Orthopedics Hyperguide Review | Dr Hutaif General Ortho -...
14 Apr 2026
56 min read
81 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedics Hyperguide Review | Dr Hutaif Gen...
00:00
Start Quiz
Question 1High Yield
A 16-year-old boy who is a competitive basketball player (Figure 43)

Explanation
- Meniscal repair
Question 2High Yield
If a closed reduction is attempted, which structure most likely will prevent a reduction?
Explanation
- Tibialis posterior tendon
Question 3High Yield
A 13-year-old girl with adolescent idiopathic scoliosis is otherwise healthy with a normal neurologic examination and she began her menstrual cycle 3 months ago. Standing radiographs show a high left thoracic curve from T1-T6 that measures 29 degrees, a right thoracic curve from T7-L1 that measures 65 degrees, and a left lumbar curve from L1-L5 that measures 31 degrees, correcting to 12, 37, and 10 degrees, respectively, on bending films. Her Risser sign is 1. What is the most appropriate management?
Explanation
The patient has typical adolescent idiopathic scoliosis with a right thoracic curve. This represents a Lenke-IB curve pattern; therefore, only treatment of the thoracic curve is required. The proximal thoracic and thoracolumbar curves are very flexible. The patient is Risser 1 and has just started her menstrual cycles; therefore, she is at significant risk for further curve progression. Bracing is not appropriate for a curve of this magnitude and will not halt the progression of this curve, nor will vertebral body stapling stop this curve. Vertebral body stapling is sometimes useful in small thoracic curves of less than 35 degrees and skeletally immature patients. Anterior and
14 • American Academy of Orthopaedic Surgeons
posterior spinal fusion is not required because the patient has no other risk factors, such as neurofibromatosis nor is she at risk for crankshaft. Anterior fusion is an option, but it is not listed.
REFERENCES: Lenke LG, Betz RR, Harmes J, et al: Adolescent idiopathic scoliosis: Anew classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001;83:1169-1181.
Lenke LG, Betz RR, Haher TR, et al: Multisurgeon assessment of surgical decision making in adolescent idiopathic scoliosis: Curve classification, operative approach, and fusion levels. Spine 2001;26:2347- 2353.
14 • American Academy of Orthopaedic Surgeons
posterior spinal fusion is not required because the patient has no other risk factors, such as neurofibromatosis nor is she at risk for crankshaft. Anterior fusion is an option, but it is not listed.
REFERENCES: Lenke LG, Betz RR, Harmes J, et al: Adolescent idiopathic scoliosis: Anew classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001;83:1169-1181.
Lenke LG, Betz RR, Haher TR, et al: Multisurgeon assessment of surgical decision making in adolescent idiopathic scoliosis: Curve classification, operative approach, and fusion levels. Spine 2001;26:2347- 2353.
Question 4High Yield
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years
ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 5High Yield
A 14-year-old girl is examined because of a pain in her left flank. The radiographs of the lumbar spine show loss of the pedicle with expansion of the lateral wall of the third lumbar vertebral body. Magnetic resonance imaging shows multiple fluid levels in the vertebral body with no additional areas of involvement. She is neurologically normal. The least invasive, effective treatment is which?
Explanation
This patient has an aneurysmal bone cyst of the vertebra. Selective arterial embolization is a minimally invasive treatment that often succeeds in arresting the lesions. Many times it is the only treatment needed. Selective arterial embolization can also be used as part of a strategy to be followed by curettage and reconstruction to decrease operative bleeding.
This lesion will continue to expand and might cause neurologic compromise or mechanical instability. Radiation therapy poses risks of later malignant degeneration. There are other ways of treating this lesion. Radical en bloc resection may unnecessarily injure neurologic structures.
While curettage is often necessary, there is no reason to introduce the risk of radiation therapy.
This lesion will continue to expand and might cause neurologic compromise or mechanical instability. Radiation therapy poses risks of later malignant degeneration. There are other ways of treating this lesion. Radical en bloc resection may unnecessarily injure neurologic structures.
While curettage is often necessary, there is no reason to introduce the risk of radiation therapy.
Question 6High Yield
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
Explanation
The patient has an axillary nerve injury, which is relatively uncommon after surgery for instability. This type of injury generally is the result of a stretch injury rather than transection or a hematoma. Therefore, observation is indicated in the early postoperative period. After approximately 6 weeks, electromyography can be used to confirm and document the point of injury. Interscalene blocks can cause prolonged nerve injury but usually are not limited to the axillary nerve.
REFERENCE: Ho E, Cofield RH, Balm MR, et al: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
REFERENCE: Ho E, Cofield RH, Balm MR, et al: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Question 7High Yield
The greatest amount of step-off that is well-tolerated in a Bennettâs fracture is:
Explanation
Studies by Livesley, Kjaer-Petersen, and others have shown that patients with fractures with more than a 1-mm step-off after reduction were more likely to develop arthritis at the thumb carpometacarpal joint. Although some studies have not shown functional outcome correlating with the presence of arthritis, Oosterbos and De Boer found that all their patients with fair and poor overall results had nonanatomic reductions. Although a cadaveric study by C ullen has shown that a 2-mm step-off may be acceptable, this contrasts with the clinical evidence currently available.
Question 8High Yield
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?

Explanation
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.
Figure 56
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.
Figure 56
Question 9High Yield
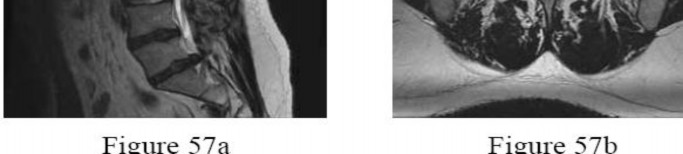
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management?
---
---

Explanation
The patient has an L5-S1 disk herniation, which has a favorable prognosis without surgical intervention. Most acute lumbar disk herniations resolve with nonsurgical management. The most appropriate course of initial treatment should be analgesics and activity modification, followed by rehabilitation as the symptoms allow. Although the MRI scan indicates a large disk herniation, he has no symptoms or signs that
would warrant urgent surgical decompression. Planned elective discectomy should be considered only if nonsurgical management fails to provide relief. Epidural injections could be considered if the initial course of treatment fails to give the patient significant relief. Posterior laminectomy and fusion is not indicated without the presence of instability.
would warrant urgent surgical decompression. Planned elective discectomy should be considered only if nonsurgical management fails to provide relief. Epidural injections could be considered if the initial course of treatment fails to give the patient significant relief. Posterior laminectomy and fusion is not indicated without the presence of instability.
Question 10High Yield
With respect to the structure identified by the arrow in Figure 22b, the meniscofemoral 25
ligaments are
ligaments are
Explanation
The stress radiographs demonstrate posterior instability of the right knee in flexion. The MR images demonstrate injury to both the anterior and posterior cruciate ligament (PCL), with the stump identified with the arrow on the MR image (Figure 22b). The PCL has 2 functional bands. The anterolateral bundle originates from the roof of the intercondylar notch. It runs in a posterolateral direction onto the tibial crest between the posterior attachment of the medial and lateral menisci. During a double-bundled posterior ligament reconstruction, the
anterolateral bundle is tensioned with the knee in a position of mid flexion. The posteromedial bundle has a variable pattern of tension both in extension and in high flexion. Tensioning of the posteromedial bundle in extension may contribute to resistance against knee hyperextension.
The meniscofemoral ligaments are variably present. Although 93% of knees have been reported to have at least 1 meniscofemoral ligament present, both ligaments are simultaneously present in approximately 50% of knees. The ligament of Humphrey (anterior meniscofemoral ligament) and ligament of Wrisberg (posterior meniscofemoral ligament) are delineated by their anatomic relationship to the posterior cruciate.
RECOMMENDED READINGS
1. [Amis AA, Bull AM, Gupte CM, Hijazi I, Race A, Robinson JR. Biomechanics of the PCL and related structures: posterolateral, posteromedial and meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2003 Sep;11(5):271-81. Epub 2003 Sep 5. Review. PubMed PMID: 12961064.](http://www.ncbi.nlm.nih.gov/pubmed/12961064)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12961064)
2. Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):257-63. Epub 2005 Oct 14. Review. PubMed PMID: 16228178.
View Abstract at PubMed . 26
anterolateral bundle is tensioned with the knee in a position of mid flexion. The posteromedial bundle has a variable pattern of tension both in extension and in high flexion. Tensioning of the posteromedial bundle in extension may contribute to resistance against knee hyperextension.
The meniscofemoral ligaments are variably present. Although 93% of knees have been reported to have at least 1 meniscofemoral ligament present, both ligaments are simultaneously present in approximately 50% of knees. The ligament of Humphrey (anterior meniscofemoral ligament) and ligament of Wrisberg (posterior meniscofemoral ligament) are delineated by their anatomic relationship to the posterior cruciate.
RECOMMENDED READINGS
1. [Amis AA, Bull AM, Gupte CM, Hijazi I, Race A, Robinson JR. Biomechanics of the PCL and related structures: posterolateral, posteromedial and meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2003 Sep;11(5):271-81. Epub 2003 Sep 5. Review. PubMed PMID: 12961064.](http://www.ncbi.nlm.nih.gov/pubmed/12961064)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12961064)
2. Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):257-63. Epub 2005 Oct 14. Review. PubMed PMID: 16228178.
View Abstract at PubMed . 26
Question 11High Yield
A 28-year-old male sustains the injury seen in Figure A. After discussing the risks and benefits of surgery, he elects to pursue nonoperative treatment. Of the following possible complications from nonoperative treatment, which is the most likely?

Explanation
In a patient with a displaced and shortened middle third clavicle fracture, nonunion would be expected to occur more often than any of the other complications listed.
The risk of nonunion following mid-shaft clavicle fractures is increased with
advanced age, female gender, displacement, and comminution ("Z-deformity"). Nonoperative management of mid-shaft clavicle fractures has also been associated with decreased shoulder strength and endurance.
Furthermore, range of motion and shoulder strength have not been shown to be sufficiently different between operative and nonoperative management.
Hoogervorst et al. reviewed the treatment of mid-shaft clavicle fractures. They cite that the rate of nonunion for fractures treated nonoperatively is about 15%. The authors note that those with >2cm of shortening and displacement
>100% of the shaft width are at a greater risk for nonunion and that nearly 66% of those who go on to nonunion eventually undergo surgical repair.
Robinson et al. performed a prospective observational cohort study to evaluate the prevalence of and risk factors for nonunion of clavicle fractures treated nonoperatively. They found that the risk of nonunion was significantly increased by advancing age, female gender, displacement of the fracture, and the presence of comminution.
Figure A shows a radiograph demonstrating a middle third clavicle shaft fracture with >100% displacement and >2cm shortening.
Incorrect Answers:
Answer 1: The rate of skin necrosis following nonoperative treatment has not been shown to be higher than nonunion.
Answer 3: The rate of complex regional pain syndrome (CRPS) was shown to be around 2% in nonoperatively treated patients.
Answer 4 ad 5: Sternoclavicular arthritis and acromioclavicular arthritis or abnormalities have been shown to be somewhere between 4-6%
The risk of nonunion following mid-shaft clavicle fractures is increased with
advanced age, female gender, displacement, and comminution ("Z-deformity"). Nonoperative management of mid-shaft clavicle fractures has also been associated with decreased shoulder strength and endurance.
Furthermore, range of motion and shoulder strength have not been shown to be sufficiently different between operative and nonoperative management.
Hoogervorst et al. reviewed the treatment of mid-shaft clavicle fractures. They cite that the rate of nonunion for fractures treated nonoperatively is about 15%. The authors note that those with >2cm of shortening and displacement
>100% of the shaft width are at a greater risk for nonunion and that nearly 66% of those who go on to nonunion eventually undergo surgical repair.
Robinson et al. performed a prospective observational cohort study to evaluate the prevalence of and risk factors for nonunion of clavicle fractures treated nonoperatively. They found that the risk of nonunion was significantly increased by advancing age, female gender, displacement of the fracture, and the presence of comminution.
Figure A shows a radiograph demonstrating a middle third clavicle shaft fracture with >100% displacement and >2cm shortening.
Incorrect Answers:
Answer 1: The rate of skin necrosis following nonoperative treatment has not been shown to be higher than nonunion.
Answer 3: The rate of complex regional pain syndrome (CRPS) was shown to be around 2% in nonoperatively treated patients.
Answer 4 ad 5: Sternoclavicular arthritis and acromioclavicular arthritis or abnormalities have been shown to be somewhere between 4-6%
Question 12High Yield
A 12-year-old boy sustains a Salter type II fracture of the proximal humerus during a fall. The fracture has an apex angulation of 40° anteriorly and laterally. The neurovascular examination is normal. The recommended treatment is:
Explanation
Recommended treatment involves no formal reduction attempt, rather placement of the arm in a sling. This simple treatment is adequate for all patients with at least 2 years of growth remaining. This is due to the tendency to self-align, the remodeling potential, and the ability to tolerate some deformity in the region with no functional consequence.
The abduction splint is cumbersome. It is not necessary because simpler means are effective due to the young age and remodeling potential.
C losed reduction and pin fixation are not needed because adequate remodeling is expected. Any residual deformity is well tolerated in this region. The pins can sometimes cause significant soft tissue irritation in the bulky area of the shoulder. Plate fixation is not feasible because of the open physis. It is also not necessary because simpler means are available. Skeletal traction is not needed because the humerus will align itself better with time in a dependent position.
The abduction splint is cumbersome. It is not necessary because simpler means are effective due to the young age and remodeling potential.
C losed reduction and pin fixation are not needed because adequate remodeling is expected. Any residual deformity is well tolerated in this region. The pins can sometimes cause significant soft tissue irritation in the bulky area of the shoulder. Plate fixation is not feasible because of the open physis. It is also not necessary because simpler means are available. Skeletal traction is not needed because the humerus will align itself better with time in a dependent position.
Question 13High Yield
A 5-year-old boy had a 1-week history of left hip pain and a limp that resolved 5 weeks prior to his office visit. Examination demonstrates a pain-free and symmetric range of motion. A radiograph is seen in Figure 42. What is the next step in management?
Explanation
DISCUSSION: Whereas bilateral Perthes of the hips occurs in 11% of cases, in patients with symmetric changes/stages, other diagnoses must be considered such as Meyers dysplasia. Multiple epiphyseal dysplasia is most _A_ r _L_ e _-_ a _M_ d _a_ il _d_ y _en_ d _a_ ia _C_ g _o_ n _p_ o _y_ sed by evaluation of other radiographs, in particular of the knee and, if confirmatory, of the
**2010 Pediatric Orthopaedic Examination Answer Book • 37**
spine to assess for spondyloepiphyseal dysplasia.
REFERENCES: Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 806-810.
Hesse B, Kohler G: Does it always have to be Perthes’ disease? What is epiphyseal dysplasia? Clin Orthop Relat
Res 2003;414:219-227.
**2010 Pediatric Orthopaedic Examination Answer Book • 37**
spine to assess for spondyloepiphyseal dysplasia.
REFERENCES: Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 806-810.
Hesse B, Kohler G: Does it always have to be Perthes’ disease? What is epiphyseal dysplasia? Clin Orthop Relat
Res 2003;414:219-227.
Question 14High Yield
The origin and insertion of the obturator internus are the ischiopubic ramus/obturator membrane and the greater trochanter, respectively.
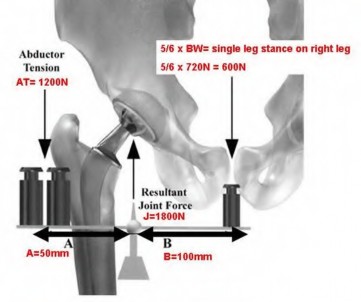
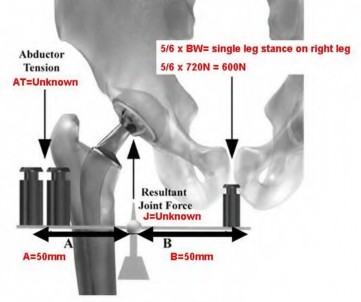
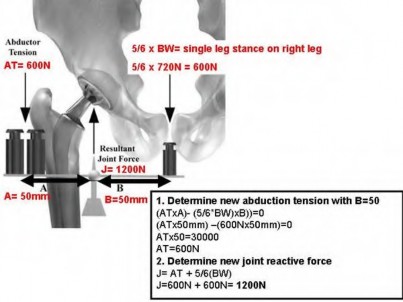
Figure A represents a free body diagram of the hip of a patient standing on the right leg. The forces and distances are labeled on the diagram and the resulting hip joint force (J) = 1800N. What is the resultant value for J when the acetabular component is medialized given the new distances shown in Figure B?
Figure A represents a free body diagram of the hip of a patient standing on the right leg. The forces and distances are labeled on the diagram and the resulting hip joint force (J) = 1800N. What is the resultant value for J when the acetabular component is medialized given the new distances shown in Figure B?


Explanation
Intra-articular hyaluronic acid is no longer recommended as an effective method of treatment for patients with symptomatic knee arthritis based on the revised AAOS clinical guidelines from 2013. The previous review from
2009 guidelines was reported as inconclusive.
Nonoperative treatment modalities whose use is supported by the literature include: activity modifications, weight loss, quadriceps strengthening, patellar taping, NSAIDs, tylenol (Now 3000mg/24hr is recommended from 4000mg/24hr), and intra-articular steroids. Treatment options that are NOT supported by the literature (or are considered inconclusive) include: intra-articular hyaluronic acid injections, lateral heel wedges for medial knee OA, glucosamine and chondroitin, needle lavage, and arthroscopy in patients with primary OA.
Illustration A shows a chart showing the rates of accuracy of intra-articular knee injections.
Incorrect Answers:
: Weight loss is considered a moderate recommendation according to the AAOS clinical guidelines.
Answer 2: Activity modification is strongly recommended according to the AAOS clinical guidelines.
Answer 3: Quadriceps strengthening is strongly recommended according to the AAOS clinical guidelines.
Answer 5: The use of intra-articular corticosteroid injections cannot be recommended for or against according to the latest AAOS clinical guidelines.
All of the following are intraoperative techniques to treat a flexion contracture in total knee arthroplasty EXCEPT:
1) Resect osteophytes
2) Release posterior capsule
3) Resect more distal femur
4) Downsize the femoral component
5) Tenotomize the hamstrings
Of the options listed, downsizing the femoral component would NOT be an intraoperative technique to treat a flexion contracture in total knee arthroplasty.
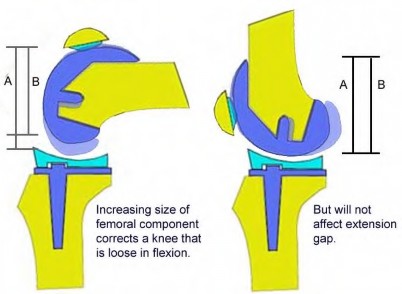
Flexion contractures (an extension gap issue) can be addressed by resecting osteophytes, resecting the posterior capsule/gastrocnemius, resecting additional distal femur, and tenotomizing the hamstrings. Downsizing the femoral component would only change the flexion gap and have no impact on a flexion contracture (an extension gap issue.) Downsizing the femoral component means decreasing the size of the implant in the anterior-posterior dimension only. There is no change in the proximal-distal dimension, and thus changing the size of the femoral implant only affects the flexion gap, and not the extension gap or a flexion contracture.
Bellemans et al. propose an algorithm to treat preoperative flexion contractures greater than 5 degrees. The steps include:
Step 1: Mediolateral ligament balancing with meticulous osteophyte removal and over resection of distal femur by 2 mm.
Step 2: Add posterior capsular release.
Step 3: Add distal femoral resection up to 4 mm. Step 4: Add hamstring tenotomy.
For flexion contractures less than 15 degrees they report steps 1 and 2 were sufficient for 100% of the cases in their study. Steps 3 and 4 were only necessary for some contractures greater than 35 degrees.
Illustration A shows how changing the femoral component size only affects the flexion gap.
Incorrect Answers
Answers 1,2, 3, and 5 are all methods to treat a flexion contractures in total knee arthroplasty.
A 64-year-old healthy female patient underwent right total hip replacement (THR) through a posterior approach 6 months ago. She has now dislocated posteriorly 3 times, each followed by closed reduction under anesthesia in the operating room. A radiograph is provided in Figure A. Treatment should include:
1) Hip spica casting
2) Revision of the femoral component to a modular stem with retention of the acetabular component
3) Revision of the acetabular component
4) Hip abduction bracing
5) Revision to a constrained liner with retention of the acetabular and femoral prostheses
The optimal acetabular component alignment is 30-50 degrees of abduction and 15-20 degrees of anteversion. This patient has a vertical acetabular component that requires revision.
Reasons for recurrent THA instability include infection, non-compliance with precautions, component malposition, impingement and inadequate soft tissue tension. Strategies that do not address the underlying cause of recurrent dislocation will not definitively treat the instability. Non-operative measures cannot account for drastic component malposition.
Figure A shows an AP pelvis after right total hip arthroplasty. The acetabular component is vertically positioned. The femoral component is in slight varus but not enough to warrant revision on its own. The version of each component cannot be definitively determined on this single film. The acetabular component has a significant amount of version that could be ante- or retroversion.
Incorrect Answers:
2009 guidelines was reported as inconclusive.
Nonoperative treatment modalities whose use is supported by the literature include: activity modifications, weight loss, quadriceps strengthening, patellar taping, NSAIDs, tylenol (Now 3000mg/24hr is recommended from 4000mg/24hr), and intra-articular steroids. Treatment options that are NOT supported by the literature (or are considered inconclusive) include: intra-articular hyaluronic acid injections, lateral heel wedges for medial knee OA, glucosamine and chondroitin, needle lavage, and arthroscopy in patients with primary OA.
Illustration A shows a chart showing the rates of accuracy of intra-articular knee injections.
Incorrect Answers:
: Weight loss is considered a moderate recommendation according to the AAOS clinical guidelines.
Answer 2: Activity modification is strongly recommended according to the AAOS clinical guidelines.
Answer 3: Quadriceps strengthening is strongly recommended according to the AAOS clinical guidelines.
Answer 5: The use of intra-articular corticosteroid injections cannot be recommended for or against according to the latest AAOS clinical guidelines.
All of the following are intraoperative techniques to treat a flexion contracture in total knee arthroplasty EXCEPT:
1) Resect osteophytes
2) Release posterior capsule
3) Resect more distal femur
4) Downsize the femoral component
5) Tenotomize the hamstrings
Of the options listed, downsizing the femoral component would NOT be an intraoperative technique to treat a flexion contracture in total knee arthroplasty.
Flexion contractures (an extension gap issue) can be addressed by resecting osteophytes, resecting the posterior capsule/gastrocnemius, resecting additional distal femur, and tenotomizing the hamstrings. Downsizing the femoral component would only change the flexion gap and have no impact on a flexion contracture (an extension gap issue.) Downsizing the femoral component means decreasing the size of the implant in the anterior-posterior dimension only. There is no change in the proximal-distal dimension, and thus changing the size of the femoral implant only affects the flexion gap, and not the extension gap or a flexion contracture.
Bellemans et al. propose an algorithm to treat preoperative flexion contractures greater than 5 degrees. The steps include:
Step 1: Mediolateral ligament balancing with meticulous osteophyte removal and over resection of distal femur by 2 mm.
Step 2: Add posterior capsular release.
Step 3: Add distal femoral resection up to 4 mm. Step 4: Add hamstring tenotomy.
For flexion contractures less than 15 degrees they report steps 1 and 2 were sufficient for 100% of the cases in their study. Steps 3 and 4 were only necessary for some contractures greater than 35 degrees.
Illustration A shows how changing the femoral component size only affects the flexion gap.
Incorrect Answers
Answers 1,2, 3, and 5 are all methods to treat a flexion contractures in total knee arthroplasty.
A 64-year-old healthy female patient underwent right total hip replacement (THR) through a posterior approach 6 months ago. She has now dislocated posteriorly 3 times, each followed by closed reduction under anesthesia in the operating room. A radiograph is provided in Figure A. Treatment should include:
1) Hip spica casting
2) Revision of the femoral component to a modular stem with retention of the acetabular component
3) Revision of the acetabular component
4) Hip abduction bracing
5) Revision to a constrained liner with retention of the acetabular and femoral prostheses
The optimal acetabular component alignment is 30-50 degrees of abduction and 15-20 degrees of anteversion. This patient has a vertical acetabular component that requires revision.
Reasons for recurrent THA instability include infection, non-compliance with precautions, component malposition, impingement and inadequate soft tissue tension. Strategies that do not address the underlying cause of recurrent dislocation will not definitively treat the instability. Non-operative measures cannot account for drastic component malposition.
Figure A shows an AP pelvis after right total hip arthroplasty. The acetabular component is vertically positioned. The femoral component is in slight varus but not enough to warrant revision on its own. The version of each component cannot be definitively determined on this single film. The acetabular component has a significant amount of version that could be ante- or retroversion.
Incorrect Answers:
Question 15High Yield
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
In a cadaver ligament sectioning study, the posterior capsular ligament was considered the most important structure for anterior-posterior stability of the sternoclavicular joint. The anterior capsular ligament also helps prevent anterior displacement but not to the same degree as the posterior ligament. The interclavicular ligament provides little support for anteroposterior translation.
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
Question 16High Yield
A high collagen concentration and a low proteoglycan concentration is found in which of the following zones of articular cartilage:
Explanation
The superficial zone has a number of important characteristics: Thinnest articular cartilage layer
Two layers:
Most superficial – fine collagen fibrils (lamina splendens)
Deep layer – flattened fibroblast-like chondrocytes (parallel to joint surface) Forms a cartilage skin
Important chemical properties:
High collagen and low proteoglycan concentration
Fibronectin and water concentrations are highest in this zone
Great tensile stiffness and strength
Seals off the cartilage from the immune system
Two layers:
Most superficial – fine collagen fibrils (lamina splendens)
Deep layer – flattened fibroblast-like chondrocytes (parallel to joint surface) Forms a cartilage skin
Important chemical properties:
High collagen and low proteoglycan concentration
Fibronectin and water concentrations are highest in this zone
Great tensile stiffness and strength
Seals off the cartilage from the immune system
Question 17High Yield
A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?
Explanation
DISCUSSION
Proper soft-tissue tension is critical to prevent instability of a reverse total shoulder implanted with the deltopectoral approach; dislocation of the prosthesis is exceedingly rare if the superior approach is employed. The arm position implicated in reverse total shoulder instability is extension, adduction, and internal rotation,
such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
DISCUSSION
Proper soft-tissue tension is critical to prevent instability of a reverse total shoulder implanted with the deltopectoral approach; dislocation of the prosthesis is exceedingly rare if the superior approach is employed. The arm position implicated in reverse total shoulder instability is extension, adduction, and internal rotation,
such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
Question 18High Yield
The deltoid inserts on this surface of the clavicle:
Explanation
The origin of the deltoid on the clavicle is J-shaped and extends from the midline on the superior aspect of the clavicle around the front of the clavicle to the inferior portion of the anterior aspect of the clavicle. Full-thickness fascial flaps must be obtained when the deltoid is released from the clavicle.
Question 19High Yield
A 34-old-male was involved in a high speed MVC. He sustained an injury to his right leg as seen in Figures A and B. He was treated initially with external fixation for 11 days before his soft-tissues would permit definitive open internal fixation. After removing the external fixator and plating the fibula, what would be next step in the operative plan for reduction and fixation of this injury?



Explanation
Figures A and B show an AO/OTA Type C Pilon fracture with metaphyseal comminution and intra-articular involvement of the tibia. There is an associated fibula fracture. The next step in the operative treatment of this injury, after removal of external fixation, would be anatomical reduction and stabilization of the articular surface.
The first step in the treatment of pilon fractures involves anatomical reduction and stabilization of the articular surface. This can be accomplished with pointed reduction clamps, K-wires, lag screws, or any combination of these. Plate fixation and reduction of the metaphyseal comminution should occur after the joint surface has been re-established. Simple fibular fractures can be plated before fixation of the tibia. Comminuted fibular fractures are usually better reconstructed after the tibia has been repaired, so that the tibia and talus can be used as a guide for positioning of the lateral malleolus.
Sirkin et al. reviewed the protocol for treatment of complex pilon fractures. They showed that the severity of soft-tissue injury will dictate the timing of fixation and choice of implant. To avoid wound healing problems, it is generally accepted that two or more stages of repair should be used.
Figure A, B and C show a high energy fracture to the distal tibia. Incorrect Answers:
Answer 1, 3: Plate preparation and insertion should be considered after
reduction and stabilization of the articular fracture fragments. The use of medial and anterolateral locking plates are appropriate for fixation of this fracture. Longer implants improve load distribution and stability.
Answer 4: The metaphyseal segment of this fracture does not require anatomical reduction. Basic fixation principles for metaphyseal comminution would include, re-establishing tibia length, rotation and angulation at the fracture site. Reduction of the metaphysis should occur after reduction of the articular surface.
Answer 5: The final step in metaphyseal reduction is usually achieved by
securing the proximal end of the plate to the tibial shaft. A kick-stand screw can be placed in the most proximal hole to increase the working length of the plate. This can be placed percutaneously if desired.
The first step in the treatment of pilon fractures involves anatomical reduction and stabilization of the articular surface. This can be accomplished with pointed reduction clamps, K-wires, lag screws, or any combination of these. Plate fixation and reduction of the metaphyseal comminution should occur after the joint surface has been re-established. Simple fibular fractures can be plated before fixation of the tibia. Comminuted fibular fractures are usually better reconstructed after the tibia has been repaired, so that the tibia and talus can be used as a guide for positioning of the lateral malleolus.
Sirkin et al. reviewed the protocol for treatment of complex pilon fractures. They showed that the severity of soft-tissue injury will dictate the timing of fixation and choice of implant. To avoid wound healing problems, it is generally accepted that two or more stages of repair should be used.
Figure A, B and C show a high energy fracture to the distal tibia. Incorrect Answers:
Answer 1, 3: Plate preparation and insertion should be considered after
reduction and stabilization of the articular fracture fragments. The use of medial and anterolateral locking plates are appropriate for fixation of this fracture. Longer implants improve load distribution and stability.
Answer 4: The metaphyseal segment of this fracture does not require anatomical reduction. Basic fixation principles for metaphyseal comminution would include, re-establishing tibia length, rotation and angulation at the fracture site. Reduction of the metaphysis should occur after reduction of the articular surface.
Answer 5: The final step in metaphyseal reduction is usually achieved by
securing the proximal end of the plate to the tibial shaft. A kick-stand screw can be placed in the most proximal hole to increase the working length of the plate. This can be placed percutaneously if desired.
Question 20High Yield
1249) A 29-year-old male sustains the isolated lower extremity injury shown in Figure A. During open reduction, what structure must be kept intact in order to protect the remaining blood supply to the talar body?

Explanation
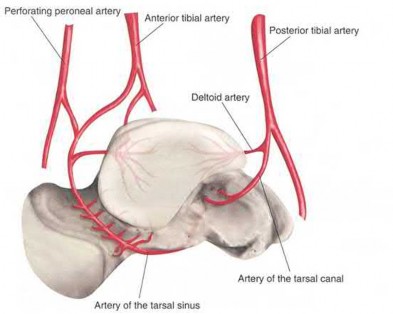
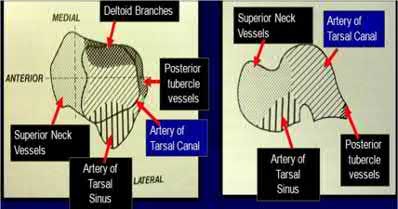
Figure A represents a type 3 Hawkins talar neck fracture. A type 3 injury is defined as a displaced fracture of the talar neck with dislocation of body of talus from both the subtalar joint and the tibiotalar joint. In these injuries, the talar body fragment typically rotates around intact deltoid ligament fibers to lie in soft tissues with the fracture surface pointing laterally and cephalad. Often, the deltoid branch of the posterior tibial artery, which lies between the leaves of the deltoid ligament and supplies up to 1/2 of the medial talar body, is the only remaining blood supply. Therefore, the deltoid ligament must be preserved to lower the risk of avascular necrosis. When performing a medial malleolar osteotomy, the deltoid ligament must remain in continuity with the malleolus to prevent disruption of the blood supply.
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
Question 21High Yield
Figure 21 shows the radiograph of an 18-year-old man who was brought to the emergency department with shoulder pain following a rollover accident on an all-terrain vehicle. Examination reveals a fracture with massive swelling; however, the skin is intact and not tented over the fracture. Based on these findings, initial management should consist of
Explanation
The radiographic and clinical findings suggest a scapulothoracic dissociation with a widely displaced clavicular fracture and a laterally displaced scapula. These injuries have a high association with neurovascular injuries to the brachial plexus and subclavian artery. Emergent vascular evaluation with arteriography and possible vascular repair are indicated. This repair can be combined with open reduction and internal fixation of the clavicle to improve stability. Delay in treatment of these vascular injuries can be devastating.
REFERENCES: Iannotti JP, Williams GR (eds): Disorders of the Shoulder. Philadelphia, PA, Lippincott, 1999, pp 632-635.
Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432.
REFERENCES: Iannotti JP, Williams GR (eds): Disorders of the Shoulder. Philadelphia, PA, Lippincott, 1999, pp 632-635.
Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432.
Question 22High Yield
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees
Explanation
DISCUSSION: The history, physical examination, and laboratory studies suggest a septic hip. Recent studies indicate that a child with elevated ESR, a WBC count of greater than 12,000/mm3, a temperature of greater than 38.5 degrees, and unwillingness to walk is very likely to have septic arthritis of the hip versus toxic synovitis. The best way to confirm the diagnosis is by hip aspiration. No medications should be started until a diagnosis is made. Toxic synovitis is common, but significantly less likely if three of the above criteria are present. This condition usually responds well to ibuprofen, but requires close observation. Septic hips are considered urgent conditions and therefore a repeat evaluation in 2 weeks is inappropriate.
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
DISCUSSION: The history, physical examination, and laboratory studies suggest a septic hip. Recent studies indicate that a child with elevated ESR, a WBC count of greater than 12,000/mm3, a temperature of greater than 38.5 degrees, and unwillingness to walk is very likely to have septic arthritis of the hip versus toxic synovitis. The best way to confirm the diagnosis is by hip aspiration. No medications should be started until a diagnosis is made. Toxic synovitis is common, but significantly less likely if three of the above criteria are present. This condition usually responds well to ibuprofen, but requires close observation. Septic hips are considered urgent conditions and therefore a repeat evaluation in 2 weeks is inappropriate.
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 23High Yield
Which of the following treatment methods is used for the majority of patients with a stress fracture:
Explanation
The majority of stress fractures are treated with rest and protected weight-bearing. When the patient rests, strain on the affected bone is reduced and formation exceeds resorption, leading to bone healing.
Electrical stimulation and ultrasound have not been shown to increase the rate of healing. For most stress fractures, surgery is not necessary.
C orrect Answer: Rest and protected weight-bearing
Electrical stimulation and ultrasound have not been shown to increase the rate of healing. For most stress fractures, surgery is not necessary.
C orrect Answer: Rest and protected weight-bearing
Question 24High Yield
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient?


Explanation
DISCUSSION: The anterior bundle of the ulnar collateral ligament of the elbow is the primary constraint to valgus force of the elbow. In pitchers and in overhead athletes, injury to this portion of the ligament results in valgus instability. Reconstruction of the anterior band of the ulnar collateral ligament is necessary in many elite athletic throwers to allow them to return to this competitive activity.
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Cain EL, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Rettig AC, Sherrill C, Snead DS, et al: Nonoperative treatment of ulnar collateral ligament injuries in
throwing athletes. Am J Sports Med 2001 ;29:15-17.
/
Figure 55a Question 55
A 22-year-old male basketball player has had knee pain for the past 3 months. He denies any history of trauma. He has symptoms of catching but no locking. He has rested for 2 weeks but symptoms returned when he resumed sporting activities. Tr and T2-weighted MRI scans are shown in Figures 55a and 55b. What is the most likely diagnosis?
1. #### Locked lateral meniscus tear
2. #### Anterior cruciate ligament tear
3. #### Ganglion cyst of the anterior cruciate ligament
4. #### Synovial osteochondromatosis
5. #### Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Cain EL, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Rettig AC, Sherrill C, Snead DS, et al: Nonoperative treatment of ulnar collateral ligament injuries in
throwing athletes. Am J Sports Med 2001 ;29:15-17.
/
Figure 55a Question 55
A 22-year-old male basketball player has had knee pain for the past 3 months. He denies any history of trauma. He has symptoms of catching but no locking. He has rested for 2 weeks but symptoms returned when he resumed sporting activities. Tr and T2-weighted MRI scans are shown in Figures 55a and 55b. What is the most likely diagnosis?
1. #### Locked lateral meniscus tear
2. #### Anterior cruciate ligament tear
3. #### Ganglion cyst of the anterior cruciate ligament
4. #### Synovial osteochondromatosis
5. #### Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
Question 25High Yield
A 45-year-old man feels a pop in the anterior aspect of his elbow while lifting furniture. He denies any antecedent pain or injury. Which examination method is best for diagnosing a distal biceps rupture?
Explanation
No detailed explanation provided for this question.
Question 26High Yield
Figures below depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after
primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to
3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1%
neutrophils. No growth of organisms is seen on routine culture. What is the best next step?
primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to
3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1%
neutrophils. No growth of organisms is seen on routine culture. What is the best next step?

Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results
show no signs of infection, so a single-stage procedure is preferred.
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results
show no signs of infection, so a single-stage procedure is preferred.
Question 27High Yield
A 32-year-old professional skydiver lands awkwardly during a jump. He presents to the emergency room with bilateral knee injuries.
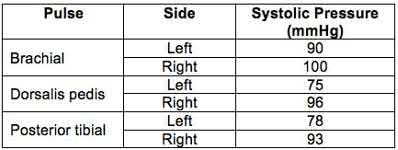
Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Explanation
The ankle-brachial index (ABI) of left and right limbs are 0.78 and 0.96 respectively. CT angiography (or conventional angiography) of the left lower extremity is indicated because of abnormal ABI <0.9. It is sufficient to observe the right lower extremity (ABI >0.9).
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI <0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Answer 1: If vascular exam is normal and ABI >0.9, neurovascular checks every 2-4 hours for 48 hours is appropriate. As ABI is abnormal on the left, CT angiogram is necessary.
Answer 2: Anticoagulation has not been shown to stop thrombus formation for non-flow limiting intimal flap tears.
Answer 3: CT angiography is indicated if ABI is abnormal post reduction. CT angiography for the right lower extremity is unnecessary as ABI >0.9.
Answer 5: Surgery is indicated if CT angiography (or conventional angiography) demonstrates intimal flap tears that are flow limiting (but not if the intimal flap is NOT flow limiting), if distal pulses are absent, or if distal ischemia, active hemorrhage, or expanding pulsatile hematoma are present.
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI <0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Answer 1: If vascular exam is normal and ABI >0.9, neurovascular checks every 2-4 hours for 48 hours is appropriate. As ABI is abnormal on the left, CT angiogram is necessary.
Answer 2: Anticoagulation has not been shown to stop thrombus formation for non-flow limiting intimal flap tears.
Answer 3: CT angiography is indicated if ABI is abnormal post reduction. CT angiography for the right lower extremity is unnecessary as ABI >0.9.
Answer 5: Surgery is indicated if CT angiography (or conventional angiography) demonstrates intimal flap tears that are flow limiting (but not if the intimal flap is NOT flow limiting), if distal pulses are absent, or if distal ischemia, active hemorrhage, or expanding pulsatile hematoma are present.
Question 28High Yield
A minimally invasive diskectomy technique poses potential for
Explanation
- increased dural tear risk.
Question 29High Yield
Which of the following commercially available cements has the lowest tensile strength value:
Explanation
Zimmer Dough has the lowest value of tensile strength; however, all of the above are FDA-approved cements and of sufficient quality
Question 30High Yield
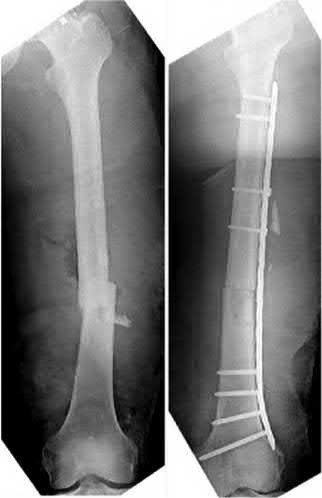
-A 45-year-old man sustained bilateral femur fractures in a motorcycle accident. On admission to the emergency department, the patient is unconscious with a heart rate of 120 bpm and a systolic blood pressure of 80 mm Hg. A chest radiograph reveals bilateral pulmonary contusions. After resuscitation with 2 L of crystalloid, the patient’s heart rate is 115 bpm, the systolic blood pressure is 90 mm Hg, and the patient’s delta base is -10 mmol/L. What is the most appropriate treatment for the femoral fractures at this point?
Explanation
No detailed explanation provided for this question.
Question 31High Yield
Recombinant human bone morphogenetic protein-2 (rhBMP-2) is US Food and Drug Administration (FDA) approved for which of the following indications?




Explanation
For long bones, rhBMP-2 is FDA approved for acute open diaphyseal fractures of the tibia treated with intramedullary (IM) nail fixation.
rhBMP-2 is approved for repair of posterolateral lumbar pseudarthrosis, anterior lumbar interbody fusions (ALIFs) with a lumbar fusion device, open tibia shaft fractures with intramedullary nail fixation. rhBMP-7 is approved under humanitarian device exemption as an alternative to autograft in long bone nonunions and as an alternative to autograft for posterolateral fusion.
Govender et al. compared 3 groups of patients: tibia fractures receiving IM nail (standard of care), IM nail with an implant containing 0.75mg/ml of rhBMP-2, and IM nail with an implant containing 1.5mg/ml of rhBMP-2. The implants were collagen sponges. Patients receiving IM nail with 1.5mg/ml of rhBMP-2 had reduced risk of delayed union, fewer interventions (bone-grafting and nail exchange), faster fracture healing, fewer hardware failures and infections.
They concluded that rhBMP-2 was superior to the standard of care.
Garrison et al. reviewed 11 trials. Four trials showed that BMP treated acute fractures required fewer subsequent procedures. Six trials showed that BMP was neither better nor worse than bone grafts for nonunion. One trial showed no difference between BMP and bone grafts for osteotomies.
Figure A shows a mid-diaphyseal femur fracture treated with an intramedullary nail. Figure B shows a mid-diaphyseal femur fracture treated with a plate.
Figure C shows a mid-diaphyseal femur fracture nonunion treated with a second supplementary anterior plate. Figure D shows a mid-diaphyseal tibia fracture treated with exchange nailing. Figure E shows a mid-diaphyseal tibia fracture treated with an intramedullary nail.
Incorrect Answers:
Answers 1 to 4: rhBMP2 is not approved for long bone fractures except for
acute open diaphyseal fractures of the tibia treated with intramedullary (IM) nailing.
rhBMP-2 is approved for repair of posterolateral lumbar pseudarthrosis, anterior lumbar interbody fusions (ALIFs) with a lumbar fusion device, open tibia shaft fractures with intramedullary nail fixation. rhBMP-7 is approved under humanitarian device exemption as an alternative to autograft in long bone nonunions and as an alternative to autograft for posterolateral fusion.
Govender et al. compared 3 groups of patients: tibia fractures receiving IM nail (standard of care), IM nail with an implant containing 0.75mg/ml of rhBMP-2, and IM nail with an implant containing 1.5mg/ml of rhBMP-2. The implants were collagen sponges. Patients receiving IM nail with 1.5mg/ml of rhBMP-2 had reduced risk of delayed union, fewer interventions (bone-grafting and nail exchange), faster fracture healing, fewer hardware failures and infections.
They concluded that rhBMP-2 was superior to the standard of care.
Garrison et al. reviewed 11 trials. Four trials showed that BMP treated acute fractures required fewer subsequent procedures. Six trials showed that BMP was neither better nor worse than bone grafts for nonunion. One trial showed no difference between BMP and bone grafts for osteotomies.
Figure A shows a mid-diaphyseal femur fracture treated with an intramedullary nail. Figure B shows a mid-diaphyseal femur fracture treated with a plate.
Figure C shows a mid-diaphyseal femur fracture nonunion treated with a second supplementary anterior plate. Figure D shows a mid-diaphyseal tibia fracture treated with exchange nailing. Figure E shows a mid-diaphyseal tibia fracture treated with an intramedullary nail.
Incorrect Answers:
Answers 1 to 4: rhBMP2 is not approved for long bone fractures except for
acute open diaphyseal fractures of the tibia treated with intramedullary (IM) nailing.
Question 32High Yield
If this lesion occurred in the spine, which features would most likely be present?
Explanation
The images and clinical history support a diagnosis of osteoid osteoma, which most commonly occurs in adolescence. Although these lesions can be seen in any bone, they are usually located in the femur and tibia. The significant inflammatory response to this tumor is secondary to high levels of prostaglandin production. Characteristic night pain is relieved with nonsteroidal anti-inflammatory drugs (NSAIDs) or by aspirin.
Radiographic images show thickened bone and a small central nidus. Thin-cut CT scan is the imaging of choice to visualize the nidus. A bone scan is associated with uptake but is not specific. Treatment options include expectant management with NSAIDs and observation under the premise that these lesions eventually burn out. Contemporary treatment involves RFA. Historically, these lesions were treated with en bloc resection; however, this technique has largely fallen out of favor because of the high efficacy and comparative low morbidity associated with RFA.
When an osteoid osteoma occurs in the spine, it is located in the posterior elements, and paraspinal pain and scoliosis often are present.
RECOMMENDED READINGS
14. [Volkmer D, Sichlau M, Rapp TB. The use of radiofrequency ablation in the treatment of musculoskeletal tumors. J Am Acad Orthop Surg. 2009 Dec;17(12):737-43. Review. PubMed PMID: 19948698. ](http://www.ncbi.nlm.nih.gov/pubmed/19948698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19948698)
15. [Donahue F, Ahmad A, Mnaymneh W, Pevsner NH. Osteoid osteoma. Computed tomography guided percutaneous excision. Clin Orthop Relat Res. 1999 Sep;(366):191-6. PubMed PMID: 10627735. ](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[View](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[ ](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10627735)
16. [Boscainos PJ, Cousins GR, Kulshreshtha R, Oliver TB, Papagelopoulos PJ. Osteoid osteoma. Orthopedics. 2013 Oct 1;36(10):792-800. doi: 10.3928/01477447-20130920-10. Review. PubMed PMID: 24093694. ](http://www.ncbi.nlm.nih.gov/pubmed/24093694)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24093694)
Radiographic images show thickened bone and a small central nidus. Thin-cut CT scan is the imaging of choice to visualize the nidus. A bone scan is associated with uptake but is not specific. Treatment options include expectant management with NSAIDs and observation under the premise that these lesions eventually burn out. Contemporary treatment involves RFA. Historically, these lesions were treated with en bloc resection; however, this technique has largely fallen out of favor because of the high efficacy and comparative low morbidity associated with RFA.
When an osteoid osteoma occurs in the spine, it is located in the posterior elements, and paraspinal pain and scoliosis often are present.
RECOMMENDED READINGS
14. [Volkmer D, Sichlau M, Rapp TB. The use of radiofrequency ablation in the treatment of musculoskeletal tumors. J Am Acad Orthop Surg. 2009 Dec;17(12):737-43. Review. PubMed PMID: 19948698. ](http://www.ncbi.nlm.nih.gov/pubmed/19948698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19948698)
15. [Donahue F, Ahmad A, Mnaymneh W, Pevsner NH. Osteoid osteoma. Computed tomography guided percutaneous excision. Clin Orthop Relat Res. 1999 Sep;(366):191-6. PubMed PMID: 10627735. ](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[View](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[ ](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10627735)
16. [Boscainos PJ, Cousins GR, Kulshreshtha R, Oliver TB, Papagelopoulos PJ. Osteoid osteoma. Orthopedics. 2013 Oct 1;36(10):792-800. doi: 10.3928/01477447-20130920-10. Review. PubMed PMID: 24093694. ](http://www.ncbi.nlm.nih.gov/pubmed/24093694)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24093694)
Question 33High Yield
A 5-year-old boy has had a limp for the past 4 weeks with intermittent pain at the foot. He remains normally active and has no history of trauma. He has no fevers, rashes, or swelling. Examination reveals tenderness at the mid-dorsum of the foot medially. Radiographs are seen in Figures la and lb. Treatment should include which of the following?

Explanation
DISCUSSION: Osteochondrosis of the tarsal navicular is most commonly identified between the ages of 2 and 9 years. The condition is benign and self limited in nature. In patients with severe pain, a period of casting may be warranted, but otherwise management usually consists of observation or a supportive orthotic.
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
8 • American Academy of Orthopaedic Surgeons**
Figure 2
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
8 • American Academy of Orthopaedic Surgeons**
Figure 2
Question 34High Yield
Figures 63a and 63b show the radiographs of a 38-year-old man who reports low back and bilateral lower extremity pain. The spondylolisthesis is best classified as which of the following?
Explanation
Spondylolisthesis can be classified into five types. Type I, dysplastic, occurs at the lumbosacral junction as a result of congenital abnormalities of the upper sacrum and/or the arch of L5.Type II, isthmic, refers to those involving a lesion in the pars interarticularis. Type IIA, lytic, represents fatigue fractures of the pars. Type IIB describes those with elongated, but intact pars. Type IIC describes those that are a result of an acute fracture of the pars. Type III, degenerative spondylolisthesis, results from longstanding intersegmental disease. Type IV, traumatic, refers to those resulting from fractures in regions other than the pars, such as the pedicles. Type V, pathologic, refers to spondylolisthesis resulting from generalized or local bone disease. The radiographs demonstrate type II, isthmic spondylolisthesis.
Question 35High Yield
Which ancillary test is not helpful in the diagnosis of C harcot-Marie-Tooth disease (C MT):
Explanation
C harcot-Marie-Tooth disease (C MT) is a neuropathic process resulting in muscle atrophy, therefore, muscle enzyme studies will not be helpful.
Electromyography (EMG) will confirm the diagnosis by displaying increased amplitude and duration of signals, both of which are indicative of a neuropathic process.
Nerve conduction velocity (NC V) will also confirm the diagnosis by displaying decreased motor and sensory conduction velocities.
Nerve biopsy can be helpful by showing loss of myelinated fibers and fibrosis. Muscle biopsy will show diffuse atrophy, fibrosis, and adipose tissue within muscle.
Electromyography (EMG) will confirm the diagnosis by displaying increased amplitude and duration of signals, both of which are indicative of a neuropathic process.
Nerve conduction velocity (NC V) will also confirm the diagnosis by displaying decreased motor and sensory conduction velocities.
Nerve biopsy can be helpful by showing loss of myelinated fibers and fibrosis. Muscle biopsy will show diffuse atrophy, fibrosis, and adipose tissue within muscle.
Question 36High Yield
When a Workers' Compensation patient recovers after an injury to a point that further restoration of function is no longer anticipated, he or she is said to have reached which of the following?
Explanation
**
This is the definition of maximum medical improvement (MMI). The patient has essentially reached the plateau of his improvement.
Functional capacity evaluations (FCE) are based upon a theoretical model of comparing job demands to worker capabilities. The results of FCEs are often used to determine musculoskeletal capacity to return to work.
Strong et al. reported on the use of FCE in the Workers' Compensation system, and note how these FCE results are required by employers to determine the level of return to work of their employees. They also mention that the reports are frequently perceived with a negative tone. The employees reported a wider range of restrictions in their varied life roles than did the FCE reports, which deal more narrowly with work roles.
Pransky et al. reported that although FCE's are relied upon for determination of ability to perform physical work, several scientific, legal, and practical concerns persist. They note that test criteria often do not accurately reflect real-life job requirements or performance, and subjective evaluation remains common. They conclude that more research into predictive linking of FCE outcomes with occupational outcomes is necessary to determine their role in the Workers' Compensation system.
Incorrect Answers:
1: A functional capacity evaluation (FCE) is set of tests, practices and observations that are combined to determine the ability of the evaluated to function in a variety of circumstances (most often employment) in an objective manner.
3: Permanent disability is any lasting disability that results in a reduced earning capacity after maximum medical improvement is reached; this implies that MMI must be reached before this is determined.
4: Impairment rating is an objective data point obtained by a physician reviewing the patient's overall condition during a functional capacity evaluation.
5: This is the process a patient uses to tell their employer they want a personal physician to treat them for a work injury.
This is the definition of maximum medical improvement (MMI). The patient has essentially reached the plateau of his improvement.
Functional capacity evaluations (FCE) are based upon a theoretical model of comparing job demands to worker capabilities. The results of FCEs are often used to determine musculoskeletal capacity to return to work.
Strong et al. reported on the use of FCE in the Workers' Compensation system, and note how these FCE results are required by employers to determine the level of return to work of their employees. They also mention that the reports are frequently perceived with a negative tone. The employees reported a wider range of restrictions in their varied life roles than did the FCE reports, which deal more narrowly with work roles.
Pransky et al. reported that although FCE's are relied upon for determination of ability to perform physical work, several scientific, legal, and practical concerns persist. They note that test criteria often do not accurately reflect real-life job requirements or performance, and subjective evaluation remains common. They conclude that more research into predictive linking of FCE outcomes with occupational outcomes is necessary to determine their role in the Workers' Compensation system.
Incorrect Answers:
1: A functional capacity evaluation (FCE) is set of tests, practices and observations that are combined to determine the ability of the evaluated to function in a variety of circumstances (most often employment) in an objective manner.
3: Permanent disability is any lasting disability that results in a reduced earning capacity after maximum medical improvement is reached; this implies that MMI must be reached before this is determined.
4: Impairment rating is an objective data point obtained by a physician reviewing the patient's overall condition during a functional capacity evaluation.
5: This is the process a patient uses to tell their employer they want a personal physician to treat them for a work injury.
Question 37High Yield
What is the statistical likelihood that this boy could develop a progressive deformity for which surgery would be necessary?
Explanation
- Lower than 5%
Question 38High Yield
A 62-year-old man experiences pain in his right shoulder (Figures 89a through 89c).


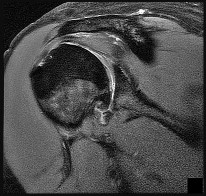
Explanation
- Anatomic total shoulder arthroplasty (TSA)_
Question 39High Yield
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
The arthroscopic image shows a tear through more than 50% of the biceps tendon; therefore, treatment should consist of tenodesis or tenotomy of the tendon. However, because this patient is relatively young and active, the treatment of choice is tenodesis of the biceps tendon.
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Burkhead WZ, Arcand MA, Zeman C, et al: The biceps tendon, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1996.
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Burkhead WZ, Arcand MA, Zeman C, et al: The biceps tendon, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1996.
Question 40High Yield
The patient ultimately undergoes rotationplasty. What is the most likely etiology of early limb loss after rotationplasty for sarcoma?
Explanation
- Vascular compromise_
Question 41High Yield
A 69-year-old man has nonpainful weakness in the upper and lower extremities. He also notes progressive instability in his gait and increasing difficulty ambulating, as well as manipulating small objects with his hands. MRI scans of his cervical spine are shown in Figures 85a and 85b. When would be the most appropriate time to proceed with surgical treatment?
---
---
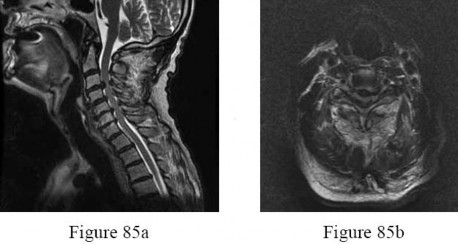
Explanation
The natural history of cervical myelopathy is one of slow deterioration over time, typically in a stepwise fashion with a variable period of stable neurologic function. More recent studies suggest that surgery should be performed as soon as possible when cervical spondylotic myelopathy has been diagnosed. Both anterior and posterior are effective and there is no statistical difference between their outcomes. Surgical outcome is related to the patient’s age, disease course, the presence of osseous spinal stenosis, preoperative comorbidities, the preoperative spinal cord functional score, and the presence of high-signal abnormalities on T2-weighted images. To improve the operative result, all the influencing factors should be considered. Patients with focal high-intensity intramedullary signal changes on T2-weighted images have better clinical outcomes following surgery than do patients with demonstrable multisegmental high-intensity intramedullary signal changes on T2-weighted sequences. The transverse area and shape of the spinal cord at the involved segment may also be predictive of surgical outcome.
With progressive compression, the cross section of the spinal cord changes from a boomerang shape to a teardrop shape to a triangular shape. In patients with a Nurick grade of I, there are signs of cord involvement, but gait remains normal. With a Nurick grade of II, there are mild gait abnormalities,not affecting the patient’s employment status. With a Nurick grade of III, gait abnormalities prevent employment, but the patient remains able to ambulate without assistance. In Nurick grade IV, the patient is only able to ambulate with assistance. In Nurick grade V, the patient is chair-bound or bedridden. Clearly, it is desirable to operate when the patient is functioning with a Nurick grade of I or II. Whereas many patients presenting with cervical spondylotic myelopathy also report axial neck pain and radicular symptoms in the upper extremities, this is not always the case. Surgical intervention will generally be effective in eliminating this pain; however, the pain is not the determining factor for performing surgery.Surgery is performed to preserve and restore function. Changes in bowel and bladder function can occur
in extremely severe cases of myelopathy, but this is quite rare.
With progressive compression, the cross section of the spinal cord changes from a boomerang shape to a teardrop shape to a triangular shape. In patients with a Nurick grade of I, there are signs of cord involvement, but gait remains normal. With a Nurick grade of II, there are mild gait abnormalities,not affecting the patient’s employment status. With a Nurick grade of III, gait abnormalities prevent employment, but the patient remains able to ambulate without assistance. In Nurick grade IV, the patient is only able to ambulate with assistance. In Nurick grade V, the patient is chair-bound or bedridden. Clearly, it is desirable to operate when the patient is functioning with a Nurick grade of I or II. Whereas many patients presenting with cervical spondylotic myelopathy also report axial neck pain and radicular symptoms in the upper extremities, this is not always the case. Surgical intervention will generally be effective in eliminating this pain; however, the pain is not the determining factor for performing surgery.Surgery is performed to preserve and restore function. Changes in bowel and bladder function can occur
in extremely severe cases of myelopathy, but this is quite rare.
Question 42High Yield
1247) When comparing the fibular plating techniques shown in Figures A and B, the plate position shown in Figure B is associated with which of the following?



Explanation
Lateral plating of the distal fibula has an increased risk of intra-articular screw penetration with the trajectory of the screws distally; bicortical screws will be intra-articular in nature, whereas posterior plating screws will exit anteriorly.
Figure A shows an antiglide (posterior) plating of the distal fibula, while Figure B shows a lateral neutralization plating of the distal fibula. Both methods are acceptable, but posterior antiglide plating is associated with increased construct stiffness and strength, decreased hardware prominence, decreased rates of ankle joint screw penetration, and improved biomechanical findings in osteoporotic bone. However, posterior plating is associated with an increased rate of peroneal tendonitis and irritation. Illustration A shows a lateral radiograph of a posterior fibular plate.
The referenced article by Ostrum et al is a case series of 32 patients who had antiglide plating; he reported a 100% union rate, 95% patient satisfaction rate, and only 4/32 reported peroneal tendinitis, with all resolving by 2
months.
The other referenced article by Schaffer et al reported that the posterolateral antiglide plate demonstrated improved biomechanical stability as compared to the lateral plating, with increased construct stiffness and load to failure.
Figure A shows an antiglide (posterior) plating of the distal fibula, while Figure B shows a lateral neutralization plating of the distal fibula. Both methods are acceptable, but posterior antiglide plating is associated with increased construct stiffness and strength, decreased hardware prominence, decreased rates of ankle joint screw penetration, and improved biomechanical findings in osteoporotic bone. However, posterior plating is associated with an increased rate of peroneal tendonitis and irritation. Illustration A shows a lateral radiograph of a posterior fibular plate.
The referenced article by Ostrum et al is a case series of 32 patients who had antiglide plating; he reported a 100% union rate, 95% patient satisfaction rate, and only 4/32 reported peroneal tendinitis, with all resolving by 2
months.
The other referenced article by Schaffer et al reported that the posterolateral antiglide plate demonstrated improved biomechanical stability as compared to the lateral plating, with increased construct stiffness and load to failure.
Question 43High Yield
A 23-year-old man is evaluated in the emergency department after a diving accident. Radiographs reveal bilateral jumped facets at C6-7. Examination reveals no motor function below the C7 level. There is some maintained sensation in the lower extremities. What is the patient's current grade on the ASIA (American Spinal Injury Association) impairment scale?
Explanation
■
The American Spinal Injury Association (ASIA) provides a standard method of measurement of spinal cord injury. The ASIA impairment scale is based on a comprehensive motor and sensory examination. An ASIA A grade is ascribed to a patient with an injury with no motor or sensory preservation below the injury. An ASIA B grade is defined as no motor preservation below the level of injury but some sensory preservation below the injury level. An ASIA C grade is defined as a motor function grade of less than 3 below the injury level.
An ASIA D grade is defined as a motor function grade of greater than 3 below the injury level. An ASIA E grade is defined as a normal neurologic examination.
The American Spinal Injury Association (ASIA) provides a standard method of measurement of spinal cord injury. The ASIA impairment scale is based on a comprehensive motor and sensory examination. An ASIA A grade is ascribed to a patient with an injury with no motor or sensory preservation below the injury. An ASIA B grade is defined as no motor preservation below the level of injury but some sensory preservation below the injury level. An ASIA C grade is defined as a motor function grade of less than 3 below the injury level.
An ASIA D grade is defined as a motor function grade of greater than 3 below the injury level. An ASIA E grade is defined as a normal neurologic examination.
Question 44High Yield
Figure 1 is the anteroposterior radiograph of a 20-year-old woman with mild right groin pain and intermittent "catching" in the hip region. What is the most appropriate next step?
41
41
Explanation
Because this patient is young, substantial bilateral acetabular dysplasia is present, and the joint space is well preserved, periacetabular osteotomy is the treatment of choice (Figure 2). Arthroscopic evaluation and treatment is insufficient to address the mechanical deformity. Although a hip injection can be diagnostically helpful, it would not alter the treatment plan in this scenario. The patient’s young age would make observation and subsequent THA less desirable. Femoral osteotomies also were performed to address rotational deformity.
42
42
Question 45High Yield
Flexion and extension of the elbow occur about an axis of rotation that
Explanation
The elbow mimics a true hinge and flexes and extends around an axis that is centered in the centers of the trochlea and capitellum. The medial epicondyle is not perfectly isometrically placed; rather the axis of rotation passes through a point on the anteroinferior aspect of the medial epicondyle. Application of a hinged external fixator is possible because of the fact that there is a single axis of rotation.
REFERENCES: Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 53-54.
London JT: Kinematics of the elbow. J Bone Joint Surg Am 1981;63:529-535.
Morrey BF, Chao EY: Passive motion of the elbow joint. J Bone Joint Surg Am 1976;58:501-508.
REFERENCES: Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 53-54.
London JT: Kinematics of the elbow. J Bone Joint Surg Am 1981;63:529-535.
Morrey BF, Chao EY: Passive motion of the elbow joint. J Bone Joint Surg Am 1976;58:501-508.
Question 46High Yield
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a
successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?

Explanation
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
Question 47High Yield
Which of the following tests is most specific for the diagnosis of Lyme disease:
Explanation
The most specific laboratory finding is an elevated antibody titer to Borrelia burgdorferi. This test is commonly referred to as a
Lyme titer.
All of the mentioned tests are generally seen in Lyme disease, however, elevated erythrocyte sedimentation rate, elevated C - reactive protein, negative antinuclear antibody, and negative rheumatoid factor are all nonspecific.
Lyme titer.
All of the mentioned tests are generally seen in Lyme disease, however, elevated erythrocyte sedimentation rate, elevated C - reactive protein, negative antinuclear antibody, and negative rheumatoid factor are all nonspecific.
Question 48High Yield
Figure below shows the radiograph obtained from a 73-year-old woman who returns status post total hip
arthroplasty 14 years earlier. She denies pain and has no discomfort on examination. She then undergoes revision total hip arthroplasty with head and liner exchange and bone grafting. After a physical therapy session two days after surgical intervention, she develops inability to dorsiflex the foot while she is sitting in a chair. The initial treatment should consist of
arthroplasty 14 years earlier. She denies pain and has no discomfort on examination. She then undergoes revision total hip arthroplasty with head and liner exchange and bone grafting. After a physical therapy session two days after surgical intervention, she develops inability to dorsiflex the foot while she is sitting in a chair. The initial treatment should consist of

Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis. This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis indefinite observation would not be appropriate. A foot drop develops 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MRI or CT may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be reduced by flexing the surgical knee and positioning the bed flat.
Question 49High Yield
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect.
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocation. Am J Sports Med 1995;23:324-331.
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocation. Am J Sports Med 1995;23:324-331.
Question 50High Yield
are the radiographs of a 23-year-old man who fell from a height and sustained an isolated injury to his right leg. Which of the following is a useful surgical technique to optimize alignment during intramedullary nailing?
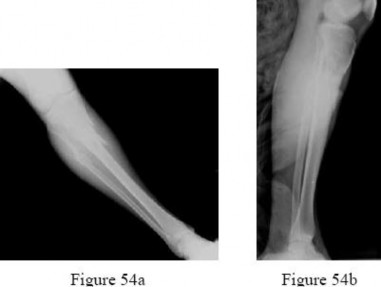
Explanation
No detailed explanation provided for this question.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon