotic spacer, and perform a second-stage reconstruction when deemed appropriate (in light of laboratory studies, repeat shoulder aspiration, frozen section analysis, and arthroscopic soft-tissue biopsy findings). Irrigation and debridement with primary exchange/conversion of components remains inferior to 2-stage reconstruction for infection eradication. Resection arthroplasty remains a salvage procedure for resistant cases that preclude reimplantation and generally is performed for symptom control and sepsis prevention.
RECOMMENDED READINGS
1. [Bohsali KI, Wirth MA, Rockwood CA Jr. Complications of total shoulder arthroplasty. J Bone Joint Surg Am. 2006 Oct;88(10):2279-92. Review. PubMed PMID: 17015609. ](http://www.ncbi.nlm.nih.gov/pubmed/17015609)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17015609)
2. [Florschütz AV, Lane PD, Crosby LA. Infection after primary anatomic versus primary reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2015 Aug;24(8):1296-301. doi: 10.1016/j.jse.2014.12.036. Epub 2015 Feb 19. PubMed PMID: 25704211. ](http://www.ncbi.nlm.nih.gov/pubmed/25704211)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25704211)
3. [Padegimas EM, Maltenfort M, Ramsey ML, Williams GR, Parvizi J, Namdari S. Periprosthetic shoulder infection in the United States: incidence and economic burden. J Shoulder Elbow Surg. 2015 May;24(5):741-6. doi: 10.1016/j.jse.2014.11.044. Epub 2015 Jan 13. ](http://www.ncbi.nlm.nih.gov/pubmed/25595360)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25595360)
4. [Leung B, Horodyski M, Struk AM, Wright TW. Functional outcome of hemiarthroplasty compared with reverse total shoulder arthroplasty in the treatment of rotator cuff tear arthropathy. J Shoulder Elbow Surg. 2012 Mar;21(3):319-23. doi: 10.1016/j.jse.2011.05.023. Epub 2011 Aug 26. PubMed PMID: 21872496. ](http://www.ncbi.nlm.nih.gov/pubmed/21872496)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21872496)
5. [Iannotti JP, Spencer EE, Winter U, Deffenbaugh D, Williams G. Prosthetic positioning in total shoulder arthroplasty. J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):111S-121S. PubMed PMID: 15726070. ](http://www.ncbi.nlm.nih.gov/pubmed/15726070)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15726070)
6. [Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992 Apr;74(4):491-500. PubMed PMID: 1583043.](http://www.ncbi.nlm.nih.gov/pubmed/1583043)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1583043)
7. [Grosso MJ, Frangiamore SJ, Ricchetti ET, Bauer TW, Iannotti JP. Sensitivity of frozen section histology for identifying Propionibacterium acnes infections in revision shoulder arthroplasty. J Bone Joint Surg Am. 2014 Mar 19;96(6):442-7. doi: 10.2106/JBJS.M.00258. ](http://www.ncbi.nlm.nih.gov/pubmed/24647499)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24647499)
Question 47High Yield
Figures 20a and 20b are the radiographs of a 19-year-old woman who was involved in a motor vehicle accident. What mechanism of injury is most consistent with the injury?
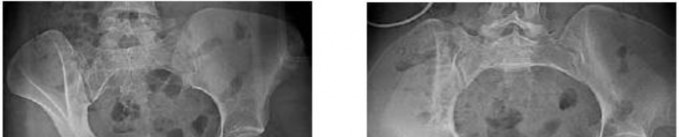


Explanation
No detailed explanation provided for this question.
Question 48High Yield
Anterior elbow release in children with cerebral palsy is likely to result in which of the following outcomes:
Explanation
Anterior elbow release consists of lengthening of the lacertus fibrosus and the brachialis fascia. It may or may not include lengthening of the biceps tendon itself. Anterior elbow release effectively decreases the excessive flexion posture of the elbow during use, which one author has termed the âflexion posture angle.â It does not result in decreased (or increased) strength of elbow flexion if the biceps tendon is preserved. Unfortunately, increased use during bimanual activity and increased grip strength are usually not observed.
Question 49High Yield
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course
of action?
of action?
Explanation
Lateral scapular winging is characteristic of trapezius palsy, whereas medial scapular winging is characteristic of long thoracic nerve palsy. During sports activity, injury to the spinal accessory nerve is rare but may occur with blunt or stretching trauma. Patients often report an asymmetric neckline, drooping shoulder, winging of the scapula, and weakness of forward elevation. Evaluation should include a complete electrodiagnostic examination.
REFERENCES: Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16.
Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27.
Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546.
Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Cohn BT, Brahms MA, Cohn M: Injury to the eleventh cranial nerve in a high school wrestler. Orthop Rev 1986;15:59-64.
REFERENCES: Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16.
Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27.
Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546.
Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Cohn BT, Brahms MA, Cohn M: Injury to the eleventh cranial nerve in a high school wrestler. Orthop Rev 1986;15:59-64.
Question 50High Yield
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?
Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon