Orthopedic With Answer Tumor/O Review | Dr Hutaif Ortho -...
14 Apr 2026
59 min read
92 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic With Answer Tumor/O Review | Dr Hu...
00:00
Start Quiz
Question 1High Yield
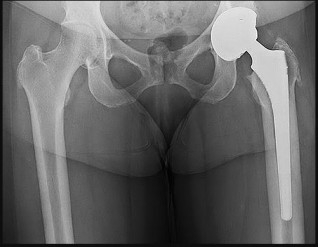
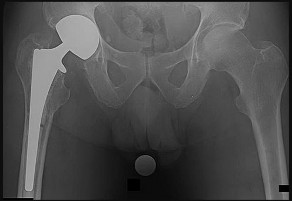
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated
left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure
left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure

Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 2High Yield
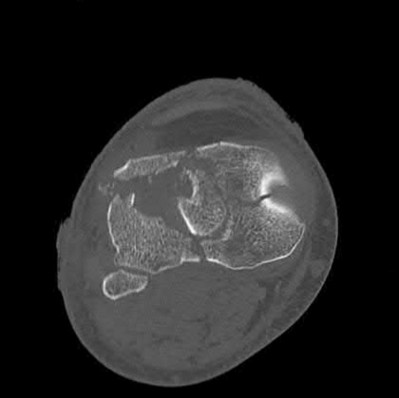
Figure 1 is the clinical photograph of an 11-year-old otherwise healthy boy who presents to the emergency department following 3 days of progressive left lateral ankle pain, difficulty bearing weight, swelling, and fever. He has a temperature of 102°F and other vitals are normal. He denies other areas of pain. He tolerates gentle ankle motion, and has exquisite point tenderness overlying the region of the distal fibular metaphysis. Radiographs of the ankle are normal. CRP is 32 mg/dL, ESR is 17, WBC count is 10.4. An MRI (Figure

Explanation
■
The clinical photograph and MRI image demonstrate focal swelling and a subperiosteal fluid collection, consistent with osteomyelitis and subperiosteal abscess. Appropriate management includes surgical drainage and antibiotics. Beginning antibiotics are both part of the treatment process, prompt identification of the subperiosteal abscess and decompression is a critical step. Neither waiting on cultures nor outpatient treatment provide sufficient treatment for the abscess. Infectious disease consultation may be utilized for antibiotic guidance; however, surgical management is necessary and takes priority.
■
The clinical photograph and MRI image demonstrate focal swelling and a subperiosteal fluid collection, consistent with osteomyelitis and subperiosteal abscess. Appropriate management includes surgical drainage and antibiotics. Beginning antibiotics are both part of the treatment process, prompt identification of the subperiosteal abscess and decompression is a critical step. Neither waiting on cultures nor outpatient treatment provide sufficient treatment for the abscess. Infectious disease consultation may be utilized for antibiotic guidance; however, surgical management is necessary and takes priority.
Question 3High Yield
1240) Which of the following factors is associated with the highest rate of nonunion of a midshaft clavicle fracture?

Explanation
The risk of nonunion in patients sustaining middle 1/3 clavicle fractures is increased in female patients.
Clavicle fractures are often secondary to direct blows to the lateral aspect of the shoulder. Physical examination is important to ascertain the status of the
skin and neurovascular structures to help guide treatment management. Although most non-displaced middle 1/3 clavicle fractures may be treated successfully with conservative measures, the risk for non-union (1-5%) increases with increasing comminution, female gender, shortening greater than 2 cm and an advanced age of the patient.
Robinson et al. reviewed 581 patients treated non-operatively for midshaft clavicle fractures. A nonunion rate of 4.5 % was identified at 24 weeks after the injury. They identified four factors that contributed to non-union, including: female gender, lack of cortical apposition, comminution of the fracture fragments and advancing age.
Zlowdzki et al. reviewed 2144 clavicle fracture cases in a comprehensive meta-analysis. They report displacement as the highest risk factor for nonunion (15.1%) in nonoperatively treated clavicle fractures, and simple slings were favored over figure of 8 braces. They also report an 86% reduction in the nonunion rate when operative fixation is chosen over nonoperative treatment for displaced clavicle fractures.
Illustration A shows the presence of a non-union of a midshaft clavicle fracture. A video is provided that reviews management of clavicle injuries.
Incorrect Answers
Answers 1, 3: Older patients and comminution of the fracture were found to be risk factors for non-union in midshaft clavicle injuries
Answers 4, 5: Neither of these are associated with an increased risk of nonunion in midshaft clavicular fractures.
Clavicle fractures are often secondary to direct blows to the lateral aspect of the shoulder. Physical examination is important to ascertain the status of the
skin and neurovascular structures to help guide treatment management. Although most non-displaced middle 1/3 clavicle fractures may be treated successfully with conservative measures, the risk for non-union (1-5%) increases with increasing comminution, female gender, shortening greater than 2 cm and an advanced age of the patient.
Robinson et al. reviewed 581 patients treated non-operatively for midshaft clavicle fractures. A nonunion rate of 4.5 % was identified at 24 weeks after the injury. They identified four factors that contributed to non-union, including: female gender, lack of cortical apposition, comminution of the fracture fragments and advancing age.
Zlowdzki et al. reviewed 2144 clavicle fracture cases in a comprehensive meta-analysis. They report displacement as the highest risk factor for nonunion (15.1%) in nonoperatively treated clavicle fractures, and simple slings were favored over figure of 8 braces. They also report an 86% reduction in the nonunion rate when operative fixation is chosen over nonoperative treatment for displaced clavicle fractures.
Illustration A shows the presence of a non-union of a midshaft clavicle fracture. A video is provided that reviews management of clavicle injuries.
Incorrect Answers
Answers 1, 3: Older patients and comminution of the fracture were found to be risk factors for non-union in midshaft clavicle injuries
Answers 4, 5: Neither of these are associated with an increased risk of nonunion in midshaft clavicular fractures.
Question 4High Yield
A 57-year-old man is involved in a rear-ended motor vehicle collision. He is able to leave his pickup and assist others involved in the collision. The next day he is seen in the emergency department with low back pain. The patient's radiograph and MRI scans of the lumbosacral spine are shown in Figures 1 through

Explanation
■
The patient has sustained a Morel-Lavallee lesion, a degloving injury of the lumbosacral and pelvic regions. It is sustained by a shear force that tears the subcutaneous tissue off the underlying muscular fascia. A resulting seroma develops secondary to blood, fat, and lymphatic fluid. The seroma often needs to be either percutaneously or surgically drained, depending on the size and associated bony injuries. Risks of inappropriately treated lesions can result in infection, tissue necrosis, or a chronic seroma.
The patient has sustained a Morel-Lavallee lesion, a degloving injury of the lumbosacral and pelvic regions. It is sustained by a shear force that tears the subcutaneous tissue off the underlying muscular fascia. A resulting seroma develops secondary to blood, fat, and lymphatic fluid. The seroma often needs to be either percutaneously or surgically drained, depending on the size and associated bony injuries. Risks of inappropriately treated lesions can result in infection, tissue necrosis, or a chronic seroma.
Question 5High Yield
Which of the following areas results in latitudinal physeal enlargement:
Explanation
The perichondrial ring of La Croix is the source of cells which differentiate into chondrocytes and results in latitudinal physeal enlargement.
The other answers refer to specifiCgrowth plate zones which have functions. The reserve zone is for matrix production and storage. The proliferative zone is for matrix production and cellular proliferation. The hypertrophiCzone contains the zone of maturation, degeneration, and provisional calcification.
The other answers refer to specifiCgrowth plate zones which have functions. The reserve zone is for matrix production and storage. The proliferative zone is for matrix production and cellular proliferation. The hypertrophiCzone contains the zone of maturation, degeneration, and provisional calcification.
Question 6High Yield
A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of the bone fragment and returns to play football the following year. He has a recurrent dislocation at football practice but decides to finish the football season before considering additional treatment. He sustains nine additional dislocations, with the last dislocation occurring while sleeping.What diagnostic test is most appropriate when planning revision surgery?
Explanation
DISCUSSION
A failed bony Bankart repair with multiple dislocations can further erode the anteroinferior glenoid, changing the sagittal morphology of the glenoid into an “inverted pear.” Quantitative bone loss is best evaluated by CT scan with 3-D reconstructions and subtraction of the humeral head. MRI and ultrasonography can assist in evaluating soft-tissue injury, but they are not as helpful in determining bone loss compared with a CT scan. An arthrogram alone is not sufficient to evaluate bone loss. Bone loss >30% necessitates glenoid augmentation with either a Latarjet procedure or iliac crest bone grafting. A revision arthroscopic or open Bankart repair with capsular shift or remplissage do not address bone loss. The Latarjet procedure can effectively restore stability with glenoid bone loss and after failed stabilizing procedures. Patients with pain before surgery are
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
DISCUSSION
A failed bony Bankart repair with multiple dislocations can further erode the anteroinferior glenoid, changing the sagittal morphology of the glenoid into an “inverted pear.” Quantitative bone loss is best evaluated by CT scan with 3-D reconstructions and subtraction of the humeral head. MRI and ultrasonography can assist in evaluating soft-tissue injury, but they are not as helpful in determining bone loss compared with a CT scan. An arthrogram alone is not sufficient to evaluate bone loss. Bone loss >30% necessitates glenoid augmentation with either a Latarjet procedure or iliac crest bone grafting. A revision arthroscopic or open Bankart repair with capsular shift or remplissage do not address bone loss. The Latarjet procedure can effectively restore stability with glenoid bone loss and after failed stabilizing procedures. Patients with pain before surgery are
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
Question 7High Yield
A 2-year-old child is brought to your office for evaluation of a "big hand." Upon examination, you notice that the child has mildly enlarged ring and small fingers. There is full range of motion without instability. The childâs parents inform you that they would like you to amputate the affected digits as soon as possible. You should:
Explanation
Although amputation may be necessary in some patients with macrodactyly, it is too early in the course of this case to begin entertaining such a drastic measure. A debulking procedure is not recommended for a 2-year-old child. Radiation therapy is not an option in uncomplicated cases of macrodactyly. The surgeon must educate the parents about the disease process and order additional testing.
Question 8High Yield
Which of the following molecules causes the expression of matrix metalloproteinases that can degrade the articular cartilage extracellular matrix:
Explanation
Interleukin I has the potential to increase expression of matrix metalloproteinases that can dissolve the extracellular matrix. The other responses are anabolic factors:
Insulin-dependent growth factor I Transforming growth factor beta Bone morphogenetic protein 2
Bone morphogenetic protein 7
Insulin-dependent growth factor I Transforming growth factor beta Bone morphogenetic protein 2
Bone morphogenetic protein 7
Question 9High Yield
A 72-year-old woman with diabetes mellitus has right hand numbness. Provocative test findings are consistent with carpal tunnel syndrome, and electrodiagnostic study (EDS) findings show prolonged median motor and sensory distal latencies with low-amplitude thenar compound muscle action potential. Poor prognosis is most associated with which factor?
Explanation
Although carpal tunnel syndrome remains a clinical diagnosis, EDS findings have become important tools. Moderate disease is defined as abnormal median sensory distal latency and prolonged median motor distal latency. Severe disease is defined as prolonged median motor and sensory distal latencies witheither absent sensory nerve action potential or mixed nerve action potential or low-amplitude or absent thenar compound muscle action potential. Although female gender and diabetes are considered risk factors, there is little association with postsurgical outcome. Severe disease as confirmed by EDS is the factor most _strongly associated with poor recovery after surgery._
Question 10High Yield
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?
Explanation
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function.
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
Question 11High Yield
Figures 6a and 6b are the radiographs of an injury for which a closed reduction procedure was unsuccessful. A dorsal approach to the metacarpophalangeal (MP) joint is chosen for open reduction. What is the most likely structure to impede the reduction?


Explanation
The radiograph shows the proximal phalanx nearly parallel with the metacarpal, where the simple dorsal dislocation of the phalanx is nearly perpendicular to the joint. A simple dislocation can be converted into a complex dislocation with attempts at closed reduction. The palmar plate, which is entrapped within the MP joint, should be incised longitudinally through its midline, allowing the metacarpal head to be reduced. For reduction of a simple dislocation, the wrist should be flexed to allow relaxation of the flexor tendons, and distal traction as well as volar-directed pressure to the base of the proximal phalanx can be successful in reducing a simple dislocation. Surgical reduction can be approached either dorsally or volarly. The volar approach jeopardizes the digital nerve. With a dorsal approach, the extensor hood and dorsal capsule should be incised longitudinally.
RECOMMENDED READINGS
1. Becton JL, Christian JD Jr, Goodwin HN, Jackson JG 3rd. A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am. 1975 Jul;57(5):698-700.
2. Green DP, Terry GC. Complex dislocation of the metacarpophalangeal joint. Correlative pathological anatomy. J Bone Joint Surg Am. 1973 Oct;55(7):1480-6.
RECOMMENDED READINGS
1. Becton JL, Christian JD Jr, Goodwin HN, Jackson JG 3rd. A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am. 1975 Jul;57(5):698-700.
2. Green DP, Terry GC. Complex dislocation of the metacarpophalangeal joint. Correlative pathological anatomy. J Bone Joint Surg Am. 1973 Oct;55(7):1480-6.
Question 12High Yield
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show
Explanation
The radiograph shows the correct tibial tunnel and anterior femoral tunnel; therefore, range of motion will most likely show loss of flexion.
REFERENCES: Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin
Bernhardt DT, Landry GL: Sports injuries in young athletes. Adv Pediatr 1995;42:465- Sports Med 1999;18:109-171.
Brown HR, Indelicato PA: Complications of anterior cruciate ligament reconstruction. Op Tech Orthop 1992;2:125-135.
REFERENCES: Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin
Bernhardt DT, Landry GL: Sports injuries in young athletes. Adv Pediatr 1995;42:465- Sports Med 1999;18:109-171.
Brown HR, Indelicato PA: Complications of anterior cruciate ligament reconstruction. Op Tech Orthop 1992;2:125-135.
Question 13High Yield
A cortisone injection in the subacromial space will most likely result in**
Explanation
A cortisone injection in the subacromial space will most likely result in elevated blood glucose levels in patients with type I diabetes mellitus. Patients should be warned of this potential complication. Cortisone does not have an effect on instability or proprioception, and a single injection would not affect osteoporosis. Repetitive injections or injection into the tendon itself could accelerate rupture of the biceps tendon.
REFERENCES: Matsen FA III, Arntz CT: Subacromial impingement, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 623-646.
Koehler BE, Urowitz MB, Killinger DW: The systemic effects of intra-articular corticosteroid. J Rheumatol 1974;1:117-125.
REFERENCES: Matsen FA III, Arntz CT: Subacromial impingement, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 623-646.
Koehler BE, Urowitz MB, Killinger DW: The systemic effects of intra-articular corticosteroid. J Rheumatol 1974;1:117-125.
Question 14High Yield
Which of the following blood vessels supplies the majority of the scaphoid:
Explanation
Gelberman and Menon used injection studies to demonstrate that the majority of scaphoid blood flow stems from branches of the radial artery entering the scaphoid at the distal pole. Of these, the branch entering the dorsal ridge supplies 70% to 80% of the intraosseous vascularity of the scaphoid bone. The proximal pole is completely dependent on the intraosseous blood supply and is vulnerable to avascular necrosis when fracture disrupts this vascular source.
Question 15High Yield
A 67-year-old man with right shoulder osteoarthritis (OA) remains symptomatic despite a course of nonsurgical treatment. A CT scan of the shoulder shows eccentric posterior glenoid wear with 10° of retroversion. What is the appropriate management of this glenoid bone loss during surgery for an anatomic total shoulder arthroplasty?
Explanation
DISCUSSION
Total shoulder arthroplasty (TSA) is superior to hemiarthroplasty for primary OA. The most common complication of TSA is glenoid loosening and malposition, which are common causes of glenoid failure. Glenoid malposition decreases the glenohumeral contact area and subsequently increases contact pressures. Altering the stem version to accommodate glenoid retroversion does not appropriately address soft-tissue balancing. A retroversion of <12° to 15° can be corrected with eccentric reaming without excessively compromising glenoid bone stock and risking glenoid vault penetration by the glenoid component. Posterior
glenoid bone grafting may be considered for glenoid retroversion >15°.
DISCUSSION
Total shoulder arthroplasty (TSA) is superior to hemiarthroplasty for primary OA. The most common complication of TSA is glenoid loosening and malposition, which are common causes of glenoid failure. Glenoid malposition decreases the glenohumeral contact area and subsequently increases contact pressures. Altering the stem version to accommodate glenoid retroversion does not appropriately address soft-tissue balancing. A retroversion of <12° to 15° can be corrected with eccentric reaming without excessively compromising glenoid bone stock and risking glenoid vault penetration by the glenoid component. Posterior
glenoid bone grafting may be considered for glenoid retroversion >15°.
Question 16High Yield
What is the incidence of malignant transformation for the lesion shown in Figures 24a and 24b?







Explanation
The lesion shown is an osteochondroma of the distal femur. In the vast majority of cases these are benign lesions, but malignant transformation to chondrosarcoma can occur in approximately 1% of solitary lesions. The malignant transformation rate can be as high as 25% to 30% among those with multiple hereditary exostosis. For solitary lesions, degeneration to chondrosarcoma occurs more commonly in sessile lesions, as opposed to those that are pedunculated, and in lesions that are located in the pelvis. Tumors typically become painful with malignant degeneration. Usually, if chondrosarcoma develops, it is a low-grade tumor.
RECOMMENDED READINGS
16. [T Scharschmidt, J Mayerson. Chrondrosarcoma. Orthopaedic Knowledge Online Journal. November 2010. ](http://www.aaos.org/OKOJ/vol8/issue10/ONC021/)http://www.aaos.org/OKOJ/vol8/issue10/ONC021/ Accessed May 2, 2016.
17. [Marco RA, Gitelis S, Brebach GT, Healey JH. Cartilage tumors: evaluation and treatment. J Am Acad Orthop Surg. 2000 Sep-Oct;8(5):292-304. Review. PubMed PMID: 11029557. ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11029557)
RECOMMENDED READINGS
16. [T Scharschmidt, J Mayerson. Chrondrosarcoma. Orthopaedic Knowledge Online Journal. November 2010. ](http://www.aaos.org/OKOJ/vol8/issue10/ONC021/)http://www.aaos.org/OKOJ/vol8/issue10/ONC021/ Accessed May 2, 2016.
17. [Marco RA, Gitelis S, Brebach GT, Healey JH. Cartilage tumors: evaluation and treatment. J Am Acad Orthop Surg. 2000 Sep-Oct;8(5):292-304. Review. PubMed PMID: 11029557. ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11029557)
Question 17High Yield
Figure 99 shows a dorsal approach for a midfoot arthrodesis following a Lisfranc injury in a 43-year-old woman. The base of the second metatarsal is labeled with the letter B. The interval used to create this exposure is
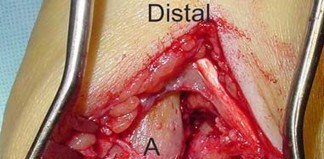
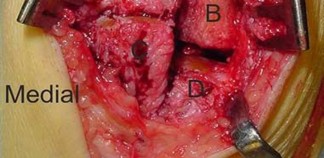
Explanation
The interval shown is between the extensor hallucis longus (left) and the extensor hallucis brevis (right), which is not an internervous plane because both are innervated by the deep peroneal nerve. The neurovascular bundle is under the extensor hallucis brevis muscle. Both
muscles are innervated by branches of the deep peroneal nerve. The superficial peroneal
86
nerve supplies muscles in the lateral compartment, and the medial plantar nerve supplies
muscles in the plantar medial aspect of the foot. The deep peroneal nerve innervates the anterior compartment muscles, the extensor hallucis brevis, and the extensor digitorum brevis muscle and supplies sensation to the dorsal first web space.
RECOMMENDED READINGS
1. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA: JB Lippincott; 1984:511-513.
2. Bellabarba C, Barei DP, Sanders RW. Dislocations of the foot. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 2. 8th ed. Philadelphia, PA: Mosby; 2007:2171-2180.
muscles are innervated by branches of the deep peroneal nerve. The superficial peroneal
86
nerve supplies muscles in the lateral compartment, and the medial plantar nerve supplies
muscles in the plantar medial aspect of the foot. The deep peroneal nerve innervates the anterior compartment muscles, the extensor hallucis brevis, and the extensor digitorum brevis muscle and supplies sensation to the dorsal first web space.
RECOMMENDED READINGS
1. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA: JB Lippincott; 1984:511-513.
2. Bellabarba C, Barei DP, Sanders RW. Dislocations of the foot. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 2. 8th ed. Philadelphia, PA: Mosby; 2007:2171-2180.
Question 18High Yield
-Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
Explanation
FOR QUESTIONS 108 THROUGH 110:**_
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
Question 19High Yield
Figure 81
Explanation
- Well-fixed uncemented stem_
Question 20High Yield
What is the most likely underlying bone problem?
Explanation
- A genetic defect in the type I collagen gene
Question 21High Yield
Figures 23a and 23b show
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
Explanation
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Penn I: Infections in the diabetic foot, in Samarco GJ (ed): The Foot in Diabetes. Philadelphia, PA, Lea & Febiger, 1991, pp 109-121. Wagner FW: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981, pp 66-122.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Penn I: Infections in the diabetic foot, in Samarco GJ (ed): The Foot in Diabetes. Philadelphia, PA, Lea & Febiger, 1991, pp 109-121. Wagner FW: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981, pp 66-122.
#
Question 22High Yield
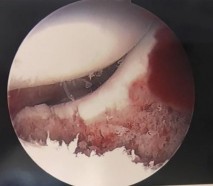
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
---
---
---
---
---
---
---
---



Explanation
The images show a full-thickness cartilage defect with significant bony involvement >4 cm2. Microfracture should be considered for lesions <2 cm2 without an underlying osseous defect. Autologous chondrocyte implantation, although used for lesions between 1 and 10 cm2, should be restricted for defects with minimal (<8 mm depth) bone loss. Osteochondral allograft transfer with the mosaicplasty technique (transfer of multiple plugs) would be well-suited for this large defect with significant osseous involvement. Dejour trochleoplasty is performed for patellar instability to correct trochlear dysplasia and _would not be indicated in this case._
Question 23High Yield
Intra-articular, not extra-articular, hydrostatic pressure changes would affect chondrocytes.
Which of the following medications exerts its influence on the clotting cascade by inhibiting the carboxylation of normal clotting factors?
Which of the following medications exerts its influence on the clotting cascade by inhibiting the carboxylation of normal clotting factors?














Explanation
Warfarin (Coumadin) exerts its anticoagulation effect by inhibiting the carboxylation of normal clotting factors. Warfarin is a vitamin K antagonist
that prevents the reductive metabolism of vitamin K epoxide back to its active form, hydroquinone, by inhibiting the enzymes responsible for the reaction. The vitamin K- dependent factors are II, VII, IX, X, proteins C, and S.
The reference by Hyers is a review article discussing the antithrombotic agents that have been used in the last 50 years and also discusses some of the newer ones that have since been developed.
Berry in his review discusses the risk factors, efficacy, and safety of agents used in 2003 after total hip arthroplasty.
: Enoxaparin binds to and increases the activity of antithrombin III. By activating antithrombin III, enoxaparin potentiates the inhibition of coagulation factors Xa and IIa.
Answer 3: Dalteparin is a low molecular weight heparin
Answer 4: Heparin binds to the enzyme inhibitor antithrombin III. The activated AT then inactivates thrombin and other proteases involved in blood clotting, most notably factor Xa.
Answer 5: Hirudin (the active component released by leeches), is often considered the most potent inhibitor of thrombin.
A 25-year-old healthy male is scheduled to undergo a a nine-level posterior spinal fusion for scoliosis. Administering preoperative recombinant erythropoietin would place the patient at increased risk of developing which of the following complications?
1) Acute renal failure
2) Increased bleeding time
3) Thrombotic event
4) Wound complications
5) Delayed spinal fusion
The use of recombinant erythropoietin(EPO) preoperatively for patients undergoing major elective orthopedic surgery has been associated with a higher incidence of deep vein thrombosis (DVT).
Johnson et al present a Level 5 review of recombinant eryrthropoetin (Epoetin alfa). When hypoxia in the body is detected, the kidney is stimulated to produce EPO in the renal cortical interstitial cells. EPO interacts with progenitor stem cells in the bone marrow to increase RBC production. The use of erythropoietin does decrease transfusion rates, but has no effect on renal function, bleeding times, wound complications, or bony healing.
The Level 1 study by Beris et al studied the use of recombinant human erythropoietin as an adjuvant treatment to autologous blood transfusions in elective surgery. They reported a 10% DVT rate with the 300 U/kg recombinant EPO (10%) dosage versus placebo (5% rate).
A 4-year-old female is brought by her parents in regard to a right sided limp that improves during the day and has been present for two months. She is found to have a right knee effusion and associated
soft-tissue swelling with no redness or warmth. Lab work reveals negative Rheumatoid factor, a positive low titer ANA and a normal WBC. Radiographs are normal for her age. What additional work up does she need?
1) Skeletal survey
2) MRI of the pelvis
3) Clotting factor levels
4) Ophthalmology evaluation
5) Bone scan
This patient has a history and physical findings consistent with juvenile idiopathic arthritis (JIA). This type of JIA specifically has a high association
with iridocyclitis, particularly in those with positive ANA studies (approximately
20%). Patients with JIA require an ophthalmology consultation for slit lamp examination to evaluate for anterior uveitis, with any type of pupil asymmetry requiring an immediate consultation. Eye involvement can be indolent and lead to blindness if not promptly identified. Due to early treatment of the uveitis, blindness has become a rare complication.
The Sherry article provides an overview of new treatment methods including intraarticular joint injections of methotrexate and etanercept, which have produced giant leaps in the treatment of the associated joint inflammation and resultant destruction.
A 25-year-old male sustains a transverse humeral shaft fracture and undergoes open reduction and internal fixation with rigid compression plating. What kind of bone healing would be expected with this type of fracture fixation?
1) Primary bone healing through haversian remodeling
2) Secondary healing through callus formation
3) Primary healing through callus formation
4) Endochondral ossification
5) Secondary healing through osteonal cutting cones
Fractures and osteotomies that are stabilized with rigid compression plating undergo primary bone healing, also known as haversian remodeling. Absolute stability constructs, such as a compression plate, allow for bone healing without visible callus formation.
Healing occurs via extension of clusters of osteoclasts (known as osteonal cutting cones) across the fracture site, along with osteoblasts depositing new bone and blood vessels to re-establish the haversian system.
Seconday bone healing occurs when fractures heal through callus formation. Relative stability constructs, such as an intramedullary nail, allow for some motion at the fracture site which leads to healing through a cartilage scaffold (endochondral ossification).
Illustration A demonstrates a transverse fracture stabilized with a compression plate. Illustration B shows a femoral shaft fracture that has healed through callus formation.
Incorrect Answers:
Answer 2: Secondary healing through callus formation occurs when fractures heal with some motion at the fracture site; for example intramedullary nailing of a diaphyseal femur fracture
Answer3: Primary healing is defined by the absence of visible callus
Answer 4: Endochondral ossification is bone generation or healing through a cartilage scaffold
Answer 5: Secondary healing does not occur through osteonal cutting cones as there not enough stability at the fracture site
When analysing complex geometric form and material property distributions, the structure of interest may be divided up into numerous connected subregions or elements within which approximate functions are used to represent the unknown quantity. What is the name for this technique?
1) Breakdown synthesis
2) Finite element method
3) Algebraic conclusion
4) Differential equations
5) Isogeometric analysis
To solve a problem with complex geometric form and material property distributions, the finite element approach is used to break the problem up into smaller “finite elements” with simple geometric form. Usually triangular or quadrilateral elements are used. A computer program is written to balance the forces and moments acting on each element, and match these forces and moments with those of its neighboring elements. For large structures with a large number of elements, the computer must solve thousands of algebraic equations to make sure all the forces are balanced in the interior of the body and at the surface where the forces are applied. In orthopedics, stress analysis of the cement fixation of implants to bone is frequently carried out using finite element analysis.
A load-elongation curve for a tendon is shown in Figure A. Which of the following statements accurately describes the region labeled "X"?
1) The failure region which has crimped tendon fibers
2) The linear region which has parallel oriented tendon fibers
3) The linear region which has crimped tendon fibers
4) The toe region which has parallel oriented tendon fibers
5) The toe region which has crimped tendon fibers
Region "X" in the illustration is the toe region of the load-elongation curve. This region represents the initial elongation during which a small amount of tension causes crimped, randomly arranged fibrils to become aligned parallel along the direction of loading.
Magnusson et al looked at the properties of tendon in relation to muscular activity and training. Collagen composition of tendon is organized in a very hierarchical manner along parallel bundles. Tendon collagen bundles have a more parallel orientation along the long axis than ligaments, making their toe region smaller. Illustration A shows all the regions of the load-elongation curve.
Which of the following molecules binds to the surface of hydroxyapatite crystals and prevents protein prenylation?
1) Calcitonin
2) Parathyroid Hormone
3) Raloxifene
4) Calcium
5) Alendronate
Bisphophonates accumulate in high concentration in bones due to their binding affinity to hydroxyapatite crystals.
There are two types of bisphosphonates with different mechanisms, although both classes ultimately inhibit osteoclast resorption of bone. Nitrogen containing bisphosphonates (alendronate/Fosamax, pamidronate/Aredia, risedronate/Actonel) prevent protein prenylation by inhibiting farnesyl diphosphate synthase, an enzyme in the mevalonate (cholesterol) pathway.
The non-nitrogenous bisphosphonates (etidronate/Didronel, clodronate, tiludronate) are metabolised in the cell to compounds that replace the terminal pyrophosphate moiety of ATP, forming a nonfunctional molecule that competes with adenosine triphosphate (ATP) in the cellular energy metabolism. Due to this disruption in metabolism, the osteoclast initiates apoptosis and dies, leading to an overall decrease in the breakdown of bone.
Which of the following foot radiographs is most consistent with the diagnosis of gout?
1) A
2) B
3) C
4) D
5) E
Figure B is most consistent with a diagnosis of gout.
Gout results from deposition of the monosodium urate crystal. It affects the lower limb, resulting in arthritis of the great toe (podagra). On radiographic evaluation, periarticular erosions in the setting of tophaceous formations may be seen.
Egan et al. describe the characteristic radiographic findings of gout in the foot. This includes asymmetric polyarthropathy, well-defined erosions with sclerotic margins, overhanging bony edges and tophaceous formations.
Figure B shows an AP radiograph of a foot affected by gout. Note the periarticular erosions, soft tissue calcifications (tophi), overhanging bony edges and asymmetric joint wear.
Incorrect Answers:
Answer 1: Figure A is consistent with psoriatic arthritis. Notice the bilateral involvement and the pencil-in-cup deformity seen in the great toe.
Answer 3: Figure C is consistent with Freiberg’s infarction. Note the flattening of the second metatarsal head in addition to joint sclerosis
Answer 4: Figure D is consistent with Charcot arthropathy. Note the involvement of the hindfoot. There is fragmentation and severe joint space narrowing
Answer 5: Figure E is consistent with rheumatoid arthritis. Note the loss of asphericity of the 1st metatarsal head, with concomitant dislocations of the
2nd and 3rd MTP joints
Which of the following sarcomas is correctly paired with its most common translocation?
1) Alveolar rhabdomyosarcoma: t(9;22)
2) Synovial sarcoma: t(11;22)
3) Ewing's sarcoma: t(12;16)
4) Myxoid liposarcoma: t(X;18)
5) Clear cell sarcoma t(12;22)
Chromosomal translocations are characteristically associated with several sub- types of soft tissue sarcomas. The most common clear cell sarcoma translocation is t(12:22). A histologic example is found in illustration A.
Many sarcomas have distinct translocations which can help identify them via cytogenetic testing. The most common are alveolar rhabdomyosarcoma:t(2;13), synovial sarcoma:t(X;18), Ewing’s sarcoma: t(11,22), myxoid liposarcoma:t(12;16), and chondrosarcoma:t(9;22). Histologic examples are in Illustrations B through F, respectively. Osteosarcoma does not have a characteristic translocation.
In a review article, Rabbits described many fusion proteins resulting from chromosomal translocations. As many are nuclear proteins, future molecular
based therapies are being developed to target steps from oncogene transcription to RNA translation. Solomon et al reviewed chromosome aberrations in rare and common tumors. A broader understanding of chromosomal abnormalities and fusion proteins will aid gene-targeted diagnosis and therapies.
A 65-year-old female undergoes a total knee arthroplasty. In addition to chemoprophylaxis for deep vein thrombosis (DVT) prevention she is given pneumatic compression devices. Which of the following is associated with pneumatic compression devices?
1) Increased endothelial fibrinogenesis
2) Decreased bleeding times
3) Increased endothelial injury
4) Increased venous compliance
5) Increased venous blood flow
External pneumatic compression devices have been shown to prevent the formation of DVTs. Modern devices evacuate blood from lower-extremity vessels in an automated fashion. Pneumatic compression may exert its protective effect against thrombus formation in part by increasing venous blood flow. Pneumatic compression devices do
not decrease bleeding time or cause endothelial injury. Pneumatic compression devices enhance endothelial derived fibrinolysis and decrease venous compliance.
Rogers et al present practice management guidelines for DVT prophylaxis in trauma patients. They state that the exact mechanism of action of pneumatic compression devices are not fully understood. However, there is good evidence that they increase mean and peak femoral vein velocity and there are a few studies concluding that the fibrinolytic system is activated.
**Which of the following substances is most osteoinductive?**
1) Calcium phosphate
2) Hydroxyapatite
3) Xenograft collagen sheet
4) Cancellous allograft
5) Cancellous autograft
An ideal bone-graft substitute must provide scaffolding for osteoconduction as well as progenitor cells and growth factors for osteoinduction. Furthermore, the bone graft must be able to integrate with the host. Autogenous bone graft contains osteoblasts, endosteal osteoprogenitor cells capable of synthesizing new bone, and a structural matrix that acts as a scaffold, making it the gold standard for bone grafting. BMP-2 is a commonly utilized adjunct for grafting, and is inherently osteoinductive.
The referenced article by Buckwalter et al is a review on the biology of bone grafting which nicely defines the various osteoinductive and osteoconductive properties of the various bone graft options.
Regarding skeletal muscles, which of the following is true?
1) Force generated is most dependent on muscle length
2) Force generated is most dependent on muscle fiber type
3) Type I muscle is comprised of fast twitch fibrils
4) Duration and speed of contraction are most dependent on cross-sectional area
5) Duration and speed of contraction are most dependent on muscle fiber type
The duration and speed of contraction is most dependent on the muscle fiber type. The force generated by the muscle is most dependent on the cross- sectional area of the muscle.
Fiber types have less to do with the force of contraction and more to do with the duration and speed of contraction. The cross-sectional area of a muscle determines to a great extent the force generated by the muscle and is controlled by the number of myofibrils that contract. Muscle length affects contraction force through the Blix curve. The morphology of a muscle can affect the cross-sectional area by varying the angle of the fibers in relation to the force vector.
Incorrect Answers:
Warfarin (Coumadin) exerts its anticoagulation effect by inhibiting the carboxylation of normal clotting factors. Warfarin is a vitamin K antagonist
that prevents the reductive metabolism of vitamin K epoxide back to its active form, hydroquinone, by inhibiting the enzymes responsible for the reaction. The vitamin K- dependent factors are II, VII, IX, X, proteins C, and S.
The reference by Hyers is a review article discussing the antithrombotic agents that have been used in the last 50 years and also discusses some of the newer ones that have since been developed.
Berry in his review discusses the risk factors, efficacy, and safety of agents used in 2003 after total hip arthroplasty.
: Enoxaparin binds to and increases the activity of antithrombin III. By activating antithrombin III, enoxaparin potentiates the inhibition of coagulation factors Xa and IIa.
Answer 3: Dalteparin is a low molecular weight heparin
Answer 4: Heparin binds to the enzyme inhibitor antithrombin III. The activated AT then inactivates thrombin and other proteases involved in blood clotting, most notably factor Xa.
Answer 5: Hirudin (the active component released by leeches), is often considered the most potent inhibitor of thrombin.
A 25-year-old healthy male is scheduled to undergo a a nine-level posterior spinal fusion for scoliosis. Administering preoperative recombinant erythropoietin would place the patient at increased risk of developing which of the following complications?
1) Acute renal failure
2) Increased bleeding time
3) Thrombotic event
4) Wound complications
5) Delayed spinal fusion
The use of recombinant erythropoietin(EPO) preoperatively for patients undergoing major elective orthopedic surgery has been associated with a higher incidence of deep vein thrombosis (DVT).
Johnson et al present a Level 5 review of recombinant eryrthropoetin (Epoetin alfa). When hypoxia in the body is detected, the kidney is stimulated to produce EPO in the renal cortical interstitial cells. EPO interacts with progenitor stem cells in the bone marrow to increase RBC production. The use of erythropoietin does decrease transfusion rates, but has no effect on renal function, bleeding times, wound complications, or bony healing.
The Level 1 study by Beris et al studied the use of recombinant human erythropoietin as an adjuvant treatment to autologous blood transfusions in elective surgery. They reported a 10% DVT rate with the 300 U/kg recombinant EPO (10%) dosage versus placebo (5% rate).
A 4-year-old female is brought by her parents in regard to a right sided limp that improves during the day and has been present for two months. She is found to have a right knee effusion and associated
soft-tissue swelling with no redness or warmth. Lab work reveals negative Rheumatoid factor, a positive low titer ANA and a normal WBC. Radiographs are normal for her age. What additional work up does she need?
1) Skeletal survey
2) MRI of the pelvis
3) Clotting factor levels
4) Ophthalmology evaluation
5) Bone scan
This patient has a history and physical findings consistent with juvenile idiopathic arthritis (JIA). This type of JIA specifically has a high association
with iridocyclitis, particularly in those with positive ANA studies (approximately
20%). Patients with JIA require an ophthalmology consultation for slit lamp examination to evaluate for anterior uveitis, with any type of pupil asymmetry requiring an immediate consultation. Eye involvement can be indolent and lead to blindness if not promptly identified. Due to early treatment of the uveitis, blindness has become a rare complication.
The Sherry article provides an overview of new treatment methods including intraarticular joint injections of methotrexate and etanercept, which have produced giant leaps in the treatment of the associated joint inflammation and resultant destruction.
A 25-year-old male sustains a transverse humeral shaft fracture and undergoes open reduction and internal fixation with rigid compression plating. What kind of bone healing would be expected with this type of fracture fixation?
1) Primary bone healing through haversian remodeling
2) Secondary healing through callus formation
3) Primary healing through callus formation
4) Endochondral ossification
5) Secondary healing through osteonal cutting cones
Fractures and osteotomies that are stabilized with rigid compression plating undergo primary bone healing, also known as haversian remodeling. Absolute stability constructs, such as a compression plate, allow for bone healing without visible callus formation.
Healing occurs via extension of clusters of osteoclasts (known as osteonal cutting cones) across the fracture site, along with osteoblasts depositing new bone and blood vessels to re-establish the haversian system.
Seconday bone healing occurs when fractures heal through callus formation. Relative stability constructs, such as an intramedullary nail, allow for some motion at the fracture site which leads to healing through a cartilage scaffold (endochondral ossification).
Illustration A demonstrates a transverse fracture stabilized with a compression plate. Illustration B shows a femoral shaft fracture that has healed through callus formation.
Incorrect Answers:
Answer 2: Secondary healing through callus formation occurs when fractures heal with some motion at the fracture site; for example intramedullary nailing of a diaphyseal femur fracture
Answer3: Primary healing is defined by the absence of visible callus
Answer 4: Endochondral ossification is bone generation or healing through a cartilage scaffold
Answer 5: Secondary healing does not occur through osteonal cutting cones as there not enough stability at the fracture site
When analysing complex geometric form and material property distributions, the structure of interest may be divided up into numerous connected subregions or elements within which approximate functions are used to represent the unknown quantity. What is the name for this technique?
1) Breakdown synthesis
2) Finite element method
3) Algebraic conclusion
4) Differential equations
5) Isogeometric analysis
To solve a problem with complex geometric form and material property distributions, the finite element approach is used to break the problem up into smaller “finite elements” with simple geometric form. Usually triangular or quadrilateral elements are used. A computer program is written to balance the forces and moments acting on each element, and match these forces and moments with those of its neighboring elements. For large structures with a large number of elements, the computer must solve thousands of algebraic equations to make sure all the forces are balanced in the interior of the body and at the surface where the forces are applied. In orthopedics, stress analysis of the cement fixation of implants to bone is frequently carried out using finite element analysis.
A load-elongation curve for a tendon is shown in Figure A. Which of the following statements accurately describes the region labeled "X"?
1) The failure region which has crimped tendon fibers
2) The linear region which has parallel oriented tendon fibers
3) The linear region which has crimped tendon fibers
4) The toe region which has parallel oriented tendon fibers
5) The toe region which has crimped tendon fibers
Region "X" in the illustration is the toe region of the load-elongation curve. This region represents the initial elongation during which a small amount of tension causes crimped, randomly arranged fibrils to become aligned parallel along the direction of loading.
Magnusson et al looked at the properties of tendon in relation to muscular activity and training. Collagen composition of tendon is organized in a very hierarchical manner along parallel bundles. Tendon collagen bundles have a more parallel orientation along the long axis than ligaments, making their toe region smaller. Illustration A shows all the regions of the load-elongation curve.
Which of the following molecules binds to the surface of hydroxyapatite crystals and prevents protein prenylation?
1) Calcitonin
2) Parathyroid Hormone
3) Raloxifene
4) Calcium
5) Alendronate
Bisphophonates accumulate in high concentration in bones due to their binding affinity to hydroxyapatite crystals.
There are two types of bisphosphonates with different mechanisms, although both classes ultimately inhibit osteoclast resorption of bone. Nitrogen containing bisphosphonates (alendronate/Fosamax, pamidronate/Aredia, risedronate/Actonel) prevent protein prenylation by inhibiting farnesyl diphosphate synthase, an enzyme in the mevalonate (cholesterol) pathway.
The non-nitrogenous bisphosphonates (etidronate/Didronel, clodronate, tiludronate) are metabolised in the cell to compounds that replace the terminal pyrophosphate moiety of ATP, forming a nonfunctional molecule that competes with adenosine triphosphate (ATP) in the cellular energy metabolism. Due to this disruption in metabolism, the osteoclast initiates apoptosis and dies, leading to an overall decrease in the breakdown of bone.
Which of the following foot radiographs is most consistent with the diagnosis of gout?
1) A
2) B
3) C
4) D
5) E
Figure B is most consistent with a diagnosis of gout.
Gout results from deposition of the monosodium urate crystal. It affects the lower limb, resulting in arthritis of the great toe (podagra). On radiographic evaluation, periarticular erosions in the setting of tophaceous formations may be seen.
Egan et al. describe the characteristic radiographic findings of gout in the foot. This includes asymmetric polyarthropathy, well-defined erosions with sclerotic margins, overhanging bony edges and tophaceous formations.
Figure B shows an AP radiograph of a foot affected by gout. Note the periarticular erosions, soft tissue calcifications (tophi), overhanging bony edges and asymmetric joint wear.
Incorrect Answers:
Answer 1: Figure A is consistent with psoriatic arthritis. Notice the bilateral involvement and the pencil-in-cup deformity seen in the great toe.
Answer 3: Figure C is consistent with Freiberg’s infarction. Note the flattening of the second metatarsal head in addition to joint sclerosis
Answer 4: Figure D is consistent with Charcot arthropathy. Note the involvement of the hindfoot. There is fragmentation and severe joint space narrowing
Answer 5: Figure E is consistent with rheumatoid arthritis. Note the loss of asphericity of the 1st metatarsal head, with concomitant dislocations of the
2nd and 3rd MTP joints
Which of the following sarcomas is correctly paired with its most common translocation?
1) Alveolar rhabdomyosarcoma: t(9;22)
2) Synovial sarcoma: t(11;22)
3) Ewing's sarcoma: t(12;16)
4) Myxoid liposarcoma: t(X;18)
5) Clear cell sarcoma t(12;22)
Chromosomal translocations are characteristically associated with several sub- types of soft tissue sarcomas. The most common clear cell sarcoma translocation is t(12:22). A histologic example is found in illustration A.
Many sarcomas have distinct translocations which can help identify them via cytogenetic testing. The most common are alveolar rhabdomyosarcoma:t(2;13), synovial sarcoma:t(X;18), Ewing’s sarcoma: t(11,22), myxoid liposarcoma:t(12;16), and chondrosarcoma:t(9;22). Histologic examples are in Illustrations B through F, respectively. Osteosarcoma does not have a characteristic translocation.
In a review article, Rabbits described many fusion proteins resulting from chromosomal translocations. As many are nuclear proteins, future molecular
based therapies are being developed to target steps from oncogene transcription to RNA translation. Solomon et al reviewed chromosome aberrations in rare and common tumors. A broader understanding of chromosomal abnormalities and fusion proteins will aid gene-targeted diagnosis and therapies.
A 65-year-old female undergoes a total knee arthroplasty. In addition to chemoprophylaxis for deep vein thrombosis (DVT) prevention she is given pneumatic compression devices. Which of the following is associated with pneumatic compression devices?
1) Increased endothelial fibrinogenesis
2) Decreased bleeding times
3) Increased endothelial injury
4) Increased venous compliance
5) Increased venous blood flow
External pneumatic compression devices have been shown to prevent the formation of DVTs. Modern devices evacuate blood from lower-extremity vessels in an automated fashion. Pneumatic compression may exert its protective effect against thrombus formation in part by increasing venous blood flow. Pneumatic compression devices do
not decrease bleeding time or cause endothelial injury. Pneumatic compression devices enhance endothelial derived fibrinolysis and decrease venous compliance.
Rogers et al present practice management guidelines for DVT prophylaxis in trauma patients. They state that the exact mechanism of action of pneumatic compression devices are not fully understood. However, there is good evidence that they increase mean and peak femoral vein velocity and there are a few studies concluding that the fibrinolytic system is activated.
**Which of the following substances is most osteoinductive?**
1) Calcium phosphate
2) Hydroxyapatite
3) Xenograft collagen sheet
4) Cancellous allograft
5) Cancellous autograft
An ideal bone-graft substitute must provide scaffolding for osteoconduction as well as progenitor cells and growth factors for osteoinduction. Furthermore, the bone graft must be able to integrate with the host. Autogenous bone graft contains osteoblasts, endosteal osteoprogenitor cells capable of synthesizing new bone, and a structural matrix that acts as a scaffold, making it the gold standard for bone grafting. BMP-2 is a commonly utilized adjunct for grafting, and is inherently osteoinductive.
The referenced article by Buckwalter et al is a review on the biology of bone grafting which nicely defines the various osteoinductive and osteoconductive properties of the various bone graft options.
Regarding skeletal muscles, which of the following is true?
1) Force generated is most dependent on muscle length
2) Force generated is most dependent on muscle fiber type
3) Type I muscle is comprised of fast twitch fibrils
4) Duration and speed of contraction are most dependent on cross-sectional area
5) Duration and speed of contraction are most dependent on muscle fiber type
The duration and speed of contraction is most dependent on the muscle fiber type. The force generated by the muscle is most dependent on the cross- sectional area of the muscle.
Fiber types have less to do with the force of contraction and more to do with the duration and speed of contraction. The cross-sectional area of a muscle determines to a great extent the force generated by the muscle and is controlled by the number of myofibrils that contract. Muscle length affects contraction force through the Blix curve. The morphology of a muscle can affect the cross-sectional area by varying the angle of the fibers in relation to the force vector.
Incorrect Answers:
Question 24High Yield
A 25-year-old, training for a marathon, presents with persistent heel pain over the past several weeks. He has difficulty with ambulation and has an antalgic gait. A squeeze test of the heel is positive. A lateral foot radiograph is shown Figure A. Of the options listed below, what is the most appropriate next step in management?


Explanation
with patient or after the diagnosis is confirmed with a MRI. However, in this scenario 4-6 months of nonweightbearing is likely excessive.
Question 25High Yield
Figures 1 through 5 are the radiograph, MRI scan, and clinical photograph of a 9-year-old boy who has a new wound of the posteromedial heel without recent injury or fevers. He has a 2-month history of heel pain and has been treated for calcaneal apophysitis with a walking boot. Complete blood count, CRP level, and ESR are normal. What is the best next step?

Explanation
■
This patient has chronic calcaneal osteomyelitis. Pediatric calcaneal osteomyelitis may follow an indolent course with a delay in diagnosis. Given the draining wound, chronic radiographic changes; and MRI evidence of abscess, operative biopsy and debridement is the next step. Iliac crest aspiration may be appropriate if leukemia is suspected based upon the complete blood count. A bone scan or skeletal survey may be a consideration if the biopsy is consistent with malignancy or if the patient has poorly localized symptoms.
■
This patient has chronic calcaneal osteomyelitis. Pediatric calcaneal osteomyelitis may follow an indolent course with a delay in diagnosis. Given the draining wound, chronic radiographic changes; and MRI evidence of abscess, operative biopsy and debridement is the next step. Iliac crest aspiration may be appropriate if leukemia is suspected based upon the complete blood count. A bone scan or skeletal survey may be a consideration if the biopsy is consistent with malignancy or if the patient has poorly localized symptoms.
Question 26High Yield
A 44-year-old female sustains the injury shown in Figures A and B as the result of a motor vehicle collision. She undergoes immediate four compartment leg fasciotomy and placement of a spanning external fixator. A post-fixator CT scan image is shown in Figure C. After allowing her soft tissues to improve, the optimal definitive stabilization of this fracture is which of the following?


Explanation
Treatment of a comminuted bicondylar tibial plateau fracture such as the one shown in Figures A and B is best treated with dual plates (or more), as the posteromedial fragment(s) is usually a large section of the medial plateau and is poorly stabilized from a single lateral plate.
Barei et al (2008) retrospectively reviewed 57 patients with bicondylar tibial plateau fractures, evaluating the frequency and morphologic characteristics of the posteromedial fragment in this injury pattern. They found that 74% of these injuries had a posteromedial fragment that may require alternate or supplementary fixation methods when managing this injury pattern.
Barei et al (2006) reviewed 83 bicondylar tibial plateau fractures that were treated with medial and lateral plate fixation through two exposures. They noted that residual dysfunction is common. Accurate articular reduction was possible in about 55% of the patients and the reduction was associated with better outcomes within the confines of the injury severity.
Figure A and B show a comminuted bicondylar tibial plateau fracture. Figure C
is an axial CT cut showing the medial fragments (anterior and posterior).
Incorrect Answers:
Answer 1: Definitive use of the spanning external fixator would lead to significant knee stiffness.
Answer 2: Conversion to a hinged knee fixator is not commonly recommended for this injury pattern.
Answer 3: This comminuted tibial plateau fracture is not amenable to treatment with an intramedullary nail.
Answer 4: Use of more than one plate to instrument this fracture is necessary.
Barei et al (2008) retrospectively reviewed 57 patients with bicondylar tibial plateau fractures, evaluating the frequency and morphologic characteristics of the posteromedial fragment in this injury pattern. They found that 74% of these injuries had a posteromedial fragment that may require alternate or supplementary fixation methods when managing this injury pattern.
Barei et al (2006) reviewed 83 bicondylar tibial plateau fractures that were treated with medial and lateral plate fixation through two exposures. They noted that residual dysfunction is common. Accurate articular reduction was possible in about 55% of the patients and the reduction was associated with better outcomes within the confines of the injury severity.
Figure A and B show a comminuted bicondylar tibial plateau fracture. Figure C
is an axial CT cut showing the medial fragments (anterior and posterior).
Incorrect Answers:
Answer 1: Definitive use of the spanning external fixator would lead to significant knee stiffness.
Answer 2: Conversion to a hinged knee fixator is not commonly recommended for this injury pattern.
Answer 3: This comminuted tibial plateau fracture is not amenable to treatment with an intramedullary nail.
Answer 4: Use of more than one plate to instrument this fracture is necessary.
Question 27High Yield
Primary treatment of thoracic outlet syndrome should include:
Explanation
Initial treatment of thoracic outlet syndrome is non-operative. Aggravating activities are modified and shoulder girdle strengthening is initiated. Surgery is considered for patients who have failed conservative therapy and suffer intractable pain, and for those who have significant neurologic or vascular deficits. Operative procedures must be tailored to the presumed pathological anatomy; there is no single best procedure.
Question 28High Yield
Figures 1 through 3 are the sagittal and axial CT scans and sagittal T2 MR image of a 21-year-old man who was thrown from his motocross bike earlier in the day. He now has significant low-back pain; however, he is neurologically intact and has no trouble voiding urine. A standing plain radiograph obtained the next day is shown in Figure

Explanation
■
Disruption of the posterior ligamentous complex is an important determinant of the stability of a burst fracture. This patient is neurologically intact and his MR images do not reveal posterior ligamentous complex (PLC) disruption. The standing radiograph confirms that overall alignment is acceptably and relatively preserved. Nonsurgical treatment with or without a brace is acceptable in this scenario; however, the patient should not be cleared to resume full activity until fracture healing, which may be as long as 3 months after the date of injury. Anterior or posterior surgery should be reserved for patients with PLC disruption, neurological injury, or, in some cases, multiple trauma.
Disruption of the posterior ligamentous complex is an important determinant of the stability of a burst fracture. This patient is neurologically intact and his MR images do not reveal posterior ligamentous complex (PLC) disruption. The standing radiograph confirms that overall alignment is acceptably and relatively preserved. Nonsurgical treatment with or without a brace is acceptable in this scenario; however, the patient should not be cleared to resume full activity until fracture healing, which may be as long as 3 months after the date of injury. Anterior or posterior surgery should be reserved for patients with PLC disruption, neurological injury, or, in some cases, multiple trauma.
Question 29High Yield
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years
ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic
feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 30High Yield
Figure 80a
Explanation
- Loose cemented stem_
Question 31High Yield
Residual angulation <30° of the humeral shaft after nonoperative fracture treatment has been shown to have what effect on patient reported outcomes?
Explanation
Acceptable angulation of humeral shaft fractures for nonoperative treatment is quite generous due to compensatory motion at the shoulder joint. Traditionally, 20° of anterior-posterior and 30° of varus-valgus angulation is acceptable. Indications for surgery have included angulation outside of this range, open fractures, brachial plexus injury, polytrauma, or other factors that preclude functional bracing. Increased amounts of angulation at the conclusion of healing can result in cosmetic dissatisfaction, but this has not been correlated with any specific degree of angulation, as patient factors are a strong influencer. Increased angulation has not been shown to affect functional outcomes within the angulation range previously described.
Question 32High Yield
Figures 1 and 2 are the radiographs of a 44-year-old man who comes to the
emergency department after a fall from a ladder with pain and a closed injury to his left shoulder. He undergoes open reduction internal fixation (ORIF) of his left proximal humerus fracture. A postoperative radiograph is shown in Figure
emergency department after a fall from a ladder with pain and a closed injury to his left shoulder. He undergoes open reduction internal fixation (ORIF) of his left proximal humerus fracture. A postoperative radiograph is shown in Figure


Explanation
The patient has a surgical neck fracture with medial calcar comminution. In patients where this cannot be anatomically reconstructed to provide cortical support, a fibular allograft can be used to prevent varus collapse. A “push” screw can be seen in Figure 3, which was used to medialize the graft into a biomechanically favorable position for this fracture pattern. Although the allograft theoretically provides the other benefits listed, they are not the primary indication for this injury.
Question 33High Yield
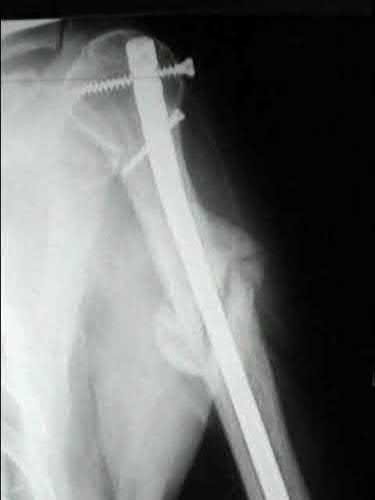
1246) A 42-year-old man reports persistent arm pain after undergoing intramedullary nailing of a humeral shaft fracture 13 months ago.
Physical exam shows near normal shoulder and elbow range-of-motion. Infection work-up is normal. A radiograph is shown in Figure
A. What is the next most appropriate step in treatment?
Physical exam shows near normal shoulder and elbow range-of-motion. Infection work-up is normal. A radiograph is shown in Figure
A. What is the next most appropriate step in treatment?
Explanation
Plate fixation (with bone graft as needed) is the procedure of choice for humeral shaft nonunions.
Rubel et al in a combined cadaveric and clinical study comparing one versus two plate constructs for humeral nonunions found that the two plate construct was significantly stiffer, but had no difference in healing rate compared with a single plate construct; 92% of the humeral shaft nonunion patients went onto union with rigid plate fixation.
Ring et al successfully treated a cohort of osteoporotic humeral shaft nonunions with locked plating. They
report 100% union rate with locking plate fixation of these humeral shaft nonunions, with use of autograft in >50% of their cases. Subjective shoulder scores were excellent or good in 22 of 24 patients.
Brinker and O'Connor analyzed the current available evidence for exchange nailing of nonunions and could not recommend this treatment for humeral shaft nonunions.
Rubel et al in a combined cadaveric and clinical study comparing one versus two plate constructs for humeral nonunions found that the two plate construct was significantly stiffer, but had no difference in healing rate compared with a single plate construct; 92% of the humeral shaft nonunion patients went onto union with rigid plate fixation.
Ring et al successfully treated a cohort of osteoporotic humeral shaft nonunions with locked plating. They
report 100% union rate with locking plate fixation of these humeral shaft nonunions, with use of autograft in >50% of their cases. Subjective shoulder scores were excellent or good in 22 of 24 patients.
Brinker and O'Connor analyzed the current available evidence for exchange nailing of nonunions and could not recommend this treatment for humeral shaft nonunions.
Question 34High Yield
Figure 1 is the MR arthrogram of a 24-year old professional baseball pitcher who complains of worsening right elbow pain and decreased pitch velocity over the past 2 months. He was initially managed with rest and forearm strengthening, but continues to complain of medial elbow pain during the long toss portion of his throwing program. What is the most appropriate treatment at this time?
Explanation
The MR arthrogram shows a rupture of the ulnar collateral ligament (UCL) from the ulnar insertion, with the classic T-sign of contrast extravasation. Medial UCL reconstruction, using either ipsilateral palmaris longus or allograft tendon, is
indicated for UCL injuries that fail nonsurgical management. Primary repair has been shown to be successful in select cases, but appropriate patient selection is essential. An arthroscopic elbow debridement would be indicated for early elbow arthritis or intra-articular loose body, which is not demonstrated here. An ulnar nerve decompression would be indicated in the setting of cubital tunnel syndrome, but this patient has no complaints of paresthesias.
40
indicated for UCL injuries that fail nonsurgical management. Primary repair has been shown to be successful in select cases, but appropriate patient selection is essential. An arthroscopic elbow debridement would be indicated for early elbow arthritis or intra-articular loose body, which is not demonstrated here. An ulnar nerve decompression would be indicated in the setting of cubital tunnel syndrome, but this patient has no complaints of paresthesias.
40
Question 35High Yield
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent?
Explanation
DISCUSSION: The supplement is creatine. Approximately 17% of high school athletes and about 30% of high school football players use creatine. Creatine is a protein synthesized in the liver and the kidney, circulates in the bloodstream, and is incorporated into muscle. Its use is associated with increased muscle mass, short-term improvement in sprinting, and may allow for increased anaerobic resistance performance. Caffeine and ephedrine are taken orally but do not increase muscle mass. Testosterone and human growth hormone are both associated with increased body mass but must be injected.
PREFERRED RESPONSE: 1
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
DISCUSSION: The supplement is creatine. Approximately 17% of high school athletes and about 30% of high school football players use creatine. Creatine is a protein synthesized in the liver and the kidney, circulates in the bloodstream, and is incorporated into muscle. Its use is associated with increased muscle mass, short-term improvement in sprinting, and may allow for increased anaerobic resistance performance. Caffeine and ephedrine are taken orally but do not increase muscle mass. Testosterone and human growth hormone are both associated with increased body mass but must be injected.
PREFERRED RESPONSE: 1
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
Question 36High Yield
A patient sustained a puncture wound to the plantar aspect of his foot. He was wearing shoes and socks at the time of the injury. Systemic antibiotic administration with specific coverage for which bacterial species (in addition to Staphylococcus aureus) should be instituted?
Explanation
Puncture wounds sustained through a shoe and sock increase risk for Pseudomonas infection. Clostridium are associated with soil-contaminated wounds. Mycobacterium marinum is associated with injuries sustained within water.
RECOMMENDED READINGS
[DeCoster TA, Miller RA. Management of Traumatic Foot Wounds. J Am Acad Orthop Surg. 1994 Jul;2(4):226-230. PubMed PMID: 10709013. ](http://www.ncbi.nlm.nih.gov/pubmed/10709013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10709013)
Raikin SM. Common infections of the foot. In: Richardson EG, ed. Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004:199-205.
RECOMMENDED READINGS
[DeCoster TA, Miller RA. Management of Traumatic Foot Wounds. J Am Acad Orthop Surg. 1994 Jul;2(4):226-230. PubMed PMID: 10709013. ](http://www.ncbi.nlm.nih.gov/pubmed/10709013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10709013)
Raikin SM. Common infections of the foot. In: Richardson EG, ed. Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004:199-205.
Question 37High Yield
A 12-year-old boy is diagnosed with osteomyelitis and subperiosteal abscess of the distal tibia demonstrated on the MRI. CRP is 13 mg/l. He is taken to the operating room (OR) for incision and drainage. Intraoperative cultures as well as blood cultures grow methicillin-resistant Staphylococcus aureus (MRSA). On postoperative day 2, he develops swelling in the leg, as well as an increased oxygen requirement. What should be the next step in evaluation?
Explanation
■
This child has a MRSA osteomyelitis. Many recent studies have shown that these infections are more difficult to treat and are associated with severe complications and longer hospitalizations. They may also require an increased number of surgical procedures to get control of the infection source. Deep venous thrombosis (DVT) and pulmonary embolism, as well as septic emboli to the lungs occur more commonly with MRSA infections. Increased swelling of the leg may be related to the onset of a DVT and venous ultrasonography is an easy and quick study to help determine if a DVT is present. Currently, the patient has an increased oxygen requirement. Helical CT scan is the next best test to evaluate for septic pulmonary emboli. Plain radiograph of the chest is helpful to look for areas of pneumonia but not diagnostic for septic emboli. Repeat MRI of the leg will be abnormal because of the recent surgical procedure and most likely will not add anything diagnostically. Given his clinical improvement and decreasing CRP, a repeat return to the OR is not indicated at this time, although it is not uncommon for children with MRSA infections to require more than one surgical procedure.
This child has a MRSA osteomyelitis. Many recent studies have shown that these infections are more difficult to treat and are associated with severe complications and longer hospitalizations. They may also require an increased number of surgical procedures to get control of the infection source. Deep venous thrombosis (DVT) and pulmonary embolism, as well as septic emboli to the lungs occur more commonly with MRSA infections. Increased swelling of the leg may be related to the onset of a DVT and venous ultrasonography is an easy and quick study to help determine if a DVT is present. Currently, the patient has an increased oxygen requirement. Helical CT scan is the next best test to evaluate for septic pulmonary emboli. Plain radiograph of the chest is helpful to look for areas of pneumonia but not diagnostic for septic emboli. Repeat MRI of the leg will be abnormal because of the recent surgical procedure and most likely will not add anything diagnostically. Given his clinical improvement and decreasing CRP, a repeat return to the OR is not indicated at this time, although it is not uncommon for children with MRSA infections to require more than one surgical procedure.
Question 38High Yield
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?
Explanation
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a “dripping candle wax” appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the “smoke up chimney” appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal.
REFERENCES: Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Kawabata H, Tsuyuguchi Y, Kawai H, et al: Melorheostosis of the upper limb: A report of two cases. J Hand Surg Am 1984;9:871-876.
REFERENCES: Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Kawabata H, Tsuyuguchi Y, Kawai H, et al: Melorheostosis of the upper limb: A report of two cases. J Hand Surg Am 1984;9:871-876.
Question 39High Yield
What is the most cost-effective implant indicated for the injury shown in Figures A and B, assuming the hospital purchases the implants at-cost from the manufacturer?



Explanation
In the intertrochanteric hip fracture displayed, a sliding hip screw (SHS) or cephalomedullary nail (CMN) would be indicated; the SHS is the cheaper implant.
In a standard obliquity intertrochanteric fracture without lateral wall comminution, an SHS is a cost-effective option. In reverse obliquity fractures or those with lateral wall comminution (unstable), there is an increased failure rate with this implant and an CMN should be considered. There is some controversy in terms of short and intermediate nail indications, which are attractive because they do not require reaming. SHS implants are contraindicated in subtrochanteric fractures. Although some hospitals receive discounts on implants, in general, intramedullary nail options are more expensive than SHS.
Swart et al. examined the cost-effectiveness of different fixation options for intertrochanteric hip fractures. They compared SHS and CMN implants using an expected-value decision-analysis model, taking into account fracture patterns, failure rates, and revision costs. In their study, the average cost of a SHS was
$2,000 compared to $3,200 for a standard CMN. They concluded that the SHS was likely more cost-effective for stable and questionably stable fractures compared to CMN fixation; CMN was more cost-effective for reverse obliquity patterns.
Kaplan et al. provided a review article on the surgical management of intertrochanteric fractures. Factors to determine treatment should include the patient's medical co-morbidities, pre-existing arthritis, bone quality, and fracture morphology. Their study did not find an appreciable difference in patient outcomes using either CMN or SHS for stable intertrochanteric fractures; surgeon experience and implant costs should, therefore, drive the decision making process for implant selection.
Figures A and B are AP and lateral right hip radiographs, respectively, demonstrating a standard obliquity intertrochanteric hip fracture. Illustration A is an AP post-operative radiograph showing a hip fracture treated with a SHS.
Incorrect Answers:
Answers 1 and 2: Both of these options are appropriate for this fracture but more costly than a SHS.
Answer 4: Arthroplasty is not indicated for this patient with an intertrochanteric fracture and preserved joint space.
Answer 5: Cannulated screws are not indicated for an intertrochanteric fracture.
In a standard obliquity intertrochanteric fracture without lateral wall comminution, an SHS is a cost-effective option. In reverse obliquity fractures or those with lateral wall comminution (unstable), there is an increased failure rate with this implant and an CMN should be considered. There is some controversy in terms of short and intermediate nail indications, which are attractive because they do not require reaming. SHS implants are contraindicated in subtrochanteric fractures. Although some hospitals receive discounts on implants, in general, intramedullary nail options are more expensive than SHS.
Swart et al. examined the cost-effectiveness of different fixation options for intertrochanteric hip fractures. They compared SHS and CMN implants using an expected-value decision-analysis model, taking into account fracture patterns, failure rates, and revision costs. In their study, the average cost of a SHS was
$2,000 compared to $3,200 for a standard CMN. They concluded that the SHS was likely more cost-effective for stable and questionably stable fractures compared to CMN fixation; CMN was more cost-effective for reverse obliquity patterns.
Kaplan et al. provided a review article on the surgical management of intertrochanteric fractures. Factors to determine treatment should include the patient's medical co-morbidities, pre-existing arthritis, bone quality, and fracture morphology. Their study did not find an appreciable difference in patient outcomes using either CMN or SHS for stable intertrochanteric fractures; surgeon experience and implant costs should, therefore, drive the decision making process for implant selection.
Figures A and B are AP and lateral right hip radiographs, respectively, demonstrating a standard obliquity intertrochanteric hip fracture. Illustration A is an AP post-operative radiograph showing a hip fracture treated with a SHS.
Incorrect Answers:
Answers 1 and 2: Both of these options are appropriate for this fracture but more costly than a SHS.
Answer 4: Arthroplasty is not indicated for this patient with an intertrochanteric fracture and preserved joint space.
Answer 5: Cannulated screws are not indicated for an intertrochanteric fracture.
Question 40High Yield
What is the most common cause of reoperation following contemporary hip resurfacing for degenerative coxarthrosis?
Explanation
DISCUSSION: Femoral neck fracture, necessitating revision surgery to a total hip arthroplasty, is the most likely common early complication after hip resurfacing. Cortical notching, varus positioning, and other technical variables appear to predispose to this complication. Limb lengths do not change appreciably after hip resurfacing; the same applies to femoral offset. Hip movement is not limited by hip resurfacing, and there is no evidence that psoas tendon impingement is increased by hip resurfacing.
REFERENCES: Steffen RT, Pandit HP, Palan J, et al: The five-year results of the Birmingham Hip Resurfacing arthroplasty: An independent series. J Bone Joint Surg Br 2008;90:436-441.
Amstutz HC: Present state of metal-on-metal hybrid hip resurfacing. J Surg Orthop Adv 2008;17:12-16.
REFERENCES: Steffen RT, Pandit HP, Palan J, et al: The five-year results of the Birmingham Hip Resurfacing arthroplasty: An independent series. J Bone Joint Surg Br 2008;90:436-441.
Amstutz HC: Present state of metal-on-metal hybrid hip resurfacing. J Surg Orthop Adv 2008;17:12-16.
Question 41High Yield
A 20-year-old elite college football player has ecchymosis, swelling, and pain on the lateral side of his foot after a game. Radiographs are shown in Figures 31a through 31c. Management should consist of
Explanation
Metaphyseal-diaphyseal junction fractures of the fifth metatarsal require careful evaluation. In athletes, early intervention with a 4.5-mm intramedullary screw correlates with an earlier return to activity. One study examining the failure of surgically managed Jones fractures revealed that use of anything other than a 4.5-mm malleolar screw for internal fixation correlated with failure.
REFERENCES: Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-252.
REFERENCES: Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-252.
Question 42High Yield
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
The PCL is a nonisometric structure with nonuniform tension during knee motion, with maximum tension at 90° of flexion. While the posteromedial PCL fibers have been found to be the most isometric, the anterolateral fibers represent the bulk of the ligament. Studies have suggested that anterior placement of the femoral tunnel is superior to placement in an isometric position. The anterolateral bundle tightens as the knee flexes; therefore, it is optimal to tension the graft at 90° of flexion.
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
Question 43High Yield
A 77-year-old man with a history of mild renal insufficiency and atrial fibrillation on warfarin therapy is scheduled to undergo a left total hip arthroplasty. He previously underwent a right total hip arthroplasty with development of significant heterotopic bone that resulted in limitation of motion. What is the most appropriate form of prophylactic treatment to minimize the formation of heterotopic bone on his left hip?

Explanation
DISCUSSION: This question centers on the prophylactic treatment to reduce the risk of heterotopic bone formation. Prophylaxis is indicated because he has already demonstrated bone formation with his prior hip arthroplasty, which places him at increased risk for developing heterotopic bone on the contralateral side. He is on warfarin and has renal insufficiency, which makes the use of NSAIDs contraindicated. The recommended dose is 600 to 800 centigrey of radiation given within 24 hours of surgery preoperatively or 72 hours postoperatively.
REFERENCES: Kolbl O, Knelles D, Barthel T, et al: Preoperative irradiation versus the use of nonsteroidal anti-inflammatory drugs for prevention of heterotopic ossification following total hip replacement: The results of a randomized trial. Int J Radiat Oncol Biol Phys 1998;42:397-401.
Pakos EE, Ioannidis JP: Radiotherapy vs nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip surgery: A meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys 2004;60:888-895.
Seegenschmiedt MH, Makoski HB, Micke O, et al: Radiation prophylaxis for heterotopic ossification about the hip joint: A multicenter study. Int J Radiat Oncol Biol Phys 2001 ;51:756-765.
Figure 23 a Figure 23b
DISCUSSION: This question centers on the prophylactic treatment to reduce the risk of heterotopic bone formation. Prophylaxis is indicated because he has already demonstrated bone formation with his prior hip arthroplasty, which places him at increased risk for developing heterotopic bone on the contralateral side. He is on warfarin and has renal insufficiency, which makes the use of NSAIDs contraindicated. The recommended dose is 600 to 800 centigrey of radiation given within 24 hours of surgery preoperatively or 72 hours postoperatively.
REFERENCES: Kolbl O, Knelles D, Barthel T, et al: Preoperative irradiation versus the use of nonsteroidal anti-inflammatory drugs for prevention of heterotopic ossification following total hip replacement: The results of a randomized trial. Int J Radiat Oncol Biol Phys 1998;42:397-401.
Pakos EE, Ioannidis JP: Radiotherapy vs nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip surgery: A meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys 2004;60:888-895.
Seegenschmiedt MH, Makoski HB, Micke O, et al: Radiation prophylaxis for heterotopic ossification about the hip joint: A multicenter study. Int J Radiat Oncol Biol Phys 2001 ;51:756-765.
Figure 23 a Figure 23b
Question 44High Yield
A 36-year-old woman presents with a grade 3 open midshaft femoral shaft fracture as the result of a high-speed motor vehicle collision. Concomitant injuries include a high-grade splenic laceration requiring splenectomy as well as a subdural hematoma that requires monitoring and maintenance of cerebral perfusion pressure. After irrigation and debridement of the open fracture, which of the following is the most appropriate management of the femoral shaft fracture at this time?
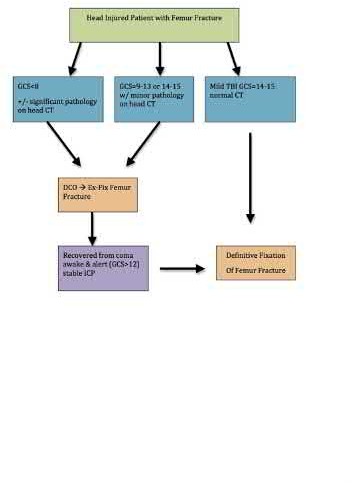
Explanation
The clinical scenario is consistent with a femoral shaft fracture in a patient that is not stable from a neurosurgical perspective. Therefore, the most appropriate treatment at this time is placement of an external fixator.
When evaluating polytrauma patients with long bone fractures, timing of surgery must be approached considering all clinical conditions. One factor most likely to adversely affect long term outcome in polytrauma patients with severe brain injury is intra-operative hypotension; therefore, whenever a patient has a subdural hematoma that requires close observation, definitive surgery of long bone fractures should be delayed.
Flierl et al. review the immunopathophysiology of traumatic brain injury and the role of the orthopaedic surgeon in avoiding a "second hit" injury to the brain by appropriately timing the fixation of femoral shaft fractures. They recommend a multidisciplinary approach, taking individual patient-specific factors into consideration and in general, DCO principles for severe head-injured patients (GCS 3-13) and "early total care" principles for patients with mild head injury (GCS 14-15).
Illustration A is a visual representation of the treatment algorithm recommended in the article.
Incorrect Answers:
Answer choice 1 is incorrect because it does not appropriately address the fracture and there is no indication for bead placement.
Answer choices 2 and 3 are incorrect as this patient is not stable for prolonged surgery.
Answer 4 is incorrect as this patient is already under general anesthesia and external fixation is a better option than traction for stabilization of the fracture.
When evaluating polytrauma patients with long bone fractures, timing of surgery must be approached considering all clinical conditions. One factor most likely to adversely affect long term outcome in polytrauma patients with severe brain injury is intra-operative hypotension; therefore, whenever a patient has a subdural hematoma that requires close observation, definitive surgery of long bone fractures should be delayed.
Flierl et al. review the immunopathophysiology of traumatic brain injury and the role of the orthopaedic surgeon in avoiding a "second hit" injury to the brain by appropriately timing the fixation of femoral shaft fractures. They recommend a multidisciplinary approach, taking individual patient-specific factors into consideration and in general, DCO principles for severe head-injured patients (GCS 3-13) and "early total care" principles for patients with mild head injury (GCS 14-15).
Illustration A is a visual representation of the treatment algorithm recommended in the article.
Incorrect Answers:
Answer choice 1 is incorrect because it does not appropriately address the fracture and there is no indication for bead placement.
Answer choices 2 and 3 are incorrect as this patient is not stable for prolonged surgery.
Answer 4 is incorrect as this patient is already under general anesthesia and external fixation is a better option than traction for stabilization of the fracture.
Question 45High Yield
A 25-year-old female presents to the emergency room for the fourth time in the last week. She has vague complaints of extremity pain. Physical examination by a male ER resident has been limited each visit because she is terrified of the pain that the clinician may cause. On physical examination, she is withdrawn and frightened.
Regions of ecchymosis are noted throughout chest and abdomen. She has requested multiple radiographs, MRI and CT scans. Today's imaging (radiographs, MRI, CT scan) has been unrevealing. What is the most likely diagnosis?
Regions of ecchymosis are noted throughout chest and abdomen. She has requested multiple radiographs, MRI and CT scans. Today's imaging (radiographs, MRI, CT scan) has been unrevealing. What is the most likely diagnosis?
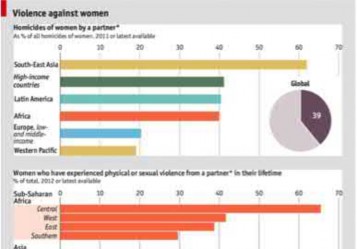
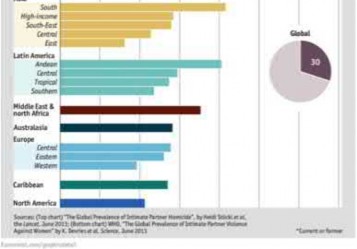
Explanation
Based on the history and clinical presentation, the most likely diagnosis is intimate partner violence.
Domestic violence or intimate partner violence can be in the form of mental or physical abuse, neglect or abandonment. Close to 25% of women will experience domestic violence. Risk factors include young age (19-29 years of age), females, pregnancy and lower socioeconomic status. Affected patients will have repeated visits to the emergency room, find reasons to stay in a treatment facility for an extended period of time and constantly seek approval
of their partner.
Shields et al. reviewed factors influence outcome in treatment of patients affected by domestic violence. They found that positive outcomes were associated with interdisciplinary approaches to management. This included better history assessment, providing written documentation regarding intervention and better access to information on community resources.
Illustration A is a chart documenting the frequency of female domestic violence throughout the world as of 2012.
Incorrect Answers
Answers 1, 2, 3, 5: These conditions are not consistent with this patient’s history.
Domestic violence or intimate partner violence can be in the form of mental or physical abuse, neglect or abandonment. Close to 25% of women will experience domestic violence. Risk factors include young age (19-29 years of age), females, pregnancy and lower socioeconomic status. Affected patients will have repeated visits to the emergency room, find reasons to stay in a treatment facility for an extended period of time and constantly seek approval
of their partner.
Shields et al. reviewed factors influence outcome in treatment of patients affected by domestic violence. They found that positive outcomes were associated with interdisciplinary approaches to management. This included better history assessment, providing written documentation regarding intervention and better access to information on community resources.
Illustration A is a chart documenting the frequency of female domestic violence throughout the world as of 2012.
Incorrect Answers
Answers 1, 2, 3, 5: These conditions are not consistent with this patient’s history.
Question 46High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---



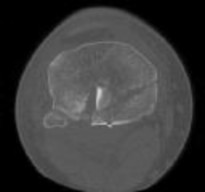
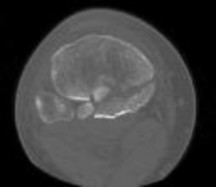





Explanation
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the
femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 47High Yield
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management?
---
---

Explanation
The patient has an L5-S1 disk herniation, which has a favorable prognosis without surgical intervention. Most acute lumbar disk herniations resolve with nonsurgical management. The most appropriate course of initial treatment should be analgesics and activity modification, followed by rehabilitation as the symptoms allow. Although the MRI scan indicates a large disk herniation, he has no symptoms or signs that
would warrant urgent surgical decompression. Planned elective discectomy should be considered only if nonsurgical management fails to provide relief. Epidural injections could be considered if the initial course of treatment fails to give the patient significant relief. Posterior laminectomy and fusion is not indicated without the presence of instability.
would warrant urgent surgical decompression. Planned elective discectomy should be considered only if nonsurgical management fails to provide relief. Epidural injections could be considered if the initial course of treatment fails to give the patient significant relief. Posterior laminectomy and fusion is not indicated without the presence of instability.
Question 48High Yield
A right-hand dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
Explanation
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on the radial tuberosity.
41
41
Question 49High Yield
A 68-year-old woman undergoes a hemiarthroplasty for a proximal humerus fracture through a deltopectoral approach. What
range of motion exercise should not be utilized in the immediate postoperative period due to concerns about lesser tuberosity fixation?
range of motion exercise should not be utilized in the immediate postoperative period due to concerns about lesser tuberosity fixation?
Explanation
Frankle et al found that passive external rotation of the shoulder placed the most stress on the lesser tuberosity fixation. The subscapularis tendon inserts on the lesser tuberosity and is the deforming force when placed under tension during external rotation. They also found that non-anatomic tuberosity reduction of 4-part proximal humerus fractures treated with hemiarthroplasty increased torque and impaired external rotation kinematics.
Question 50High Yield
What is the preferred treatment for a type CperiprosthetiCfracture with a well-fixed humeral component:
Explanation
In patients with a type CperiprosthetiCfracture (distal to the tip of the prosthesis) and a well-fixed humeral component, the injury can be treated similar to a closed humerus fracture
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon