Orthopedics Hyperguide Review | Dr Hutaif General Ortho -...
14 Apr 2026
57 min read
75 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedics Hyperguide Review | Dr Hutaif Gen...
00:00
Start Quiz
Question 1High Yield
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of
Explanation
The patient has a proximal synostosis; therefore, resection of the synostosis is considered the best option to regain motion. While forearm osteotomy can place the hand in a more functional position, rotation will not be restored. Proximal radial excision can provide forearm rotation; however, this procedure is reserved for patients who have a proximal radioulnar synostosis that is too extensive to allow a safe resection, involves the articular surface, and is associated with an anatomic deformity. Motion will not be restored with dynamic splinting.
REFERENCES: Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Jupiter JB, Ring D: Operative treatment of post-traumatic proximal radioulnar synostosis.
J Bone Joint Surg Am 1998;80:248-257.
REFERENCES: Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Jupiter JB, Ring D: Operative treatment of post-traumatic proximal radioulnar synostosis.
J Bone Joint Surg Am 1998;80:248-257.
Question 2High Yield
Injuries to what two structures would result in a “floating shoulder"?
Explanation
The superior shoulder suspensory complex (SSSC) is a bone and soft-tissue ring secured to the trunk by superior and inferior bony struts, from which the upper extremity is suspended. The ring is composed of the glenoid process, coracoid process, coracoclavicular ligaments, distal clavicle, acromioclavicular joint, and acromial process. Double lesions of the SSSC are referred to as “floating shoulder” injuries, as in this case in which the injury involves a fractured scapular neck and ipsilateral clavicle fracture. Ipsilateral acromioclavicular dislocation and coracoid fracture is a less common double disruption of the SSSC. Although several case studies have been published on surgical and nonsurgical management of these injuries, no study provides measurable surgical indications beyond the simple presence of the double lesion. This is often referred to as an unstable shoulder girdle.
47
47
Question 3High Yield
A 34-year-old woman twists her right ankle stepping off the city bus. An AP ankle radiograph is provided in Figure A. Which of the following statements accurately describe this radiograph?


Explanation
The AP radiograph demonstrates a stable, minimally displaced Weber B ankle fracture. It is consistent with a Lauge-Hansen supination-external rotation injury pattern.
Harper et al performed cadaveric measurements to define normal radiographic values for standard ankle imaging. The tibiofibular overlap is defined as the horizontal distance from the lateral border of the posterior tibial malleolus (the incisura fibularis) and the medial border of the fibula at the point where the posterior malleolus is widest on an AP radiograph should be great than 6 mm. Tibiofibular clear space is defined as the horizontal distance between the medial border of the fibula and the lateral border of the anterior tibial prominence on an AP radiograph, and should be <6mm. The medial clear space, defined as the distance between the lateral aspect of the medial malleolus and the medial border of the talus at the level of the talar dome on the mortise radiograph should be less than 4 mm.
Ostrum et al performed a radiographic study on human volunteers and noted gender differences. In this study, normal tibial clear space should be less than
5.2 mm in women and less than 6.5 mm in men. The tibiofibular overlap should be greater than 2.7 mm in women and greater than 5.7 mm in men.
Illustration A is an example of the proper measurement of the tib-fib clear space.
Harper et al performed cadaveric measurements to define normal radiographic values for standard ankle imaging. The tibiofibular overlap is defined as the horizontal distance from the lateral border of the posterior tibial malleolus (the incisura fibularis) and the medial border of the fibula at the point where the posterior malleolus is widest on an AP radiograph should be great than 6 mm. Tibiofibular clear space is defined as the horizontal distance between the medial border of the fibula and the lateral border of the anterior tibial prominence on an AP radiograph, and should be <6mm. The medial clear space, defined as the distance between the lateral aspect of the medial malleolus and the medial border of the talus at the level of the talar dome on the mortise radiograph should be less than 4 mm.
Ostrum et al performed a radiographic study on human volunteers and noted gender differences. In this study, normal tibial clear space should be less than
5.2 mm in women and less than 6.5 mm in men. The tibiofibular overlap should be greater than 2.7 mm in women and greater than 5.7 mm in men.
Illustration A is an example of the proper measurement of the tib-fib clear space.
Question 4High Yield
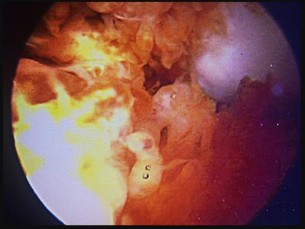
Figures 1 and 2 are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared with traditional arthroscopic techniques when evaluating which outcome?








Explanation
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the two techniques.
Question 5High Yield
The abrupt appearance of which of the following collagens heralds the onset of ossification in the physis:
Explanation
The terminal hypertrophiCchondrocytes in the hypertrophiCzone produce Type X collagen. The appearance of Type X collagen heralds ossification. Remember that Type II collagen is the most abundant collagen in the hypertrophiCzone
Question 6High Yield
An 11-year-old gymnast sustains a right dominant elbow dislocation. She undergoes a closed reduction in the emergency department with conscious sedation. Figures 1 and 2 are the postreduction radiographs. The best next step in treatment is

Explanation
■
The AP lateral radiographs show an incarcerated medial epicondyle. This is one of the absolute indications for surgical treatment of a displaced medial epicondyle fracture. The radiograph views show a nonconcentric reduction; therefore, immobilization without reduction will result in a painful stiff elbow. Although both MRI and CT scan will confirm the diagnosis, they are not necessary, are expensive, and a CT scan would expose the child to significant radiation.
Although controversy exists regarding surgical fixation of displaced nonincarcerated medial epicondyles, almost all surgeons agree that entrapped fragments should undergo open reduction and internal fixation. A number of fixation techniques are avaiable including divergent Kirschner wires, cannulated screws, suture anchors, and removal of the fragment with suture fixation. Screw fixation allows for shorter immobilization times and earlier motion.
■
The AP lateral radiographs show an incarcerated medial epicondyle. This is one of the absolute indications for surgical treatment of a displaced medial epicondyle fracture. The radiograph views show a nonconcentric reduction; therefore, immobilization without reduction will result in a painful stiff elbow. Although both MRI and CT scan will confirm the diagnosis, they are not necessary, are expensive, and a CT scan would expose the child to significant radiation.
Although controversy exists regarding surgical fixation of displaced nonincarcerated medial epicondyles, almost all surgeons agree that entrapped fragments should undergo open reduction and internal fixation. A number of fixation techniques are avaiable including divergent Kirschner wires, cannulated screws, suture anchors, and removal of the fragment with suture fixation. Screw fixation allows for shorter immobilization times and earlier motion.
Question 7High Yield
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?**
Explanation
Scapulothoracic dissociation is a rare, violent traumatic injury in which the scapula is torn away from the chest wall but the skin remains intact. Massive swelling and ecchymosis are common. Neurovascular injury is the rule with possible subclavian or axillary artery disruption and severe partial or complete brachial plexus paralysis. The diagnosis is made on a nonrotated chest radiograph that shows significant lateral displacement of the medial scapular border from the sternal notch. A right midshaft clavicular fracture is present but is not considered the most significant finding.
REFERENCES: Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432.
Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23.
Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Oreck SL, Burgess A, Levine AM: Traumatic lateral displacement of the scapula: A radiographic sign of neurovascular disruption. J Bone Joint Surg Am 1984;66:758-763.
REFERENCES: Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432.
Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23.
Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Oreck SL, Burgess A, Levine AM: Traumatic lateral displacement of the scapula: A radiographic sign of neurovascular disruption. J Bone Joint Surg Am 1984;66:758-763.
Question 8High Yield
Pagetâs disease is common in all of the listed locations except:
Explanation
Key features of Pagetâs disease
Remodeling disease caused by excessive osteoclastiCactivity
Rarely diagnosed in patients younger than 40 years of age; most patients diagnosed after age 50
Most common sites include pelvis, femur, spine, skull, and tibia
Less common sites include clavicles, scapulae, ribs, and facial bones
Rarely found in the hands and feet
PagetiCbone
is more susceptible to fracture is less compact
is more vascular
tends to bow in weight bearing areas
GeographiCclustering (up to 4% in patients older than 55 years of age) England
Northern Europe North America Australia, New Zealand
Rare in Asia, China, Indonesia, Malaysia, and sub-Saharan Africa
Possibly a slow viral disease
RNA paramyxovirus (e.g., respiratory syncytial virus and measles) Correct Answer: Sub-Saharan Africa
Remodeling disease caused by excessive osteoclastiCactivity
Rarely diagnosed in patients younger than 40 years of age; most patients diagnosed after age 50
Most common sites include pelvis, femur, spine, skull, and tibia
Less common sites include clavicles, scapulae, ribs, and facial bones
Rarely found in the hands and feet
PagetiCbone
is more susceptible to fracture is less compact
is more vascular
tends to bow in weight bearing areas
GeographiCclustering (up to 4% in patients older than 55 years of age) England
Northern Europe North America Australia, New Zealand
Rare in Asia, China, Indonesia, Malaysia, and sub-Saharan Africa
Possibly a slow viral disease
RNA paramyxovirus (e.g., respiratory syncytial virus and measles) Correct Answer: Sub-Saharan Africa
Question 9High Yield
Videos 1 and 2 are the coronal plane MRI scan and arthroscopic evaluation of a 48-year-old woman with 2 weeks of posterior knee pain after feeling a “pop” in the knee while climbing stairs. Physical examination reveals passive range of motion of +5° to 120°, with pain limiting her in terminal extension. Failure of surgical repair of the injured structure is most associated with
Explanation
The MRI scan and surgical video are showing an example of a posterior medial meniscal root tear/avulsion. Many studies have shown successful treatment of these tears with repair using various techniques and minimal progression to osteoarthritis (OA). Most studies exclude patients with high BMI. Brophy and associates demonstrated in their series that high BMI was associated with higher rates of clinical OA and need for subsequent surgery.
Multiple studies in the literature demonstrate good results with a variety of techniques. A valgus alignment in this setting would be considered protective, as opposed to a varus alignment >5°, which has also been associated with worse outcomes. The vascularity of the meniscus is consistently poor throughout most of its volume, including the root, and is not considered to be significantly different from person to person and should affect all root repairs equally.
Multiple studies in the literature demonstrate good results with a variety of techniques. A valgus alignment in this setting would be considered protective, as opposed to a varus alignment >5°, which has also been associated with worse outcomes. The vascularity of the meniscus is consistently poor throughout most of its volume, including the root, and is not considered to be significantly different from person to person and should affect all root repairs equally.
Question 10High Yield
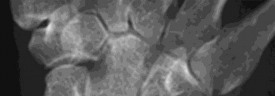
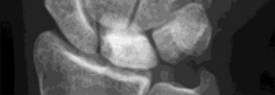
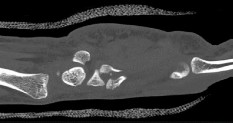
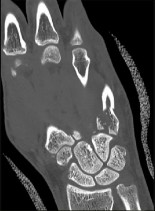
Figure 1 is the radiograph of a 22-year-old man who underwent an open reduction and pinning of a perilunate dislocation 10 weeks ago. The hardware has been removed. What is the best next step?
---
---
Explanation
Lunate or perilunate dislocations are usually treated with open reduction and internal fixation through a dorsal or combined dorsal and volar approach. A high index of suspicion is necessary when treating patients who sustain multiple trauma because as many as 25% of lunate or perilunate dislocations are missed initially. The radio dense appearance of the lunate seen in Figure 1 is an example of transient ischemia of the lunate that can occur following treatment of lunate and perilunate dislocations. It has been reported in up to 12.5% of cases. This usually is seen between 1 and 4 months post injury with a relative radio density of the lunate. This appearance of the lunate should not be over treated and usually is a benign self-limiting event. Surgery is not indicated at this time; the incorrect responses are treatment options for Kienbock disease. Treatment of the lunate or perilunate dislocation involves initial gentle closed reduction followed by open reduction, ligamentous and bone repair, and internal fixation. Median nerve dysfunction is common, and a simultaneous carpal tunnel release is often performed. Early treatment seems to produce better results, but good results have been reported when treatment is delayed for up to 6 months. The many questions regarding treatment of this problem involve the use of capsulodesis to supplement intercarpal ligament repair, repair/stabilization of the lunotriquetral interval vs no treatment of that articulation, and intercarpal fixation techniques. In delayed cases, proximal row carpectomy when the head of the capitate is intact and total wrist fusion if there are degenerative changes have been used. Chondral injuries are common, may not be recognized on radiographs, and may negatively affect longterm outcomes. Even when treatment is optimal, this injury is associated with a guarded prognosis and possible permanent partial loss of wrist motion and grip strength. At 10-year follow-up, radiographs will often demonstrate degenerative changes, but these changes do not always substantially negatively affect _hand function._
Question 11High Yield
Which of the following best describes the most common anatomic variation seen in the glenoid labrum and the middle glenohumeral ligament in the anterosuperior quadrant of the shoulder?
Explanation
Wide variations in the anatomy of the anterosuperior portion of the labrum and the middle glenohumeral ligament have been reported and are more common than previously thought. The labrum attached to the glenoid rim and a flat/broad middle glenohumeral ligament is the most common “normal” variation. A cord-like middle glenohumeral ligament is often associated with the presence of a sublabral hole. An anterosuperior labrum confluent with a cord-like middle glenohumeral ligament and no labral attachment to bone is the configuration of the Buford complex. The prevalence of each variation from one recent study is as follows: #1: 86.6%; #2: 3.3%; #3: 8.6%; and #4: 1.5%.
REFERENCES: Rao AG, Kim TK, Chronopoulos E, et al: Anatomical variants in the anterosuperior aspect of the glenoid labrum. J Bone Joint Surg Am 2003;85:653-659.
Ilahi OA, Labbe MR, Cosculluela P: Variants of the anterosuperior glenoid labrum and associated pathology. Arthroscopy 2002;18:882-886.
Williams MM, Snyder SJ, Buford D: The Buford complex-The “cord-like” middle glenohumeral ligament and absent anterosuprior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
REFERENCES: Rao AG, Kim TK, Chronopoulos E, et al: Anatomical variants in the anterosuperior aspect of the glenoid labrum. J Bone Joint Surg Am 2003;85:653-659.
Ilahi OA, Labbe MR, Cosculluela P: Variants of the anterosuperior glenoid labrum and associated pathology. Arthroscopy 2002;18:882-886.
Williams MM, Snyder SJ, Buford D: The Buford complex-The “cord-like” middle glenohumeral ligament and absent anterosuprior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 12High Yield
The next step in this patient’s workup should be
Explanation
- aspiration.
Question 13High Yield
When first seen in the emergency department, the patient with the injury seen in Figures 15a and 15b was not able to extend the wrist or the thumb. What is the best initial management?

Explanation
DISCUSSION: The injury is a type 3 supracondylar humerus firaacture with a radial nerve injury. Most nerve
injuries associated with fractures recover spontaneously within 6 to 12 weeks. Complete recovery is expected within 3 to 6 months. Closed reduction and percutaneous pinning is the recommended treatment for supracondylar fractures of the elbow. Cast treatment for displaced fractures carries a higher risk of associated compartment syndrome. There is no indication for exploring the radial nerve acutely. Open reduction is necessary only if the closed reduction fails.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 406-409.
Campbell CC, Water PM, Emans JB, et al: Neurovascular injury and displacement in type III
supracondylar humerus fractures. J Pediatr Orthop 1995;15:47-52.
**2010 Pediatric Orthopaedic Examination Answer Book • 19**
Figure 16
injuries associated with fractures recover spontaneously within 6 to 12 weeks. Complete recovery is expected within 3 to 6 months. Closed reduction and percutaneous pinning is the recommended treatment for supracondylar fractures of the elbow. Cast treatment for displaced fractures carries a higher risk of associated compartment syndrome. There is no indication for exploring the radial nerve acutely. Open reduction is necessary only if the closed reduction fails.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 406-409.
Campbell CC, Water PM, Emans JB, et al: Neurovascular injury and displacement in type III
supracondylar humerus fractures. J Pediatr Orthop 1995;15:47-52.
**2010 Pediatric Orthopaedic Examination Answer Book • 19**
Figure 16
Question 14High Yield
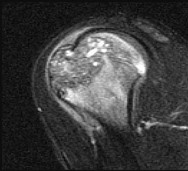
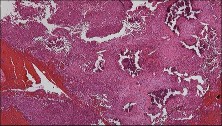
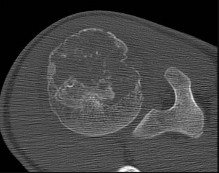
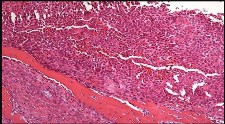
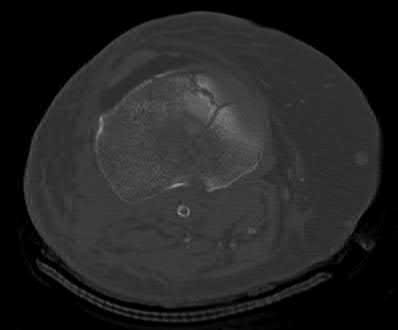
Figures 48a through 48e are the MR image, radiograph, CT scan, and biopsy specimens of a 14-year-old boy with right shoulder pain without antecedent trauma. What is the most likely diagnosis?


Explanation
Imaging reveals a destructive mineralized lesion of the epiphysis and metaphysis in a skeletally immature patient. Epiphyseal lesions include chondroblastoma in skeletally immature patients and giant-cell tumors in skeletally mature patients. The histology confirms the diagnosis with the presence of multinucleated giant cells, “chicken-wire” calcifications, and chondroid islands. Chondrosarcoma would look histologically more aggressive than this and is unusual in children. Unicameral bone cysts do not have mineralization and are typically confined to the metaphysis radiologically. Eosinophilic granuloma can mimic many different lesions radiographically and can occasionally be found in the epiphysis of children, but the histology does not demonstrate classic Langerhans cells.
RECOMMENDED READINGS
34. Wold LE, Unni KK, Sim FH, Sundaram M, Adler C-P, eds. _Atlas of Orthopedic Pathology_. 2nd edition. Philadelphia PA: Saunders; 2003:232:237.
35. [De Mattos CB, Angsanuntsukh C, Arkader A, Dormans JP. Chondroblastoma and chondromyxoid fibroma. J Am Acad Orthop Surg. 2013 Apr;21(4):225-33. doi: 10.5435/JAAOS-21-04-225. Review. PubMed PMID: 23545728.](http://www.ncbi.nlm.nih.gov/pubmed/23545728)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23545728)
CLINICAL SITUATION FOR QUESTIONS 49 AND 50
Figure 49 is the radiograph of a 22-year-old woman with pain and snapping about the knee. Her husband does not have this condition.
RECOMMENDED READINGS
34. Wold LE, Unni KK, Sim FH, Sundaram M, Adler C-P, eds. _Atlas of Orthopedic Pathology_. 2nd edition. Philadelphia PA: Saunders; 2003:232:237.
35. [De Mattos CB, Angsanuntsukh C, Arkader A, Dormans JP. Chondroblastoma and chondromyxoid fibroma. J Am Acad Orthop Surg. 2013 Apr;21(4):225-33. doi: 10.5435/JAAOS-21-04-225. Review. PubMed PMID: 23545728.](http://www.ncbi.nlm.nih.gov/pubmed/23545728)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23545728)
CLINICAL SITUATION FOR QUESTIONS 49 AND 50
Figure 49 is the radiograph of a 22-year-old woman with pain and snapping about the knee. Her husband does not have this condition.
Question 15High Yield
The most common cause of vascular injury during total hip arthroplasty (THA) is:
Explanation
A previous review of vascular injuries sustained during THA revealed the most common etiology of vascular injury as thromboemboliCphenomena, followed by laceration, pseudoaneurysm, and arteriovenous fistula
Question 16High Yield
Isolated subtalar fusion:
Explanation
In 48 subtalar fusions followed for 5 years, 36% of patients developed ankle arthritis and 41% of patients developed transverse tarsal joint arthritis.
Question 17High Yield
What is the most appropriate next step in the treatment of increasing forearm pain and new numbness?
Explanation
- Obtain forearm compartment pressure measurements_
Question 18High Yield
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
DISCUSSION:
Classic posterior elbow dislocations result from a posterolateral rotatory mechanism, whereby the hand is fixed (typically on the ground) while the weight of the body creates a valgus and external rotation moment on the elbow. This results first in tearing of the lateral collateral ligament that proceeds medially through the anterior and posterior joint capsules, ending with potential involvement of the ulnar collateral ligament (but this is not universal). McKee and associates assessed the lateral soft-tissue injury pattern of elbow dislocations
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
DISCUSSION:
Classic posterior elbow dislocations result from a posterolateral rotatory mechanism, whereby the hand is fixed (typically on the ground) while the weight of the body creates a valgus and external rotation moment on the elbow. This results first in tearing of the lateral collateral ligament that proceeds medially through the anterior and posterior joint capsules, ending with potential involvement of the ulnar collateral ligament (but this is not universal). McKee and associates assessed the lateral soft-tissue injury pattern of elbow dislocations
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 19High Yield
What is the function of the rotator cuff during throwing?
Explanation
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head.
Scientific References
- : Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
Question 20High Yield
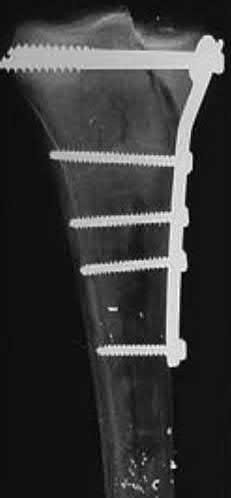
A 40-year-old male sustains a fall from a height. He sustains the isolated injury shown in the radiograph and CT images seen in Figures A through C. Surgery is planned. Which of the following constructs is the most appropriate definitive fixation for this injury?


Explanation
This patient has a medial tibial plateau fracture. Medial buttress plating (MBP) is indicated.
Medial tibial plateau fractures (Schatzker IV, Hohl and Moore II) may represent fracture dislocations of the knee. Neurovascular injuries must be excluded. In these instances, the medial fragment represents the stable fragment, and the rest of the tibia is the fractured fragment, with the entire leg acting as the lever arm.
Berkson et al. reviewed high energy tibial plateau fractures. Medial fractures may be treated with a medial plate or external fixation. Open reduction may be necessary because of fracture line obliquity and propensity of the medial plateau to shorten and rotate in the sagittal plane. Meniscal injuries should be repaired and avulsed cruciates fixed early. Collateral ligaments should be reconstructed after obtaining bone healing and range of motion.
Ratcliff et al. compared the stability of lateral locked plates and medial buttress plates in a cadaver model. They found that the medial buttress plate had greater fixation strength/failure force (4136N) compared with the lateral locking plate (2895N), although maximum cyclic displacement and residual displacement results were not different. They concluded that for vertically
orientated medial tibial plateau fractures, medial buttress plates were more stable.
Figure A is a radiograph showing a medial tibial plateau fracture extending across the tibial eminence. This is also classified as a Hohl and Moore Type II fracture. Figures B and C are coronal and axial CT scan images confirming the medial tibial plateau fracture and excluding a bicondylar fracture. Illustration A shows a medial tibial plateau fracture fixed with a medial buttress plate (cadaveric model with fibula removed). Illustration B shows the Hohl and Moore Type II fracture involving the entire condyle.
Incorrect Answers:
Answer 1: Lateral locked plating is biomechanically inferior to medial buttress plating for medial tibial plateau fractures (see reference above).
Answer 2: Medial bridge plating is appropriate for segmental or comminuted fractures
Answer 4: Lag screw fixation alone is contraindicated because of the long lever arm of the leg may lead to implant failure.
Answer 5: Temporary spanning external fixation may be appropriate for extensive comminution or soft tissue injury/swelling. Definitive external fixation (non-joint spanning) with olive wires, monolateral half-pins or both (hybrid) are possible options but less preferred as wires <14mm from the articular surface risk joint capsule penetration and septic arthritis.
Medial tibial plateau fractures (Schatzker IV, Hohl and Moore II) may represent fracture dislocations of the knee. Neurovascular injuries must be excluded. In these instances, the medial fragment represents the stable fragment, and the rest of the tibia is the fractured fragment, with the entire leg acting as the lever arm.
Berkson et al. reviewed high energy tibial plateau fractures. Medial fractures may be treated with a medial plate or external fixation. Open reduction may be necessary because of fracture line obliquity and propensity of the medial plateau to shorten and rotate in the sagittal plane. Meniscal injuries should be repaired and avulsed cruciates fixed early. Collateral ligaments should be reconstructed after obtaining bone healing and range of motion.
Ratcliff et al. compared the stability of lateral locked plates and medial buttress plates in a cadaver model. They found that the medial buttress plate had greater fixation strength/failure force (4136N) compared with the lateral locking plate (2895N), although maximum cyclic displacement and residual displacement results were not different. They concluded that for vertically
orientated medial tibial plateau fractures, medial buttress plates were more stable.
Figure A is a radiograph showing a medial tibial plateau fracture extending across the tibial eminence. This is also classified as a Hohl and Moore Type II fracture. Figures B and C are coronal and axial CT scan images confirming the medial tibial plateau fracture and excluding a bicondylar fracture. Illustration A shows a medial tibial plateau fracture fixed with a medial buttress plate (cadaveric model with fibula removed). Illustration B shows the Hohl and Moore Type II fracture involving the entire condyle.
Incorrect Answers:
Answer 1: Lateral locked plating is biomechanically inferior to medial buttress plating for medial tibial plateau fractures (see reference above).
Answer 2: Medial bridge plating is appropriate for segmental or comminuted fractures
Answer 4: Lag screw fixation alone is contraindicated because of the long lever arm of the leg may lead to implant failure.
Answer 5: Temporary spanning external fixation may be appropriate for extensive comminution or soft tissue injury/swelling. Definitive external fixation (non-joint spanning) with olive wires, monolateral half-pins or both (hybrid) are possible options but less preferred as wires <14mm from the articular surface risk joint capsule penetration and septic arthritis.
Question 21High Yield
A 68-year-old woman undergoes a hemiarthroplasty for a proximal humerus fracture through a deltopectoral approach. What
range of motion exercise should not be utilized in the immediate postoperative period due to concerns about lesser tuberosity fixation?
range of motion exercise should not be utilized in the immediate postoperative period due to concerns about lesser tuberosity fixation?
Explanation
Frankle et al found that passive external rotation of the shoulder placed the most stress on the lesser tuberosity fixation. The subscapularis tendon inserts on the lesser tuberosity and is the deforming force when placed under tension during external rotation. They also found that non-anatomic tuberosity reduction of 4-part proximal humerus fractures treated with hemiarthroplasty increased torque and impaired external rotation kinematics.
Question 22High Yield
A 4-year-old child has droopy shoulders. Examination shows that the child has a large head, short stature, and a narrow chest. Radiographs of the spine and chest show absent clavicles, delayed ossification of the pubis and ischium, and mild coxa vara. What is the inheritance pattern for this condition?
Explanation
DISCUSSION: The child has the clinical and radiographic features of cleidocranial dysostosis. This is a disorder of bones formed by intramembranous ossification. It is inherited as an autosomal-dominant condition. About two thirds of cases are familial.
REFERENCES: Dietz FR, Mathews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Joint Bone Surg Am 1996;78:1583-1598.
Lee B, Thirunavukkarasu K, Zhou L, et al: Missense mutations abolishing DNA binding of osteoblast- specific transcription factor OSF2/CBFA1 in cleidocranial dysplasia. Nat Genet 1997;16:307-310.
cU.u^Ml**_[**ORTHO MCQS 011 FREE BANK 02**](http://hutaifortho.com/878)_**
---
**_[**ORTHO MCQS 011 FREE BANK**](http://hutaifortho.com/877)_**
**_[**Orthopedic MCQS online Hip and knee ADULT...**](http://hutaifortho.com/876)_**
**_[**ORTHOPEDIC MCQS OB 20 TRAUMA1**](http://hutaifortho.com/875)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC5**](http://hutaifortho.com/874)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC7**](http://hutaifortho.com/873)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 6**](http://hutaifortho.com/872)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 44**](http://hutaifortho.com/871)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 4**](http://hutaifortho.com/870)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 3**](http://hutaifortho.com/869)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 2**](http://hutaifortho.com/868)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 1**](http://hutaifortho.com/867)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4**](http://hutaifortho.com/865)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3**](http://hutaifortho.com/864)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2**](http://hutaifortho.com/863)_**
**_[**1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW**](http://hutaifortho.com/862)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01**](http://hutaifortho.com/861)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01**](http://hutaifortho.com/860)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01**](http://hutaifortho.com/859)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02**](http://hutaifortho.com/858)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02**](http://hutaifortho.com/857)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02**](http://hutaifortho.com/856)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER FOOT 03**](http://hutaifortho.com/855)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER SPINE 03**](http://hutaifortho.com/854)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03**](http://hutaifortho.com/853)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER HIP 04**](http://hutaifortho.com/852)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER PEDS 04**](http://hutaifortho.com/851)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER SPORT 04**](http://hutaifortho.com/850)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05**](http://hutaifortho.com/849)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05**](http://hutaifortho.com/848)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05**](http://hutaifortho.com/847)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06**](http://hutaifortho.com/846)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...**](http://hutaifortho.com/845)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06**](http://hutaifortho.com/844)_**
**_[**ORTHOPEDIC MCQS with Answers ONLINE BASIC 06**](http://hutaifortho.com/843)_**
**_[**ORTHOPEDIC MCQS ONLINE PEDIATRICS 07**](http://hutaifortho.com/842)_**
**_[**ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07**](http://hutaifortho.com/841)_**
**_[**ONLINE ORTHOPEDIC MCQS SPORT07**](http://hutaifortho.com/840)_**
**_[**ONLINE ORTHOPEDIC MCQS UPPER LIMB08**](http://hutaifortho.com/839)_**
**_[**ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08**](http://hutaifortho.com/838)_**
**_[**ONLINE ORTHOPEDIC MCQS ANATOMY08**](http://hutaifortho.com/837)_**
**_[**ONLINE ORTHOPEDIC MCQS FOOT0 9**](http://hutaifortho.com/836)_**
**_[**ONLINE ORTHOPEDIC MCQS SPINE0 9**](http://hutaifortho.com/835)_**
**_[**ONLINE ORTHOPEDIC MCQS TRAUMA 9**](http://hutaifortho.com/834)_**
**_[**Orthopedic MCQS online sports Medicine**](http://hutaifortho.com/833)_**
**_[**Orthopedic MCQS online Shoulder and Elbow**](http://hutaifortho.com/832)_**
**_[**Orthopedic MCQS online Hip and knee**](http://hutaifortho.com/831)_**
**_[**online orthopedic mcqs**](http://hutaifortho.com/830)_**
**_[**Shoulder and elbow: Mcqs AND EMQS Answers**](http://hutaifortho.com/766)_**
**_[**Shoulder And Elbow: Questions Mcqs AND EMQS**](http://hutaifortho.com/765)_**
**_[**Hand and wrist: Answers MCQS EMQS**](http://hutaifortho.com/764)_**
**_[**Hand and wrist: MCQ AND EMQ Questions**](http://hutaifortho.com/763)_**
**_[**2021 SHOULDER AND ELBOW MCQS FREE**](http://hutaifortho.com/689)_**
**_[**Pediatric Orthopaedic MCQS Self-Assessment...**](http://hutaifortho.com/685)_**
**_[**Self-Assessment Examination 2020 Adult Spine MCQS**](http://hutaifortho.com/684)_**
**_[**Foot and Ankle free MCQS2020 Online**](http://hutaifortho.com/681)_**
**_[**UPDATED ORTHOPEDIC MCQS**](http://hutaifortho.com/680)_**
**_[**FREE Orthopedics MCQS 2022 1951.-2000.**](http://hutaifortho.com/677)_**
**_[**FREE Orthopedics MCQS 2022 1901.-1950.**](http://hutaifortho.com/676)_**
**_[**FREE Orthopedics MCQS 2022 1851-1900.**](http://hutaifortho.com/675)_**
**_[**FREE Orthopedics MCQS 2022 1751-1850..**](http://hutaifortho.com/674)_**
**_[**FREE Orthopedics MCQS 2022 1751-1800..**](http://hutaifortho.com/673)_**
**_[**Foot and Ankle FREE ORTHOPEDICS MCQS Question 11**](http://hutaifortho.com/672)_**
**_[**FREE Orthopedics MCQS 2022 1701-1750.**](http://hutaifortho.com/668)_**
**_[**FREE Orthopedics MCQS 2022 1651-1700**](http://hutaifortho.com/667)_**
**_[**FREE Orthopedics MCQS 2022 1601-1650.**](http://hutaifortho.com/666)_**
**_[**ORTHOPEDIC MCQS FREE 2023**](http://hutaifortho.com/665)_**
**_[**FREE Orthopedics MCQS 2022 1551-1600**](http://hutaifortho.com/664)_**
**_[**FREE Orthopedics MCQS 2022 1501-1550**](http://hutaifortho.com/663)_**
**_[**FREE Orthopedics MCQS 2022 1451-1500**](http://hutaifortho.com/662)_**
**_[**FREE Orthopedics MCQS 2022 1401-1450**](http://hutaifortho.com/661)_**
**_[**FREE Orthopedics MCQS 2022 1351 -1400**](http://hutaifortho.com/660)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350**](http://hutaifortho.com/659)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300**](http://hutaifortho.com/658)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200**](http://hutaifortho.com/656)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150**](http://hutaifortho.com/655)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100**](http://hutaifortho.com/654)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051**](http://hutaifortho.com/653)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 951-1000**](http://hutaifortho.com/652)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 901-950**](http://hutaifortho.com/651)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 851-900**](http://hutaifortho.com/650)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 800-850**](http://hutaifortho.com/649)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 751-800**](http://hutaifortho.com/647)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 701-750**](http://hutaifortho.com/646)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 651-700**](http://hutaifortho.com/645)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 601-650**](http://hutaifortho.com/644)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 551-600**](http://hutaifortho.com/643)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 501-550**](http://hutaifortho.com/642)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 451-500**](http://hutaifortho.com/641)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 401-450**](http://hutaifortho.com/640)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 351-400**](http://hutaifortho.com/639)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 301-350**](http://hutaifortho.com/638)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 251-300**](http://hutaifortho.com/637)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 201-250**](http://hutaifortho.com/636)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 151-200**](http://hutaifortho.com/635)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 101-150**](http://hutaifortho.com/634)_**
**_[**FREE Orthopedics MCQS 2022 51-100**](http://hutaifortho.com/633)_**
**_[**Orthopedics Hyperguide MCQ 1-50**](http://hutaifortho.com/631)_**
DISCUSSION: The child has the clinical and radiographic features of cleidocranial dysostosis. This is a disorder of bones formed by intramembranous ossification. It is inherited as an autosomal-dominant condition. About two thirds of cases are familial.
REFERENCES: Dietz FR, Mathews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Joint Bone Surg Am 1996;78:1583-1598.
Lee B, Thirunavukkarasu K, Zhou L, et al: Missense mutations abolishing DNA binding of osteoblast- specific transcription factor OSF2/CBFA1 in cleidocranial dysplasia. Nat Genet 1997;16:307-310.
cU.u^Ml
---
**_[**ORTHO MCQS 011 FREE BANK**](http://hutaifortho.com/877)_**
**_[**Orthopedic MCQS online Hip and knee ADULT...**](http://hutaifortho.com/876)_**
**_[**ORTHOPEDIC MCQS OB 20 TRAUMA1**](http://hutaifortho.com/875)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC5**](http://hutaifortho.com/874)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC7**](http://hutaifortho.com/873)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 6**](http://hutaifortho.com/872)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 44**](http://hutaifortho.com/871)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 4**](http://hutaifortho.com/870)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 3**](http://hutaifortho.com/869)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 2**](http://hutaifortho.com/868)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 1**](http://hutaifortho.com/867)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4**](http://hutaifortho.com/865)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3**](http://hutaifortho.com/864)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2**](http://hutaifortho.com/863)_**
**_[**1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW**](http://hutaifortho.com/862)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01**](http://hutaifortho.com/861)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01**](http://hutaifortho.com/860)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01**](http://hutaifortho.com/859)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02**](http://hutaifortho.com/858)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02**](http://hutaifortho.com/857)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02**](http://hutaifortho.com/856)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER FOOT 03**](http://hutaifortho.com/855)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER SPINE 03**](http://hutaifortho.com/854)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03**](http://hutaifortho.com/853)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER HIP 04**](http://hutaifortho.com/852)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER PEDS 04**](http://hutaifortho.com/851)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER SPORT 04**](http://hutaifortho.com/850)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05**](http://hutaifortho.com/849)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05**](http://hutaifortho.com/848)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05**](http://hutaifortho.com/847)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06**](http://hutaifortho.com/846)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...**](http://hutaifortho.com/845)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06**](http://hutaifortho.com/844)_**
**_[**ORTHOPEDIC MCQS with Answers ONLINE BASIC 06**](http://hutaifortho.com/843)_**
**_[**ORTHOPEDIC MCQS ONLINE PEDIATRICS 07**](http://hutaifortho.com/842)_**
**_[**ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07**](http://hutaifortho.com/841)_**
**_[**ONLINE ORTHOPEDIC MCQS SPORT07**](http://hutaifortho.com/840)_**
**_[**ONLINE ORTHOPEDIC MCQS UPPER LIMB08**](http://hutaifortho.com/839)_**
**_[**ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08**](http://hutaifortho.com/838)_**
**_[**ONLINE ORTHOPEDIC MCQS ANATOMY08**](http://hutaifortho.com/837)_**
**_[**ONLINE ORTHOPEDIC MCQS FOOT0 9**](http://hutaifortho.com/836)_**
**_[**ONLINE ORTHOPEDIC MCQS SPINE0 9**](http://hutaifortho.com/835)_**
**_[**ONLINE ORTHOPEDIC MCQS TRAUMA 9**](http://hutaifortho.com/834)_**
**_[**Orthopedic MCQS online sports Medicine**](http://hutaifortho.com/833)_**
**_[**Orthopedic MCQS online Shoulder and Elbow**](http://hutaifortho.com/832)_**
**_[**Orthopedic MCQS online Hip and knee**](http://hutaifortho.com/831)_**
**_[**online orthopedic mcqs**](http://hutaifortho.com/830)_**
**_[**Shoulder and elbow: Mcqs AND EMQS Answers**](http://hutaifortho.com/766)_**
**_[**Shoulder And Elbow: Questions Mcqs AND EMQS**](http://hutaifortho.com/765)_**
**_[**Hand and wrist: Answers MCQS EMQS**](http://hutaifortho.com/764)_**
**_[**Hand and wrist: MCQ AND EMQ Questions**](http://hutaifortho.com/763)_**
**_[**2021 SHOULDER AND ELBOW MCQS FREE**](http://hutaifortho.com/689)_**
**_[**Pediatric Orthopaedic MCQS Self-Assessment...**](http://hutaifortho.com/685)_**
**_[**Self-Assessment Examination 2020 Adult Spine MCQS**](http://hutaifortho.com/684)_**
**_[**Foot and Ankle free MCQS2020 Online**](http://hutaifortho.com/681)_**
**_[**UPDATED ORTHOPEDIC MCQS**](http://hutaifortho.com/680)_**
**_[**FREE Orthopedics MCQS 2022 1951.-2000.**](http://hutaifortho.com/677)_**
**_[**FREE Orthopedics MCQS 2022 1901.-1950.**](http://hutaifortho.com/676)_**
**_[**FREE Orthopedics MCQS 2022 1851-1900.**](http://hutaifortho.com/675)_**
**_[**FREE Orthopedics MCQS 2022 1751-1850..**](http://hutaifortho.com/674)_**
**_[**FREE Orthopedics MCQS 2022 1751-1800..**](http://hutaifortho.com/673)_**
**_[**Foot and Ankle FREE ORTHOPEDICS MCQS Question 11**](http://hutaifortho.com/672)_**
**_[**FREE Orthopedics MCQS 2022 1701-1750.**](http://hutaifortho.com/668)_**
**_[**FREE Orthopedics MCQS 2022 1651-1700**](http://hutaifortho.com/667)_**
**_[**FREE Orthopedics MCQS 2022 1601-1650.**](http://hutaifortho.com/666)_**
**_[**ORTHOPEDIC MCQS FREE 2023**](http://hutaifortho.com/665)_**
**_[**FREE Orthopedics MCQS 2022 1551-1600**](http://hutaifortho.com/664)_**
**_[**FREE Orthopedics MCQS 2022 1501-1550**](http://hutaifortho.com/663)_**
**_[**FREE Orthopedics MCQS 2022 1451-1500**](http://hutaifortho.com/662)_**
**_[**FREE Orthopedics MCQS 2022 1401-1450**](http://hutaifortho.com/661)_**
**_[**FREE Orthopedics MCQS 2022 1351 -1400**](http://hutaifortho.com/660)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350**](http://hutaifortho.com/659)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300**](http://hutaifortho.com/658)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200**](http://hutaifortho.com/656)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150**](http://hutaifortho.com/655)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100**](http://hutaifortho.com/654)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051**](http://hutaifortho.com/653)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 951-1000**](http://hutaifortho.com/652)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 901-950**](http://hutaifortho.com/651)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 851-900**](http://hutaifortho.com/650)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 800-850**](http://hutaifortho.com/649)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 751-800**](http://hutaifortho.com/647)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 701-750**](http://hutaifortho.com/646)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 651-700**](http://hutaifortho.com/645)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 601-650**](http://hutaifortho.com/644)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 551-600**](http://hutaifortho.com/643)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 501-550**](http://hutaifortho.com/642)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 451-500**](http://hutaifortho.com/641)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 401-450**](http://hutaifortho.com/640)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 351-400**](http://hutaifortho.com/639)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 301-350**](http://hutaifortho.com/638)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 251-300**](http://hutaifortho.com/637)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 201-250**](http://hutaifortho.com/636)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 151-200**](http://hutaifortho.com/635)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 101-150**](http://hutaifortho.com/634)_**
**_[**FREE Orthopedics MCQS 2022 51-100**](http://hutaifortho.com/633)_**
**_[**Orthopedics Hyperguide MCQ 1-50**](http://hutaifortho.com/631)_**
Question 23High Yield
A 28-year-old man has a progressive drop-foot deformity secondary to Charcot-Marie-Tooth disease.Examination reveals no tibialis anterior or peroneus brevis function. He has a 5-degree equinis contracture. Tibialis posterior and flexor digitorum longus are 5/5 strength. There are no fixed deformities of any joints. What is the most appropriate surgical option?
1/. A gastrocnemius lengthening and transfer of the tibialis posterior tendon to the dorsum of the foot
1/. A gastrocnemius lengthening and transfer of the tibialis posterior tendon to the dorsum of the foot

Explanation
At this point, the deformities are supple and fusions are not indicated. The tibialis posterior is the force couple or antagonist of peroneus brevis. With no peroneus brevis, the tibialis posterior is not only a deforming force, pulling the foot into inversion, but it is also the strongest muscle to use as an ankle dorsiflexor. By transferring it, the deforming force is removed and converted into an ankle dorsiflexor. With the equinis contracture, the gastrocnemius should be lengthened to allow the transferred tendon to dorsiflex the ankle beyond neutral.
---
---
Question 24High Yield
A 56-year-old woman sustains a type IIIB open tibial shaft fracture. She undergoes irrigation and debridement and intramedullary nailing with flap coverage 24 hours later. Cultures are taken pre-debridement and post-debridement. She develops a surgical site infection at 6 weeks, which requires removing the hardware and placing
show
Commented [1]:
an external fixator. Deep cultures are most likely to pathogens found in
show
Commented [1]:
an external fixator. Deep cultures are most likely to pathogens found in
Explanation
One study found only 8% of organisms grown on pre-debridement cultures eventually caused infection; 7% of cases with negative pre-debridement cultures became infected. Of cases that did become infected, pre-debridement cultures grew the infecting organism only 22% of the time. Post-debridement cultures were more accurate in predicting infection. However, of cases that became infected, the infecting organism was present on post-debridement cultures only 42% of the time. It is concluded that pre-debridement and post-debridement bacterial cultures from open fracture wounds are of essentially no value. It is recommended that they not be done.
In another study, before any interventions were performed, initial aerobic and anaerobic cultures of the wounds of 117 consecutive open extremity fractures grades I through III were obtained. The results of these cultures were correlated with the development of a wound infection. If an infection occurred, the organism grown from the infected wound was compared with any organism grown from the primary wound cultures. Of the initial cultures, 76% (89/117) did not demonstrate any growth, while the other 24% (28/117) only grew skin flora. There were only 7 (6%) wound infections, and 71% (5/7) initially did not grow any organisms. Of the isolates that grew from the initial cultures, none were the organisms that eventually led to
47
wound infections. The use of primary wound cultures in open extremity injuries has no value in the management of patients suffering from infections after long bone open extremity fractures.
In another study, before any interventions were performed, initial aerobic and anaerobic cultures of the wounds of 117 consecutive open extremity fractures grades I through III were obtained. The results of these cultures were correlated with the development of a wound infection. If an infection occurred, the organism grown from the infected wound was compared with any organism grown from the primary wound cultures. Of the initial cultures, 76% (89/117) did not demonstrate any growth, while the other 24% (28/117) only grew skin flora. There were only 7 (6%) wound infections, and 71% (5/7) initially did not grow any organisms. Of the isolates that grew from the initial cultures, none were the organisms that eventually led to
47
wound infections. The use of primary wound cultures in open extremity injuries has no value in the management of patients suffering from infections after long bone open extremity fractures.
Question 25High Yield
Figures 46a through 46e are the radiographs and CT scans of a 21-year-old right-hand-dominant man who injured his right hand in a martial arts competition 3 weeks before seeking treatment. An
examination reveals substantial ulnar-sided hand swelling and tenderness at the base of the fifth metacarpal. Digital flexion is nearly full with no malrotation. The most appropriate treatment is
examination reveals substantial ulnar-sided hand swelling and tenderness at the base of the fifth metacarpal. Digital flexion is nearly full with no malrotation. The most appropriate treatment is



Explanation
This fifth metacarpal base fracture is displaced, comminuted, and impacted. It is also associated with dorsal subluxation of the metacarpal on the hamate. The CT scan confirms the impaction of a sizable portion of the articular surface of the metacarpal base. In addition, the injury is 3 weeks old and is not likely to reduce by closed means. Open reduction, which would enable more accurate restoration of the articular surface, is necessary. If the patient had arrived for treatment earlier, a closed reduction percutaneous pinning may have been successful but may not have reduced the impacted articular segment. This injury usually results from a longitudinally directed force along the axis of the fifth metacarpal. Although a fifth CMC arthrodesis is an option, it likely is not appropriate as an initial treatment option and should be reserved for patients with painful posttraumatic arthritis.
RECOMMENDED READINGS
45. [Bora FW Jr, Didizian NH. The treatment of injuries to the carpometacarpal joint of the little finger. J Bone Joint Surg Am. 1974 Oct;56(7):1459-63. PubMed PMID: 4433366. ](http://www.ncbi.nlm.nih.gov/pubmed/4433366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4433366)
46. [Kjaer-Petersen K, Jurik AG, Petersen LK. Intra-articular fractures at the base of the fifth metacarpal. A clinical and radiographical study of 64 cases. J Hand Surg Br. 1992 Apr;17(2):144-7. PubMed PMID: 1588193. ](http://www.ncbi.nlm.nih.gov/pubmed/1588193)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1588193)
RECOMMENDED READINGS
45. [Bora FW Jr, Didizian NH. The treatment of injuries to the carpometacarpal joint of the little finger. J Bone Joint Surg Am. 1974 Oct;56(7):1459-63. PubMed PMID: 4433366. ](http://www.ncbi.nlm.nih.gov/pubmed/4433366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4433366)
46. [Kjaer-Petersen K, Jurik AG, Petersen LK. Intra-articular fractures at the base of the fifth metacarpal. A clinical and radiographical study of 64 cases. J Hand Surg Br. 1992 Apr;17(2):144-7. PubMed PMID: 1588193. ](http://www.ncbi.nlm.nih.gov/pubmed/1588193)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1588193)
Question 26High Yield
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history
of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. Unicompartmental knee arthroplasty (UKA) is discussed with the patient. The most appropriate next radiographic evaluation should be
of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. Unicompartmental knee arthroplasty (UKA) is discussed with the patient. The most appropriate next radiographic evaluation should be

Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 27High Yield
A 56-year-old diabetic male presents to the emergency department by ambulance after developing high-grade fevers, malaise, and altered mental status. Upon presentation, he is found to be hypotensive and initial labs show an elevated WBC with a profound left shift. Figure A shows skin manifestations confined to the foot at initial presentation. He is started on broad spectrum antibiotics. Upon followup exam 3 hours later his clinical condition deteriorates (Figure B) and he is taken to the operating room for surgical debridement. In a bacterial culture, what would be the most common single isolate for this condition?



Explanation
The above clinical vignette is describing necrotizing fasciitis. Necrotizing fasciitis is a rare and often fatal soft-tissue infection that requires high clinical suspicion and prompt administration of broad-spectrum antibiotics and aggressive surgical debridement (illustrations A). Fontes et al found that although polymicrobial infections including gram-positive, gram-negative, aerobic, and anaerobic bacteria were found most commonly in necrotizing fasciitis, Group A streptococcus was the most common bacterial isolate. Wong et al also found the most isolated organism to be group A streptococcus. In their study, the highest associated medical comorbidity was diabetes mellitus (71%). They found that delay in surgery of more than 24 hours was correlated with increased risk of death.
Question 28High Yield
A 79-year-old woman is seen for follow-up of a right arm posterior compartment high-grade soft-tissue sarcoma after undergoing wide resection of the tumor with preservation of the radial nerve
and minimal stripping of the posterior humeral periosteum. She then received 70 Gy of postsurgical radiation. Local recurrence occurred 4 years later, and she was treated with re-resection and adjuvant doxorubicin and ifosfamide chemotherapy. At that time, she learned she had osteoporosis and was treated with alendronate. She experienced an atraumatic fracture 2 years later without evidence of local recurrence. Which treatment poses highest risk for fracture in this scenario?
and minimal stripping of the posterior humeral periosteum. She then received 70 Gy of postsurgical radiation. Local recurrence occurred 4 years later, and she was treated with re-resection and adjuvant doxorubicin and ifosfamide chemotherapy. At that time, she learned she had osteoporosis and was treated with alendronate. She experienced an atraumatic fracture 2 years later without evidence of local recurrence. Which treatment poses highest risk for fracture in this scenario?
Explanation
Although postsurgical radiation is associated with lower rates of wound complication, radiation that is administered after surgery necessitates higher radiation doses and a larger tissue field than radiation administered before surgery. Risk for radiation-associated fracture increases with larger fields and higher doses. Retrospective studies have demonstrated increased fracture risk with postsurgical radiation doses of at least 60 Gy compared with presurgical radiation doses of 50 Gy. The influence of periosteal stripping on fracture risk is controversial. In a series of patients receiving primarily postsurgical radiation, extensive stripping was an accepted risk factor, but it was not found to be a significant risk factor in a more recent analysis of patients receiving lower-dose presurgical radiation. Cytotoxic chemotherapy is detrimental to healing of established fractures but does not correlate with risk for fracture in soft-tissue sarcoma. Chronic bisphosphonate use is associated with atypical fractures, but the location, timing, and radiographic appearance in this scenario are not consistent with this etiology.
RECOMMENDED READINGS
15. Gortzak Y, Lockwood GA, Mahendra A, Wang Y, Chung PW, Catton CN, O'Sullivan B, Deheshi BM, [Wunder JS, Ferguson PC. Prediction of pathologic fracture risk of the femur after combined modality treatment of soft tissue sarcoma of the thigh. Cancer. 2010 Mar 15;116(6):1553-9. doi: 10.1002/cncr.24949. PubMed PMID: 20108335.](http://www.ncbi.nlm.nih.gov/pubmed/20108335)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20108335)
16. Haas RL, Delaney TF, O'Sullivan B, Keus RB, Le Pechoux C, Olmi P, Poulsen JP, Seddon B, Wang
[D. Radiotherapy for management of extremity soft tissue sarcomas: why, when, and where? Int J Radiat Oncol Biol Phys. 2012 Nov 1;84(3):572-80. doi: 10.1016/j.ijrobp.2012.01.062. Epub 2012 Apr 18. Review. PubMed PMID: 22520481.](http://www.ncbi.nlm.nih.gov/pubmed/22520481)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22520481)
17. [Holt GE, Griffin AM, Pintilie M, Wunder JS, Catton C, O'Sullivan B, Bell RS. Fractures following radiotherapy and limb-salvage surgery for lower extremity soft-tissue sarcomas. A comparison of high-dose and low-dose radiotherapy. J Bone Joint Surg Am. 2005 Feb;87(2):315-9. PubMed PMID: 15687153. ](http://www.ncbi.nlm.nih.gov/pubmed/15687153)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15687153)
18. [Helmstedter CS, Goebel M, Zlotecki R, Scarborough MT. Pathologic fractures after surgery and radiation for soft tissue tumors. Clin Orthop Relat Res. 2001 Aug;(389):165-72. PubMed PMID: 11501806. ](http://www.ncbi.nlm.nih.gov/pubmed/11501806)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11501806)
CLINICAL SITUATION FOR QUESTIONS 35 THROUGH 37
Figure 35 is the intraoperative finding of a 28-year-old man with a recurrent nontraumatic effusion who undergoes arthroscopy.
RECOMMENDED READINGS
15. Gortzak Y, Lockwood GA, Mahendra A, Wang Y, Chung PW, Catton CN, O'Sullivan B, Deheshi BM, [Wunder JS, Ferguson PC. Prediction of pathologic fracture risk of the femur after combined modality treatment of soft tissue sarcoma of the thigh. Cancer. 2010 Mar 15;116(6):1553-9. doi: 10.1002/cncr.24949. PubMed PMID: 20108335.](http://www.ncbi.nlm.nih.gov/pubmed/20108335)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20108335)
16. Haas RL, Delaney TF, O'Sullivan B, Keus RB, Le Pechoux C, Olmi P, Poulsen JP, Seddon B, Wang
[D. Radiotherapy for management of extremity soft tissue sarcomas: why, when, and where? Int J Radiat Oncol Biol Phys. 2012 Nov 1;84(3):572-80. doi: 10.1016/j.ijrobp.2012.01.062. Epub 2012 Apr 18. Review. PubMed PMID: 22520481.](http://www.ncbi.nlm.nih.gov/pubmed/22520481)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22520481)
17. [Holt GE, Griffin AM, Pintilie M, Wunder JS, Catton C, O'Sullivan B, Bell RS. Fractures following radiotherapy and limb-salvage surgery for lower extremity soft-tissue sarcomas. A comparison of high-dose and low-dose radiotherapy. J Bone Joint Surg Am. 2005 Feb;87(2):315-9. PubMed PMID: 15687153. ](http://www.ncbi.nlm.nih.gov/pubmed/15687153)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15687153)
18. [Helmstedter CS, Goebel M, Zlotecki R, Scarborough MT. Pathologic fractures after surgery and radiation for soft tissue tumors. Clin Orthop Relat Res. 2001 Aug;(389):165-72. PubMed PMID: 11501806. ](http://www.ncbi.nlm.nih.gov/pubmed/11501806)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11501806)
CLINICAL SITUATION FOR QUESTIONS 35 THROUGH 37
Figure 35 is the intraoperative finding of a 28-year-old man with a recurrent nontraumatic effusion who undergoes arthroscopy.
Question 29High Yield
Figure 5 shows the deformity that developed in a 49-year-old woman who had previously undergone a bunion correction. The patient’s great toe is easily corrected to a neutral position but tends to spring back to a varus position. She reports pain in the first metatarsophalangeal joint and has difficulty wearing most shoes. What is the most appropriate management plan?
Explanation
Osteotomy and tendon transfer is the management of choice. The previous bunion correction resulted in excessive translation of the metatarsal head. The orthopaedic surgeon must first correct the bony deformity and allow the proximal phalanx to sit in a congruent position. The next step is to reconstruct the soft-tissue components and this can be done by releasing the medial capsule,and transferring part of the extensor hallucis longus tendon into the proximal phalanx, under the intermetatarsal ligament laterally. All three procedures are needed to adequately correct this deformity. A great toe fusion is indicated for an uncorrectable deformity or in an older patient.
Question 30High Yield
Figures 1 and 2 are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?

Explanation
■
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
Question 31High Yield
Figure 28 is the radiograph of a 14-year-old boy with an ankle injury.
Explanation
- CT scan
Question 32High Yield
A 21-year-old male is brought to the emergency department after being involved in gang-related violence. A radiograph of his pelvis is shown in Figure A. The patient is hemodynamically stable. Which of the following imaging modalities is the next best step in evaluating this patient for the most common associated injury?

Explanation
Low velocity gunshot wounds (GSW) to the hip are most commonly associated with bowel perforation. Consultation with general surgery (or in some facilities, trauma surgery) is necessary to exclude this.
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative
procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Answers 1, 3, 4: Urogenital and vascular injuries are not as common as bowel injuries.
Answer 5: Intraarticular bullet fragments should be removed to prevent lead toxicity (plumbism), which arises from fragments dissolving in synovial fluid. Other reasons for removal include prevention of third body wear, joint sepsis and lead arthropathy. It is not the priority in this case and exclusion of bowel injury must take precedence.
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative
procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Answers 1, 3, 4: Urogenital and vascular injuries are not as common as bowel injuries.
Answer 5: Intraarticular bullet fragments should be removed to prevent lead toxicity (plumbism), which arises from fragments dissolving in synovial fluid. Other reasons for removal include prevention of third body wear, joint sepsis and lead arthropathy. It is not the priority in this case and exclusion of bowel injury must take precedence.
Question 33High Yield
A 25-year-old professional soccer player presents with a chief complaint of left ankle pain. He has a history of a grade 3 lateral ankle sprain that was treated nonsurgically with rest and physical therapy approximately 4 months ago but has yet to return to play. He continues to report lateral-sided ankle pain and a mechanical snapping sensation. A current MRI scan is shown in Figure
Explanation
The patient's MRI scan reveals peroneal tendon dislocation. This is a relatively uncommon condition that tends to occur in young, athletic individuals frequently in the setting of a high-grade lateral ankle ligament sprain. The mechanism of injury is
thought to be a rapid forced dorsiflexion of the foot while in an inverted position leading to reflexive contraction of the peroneal tendons. This can lead to a disruption of the superior peroneal retinaculum and subsequently peroneal tendon subluxation or dislocation. Continued subluxation may lead to longitudinal split tears, particularly within the peroneal brevis tendon. Acute injuries in recreational athletes with reducible tendons may be treated with cast immobilization. Elite athletes with an acute injury may be treated with a 77
primary repair of the superior retinaculum; however, chronic injuries may require a fibular groove deepening procedure to reliably stabilize the tendons.
thought to be a rapid forced dorsiflexion of the foot while in an inverted position leading to reflexive contraction of the peroneal tendons. This can lead to a disruption of the superior peroneal retinaculum and subsequently peroneal tendon subluxation or dislocation. Continued subluxation may lead to longitudinal split tears, particularly within the peroneal brevis tendon. Acute injuries in recreational athletes with reducible tendons may be treated with cast immobilization. Elite athletes with an acute injury may be treated with a 77
primary repair of the superior retinaculum; however, chronic injuries may require a fibular groove deepening procedure to reliably stabilize the tendons.
Question 34High Yield
The iliopectineal fascia runs between which of the following structures? ](http://www.orthobullets.com/anatomy/10111/femoral-nerve)
Explanation
No detailed explanation provided for this question.
Question 35High Yield
After full healing from this injury, which option most likely will help to optimize this patient's activities?
Explanation
Midfoot fracture dislocations typically occur after a fall from a height or a motor vehicle collision involving severe dorsiflexion loading of the foot from a brake pedal or the floorboards. The deformity that results may be subtle because the subluxation may be a valgus or varus rotation around the midfoot rather than pure dorsiflexion. Early recognition and reduction is indicated to minimize secondary complications such as nerve injury or vascular compromise. Closed reduction usually necessitates formal anesthesia in an operating room to permit adequate relaxation and reduction. In many cases, satisfactory reduction can be accomplished closed, but the surgeon must be prepared to perform an open reduction if needed. The most common reason for failed closed reduction is that the talar head is caught by the tibialis posterior tendon (under which the talar head has protruded). This acts as a Chinese finger trap, preventing relocation by the usual distraction followed by
a plantar flexion maneuver. In these cases, open reduction is performed through a dorsomedial incision through which the tibialis posterior is retracted medially, allowing reduction of the talonavicular joint. The joints usually require pinning to maintain stability during healing. The long-term prognosis for these injuries is guarded because many patients develop degenerative changes in the Chopart joint. If symptomatic arthritis develops, helpful external supports are designed to limit sagittal motion at the joint (for example, carbon fiber inserts or rocker-bottom soles).
RECOMMENDED READINGS
[Swords MP, Schramski M, Switzer K, Nemec S. Chopart fractures and dislocations. Foot Ankle Clin. 2008 Dec;13(4):679-93, viii. Doi: 10.1016/j.fcl.2008.08.004. Review. PubMed PMID: 19013402.](http://www.ncbi.nlm.nih.gov/pubmed/19013402)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19013402)
[Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: initial open reduction provides better outcome than closed reduction. Foot Ankle Int. 2004 May;25(5):340-8. PubMed PMID: 15134617. ](http://www.ncbi.nlm.nih.gov/pubmed/15134617)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15134617)
a plantar flexion maneuver. In these cases, open reduction is performed through a dorsomedial incision through which the tibialis posterior is retracted medially, allowing reduction of the talonavicular joint. The joints usually require pinning to maintain stability during healing. The long-term prognosis for these injuries is guarded because many patients develop degenerative changes in the Chopart joint. If symptomatic arthritis develops, helpful external supports are designed to limit sagittal motion at the joint (for example, carbon fiber inserts or rocker-bottom soles).
RECOMMENDED READINGS
[Swords MP, Schramski M, Switzer K, Nemec S. Chopart fractures and dislocations. Foot Ankle Clin. 2008 Dec;13(4):679-93, viii. Doi: 10.1016/j.fcl.2008.08.004. Review. PubMed PMID: 19013402.](http://www.ncbi.nlm.nih.gov/pubmed/19013402)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19013402)
[Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: initial open reduction provides better outcome than closed reduction. Foot Ankle Int. 2004 May;25(5):340-8. PubMed PMID: 15134617. ](http://www.ncbi.nlm.nih.gov/pubmed/15134617)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15134617)
Question 36High Yield
A 19-year-old collegiate lacrosse player stumbles to the sideline after a collision with an opposing player during the first quarter of a game. She complains of dizziness and is disoriented to place and time. She initially shows disturbances in balance. The player is diagnosed as having sustained a concussion and is removed from the rest of the game. What should the coaching staff be advised of regarding the player’s return to activity?
Explanation
Concussions can be defined as a traumatically induced transient disturbance of brain function. There is currently no consensus regarding the definition of a concussion, nor is a there a defined biomechanical threshold of a concussion. Concussions occur when either linear and/or rotational forces are transmitted to the brain. A complex disturbance in neurometabolic activity follows. Until normal metabolic activity is restored, a second injury can result in worsening metabolic changes and significant cognitive defects. Given this reasoning, under no circumstances should an athlete be allowed same-day return to physical activity. In terms of return to play, studies have shown that strict rest may actually delay recovery and prolong symptoms. Most studies recommend a 24 to 48 hour period of symptom limited cognitive and physical rest, followed by sub-symptom threshold light aerobic activity.
20
20
Question 37High Yield
If nonsurgical treatment of this wound fails, the most likely cause for failure is
Explanation
- underlying osteomyelitis.
Question 38High Yield
During fracture repair systemiCas well as local factors come into play. Which of the following is considered a systemiCfactor in fracture healing:
Explanation
The degree of vascular injury is considered a local factor in fracture healing. Other such factors include degree of local trauma, type of bone affected, degree of bone loss, degree of immoblization, infection and local pathologiCconditions. SystemiCfactors include age of the patient, hormone function, functional activity, nerve function and nutritional state
Question 39High Yield
A 36-year-old woman has neck pain in the upper cervical region and occipital discomfort after being involved in a motor vehicle accident. Examination reveals no forehead or scalp lacerations. The neurologic examination is normal. A CT scan shows no evidence of bony injury. Figures 39a and 39b show a lateral radiograph and an MRI scan. Management should consist of
Explanation
The lateral radiograph shows 8 mm of atlantoaxial translation. In the absence of a bony injury, this represents rupture of the transverse atlantal ligament. The MRI scan reveals soft-tissue swelling posterior to the odontoid and a high intensity zone in the atlanto-dens interval consistent with acute injury. These injuries require arthrodesis because nonsurgical measures will not provide stability. Techniques for C1-2 fusion include Gallie, Brooks, or triple wiring. Transarticular screw fixation across the C1-2 articulation provides the most rigid means of fixation and the highest arthrodesis rates but is technically demanding. Anterior C2-3 arthrodesis will not address the level of instability. The normal atlanto-dens interval is 3 mm in an adult and 4 mm in a child.
REFERENCES: Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed):
The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Fielding JW, Cochran GB, Lansing JF III, et al: Tears of the transverse ligament of the atlas:
A clinical and biomechanical study. J Bone Joint Surg Am 1974;56:1683-1691.
REFERENCES: Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed):
The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Fielding JW, Cochran GB, Lansing JF III, et al: Tears of the transverse ligament of the atlas:
A clinical and biomechanical study. J Bone Joint Surg Am 1974;56:1683-1691.
Question 40High Yield
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
Creatine is currently used as a nutritional supplement in an attempt to enhance athletic performance. The physiologic basis for its use is based on its conversion by CK to PCr, which acts as an energy reservoir in muscle cells for the production of ATP. A number of studies that examined the effect of creatine supplementation on performance concluded that while creatine does not increase peak force production, it can increase the amount of work done in the first few anaerobic short duration, maximal effort trials. The mechanism for this enhancement of work is unknown, but it is most likely secondary to the increase in the available PCr pool.
REFERENCES: Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110.
Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571.
Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL: Muscle creatine loading in men. J Appl Physiol 1996;81:232-237.
REFERENCES: Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110.
Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571.
Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL: Muscle creatine loading in men. J Appl Physiol 1996;81:232-237.
Question 41High Yield
Figures 1 and 2 show the intraoperative photographs obtained from a man who is undergoing open reduction and internal fixation of a fifth carpometacarpal joint fracture dislocation. If the structure marked with an arrow in Figure 2 is cut, the patient can expect to experience
---
---












Explanation
The arrow in Figure 2 marks the dorsal sensory branch of the ulnar nerve. Injury to this nerve results in sensory loss of the dorsal ulnar palm and the dorsal small and ring finger digits. The dorsal sensory branch of the ulnar nerve exits the main ulnar nerve at an average distance of 8.3 cm from the proximal border of the pisiform. It becomes subcutaneous on the ulnar aspect of the forearm at an average distance of 5
cm from the proximal edge of the pisiform. It then travels dorsal to the extensor carpi ulnaris tendon to innervate the dorsal ulnar hand and the dorsal ring and small digits. Injuries to this nerve can occur from open and arthroscopic procedures (such as triangular fibrocartilage complex repair) as well as from procedures requiring percutaneous pinning. Care must be taken to identify and protect this nerve to avoid the complications of numbness and possible neuroma formation. The inability to extend the small finger would be caused by an injury to the extensor tendon(s) in this area, and the inability to abduct the small finger would require an injury to the abductor digiti minimi muscle/tendon unit or the ulnar nerve motor branch, which is located on the volar aspect of the proximal palm. Clawing of the small and ring fingers would be caused by absent intrinsic function due to an injury to the ulnar motor nerve branch located on _the volar proximal palm._
cm from the proximal edge of the pisiform. It then travels dorsal to the extensor carpi ulnaris tendon to innervate the dorsal ulnar hand and the dorsal ring and small digits. Injuries to this nerve can occur from open and arthroscopic procedures (such as triangular fibrocartilage complex repair) as well as from procedures requiring percutaneous pinning. Care must be taken to identify and protect this nerve to avoid the complications of numbness and possible neuroma formation. The inability to extend the small finger would be caused by an injury to the extensor tendon(s) in this area, and the inability to abduct the small finger would require an injury to the abductor digiti minimi muscle/tendon unit or the ulnar nerve motor branch, which is located on the volar aspect of the proximal palm. Clawing of the small and ring fingers would be caused by absent intrinsic function due to an injury to the ulnar motor nerve branch located on _the volar proximal palm._
Question 42High Yield
Figure A shows intra-operative radiographs of a 44-year-old male patient that has undergone fracture fixation of an acute elbow dislocation. Examination under anesthesia in the operating room reveals there is residual posterolateral instability when the elbow is extended < 35°. What would be the next most appropriate step in the management of his injury?

Explanation
This patient has sustained a terrible triad injury. He has undergone successful fixation of the radial head and coronoid fractures, but has residual posterolateral instability. The next most appropriate step in the management would be repairing the LCL in the operating room.
The step-wise principles for the operative management of terrible triad injuries include, (1) restore coronoid stability through fracture fixation or capsular repair, (2) restore radial head stability through fracture fixation or replacement with a metal prosthesis, (3) restore lateral elbow stability through repair of the lateral collateral ligament (LCL) complex (4) repair the medial collateral ligament (MCL) in patients with residual posterior instability, and (5) apply a hinged external fixator when conventional repair did not establish sufficient joint stability to allow early motion.
Pugh et al. provided a surgical protocol for elbow dislocations with associated radial head and coronoid fractures. They showed that early intervention, stable fixation, and repair would provide sufficient stability to allow motion in patients postoperatively and enhance functional outcomes. Prolonged immobilization following an acute episode of elbow instability is associated with poor results.
Ring et al. retrospectively reviewed eleven patients that underwent operative fixation of terrible triad injuries. At two year follow-up, three patients were considered to have a failure of the initial treatment. There was significant loss of elbow range of motion with an average of 92 degrees (range, 40 degrees to 130 degrees) of ulnohumeral motion.
Schneeberger et al. examined the role of the radial head and coronoid process as posterolateral rotatory stabilizers of the elbow. Excision of the radial head in an elbow with intact collateral ligaments caused a mean posterolateral rotatory laxity of 18.6 degrees (p < 0.0001) compared to 5.4 degrees in the intact elbows. Additional removal of 30% of the height of the coronoid fully destabilized the elbows, always resulting in ulnohumeral dislocation despite intact ligaments.
Figure A shows intraoperative radiographs following open reduction internal fixation of the coronoid fracture and radial head fracture.
Incorrect Answer:
Answer 1: Prolonged immobilization following an acute episode of elbow instability is associated with poor results.
Answer 2: A hinged brace would not address the residual posterolateral instability in this patient. Surgical repair of LCL +/- MCL +/- application of external fixator would be required, sequentially, until elbow stability is restored.
Answer 4: Medial collateral ligament repair is indicated in patients with residual instability after fixing the lateral collateral ligament complex.
Answer 5: Application of an elbow external fixator would be the final step in the surgical algorithm to maintain elbow stability after the medial collateral ligament is repaired.
The step-wise principles for the operative management of terrible triad injuries include, (1) restore coronoid stability through fracture fixation or capsular repair, (2) restore radial head stability through fracture fixation or replacement with a metal prosthesis, (3) restore lateral elbow stability through repair of the lateral collateral ligament (LCL) complex (4) repair the medial collateral ligament (MCL) in patients with residual posterior instability, and (5) apply a hinged external fixator when conventional repair did not establish sufficient joint stability to allow early motion.
Pugh et al. provided a surgical protocol for elbow dislocations with associated radial head and coronoid fractures. They showed that early intervention, stable fixation, and repair would provide sufficient stability to allow motion in patients postoperatively and enhance functional outcomes. Prolonged immobilization following an acute episode of elbow instability is associated with poor results.
Ring et al. retrospectively reviewed eleven patients that underwent operative fixation of terrible triad injuries. At two year follow-up, three patients were considered to have a failure of the initial treatment. There was significant loss of elbow range of motion with an average of 92 degrees (range, 40 degrees to 130 degrees) of ulnohumeral motion.
Schneeberger et al. examined the role of the radial head and coronoid process as posterolateral rotatory stabilizers of the elbow. Excision of the radial head in an elbow with intact collateral ligaments caused a mean posterolateral rotatory laxity of 18.6 degrees (p < 0.0001) compared to 5.4 degrees in the intact elbows. Additional removal of 30% of the height of the coronoid fully destabilized the elbows, always resulting in ulnohumeral dislocation despite intact ligaments.
Figure A shows intraoperative radiographs following open reduction internal fixation of the coronoid fracture and radial head fracture.
Incorrect Answer:
Answer 1: Prolonged immobilization following an acute episode of elbow instability is associated with poor results.
Answer 2: A hinged brace would not address the residual posterolateral instability in this patient. Surgical repair of LCL +/- MCL +/- application of external fixator would be required, sequentially, until elbow stability is restored.
Answer 4: Medial collateral ligament repair is indicated in patients with residual instability after fixing the lateral collateral ligament complex.
Answer 5: Application of an elbow external fixator would be the final step in the surgical algorithm to maintain elbow stability after the medial collateral ligament is repaired.
Question 43High Yield
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
The PCL is a nonisometric structure with nonuniform tension during knee motion, with maximum tension at 90° of flexion. While the posteromedial PCL fibers have been found to be the most isometric, the anterolateral fibers represent the bulk of the ligament. Studies have suggested that anterior placement of the femoral tunnel is superior to placement in an isometric position. The anterolateral bundle tightens as the knee flexes; therefore, it is optimal to tension the graft at 90° of flexion.
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
Question 44High Yield
A patient with spondyloepiphyseal dysplasia congenita reaches the age of 5 without being able to walk with a walker. She has five beats of clonus in both ankles. Her reflexes are brisk and her toes are upgoing. The most likely problem that accounts for these findings is:
Explanation
Atlantoaxial instability, sometimes combined with stenosis of the atlas, is a frequent cause of myelopathy in spondyloepiphyseal dysplasia congenita.
Scoliosis does not account for developmental delay or myelopathy.
Foramen magnum stenosis is rare in spondyloepiphyseal dysplasia congenita.
Lumbar stenosis is rare with spondyloepiphyseal dysplasia congenita and would not account for myelopathy. Thoracolumbar kyphosis severe enough to cause myelopathy is rare in spondyloepiphyseal dysplasia congenita condition.
Scoliosis does not account for developmental delay or myelopathy.
Foramen magnum stenosis is rare in spondyloepiphyseal dysplasia congenita.
Lumbar stenosis is rare with spondyloepiphyseal dysplasia congenita and would not account for myelopathy. Thoracolumbar kyphosis severe enough to cause myelopathy is rare in spondyloepiphyseal dysplasia congenita condition.
Question 45High Yield
Alternating single-leg-stance radiographs are most helpful for evaluation of which of the following diagnoses?
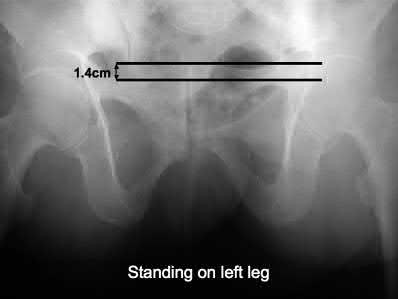
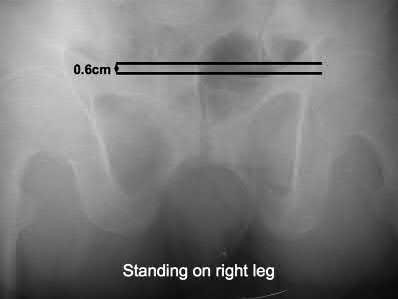
Explanation
Alternating single-leg-stance radiographs are used for the diagnosis of chronic or subtle pelvic instability.
Pelvic instability is a rare etiology of lumbar and low-back discomfort; patients report subjective instability and mechanical symptoms. Static radiographs (AP pelvis, inlet pelvis, outlet pelvis) are often not adequate for diagnosis of this condition.
Garras et al. performed a study of healthy volunteers and reported on the normal range of physiologic motion with single leg stance radiographs. They found that multiparous women exhibited the most symphyseal motion with alternating single leg stance weightbearing AP pelvic radiographs, and up to 5mm of symphyseal translation was seen in healthy, asymptomatic patients.
Siegel et al. reviewed 38 patients with pelvic instability and pain. They found that single leg stance radiographs were more indicative of instability than standard AP pelvis and inlet/outlet radiographs. They found that up to 5 cm of sympyhseal translation can be present with these injuries.
Illustration A shows a single leg stance (left leg) AP pelvis radiograph with cephalad displacement of the left hemipelvis. Illustration B shows a single leg stance (right leg) AP pelvis radiograph, with cephalad displacement of the right hemipelvis.
Incorrect Answers:
Answer 1,3,4,5: Standing alternating single-leg-stance radiographs are not used for diagnosis or evaluation of these disorders.
Pelvic instability is a rare etiology of lumbar and low-back discomfort; patients report subjective instability and mechanical symptoms. Static radiographs (AP pelvis, inlet pelvis, outlet pelvis) are often not adequate for diagnosis of this condition.
Garras et al. performed a study of healthy volunteers and reported on the normal range of physiologic motion with single leg stance radiographs. They found that multiparous women exhibited the most symphyseal motion with alternating single leg stance weightbearing AP pelvic radiographs, and up to 5mm of symphyseal translation was seen in healthy, asymptomatic patients.
Siegel et al. reviewed 38 patients with pelvic instability and pain. They found that single leg stance radiographs were more indicative of instability than standard AP pelvis and inlet/outlet radiographs. They found that up to 5 cm of sympyhseal translation can be present with these injuries.
Illustration A shows a single leg stance (left leg) AP pelvis radiograph with cephalad displacement of the left hemipelvis. Illustration B shows a single leg stance (right leg) AP pelvis radiograph, with cephalad displacement of the right hemipelvis.
Incorrect Answers:
Answer 1,3,4,5: Standing alternating single-leg-stance radiographs are not used for diagnosis or evaluation of these disorders.
Question 46High Yield
A minimally invasive plate osteosynthesis is seen in Figure 15. The resultant fracture healing can best be attributed to a fixation construct that was

Explanation
**
Locked plating constructs with long-working lengths provide flexible but stable constructs that promote (not inhibit) endochondral ossification. Because of the longer working length they are not stiff, and these fractures do not heal with intramembranous ossification which occurs in bones like the calvarium. Direct osteonal healing is usually seen with constructs
where absolute stability is achieved through interfragmentary compression, unlike in this case.
Locked plating constructs with long-working lengths provide flexible but stable constructs that promote (not inhibit) endochondral ossification. Because of the longer working length they are not stiff, and these fractures do not heal with intramembranous ossification which occurs in bones like the calvarium. Direct osteonal healing is usually seen with constructs
where absolute stability is achieved through interfragmentary compression, unlike in this case.
Question 47High Yield
Recommendations for sports activity should include
Explanation
- avoidance of contact or collision sports.
Question 48High Yield
A 21-year-old female cross-country runner is brought to the medical tent after completing her run. The race took place during an unseasonably warm day in August. The patient is disoriented upon her arrival to the tent and cannot state the exact date. What is the next most appropriate course of action?
37
37
Explanation
The patient is suffering from heat stroke due to the neurologic changes noted by confusion (can not state the date). This is a medical emergency and should be treated with immediate cold-water ice bath immersion and temperature monitoring with a rectal thermometer. Administration of IV fluids is controversial and is not first-line treatment for heat stroke. Transport to a hospital should be delayed until immediate cooling has been achieved and rectal temperature begins to decrease.
Question 49High Yield
A 21-year-old woman is struck by a car and sustains a Gustillo IIIB fracture of the tibia. The wound was debrided and immobilized with an external fixator. Radiographs are shown in Figure A. The soft tissue defect was covered with a free flap. Her recovery was complicated by wound infection with Klebsiella pneumoniae and Escherichia coli. One month after her injury, she underwent intramedullary nailing and placement of an antibiotic spacer measuring 15cm in length. Radiographs are shown in Figure B. At the next stage of surgery 6 weeks later, the surgeon should plan to do all of the following:


Explanation
The second stage of the Masquelet technique requires removal of the cement bolus, incision into the induced membranes and bone grafting. The existing hardware is preserved where possible as the fracture is still not stable. Bone graft is inserted INTO the membranous cavity, AROUND the nail.
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include: (1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur); (2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest), and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Answer 1: Excising the spacer alone will leave a cavity around the nail. Small amounts of bone form on the inside of the membrane, but without bone
grafting, bone will not bridge the gap. Bone graft should be inserted into the cavity at the same sitting as cement removal.
Answers 2 and 3: The membrane prevents bone graft resorption and contributes growth factors. Debriding the membrane will negate these effects. Exchange nailing will result in a period of instability and may compromise the membrane.
Answer 5: The nail cannot be removed as yet because there is no fracture site stability.
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include: (1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur); (2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest), and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Answer 1: Excising the spacer alone will leave a cavity around the nail. Small amounts of bone form on the inside of the membrane, but without bone
grafting, bone will not bridge the gap. Bone graft should be inserted into the cavity at the same sitting as cement removal.
Answers 2 and 3: The membrane prevents bone graft resorption and contributes growth factors. Debriding the membrane will negate these effects. Exchange nailing will result in a period of instability and may compromise the membrane.
Answer 5: The nail cannot be removed as yet because there is no fracture site stability.
Question 50High Yield
The radiographs (Figures 1 and

Explanation
■
The radiographs are of a child with multiple hereditary exostosis. This is a condition characterized by multiple osteochondromata. It is inherited as an autosomal dominant trait but can also arise from a new mutation. The abnormal genes are EXT1 and EXT2. COL1A1 and COL1A2 genes are associated with osteogenesis imperfecta and the NF1 gene is found in neurofibromatosis. Abnormalities in the FGFR-3 gene are seen in achondroplasia.
■
The radiographs are of a child with multiple hereditary exostosis. This is a condition characterized by multiple osteochondromata. It is inherited as an autosomal dominant trait but can also arise from a new mutation. The abnormal genes are EXT1 and EXT2. COL1A1 and COL1A2 genes are associated with osteogenesis imperfecta and the NF1 gene is found in neurofibromatosis. Abnormalities in the FGFR-3 gene are seen in achondroplasia.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon