Free Orthopedics Review | Dr Hutaif General Orthopedics -...
14 Apr 2026
196 min read
74 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Free Orthopedics Review | Dr Hutaif General O...
00:00
Start Quiz
Question 1High Yield
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. Risk for vascular injury during transtibial drilling for reconstruction of this injury is increased by
---
---

Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases,
the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
Question 2High Yield
For patients who sustain their first anterior glenohumeral dislocation during sports activity, which associated injury is most commonly expected at the time of the initial dislocation?
Explanation
- Axillary nerve palsy_
Question 3High Yield
The most common complication following triple arthrodesis in the adult patient is:
Explanation
Each of the possible answers may occur following triple arthrodesis. In numerous studies, ankle arthritis is the complication most likely to occur regardless of the underlying disease process.
Question 4High Yield
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The most likely complication in this child is:
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The most likely complication in this child is:
Explanation
Ulnar carpal translocation occurs due to the steep radial articular angulation that occurs due to the tethering effect of a shortened ulna and is already apparent in early stages in the first radiograph. While peroneal palsy is possible due to a proximal fibula lesion, it is less common. Malignant transformation occurs, risk varies with families.
Question 5High Yield
Figure 1 is the radiograph of a 6-year-old boy who falls off a tire swing and sustains an isolated left femur fracture that is treated with submuscular plating (Figure 2). He went on to uneventful union and full return to activity without disability. Recommendations should include

Explanation
■
Submuscular plating of pediatric femur fractures is a reliable technique for length in unstable fractures in the 5- to 10-year-old age group. Several reports have demonstrated a propensity for late valgus development with a contoured lateral plate adjacent to the distal femoral physis and recommend for routine implant removal following fracture union and remodeling prior to development of this sequelae, rather than observation and additional treatment once it occurs. This fracture carries no significant risk of avascular necrosis; thus, future arthroplasty is not relevant to this decision making. Activity restriction is recommended for 4 to 6 weeks following implant removal to minimize the risk of pathologic fracture through a screw hole.
■
Submuscular plating of pediatric femur fractures is a reliable technique for length in unstable fractures in the 5- to 10-year-old age group. Several reports have demonstrated a propensity for late valgus development with a contoured lateral plate adjacent to the distal femoral physis and recommend for routine implant removal following fracture union and remodeling prior to development of this sequelae, rather than observation and additional treatment once it occurs. This fracture carries no significant risk of avascular necrosis; thus, future arthroplasty is not relevant to this decision making. Activity restriction is recommended for 4 to 6 weeks following implant removal to minimize the risk of pathologic fracture through a screw hole.
Question 6High Yield
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?**
Explanation
Medial clavicle excision alone can be associated with postoperative instability of the clavicle. The clavicle should be stabilized to the first rib by reconstructing the costoclavicular ligament if it is torn or if the resection is lateral to its clavicular insertion. Therefore, care must be taken to resect only that part of the clavicle that is medial to the costoclavicular ligament. Adequate protection for vital structures that lie posterior to the medial end of the clavicle must be provided.
REFERENCES: Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 583-586.
REFERENCES: Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 583-586.
Question 7High Yield
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable.
---
---
Which of the four muscles of the rotator cuff provides the most resistance to this patient's direction of instability?
---
---
Which of the four muscles of the rotator cuff provides the most resistance to this patient's direction of instability?


Explanation
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through, as seen in this patient. The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion, at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The four muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the four rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation. This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Beighton sign findings would be negative), a posterior capsular shift with rotator interval closure is
indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate.
indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate.
Question 8High Yield
Figures 1 through 5 are the radiographs and MRI scans of an 80-year-old woman who had a total hip arthroplasty (THA) 10 years ago and recently experienced an episode of dislocation that was reduced. She currently has no pain, but has a limp and moderate apprehension. Her erythrocyte sedimentation rate is 32 and C-reactive protein is 34. Her cobalt level is 32.8 ug/L (normal <1ug/L) and chromium level 14 ug/L (normal < 5ug/L). The hip aspiration is negative. What is the most appropriate treatment? 35
Explanation
36
The patient has a metal-on-metal articulation with pseudotumor, causing instability and destruction of the abductors. Although inflammatory markers are elevated, this may occur with adverse local soft-tissue reaction, and aspiration may be necessary to rule out infection. Conversion to a polyethylene articulation is necessary to prevent ongoing damage. The MRI scan reveals compromise of abductors by the pseudotumor, but sparing of the gluteus maximus.This facilitates abductor reconstruction to address the limp and improve stability.
The patient has a metal-on-metal articulation with pseudotumor, causing instability and destruction of the abductors. Although inflammatory markers are elevated, this may occur with adverse local soft-tissue reaction, and aspiration may be necessary to rule out infection. Conversion to a polyethylene articulation is necessary to prevent ongoing damage. The MRI scan reveals compromise of abductors by the pseudotumor, but sparing of the gluteus maximus.This facilitates abductor reconstruction to address the limp and improve stability.
Question 9High Yield
Figure 22 shows the radiographs of a 16-year-old boy who injured his elbow in a fall 1 year ago. Although he has no pain, he reports restricted forearm rotation and elbow flexion. What is the most likely diagnosis?
Explanation
Congenital dislocation of the radial head is often confused with posttraumatic dislocation. The distinguishing feature here is the dome-shaped radial head. Some patients with congenital anomalies fail to recognize their limitations until an injury occurs. Soft-tissue contractures do not cause radial head dislocation nor do they usually cause this pattern of motion restriction (mainly flexion and rotation without significant loss of extension). There is no deformity of the ulna to suggest an old Monteggia lesion.
REFERENCES: Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Bell SN, Morrey BF, Bianco AJ Jr: Chronic posterior subluxation and dislocation of the radial head. J Bone Joint Surg Am 1991;73:392-396.
REFERENCES: Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Bell SN, Morrey BF, Bianco AJ Jr: Chronic posterior subluxation and dislocation of the radial head. J Bone Joint Surg Am 1991;73:392-396.
Question 10High Yield
A 24-year-old male sustains the injury seen in Figure A after being thrown from a motorcycle at a high speed. Which of the following fixation methods has been shown to be the most stable fixation construct for this injury?

Explanation
Figure A shows an APC III injury, which is a rotationally and vertically unstable injury, with damage to the anterior ring, pelvic floor, and posterior ligamentous stabilizing structures.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
Question 11High Yield
A positive straight leg raising sign is when pain radiates distal to the knee when the affected leg is passively elevated. The increased tension generally occurs between

Explanation
A positive straight leg raising sign causes pain radiating distal to the knee when the nerve is under tension. This increased tension generally occurs between 30 degrees and 70 degrees of passive elevation.
---
---
Question 12High Yield
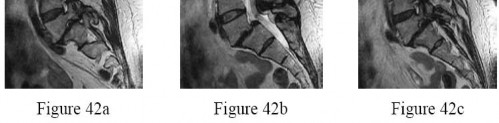
Figure 1
A 14-year-old boy presents for treatment of a painful foot, which has been present for 2 years. He has limited his athletic activities. He has similar symptoms in the opposite foot, although not as severe. On clinical examination, the alignment and appearance of the foot are normal; motion of the foot and ankle is good; and some discomfort is present in the sinus tarsi. Standard radiographs, of which the lateral view is presented, include anteroposterior, lateral, and oblique views. Because the diagnosis is unclear, more imaging studies are required. The next study to obtain is:
A 14-year-old boy presents for treatment of a painful foot, which has been present for 2 years. He has limited his athletic activities. He has similar symptoms in the opposite foot, although not as severe. On clinical examination, the alignment and appearance of the foot are normal; motion of the foot and ankle is good; and some discomfort is present in the sinus tarsi. Standard radiographs, of which the lateral view is presented, include anteroposterior, lateral, and oblique views. Because the diagnosis is unclear, more imaging studies are required. The next study to obtain is:
Explanation
The radiograph demonstrates changes in the subtalar joint suggestive of a middle facet coalition. Note the sclerosis of the joint surface. Although a computed axial tomography scan may be helpful, standard axial views of the subtalar joint (Harris) taken in the plane of the joint are usually diagnostic of tarsal coalition. Motion of the subtalar joint may be normal in the adolescent with a tarsal coalition.
Question 13High Yield
A 27-year-old male athlete presents with a 2-month history of pain along the posteromedial ankle. Swelling is present posteriomedially. The pain is exacerbated with resisted plantarflexion and inversion of the foot. This condition is likely to be associated with:
Explanation
The presence of posterior tibial tendonitis in a young individual should raise the concern for seronegative arthritis. Although a stress fracture of the medial malleolus may be present, pain is not exacerbated with resisted inversion.
Question 14High Yield
Which of the following statements is true regarding metaphyseal cortical bone formation in a child with open physes:
Explanation
Cadet and colleagues studied the formation of cortical bone in the metaphyses of rabbits. They found that the metaphyseal cortical bone is formed by coalescence of enchondral trabecular bone.
Important points from this study include:
Metaphyseal cortical bone is formed by coalescence of enchondral trabecular bone. The coalescence is formed by an increased osteoblast surface.
The increased osteoblast surface is likely caused by factors from the periosteum.
The bone that is produced by the cells in the groove of Ranvier probably does not contribute to the metaphyseal cortical bone.
Important points from this study include:
Metaphyseal cortical bone is formed by coalescence of enchondral trabecular bone. The coalescence is formed by an increased osteoblast surface.
The increased osteoblast surface is likely caused by factors from the periosteum.
The bone that is produced by the cells in the groove of Ranvier probably does not contribute to the metaphyseal cortical bone.
Question 15High Yield
A 42-year-old male who works as a professional clown presents with severe ankle pain and gross deformity after tripping and falling over his props at a children’s birthday party. His radiograph is shown in Figure A. Following fixation of the medial and lateral malleolar fractures, the syndesmosis is assessed and is found to be persistently unstable. All of the following are true regarding posterior malleolar fixation EXCEPT:

Explanation
Fixation of the posterior malleolus has been shown to be biomechanically superior to single-screw trans-articular syndesmotic fixation. Anatomic reduction and fixation will most often obviate the need for syndesmotic fixation, as the posterior inferior tibiofibular ligament (PITFL) is typically intact and attached to the fragment.
Posterior malleolar integrity is essential to ankle function and stability. The posterior malleolus not only contains the talus posteriorly but adds to articular congruity for tibiotalar load transfer and contributes to rotatory ankle stability through the PITFL. As a result, posterior malleolar fractures compromise these critical functions. Operative management is therefore aimed at containment of
the talus, restoration of articular congruity, reduction of the incisura, and restoring integrity to the syndesmosis. Functional and radiographic outcomes following posterior malleolar fixation have been shown to be at least equivalent to those following syndesmotic fixation.
Miller et al. compared the need for syndesmotic fixation in bi- and tri-malleolar ankle fractures following anatomic reduction and fixation in the prone position versus initial conservative management in the supine position. The authors found that fixation of the posterior malleolus obviated the need for syndesmotic fixation in 97.9% of cases, while nearly 25% of patients with no initial fixation required stabilization. They concluded that prone positioning and anatomic fixation of the posterior malleolus should be performed as this adequately restored syndesmotic stability in almost all cases.
Gardner et al. performed a radiographic evaluation of syndesmotic integrity in the setting of pronation-external rotation stage 4 ankle fractures with associated posterior malleolar fractures. Based on radiographs and MRI, no complete tears of the posterior-inferior tibiofibular ligament were evident. The fracture pattern was then simulated in cadavers, and posterior malleolar fixation restored 70% of the native stability while syndesmotic fixation alone restored only 40% of the native stability. The authors advocated for posterior malleolar fixation over syndesmotic stabilization.
Miller et al. prospectively compared the outcomes following posterior malleolar and syndesmotic fixation for unstable ankle fractures with partial syndesmotic injury. At a minimum one-year follow-up, the authors found that patients who had undergone open reduction with fixation of posterior malleolar fractures had no difference in outcomes as compared to those who underwent syndesmotic fixation. They concluded that not only was syndesmotic reduction maintained at final follow-up following posterior malleolar fixation, but that functional outcomes were at least equivalent to syndesmotic fixation.
Fitzpatrick et al. evaluated the impact of posterior malleolar fixation toward restoring syndesmotic stability in a cadaveric supination-external rotation stage 4 fracture model. The authors found that failure to fix or anatomically reduce posterior malleolar fragments resulted in non-anatomic translation of the fibula and ultimately in syndesmotic malreduction. They advocated for anatomic reduction and fixation of larger posterior malleolar fractures.
Figure A is an AP radiograph of the right ankle demonstrating a displaced trimalleolar ankle fracture with maintained relationship between the distal fibula and posterior malleolar fragment.
Incorrect Answers:
Answer 1: Fixation of the posterior malleolus has been shown to adequately restore syndesmotic stability and obviate the need for additional trans-articular syndesmotic screw fixation in the majority of cases.
Answer 3: Studies comparing clinical and functional outcomes following posterior malleolar and syndesmotic fixation have shown equivalent results with improved maintenance of radiographic syndesmotic reduction following posterior malleolar fixation.
Answer 4: Non-anatomic fixation of both small and large posterior malleolar fragments has been shown to compromise syndesmotic integrity and anatomic syndesmotic reduction.
Answer 5: Radiographic studies evaluating syndesmotic integrity via MRI have shown the PITFL to be completely intact or only partially injured in most cases.
Posterior malleolar integrity is essential to ankle function and stability. The posterior malleolus not only contains the talus posteriorly but adds to articular congruity for tibiotalar load transfer and contributes to rotatory ankle stability through the PITFL. As a result, posterior malleolar fractures compromise these critical functions. Operative management is therefore aimed at containment of
the talus, restoration of articular congruity, reduction of the incisura, and restoring integrity to the syndesmosis. Functional and radiographic outcomes following posterior malleolar fixation have been shown to be at least equivalent to those following syndesmotic fixation.
Miller et al. compared the need for syndesmotic fixation in bi- and tri-malleolar ankle fractures following anatomic reduction and fixation in the prone position versus initial conservative management in the supine position. The authors found that fixation of the posterior malleolus obviated the need for syndesmotic fixation in 97.9% of cases, while nearly 25% of patients with no initial fixation required stabilization. They concluded that prone positioning and anatomic fixation of the posterior malleolus should be performed as this adequately restored syndesmotic stability in almost all cases.
Gardner et al. performed a radiographic evaluation of syndesmotic integrity in the setting of pronation-external rotation stage 4 ankle fractures with associated posterior malleolar fractures. Based on radiographs and MRI, no complete tears of the posterior-inferior tibiofibular ligament were evident. The fracture pattern was then simulated in cadavers, and posterior malleolar fixation restored 70% of the native stability while syndesmotic fixation alone restored only 40% of the native stability. The authors advocated for posterior malleolar fixation over syndesmotic stabilization.
Miller et al. prospectively compared the outcomes following posterior malleolar and syndesmotic fixation for unstable ankle fractures with partial syndesmotic injury. At a minimum one-year follow-up, the authors found that patients who had undergone open reduction with fixation of posterior malleolar fractures had no difference in outcomes as compared to those who underwent syndesmotic fixation. They concluded that not only was syndesmotic reduction maintained at final follow-up following posterior malleolar fixation, but that functional outcomes were at least equivalent to syndesmotic fixation.
Fitzpatrick et al. evaluated the impact of posterior malleolar fixation toward restoring syndesmotic stability in a cadaveric supination-external rotation stage 4 fracture model. The authors found that failure to fix or anatomically reduce posterior malleolar fragments resulted in non-anatomic translation of the fibula and ultimately in syndesmotic malreduction. They advocated for anatomic reduction and fixation of larger posterior malleolar fractures.
Figure A is an AP radiograph of the right ankle demonstrating a displaced trimalleolar ankle fracture with maintained relationship between the distal fibula and posterior malleolar fragment.
Incorrect Answers:
Answer 1: Fixation of the posterior malleolus has been shown to adequately restore syndesmotic stability and obviate the need for additional trans-articular syndesmotic screw fixation in the majority of cases.
Answer 3: Studies comparing clinical and functional outcomes following posterior malleolar and syndesmotic fixation have shown equivalent results with improved maintenance of radiographic syndesmotic reduction following posterior malleolar fixation.
Answer 4: Non-anatomic fixation of both small and large posterior malleolar fragments has been shown to compromise syndesmotic integrity and anatomic syndesmotic reduction.
Answer 5: Radiographic studies evaluating syndesmotic integrity via MRI have shown the PITFL to be completely intact or only partially injured in most cases.
Question 16High Yield
When performing an ulnar nerve decompression at the elbow, the surgeon must be aware of the
Explanation
The medial antebrachial cutaneous and medial brachial cutaneous are nerves that can be injured during ulnar nerve decompression at the elbow. The medial antebrachial cutaneous nerve crosses the surgical field at an average of 3.1 cm distal to the medial epicondyle. The medial brachial cutaneous nerve crosses the field 7 cm proximal to the medial epicondyle and arborizes into two to three terminal branches. Because the surgical approach involves dissection on the medial side, the posterior antebrachial cutaneous nerve is distant from the exposure. Although the median nerve potentially can be located in the deep dissection of a submuscular transposition, it is considered distant to an in situ decompression.
Question 17High Yield
Figure 92
Explanation
- Infantile vascular interruption
Question 18High Yield
Which treatment factor associated with the acute injury shown in the clinical photographs and radiograph (Figures 58a through 58c) is most important?



Explanation
This is an example of a closed-mallet deformity with disruption of the extensor tendon with a fracture. There is full passive correction of the deformity (Figure 58b). The radiograph does not show subluxation of the distal phalanx on the middle phalanx (Figure 58c), so the most important part of this treatment is to maintain the DIP joint in full extension for 6 to 8 weeks. This can be done with a dorsal or volar DIP joint splint with the proximal interphalangeal (PIP) joint free. PIP motion should be encouraged but is not the hallmark of treatment. The DIP joint should not be allowed to flex for the period of immobilization. Attention should be paid to the health of the dorsal skin. A transarticular Kirschner wire can be used to maintain extension for a patient who would have difficulty performing his or her occupation, such as a surgeon or dentist. Night splinting may be continued for another month. The fracture fragments do not need to be
anatomically aligned. This injury is not associated with a nail bed injury, so nail bed repair is not needed.
Mallet deformities result from extensor tendon disruption at the DIP joint through either tendon or bone. A functional range of motion with a minimal extensor lag will be obtained. Patients should be informed about the potential for a residual DIP extensor lag and swan-neck finger deformity with all methods of treatment.
RECOMMENDED READINGS
10. Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg. 2005 Sep;13(5):336-
44/. Review. PubMed PMID: 16148359.
11. Leinberry C. Mallet finger injuries. J Hand Surg Am. 2009 Nov;34(9):1715-7. doi: 10.1016/j.jhsa.2009.06.018. Epub 2009 Sep 20. PubMed PMID: 19773131.
12. Renfree KJ. Acute, closed tendinous mallet injuries. J Hand Surg Am. 2014 Dec;39(12):2502-5; quiz 2505. doi: 10.1016/j.jhsa.2014.08.045. Epub 2014 Oct 22. PubMed PMID: 25443171.
13. Moradi A, Kachooei AR, Mudgal CS. Mallet fracture. J Hand Surg Am. 2014 Oct;39(10):2067-9. doi: 10.1016/j.jhsa.2014.06.022. Epub 2014 Aug 16. Review. PubMed PMID: 25135247.
anatomically aligned. This injury is not associated with a nail bed injury, so nail bed repair is not needed.
Mallet deformities result from extensor tendon disruption at the DIP joint through either tendon or bone. A functional range of motion with a minimal extensor lag will be obtained. Patients should be informed about the potential for a residual DIP extensor lag and swan-neck finger deformity with all methods of treatment.
RECOMMENDED READINGS
10. Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg. 2005 Sep;13(5):336-
44/. Review. PubMed PMID: 16148359.
11. Leinberry C. Mallet finger injuries. J Hand Surg Am. 2009 Nov;34(9):1715-7. doi: 10.1016/j.jhsa.2009.06.018. Epub 2009 Sep 20. PubMed PMID: 19773131.
12. Renfree KJ. Acute, closed tendinous mallet injuries. J Hand Surg Am. 2014 Dec;39(12):2502-5; quiz 2505. doi: 10.1016/j.jhsa.2014.08.045. Epub 2014 Oct 22. PubMed PMID: 25443171.
13. Moradi A, Kachooei AR, Mudgal CS. Mallet fracture. J Hand Surg Am. 2014 Oct;39(10):2067-9. doi: 10.1016/j.jhsa.2014.06.022. Epub 2014 Aug 16. Review. PubMed PMID: 25135247.
Question 19High Yield
An otherwise healthy 30-year-old man undergoes right shoulder arthroscopic Bankart repair under regional anesthesia using an interscalene brachial plexus block. In the recovery room, he reports mild difficulty breathing and his chest radiograph shows a high riding diaphragm on the right side. His peripheral oxygenation is 97% on 2 liters of oxygen by nasal cannula. What is the most appropriate management?
Explanation
**
Because the phrenic nerve lies in close proximity to the site of anesthetic injection, temporary hemidiaphragmatic paresis is a very common side effect of interscalene brachial plexus block. Pulmonary function and chest wall mechanics may be slightly compromised, but can easily be compensated in a healthy patient. Therefore, with
sufficient oxygenation, aggressive assessments or treatments such as arterial blood gas measurements,
emergent spiral CT scans, chest tube insertions, or endotracheal intubation are not warranted. For this stable patient, continued monitoring with gradual withdrawal of oxygen is the most appropriate treatment.
Because the phrenic nerve lies in close proximity to the site of anesthetic injection, temporary hemidiaphragmatic paresis is a very common side effect of interscalene brachial plexus block. Pulmonary function and chest wall mechanics may be slightly compromised, but can easily be compensated in a healthy patient. Therefore, with
sufficient oxygenation, aggressive assessments or treatments such as arterial blood gas measurements,
emergent spiral CT scans, chest tube insertions, or endotracheal intubation are not warranted. For this stable patient, continued monitoring with gradual withdrawal of oxygen is the most appropriate treatment.
Question 20High Yield
A series of axial T1-weighted MR images is shown in Figure 84. The postfracture MRI reveals tissue contamination by fracture hematoma. Based upon the MRI findings, which aspect of limb-sparing resection and reconstruction will be most challenging?
Explanation
- En bloc extra-articular resection of the knee joint_
Question 21High Yield
1253) A 69-year-old female sustains the injuries seen in Figures A and
B. This injury is best classified as which of the following?
B. This injury is best classified as which of the following?



Explanation
The radiographs and CT scan images show a depressed lateral tibial plateau fracture, which is correctly classified as a Schatzker III tibial plateau fracture. This fracture typically occurs as the result of the femoral condyle directly impacting the articular surface in older patients with osteopenia.
The referenced article by Bennett et al reviews the associated soft tissue injury with tibial plateau fractures. They found a 56% frequency of associated soft tissue injuries overall, with MCL injured in 20%, the LCL in 3% , the menisci in 20%, the peroneal nerve in 3%, and the anterior cruciate ligaments in 10%.
Schatzker type IV and type II fracture patterns were associated with the highest frequency of soft tissue injuries.
The referenced article by Bennett et al reviews the associated soft tissue injury with tibial plateau fractures. They found a 56% frequency of associated soft tissue injuries overall, with MCL injured in 20%, the LCL in 3% , the menisci in 20%, the peroneal nerve in 3%, and the anterior cruciate ligaments in 10%.
Schatzker type IV and type II fracture patterns were associated with the highest frequency of soft tissue injuries.
Question 22High Yield
A 26-year-old woman presents for treatment of painful forefoot deformity. Hallux valgus is present, with a 35° angle, and arthritis of the metatarsophalangeal (MP) joint. The second and third lesser toe MP joints are dislocated with juxta-articular erosions of the fourth metatarsal head noted. The ideal surgical treatment is:
Explanation
For the patient with rheumatoid arthritis, stabilization of the hallux metatarsophalangeal joint is necessary, and a combination bunionectomy and metatarsal osteotomy is unlikely to succeed in the long-term when arthritis is present. Although shortening osteotomies of the lesser toe metatarsals may be considered to reduce the joint dislocations, this procedure has not yet been reported with long-term follow-up. Silastic joint replacement is not a procedure with long-term benefit, and is not indicated for the lesser toes.
Question 23High Yield
Figures A and B demonstrate a proximal tibial metaphyseal fracture which will be treated with an intramedullary nail. Placing blocking screws at the sites marked with x's in the figures would help to prevent what type of malreduction deformity?




Explanation
Placing blocking screws at the sites shown would help to prevent a valgus and procurvatum deformity. This represents the most common pattern of malreduction for this fracture pattern.
Proximal tibial metaphyseal fractures being treated with an intramedullary nail are known to commonly fall into a valgus and procurvatum deformity due to lack of cortical fit in the metaphyseal segment. To help prevent this deformity blocking screws may be used. As a general rule, a blocking screw should be placed in the concavity of the deformity you intend to prevent. Thus, to prevent a valgus deformity you would place a screw just lateral to the nail.
Likewise, to prevent a procurvatum deformity you would place a blocking screw just posterior to the nail. These screws would provide a buttress to keep the metaphyseal segment in line with the tibial shaft.
Ricci et al. present a prospective cohort of 12 patients who presented with a proximal tibial metaphyseal fracture treated with an intramedullary nail and blocking screws. They found that all 12 patients went on to heal with less than 5° of angulation in all planes in which a blocking screw was used. They concluded that blocking screws are effective at maintaining proper alignment for this type of fracture being treated with an intramedullary nail.
Hiesterman et al. present a review on treatment techniques for extraarticular proximal tibia fractures treated with an intramedullary nail. They note that valgus and apex anterior deformities are most common. They cite several techniques for preventing this deformity including alternate patient positioning or approach, a universal distractor, unicortical plates, and blocking screws.
Figure A is an AP radiograph of a proximal third tibia fracture with a marking to indicate placement of a blocking screw just lateral to the central axis of the tibia. Figure B is a lateral radiograph of a proximal third tibia fracture with a marking to indicate placement of a blocking screw just posterior to the central axis of the tibia. Illustration A and B are AP and lateral radiographs of the tibia fracture seen above treated with an intramedullary nail and no blocking screws. Note the resulting valgus and procurvatum deformity about the fracture even with the nail in place. Illustrations C and D are diagrams illustrating the use of lateral and posterior blocking screws to properly align the fracture.
Incorrect Answers:
Answers 2, 3, 4, and 5: These do not correctly identify the deformity that would be prevented with locking screws placed lateral and posterior to the
intramedullary nail.
Proximal tibial metaphyseal fractures being treated with an intramedullary nail are known to commonly fall into a valgus and procurvatum deformity due to lack of cortical fit in the metaphyseal segment. To help prevent this deformity blocking screws may be used. As a general rule, a blocking screw should be placed in the concavity of the deformity you intend to prevent. Thus, to prevent a valgus deformity you would place a screw just lateral to the nail.
Likewise, to prevent a procurvatum deformity you would place a blocking screw just posterior to the nail. These screws would provide a buttress to keep the metaphyseal segment in line with the tibial shaft.
Ricci et al. present a prospective cohort of 12 patients who presented with a proximal tibial metaphyseal fracture treated with an intramedullary nail and blocking screws. They found that all 12 patients went on to heal with less than 5° of angulation in all planes in which a blocking screw was used. They concluded that blocking screws are effective at maintaining proper alignment for this type of fracture being treated with an intramedullary nail.
Hiesterman et al. present a review on treatment techniques for extraarticular proximal tibia fractures treated with an intramedullary nail. They note that valgus and apex anterior deformities are most common. They cite several techniques for preventing this deformity including alternate patient positioning or approach, a universal distractor, unicortical plates, and blocking screws.
Figure A is an AP radiograph of a proximal third tibia fracture with a marking to indicate placement of a blocking screw just lateral to the central axis of the tibia. Figure B is a lateral radiograph of a proximal third tibia fracture with a marking to indicate placement of a blocking screw just posterior to the central axis of the tibia. Illustration A and B are AP and lateral radiographs of the tibia fracture seen above treated with an intramedullary nail and no blocking screws. Note the resulting valgus and procurvatum deformity about the fracture even with the nail in place. Illustrations C and D are diagrams illustrating the use of lateral and posterior blocking screws to properly align the fracture.
Incorrect Answers:
Answers 2, 3, 4, and 5: These do not correctly identify the deformity that would be prevented with locking screws placed lateral and posterior to the
intramedullary nail.
Question 24High Yield
What is the most common mode of failure of the lateral ulnar collateral ligament associated with an elbow dislocation?
Explanation
The lateral ulnar collateral ligament (LUCL) is often injured with elbow dislocations, and is most commonly injured at the proximal origin.
McKee noted that in 62 consecutive operative elbow dislocations and fracture/dislocations, the LUCL was ruptured in all of the patients, proximally in 32, bony avulsion proximally in 5, midsubstance rupture in 18, ulnar detachment in 3, ulnar bony avulsion in only 1, and combined patterns in 3.
Pugh et al established a standard protocol to treat elbow fracture dislocations (terrible triad) which includes coronoid repair, radial head repair/replacement, LUCL repair, and MCL and/or external fixation as needed.
McKee noted that in 62 consecutive operative elbow dislocations and fracture/dislocations, the LUCL was ruptured in all of the patients, proximally in 32, bony avulsion proximally in 5, midsubstance rupture in 18, ulnar detachment in 3, ulnar bony avulsion in only 1, and combined patterns in 3.
Pugh et al established a standard protocol to treat elbow fracture dislocations (terrible triad) which includes coronoid repair, radial head repair/replacement, LUCL repair, and MCL and/or external fixation as needed.
Question 25High Yield
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study
results fits the definition of chronic prosthetic joint infection?
results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 26High Yield
A 37-year-old woman has had persistent right lateral ankle pain after sustaining a minor sprain 5 months ago. She has a sense of instability on
uneven ground. Physical therapy has not helped. She is tender along the peroneal tendons and in the sinus tarsi. She has a negative anterior drawer test result for the ankle and no tenderness over the anterior lateral malleolus. She also has bilateral pes planus that persists with heel rise.
uneven ground. Physical therapy has not helped. She is tender along the peroneal tendons and in the sinus tarsi. She has a negative anterior drawer test result for the ankle and no tenderness over the anterior lateral malleolus. She also has bilateral pes planus that persists with heel rise.
Explanation
- Casting
Question 27High Yield
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
Nearly all approaches to shoulder arthroplasty require detachment of the subscapularis tendon from the humerus and subsequent repair. Healing of this tenotomy is one of the limiting factors in postoperative recovery. Failure of the tenotomy repair must be recognized and treated early with repeat repair or pectoralis muscle transfer for optimal results. Failure of the subscapularis is diagnosed clinically as excessive external rotation and weakness, especially in the lift-off or belly press position. Muscle testing can be difficult in the postoperative period and may not be possible to assess in those positions. Although MRI might be useful to confirm the diagnosis, studies may be limited by artifact. CT or electromyography would not be diagnostic.
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
76. A 52-year-old man has shoulder pain and stiffness after undergoing a “mini-lateral” rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/ mm3 (normal 3,500 to 10,500/ mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
1- Subacromial corticosteroid injection
2- Aspiration of the subacromial and glenohumeral joint spaces
3- Nonsteroidal anti-inflammatory drugs
4- Extensive surgical debridement
5- Diagnostic arthroscopy
PREFERRED RESPONSE: 2
DISCUSSION: Deep sepsis of the shoulder following rotator cuff repair is an uncommon problem. Patients with infections of this type typically report persistent pain and are not systemically ill. They may have signs of local wound problems such as erythema, drainage, and dehiscence. Laboratory studies can be helpful in making an accurate diagnosis. Most patients will not show a significant elevation of the WBC count; however, an elevated erythrocyte sedimentation rate is nearly always present and should alert the clinician to the presence of infection. Aspiration of both subacromial and glenohumeral joint spaces is necessary to confirm the diagnosis. The most effective treatment for deep shoulder sepsis following rotator cuff repair involves extensive surgical debridement, removing all suspicious soft tissue as well as implants. Administration of appropriate antibiotic therapy is needed for complete control of the infection.
REFERENCES: Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121.
Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
76. A 52-year-old man has shoulder pain and stiffness after undergoing a “mini-lateral” rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/ mm3 (normal 3,500 to 10,500/ mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
1- Subacromial corticosteroid injection
2- Aspiration of the subacromial and glenohumeral joint spaces
3- Nonsteroidal anti-inflammatory drugs
4- Extensive surgical debridement
5- Diagnostic arthroscopy
PREFERRED RESPONSE: 2
DISCUSSION: Deep sepsis of the shoulder following rotator cuff repair is an uncommon problem. Patients with infections of this type typically report persistent pain and are not systemically ill. They may have signs of local wound problems such as erythema, drainage, and dehiscence. Laboratory studies can be helpful in making an accurate diagnosis. Most patients will not show a significant elevation of the WBC count; however, an elevated erythrocyte sedimentation rate is nearly always present and should alert the clinician to the presence of infection. Aspiration of both subacromial and glenohumeral joint spaces is necessary to confirm the diagnosis. The most effective treatment for deep shoulder sepsis following rotator cuff repair involves extensive surgical debridement, removing all suspicious soft tissue as well as implants. Administration of appropriate antibiotic therapy is needed for complete control of the infection.
REFERENCES: Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121.
Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 28High Yield
A 45-year-old man has had 3 months of increasing upper back pain, “balance" issues, and heaviness in his legs. His physical examination reveals a normal neurological examination, but he is noted to be anemic. His MRI scans and biopsy specimen are shown in Figures 1 through

Explanation
■
The MRI scan reveals a large posterior element tumor, which is compressing the spinal cord. Multiple lesions within the spinal column are consistent with multiple myeloma. Myeloma is a radiosensitive tumor. Additionally, he has a SINS of 6. This score helps the treating physician determine the tumor-related instability of the vertebral column to guide the decision for operative management. A SINS of 0-6 is thought to be stable; 7-12, potentially stable, and >13, unstable. Appropriate treatment in a neurologically intact patient with a radiosensitive tumor with a low SINS would be radiation treatment versus surgical treatment, despite the degree of spinal cord compression.
The MRI scan reveals a large posterior element tumor, which is compressing the spinal cord. Multiple lesions within the spinal column are consistent with multiple myeloma. Myeloma is a radiosensitive tumor. Additionally, he has a SINS of 6. This score helps the treating physician determine the tumor-related instability of the vertebral column to guide the decision for operative management. A SINS of 0-6 is thought to be stable; 7-12, potentially stable, and >13, unstable. Appropriate treatment in a neurologically intact patient with a radiosensitive tumor with a low SINS would be radiation treatment versus surgical treatment, despite the degree of spinal cord compression.
Question 29High Yield
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
The patient has an acute peroneal tendon dislocation. The evaluation for syndesmotic injury and lateral ankle instability is negative. The cortical avulsion off the distal tip of the lateral malleolus, a rim fracture, is characteristic of peroneal tendon dislocations. The sensation of apprehension or frank subluxation of the peroneal tendons with active dorsiflexion of the foot while the foot is held in plantar flexion confirms the diagnosis. Based on these findings, initial management should consist of cast immobilization and protected weight bearing. If a recurrent or chronic condition develops, surgery is the most reliable treatment option.
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
Question 30High Yield
Figures 32a through 32d are the radiographs and MR images of a 13-year-old girl with new posterolateral knee pain following a fall. What is the best next step?



Explanation
This patient has an incidentally noted benign-appearing fibro-osseous lesion of her proximal tibia. The lesion does not correspond to her area of pain, and there is no indication she experienced pain from the lesion prior to the fall. Radiographs and MR imaging findings are consistent with a fibrous cortical defect or nonossifying fibroma. There is no surrounding edema in the bone or soft tissue and no soft-tissue mass, and the lesion has a sclerotic rim around it. These are common lesions in children, and there is no need for a biopsy, curettage, or referral to a tumor specialist. This patient should not be at high risk for pathologic fracture from this lesion. Observation with follow-up radiographs in 3 to 6 months is the treatment of choice.
RECOMMENDED READINGS
11. [Gebhardt MC, Ready JE, Mankin HJ. Tumors about the knee in children. Clin Orthop Relat Res. 1990 Jun;(255):86-110. Review. PubMed PMID: 2189635.](http://www.ncbi.nlm.nih.gov/pubmed/2189635)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2189635)
12. [Aboulafia AJ, Kennon RE, Jelinek JS. Benign bone tumors of childhood. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):377-88. Review. PubMed PMID: 11505926. ](http://www.ncbi.nlm.nih.gov/pubmed/11505926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11505926)
RECOMMENDED READINGS
11. [Gebhardt MC, Ready JE, Mankin HJ. Tumors about the knee in children. Clin Orthop Relat Res. 1990 Jun;(255):86-110. Review. PubMed PMID: 2189635.](http://www.ncbi.nlm.nih.gov/pubmed/2189635)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2189635)
12. [Aboulafia AJ, Kennon RE, Jelinek JS. Benign bone tumors of childhood. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):377-88. Review. PubMed PMID: 11505926. ](http://www.ncbi.nlm.nih.gov/pubmed/11505926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11505926)
Question 31High Yield
A 28-year-old man reports a 3-month history of foot pain and swelling after stepping on a nail while working at a construction site. He was wearing rubber-soled boots at the time he sustained this deep puncture wound. Initial management consisted of tetanus prophylaxis, superficial wound cleansing, and oral antibiotics.
Imaging shows no evidence of bony infection. What is the most appropriate treatment?
Imaging shows no evidence of bony infection. What is the most appropriate treatment?
Explanation
Patients wearing rubber-soled shoes while sustaining deep puncture wound injuries to the foot may experience complications such as abscess formation and osteomyelitis. Frequently, there is delayed diagnosis of potential retained foreign bodies. Therefore, appropriate treatment involves wound exploration, débridement with removal of the foreign material, and IV antibiotics. A combination of formal surgery and administration of antibiotics is required for treatment of these deep wound infections;drainage or antibiotics alone will not suffice.
Question 32High Yield
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of
Explanation
Open reduction and transfer of the subscapularis and lesser tuberosity into the humeral head defect is the treatment of choice for chronic posterior dislocations in which the articular defect consists of 20% to 40% of the articular surfaces. Closed reduction can be used if the dislocation is recognized early and the articular defect is less than 20% of the articular surface. Humeral arthroplasty is reserved for patients with an articular defect that is greater than 45% to 50% of the head.
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Checchia SL, Santos PD, Miyazaki AN: Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg 1998;7:53-65.
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Checchia SL, Santos PD, Miyazaki AN: Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg 1998;7:53-65.
Question 33High Yield
A 63-year-old woman with diabetes has had an ulcer under the plantar aspect of the foot for 3 months. The ulcer extends from the inferior aspect of the heel pad toward the midfoot. Nonoperative measures have failed to heal the ulcer. The amputation that is most likely to be successful is a:
Explanation
A foot salvage amputation, including the transarticular ankle amputation (Symeâs amputation), will not work in the presence of a disrupted heel pad (with or without ulceration) and infection of the heel.
Question 34High Yield
A 28-year-old man fell off his bike and sustained a fall onto his outstretched hand. He experiences thumb and index finger numbness. Attempts at reduction of his grade I open extra-articular distal radius fracture are unsuccessful. The next appropriate step of management is:
Explanation
A patient with this injury represents a high-energy fracture in a high demand individual. The patient will require incision and drainage of his open wound, open reduction with internal fixation, and carpal tunnel release. Bone grafting would not be appropriate in a patient with open fracture.
Question 35High Yield
What is the most common complication after successful treatment of a distal femoral physeal fracture?
Explanation
■
Distal femoral physeal fracture have a high rate of premature physeal closure which can lead to limb length discrepancy or angular deformity. These fracture heal rapidly and vascular injury and knee stiffness are rarely reported. Compartment syndrome is more frequently reported with tibial tubercle fractures and not distal femoral physeal fractures.
Distal femoral physeal fracture have a high rate of premature physeal closure which can lead to limb length discrepancy or angular deformity. These fracture heal rapidly and vascular injury and knee stiffness are rarely reported. Compartment syndrome is more frequently reported with tibial tubercle fractures and not distal femoral physeal fractures.
Question 36High Yield
ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03
**ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03**
1/. A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include
1
CT of the abdomen.
2
MRI of the cervical spine.
3
a bone scan for occult fracture.
4
radiographs of the hands and feet.
5
electromyography to assess neurologic function.
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel.
**ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03**
1/. A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include
1
CT of the abdomen.
2
MRI of the cervical spine.
3
a bone scan for occult fracture.
4
radiographs of the hands and feet.
5
electromyography to assess neurologic function.
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel.
Scientific References
- : Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
LeGay D, Petrie DP, Alexander DI: Flexion-distraction injuries of the lumbar spine and associated abdominal trauma. J Trauma 1990;30:436-444.
2/. A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by
Explanation
Lateral subtalar dislocations, which are less common than medial subtalar dislocations, are high-energy injuries that are frequently associated with small osteochondral fractures. It is generally recommended that large fragments be internally fixed, and small fragments entrapped within the joint be excised. Although arthrosis frequently occurs after this injury and is the most common long-term complication, primary subtalar arthrodesis is not indicated. A talar neck fracture is not evident on the radiographs, and lateral subtalar dislocation usually does not lead to instability.
REFERENCE: Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
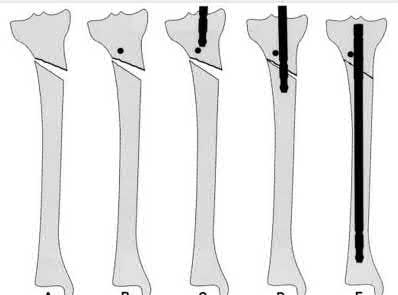
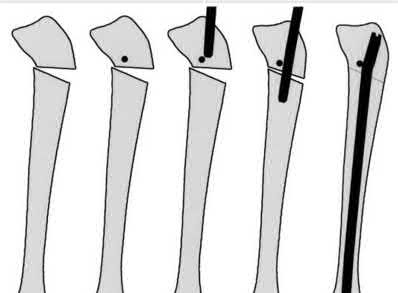
3/. Figure 2 shows the lateral radiograph of an 8-year-old boy who sustained an acute injury to the elbow after falling down the stairs. Management should consist of
1- closed reduction, followed by a long arm cast in 120 degrees of flexion.
2- closed reduction, followed by percutaneous cross pin fixation.
3- open reduction and internal fixation using an oblique screw combined with an absorbable suture as a tension band.
4- a large intramedullary screw.
5- a long arm cast in full extension.
PREFERRED RESPONSE: 3
DISCUSSION: The patient has a flexion-type olecranon fracture, and the integrity of the extensor mechanism is disrupted. With this degree of displacement, closed reduction and extension casting would not be adequate. The strongest construct is an oblique screw across the fracture site, with a tension band. Healing is rapid in this age group; therefore one of the heavy absorbable sutures can be used as the tension band. Two parallel pins with the stainless steel tension band wire (AO technique) can be used but requires wire dissection for removal. Once the fracture is healed, the single screw can be removed easily with only a small incision. The presence of the screw, across the apophysis, has not been shown to produce any significant growth disturbance. Use of a large intramedullary screw would not be advisable because of the small size of the proximal fragment.
REFERENCES: Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Chambers HG, Wilkins KE: Part IV: Fractures of the proximal radius and ulna, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 629-630.
4/. A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of
1- open reduction and internal fixation via an anteromedial arthrotomy.
2- talectomy.
3- primary tibiotalocalcaneal arthrodesis.
4- open reduction and internal fixation via a medial malleolar osteotomy and limited anterior lateral arthrotomy.
5- closed reduction and a non-weight-bearing cast.
PREFERRED RESPONSE: 4
DISCUSSION: The radiographs show a comminuted talar body fracture. The goal of treatment is to minimize the risks of posttraumatic arthrosis of the ankle and subtalar joint and to maintain vascularity. Open reduction and internal fixation with an attempt at anatomic reduction will lead to improved outcomes. Attempting to repair this fracture via an arthrotomy only is extremely difficult, and the addition of a medial malleolar osteotomy is warranted. A limited anterior lateral arthrotomy with minimal soft-tissue stripping may assist with fixation of anterior-lateral and lateral fragments and allow better assessment of reduction of the major fracture line. Nonsurgical care would lead to inadequate reduction and increased risk of both ankle and hindfoot arthrosis. Talectomy and primary ankle and hindfoot arthrodesis should not be performed as primary surgical reconstructive options in this closed injury pattern.
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp
1465-1518.
Grob D, Simpson LA, Weber BG, Bray T: Operative treatment of displaced talus fractures. Clin Orthop 1985;199:88-96.
5/. Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?
1- Sacral fracture through the foramen
2- Sacral fracture through the ala
3- Sacroiliac joint dislocation
4- Reverse fracture-dislocation of the sacroiliac joint through the ilium
5- Iliac wing fracture
PREFERRED RESPONSE: 3
DISCUSSION: Although all of the above displaced injuries require reduction, the sacroiliac joint dislocation is a ligamentous injury. Without fixation, healing is unlikely and the result will be a painful dislocation. Both Holdsworth and Tile showed that the sacroiliac joint must be reduced anatomically and stabilized. The injuries through bone will unite fairly rapidly and, if reduced and stabilized with traction or external fixation, will generally result in an acceptable outcome unless modified by other associated problems such as neurologic injury.
REFERENCES: Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995.
Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
Henderson RC: The long-term results of nonoperatively treated major pelvic disruptions. J Orthop Trauma 1989;3:41-47.
6/. A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
1- Patellar sleeve fracture
2- Avulsion of the tibial tubercle
3- Avulsion of the anterior tibial spine
4- Osteochondral fracture of the femoral condyle
5- Osteochondral fracture of the patella
PREFERRED RESPONSE: 1
DISCUSSION: This is a typical patellar sleeve fracture. The patellar tendon avulses a portion of the distal bony patella, along with the retinaculum and articular cartilage from the inferior pole of the patella. It is common in children between ages 8 and 10 years. Anatomic reduction and repair of the extensor mechanism are mandatory to reestablish full knee extension.
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
7/. A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in
1- a painful nonunion.
2- asymptomatic nonunion.
3- chronic elbow instability.
4- tardy ulnar nerve palsy.
5- cubitus varus.
PREFERRED RESPONSE: 2
DISCUSSION: The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures.
REFERENCES: Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Farsetti P, Potenza V, Caterini R, Ippolito E: Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;83:1299-1305.
8/. Which of the following factors is considered most important when assessing an ankle fracture for surgical treatment?
1- Level of the fibular fracture
2- Displacement of the fibular fracture
3- Size of the posterior malleolus
4- Position of the talus in the mortise
5- Rupture of the deltoid ligament
PREFERRED RESPONSE: 4
DISCUSSION: Although all of these factors may influence the decision to perform surgery, the most important is the position of the talus in the mortise. The goal of treatment of ankle fractures is to maintain the talus centered in the mortise. If it is in this position, the other factors do not enter into the decision to intervene surgically.
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
9/. A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindfoot deformity. A lateral radiograph is shown in Figure 6. Surgical reconstruction is best accomplished with
1- calcaneal osteotomy.
2- subtalar joint arthrodesis.
3- triple arthrodesis.
4- pantalar arthrodesis.
5- distraction bone block arthrodesis.
PREFERRED RESPONSE: 2
DISCUSSION: The patient has posttraumatic subtalar joint arthrosis that developed following a calcaneal fracture. Because there is no hindfoot deformity, in situ subtalar joint arthrodesis is the treatment of choice. Calcaneal osteotomy or distraction bone block arthrodesis is beneficial in patients with severe talar dorsiflexion or malunion of the calcaneal body. Triple arthrodesis is not warranted without changes at the transverse tarsal joint, and typically even with injury into the calcaneocuboid joint, this joint is often asymptomatic. Pantalar arthrodesis is not indicated as the pathology is occurring at the subtalar joint and not in the ankle joint.
REFERENCES: Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 1422-1464.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Chandler JT, Bonar SK, Anderson RB, Davis WH: Results of in situ subtalar arthrodesis for late sequelae of calcaneus fractures. Foot Ankle Int 1999;20:18-24.
10/. Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?
1- Respiratory depression
2- Increased salivary secretion
3- Hypertension
4- Emergence phenomena
5- Cerebral vasoconstriction
PREFERRED RESPONSE: 2
DISCUSSION: The most common deleterious side effect of ketamine is increased salivation and tracheobronchial secretions. For this reason, an antisialagogue agent should be given. While lack of sufficient respiratory depression is one of the major advantages of using ketamine, apnea can occur if the drug is given too rapidly intravenously. Emergence phenomena is common in adults but relatively rare in children.
REFERENCES: Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63.
White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
McCarty EC, Mencio GA, Walker LA, Green NE: Ketamine sedation for the reduction of children’s fractures in the emergency department. J Bone Joint Surg Am 2000;82:912-918.
11/. Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Figure 7c. Following gradual progression of weight bearing, she reports that she slipped again and placed full weight on the extremity. She now notes a new onset of increased pain in her left thigh and hip region. Follow-up radiographs are shown in Figures 7d and 7e. Reconstruction should consist of
1- conversion to a longer side plate with the same compression screw and tube angle.
2- in situ bone grafting.
3- hardware removal and reconstruction with an intramedullary device that provides fixation into the femoral head and neck.
4- hardware removal and retrograde femoral nailing.
5- revision reconstruction with cerclage wiring.
PREFERRED RESPONSE: 3
DISCUSSION: The initial fracture was an unstable reverse oblique intertrochanteric fracture with subtrochanteric extension. Initial fixation with a high-angled screw and side plate construct may not provide stability as well as a 95 degree fixed-angle device or a intramedullary hip screw device. The follow-up radiographs show loss of fixation and further propagation of the fracture distally. Reconstruction would best be accomplished with hardware removal and conversion to a long intramedullary nail with femoral head fixation or a 95 degree angled plate and screw device. Conversion to a longer plate does not improve the biomechanical situation at the primary fracture site. In situ bone grafting would not provide any additional stability and would not correct the deformity. The proximal femoral fracture is not amenable to retrograde nailing. Cerclage wiring will not sufficiently enhance stability and is not indicated.
REFERENCES: Bridle SH, Patel AD, Bircher M, Calvert PT: Fixation of intertrochanteric fractures of the femur: A randomized prospective comparison of a gamma nail and dynamic hip screw. J Bone Joint Surg Br 1991;73:330-334.
DeLee JC: Fractures and dislocations of the hip, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1659-1825.
Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
12/. An intoxicated 68-year-old man fell at home. Examination reveals abrasions on his forehead, 2/5 weakness of his hand intrinsics and finger flexors, and 4/5 strength of the deltoid, biceps, and triceps bilaterally. Lower extremity motor function is 5/5. Sensory examination to pain and temperature is diminished in his hands but intact in his lower extremities. Deep tendon reflexes are depressed in all four extremities, but perianal sensation and rectal tone are intact. Foley catheterization yields 700 mL of urine. Radiographs of the cervical spine reveal multilevel spondylosis without fracture or subluxation. An MRI scan reveals high-intensity signal change within the cord substance at C5. What is the most likely diagnosis?
1- Brown-Sequard syndrome
2- Central cord syndrome
3- Anterior cord syndrome
4- Posterior cord syndrome
5- Bilateral brachial plexus palsy
PREFERRED RESPONSE: 2
DISCUSSION: Central cord syndrome is characterized by greater neurologic involvement of the upper extremities than the lower extremities. This is typically seen in older patients with cervical spondylosis without associated bony injury or joint subluxation. The prognosis for recovery is fair. Patients with Brown-Sequard syndrome have an ipsilateral motor deficit and contralateral loss of pain and temperature. Prognosis for recovery depends on the mechanism of injury, which is often of a penetrating nature. Anterior cord syndrome results from anterior compression such as occurs with a burst or teardrop fracture of the vertebral body; patients have bilateral motor loss, pain, and temperature loss with preservation of proprioception and vibratory sensation (posterior column function). The prognosis for recovery is generally poor. Posterior cord syndrome is rare and is associated with loss of posterior column function (proprioception and vibration).
REFERENCES: Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 541-549.
Schneider RC, Thompson JM, Rebin J: The syndrome of acute central cervical spinal cord injury. J Neurol Neurosurg Psychiatry 1958;21:216-227.
13/. A 23-year-old woman sustains an injury to her right hand after falling off her snowboard. Examination reveals that she has difficulty moving her fingers. A radiograph and a clinical photograph are shown in Figures 8a and Figure 8b. Management should consist of
1- closed reduction and buddy taping.
2- in situ pinning.
3- open reduction and internal fixation.
4- casting for 6 weeks.
5- dynamic extension splinting.
PREFERRED RESPONSE: 3
DISCUSSION: The radiograph reveals oblique fractures of the third and fourth metacarpals. The rotational component of the fracture displacement is well visualized on the clinical photograph, which shows scissoring of the middle finger over the ring finger. The fracture obliquity results in rotational deformity that cannot be adequately maintained and held by closed treatment. The treatment of choice is open reduction and internal fixation.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Freeland AE, Benoist LA, Melancon KP: Parallel miniature screw fixation of spiral and long oblique hand phalangeal fractures. Orthopedics 1994;17:199-200.
Freeland AE, Geissler WB: Plate fixation of metacarpal shaft fractures, in Blair WF (ed): Techniques in Hand Surgery. Baltimore, MD, Williams and Wilkins, 1996, pp 255-264.
14/. A 32-year-old man sustained an L1 burst fracture with 90% canal compromise, intact posterior elements, and kyphosis of 25% at the L1 level. He has an incomplete neurologic injury. Definitive management should consist of
1- bed rest for 8 weeks, followed by mobilization in a total contact thoracolumbosacral orthosis.
2- immediate laminectomy only.
3- anterior decompression, vertebral body reconstruction, and stabilization.
4- in situ posterior fusion.
5- short segment posterior fixation and fusion.
PREFERRED RESPONSE: 3
DISCUSSION: With an incomplete injury, the best chance for recovery occurs when the canal is cleared and the neural structures are decompressed. Anterior decompression, vertebral body reconstruction, and anterior stabilization have been shown to be highly effective in the treatment of burst-type injuries. Laminectomy alone is contraindicated because it increases the instability. Short segment posterior fixation has a high rate of failure in this type of injury at this level.
REFERENCES: Kaneda K, Abumi K: Burst fractures with neurologic deficits of the thoracolumbar spine. J Bone Joint Surg Am 1997;79:69-83.
McGuire R Jr: The role of anterior surgery in the treatment of thoracolumbar fractures. Orthopedics 1997;20:959-962.
15/. The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?
1- Anatomic alignment
2- Indirect reduction
3- Anatomic reduction of the fragments
4- Relatively stable fixation
5- Functional aftercare
PREFERRED RESPONSE: 3
DISCUSSION: Although the original concept of internal fixation was one of anatomic reduction and stable fixation, over the past 10 to 15 years there has been a change based on the advent of intramedullary nailing and bridge plating. It is now appreciated that in a multifragmentary diaphyseal fracture, particularly of the lower extremity, the achievement of axis alignment (mechanical and anatomic axis) is all that is required. Healing will occur by callus. Relatively stable fixation is achieved through intramedullary nailing or bridge plating, providing adequate pain relief for functional aftercare.
REFERENCES: Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000,
pp 7-32.
deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Mast J, Jakob R, Ganz R: Planning and Reduction Techniques in Fracture Surgery. Berlin, Springer-Verlag, 1989.
16/. A 68-year-old woman who sustained a closed distal tibia fracture 2 years ago was initially treated with an external fixator across the ankle for 12 weeks, followed by intramedullary nailing of the fibula and lag screw fixation of the tibia. She continued to report persistent pain so she was treated with a brace and a bone stimulator. She now reports pain in her ankle. Examination reveals ankle range of motion of 8 degrees of dorsiflexion to 25 degrees of plantar flexion. She is neurovascularly intact. Current radiographs are shown in Figures 9a through 9c. What is the next most appropriate step in management?
1- A cast and weight bearing as tolerated
2- A brace and an ultrasound bone stimulator
3- Intramedullary nailing
4- Open reduction and plate fixation with bone grafting
5- Fibular osteotomy
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a nonunion of the distal fifth of the tibia. The nonunion appears to be oligotrophic, somewhere between atrophic and hypertrophic. Management requires stabilization and stimulation of the local biology, which can be accomplished with open reduction and internal fixation with bone grafting. Bracing or casting does not provide enough stability. Ultrasound bone stimulation has been shown to speed fresh fracture repair but is not indicated in nonunions. The distal segment is too short for intramedullary nailing. A fibular osteotomy alone would increase instability and, even with prolonged casting, would be unlikely to lead to successful repair.
REFERENCES: Carpenter CA, Jupiter JB: Blade plate reconstruction of metaphyseal nonunion of the tibia. Clin Orthop 1996;332:23-28.
Lonner JH, Siliski JM, Jupiter JB, Lhowe DW: Posttraumatic nonunion of the proximal tibial metaphysis. Am J Orthop 1999;28:523-528.
Stevenson S: Enhancement of fracture healing with autogenous and allogeneic bone grafts. Clin Orthop 1998;355:S239-S246.
Wiss DA, Johnson DL, Miao M: Compression plating for non-union after failed external fixation of open tibial fractures. J Bone Joint Surg Am 1992;74:1279-1285.
17/. A patient has a displaced midshaft transverse fracture of the humerus and is neurologically intact. Following closed reduction and application of a coaptation splint, the patient cannot dorsiflex the wrist or the fingers at the metacarpophalangeal joints of the hand. What is the next most appropriate step in management?
1- Observation with a high expectation for recovery
2- Observation for 1 week, followed by exploration if recovery is not evident
3- Immediate exploration of the radial nerve and fracture fixation
4- Immediate exploration of the radial nerve without fracture fixation
5- Removal of the coaptation splint and repeat reduction
PREFERRED RESPONSE: 1
DISCUSSION: The answer to this question is controversial. All of the standard textbooks state that development of a radial nerve palsy during initial fracture management may represent a laceration or injury of the nerve by bone fragments at the time of manipulation; therefore, surgery should be considered. However, it appears that there is no scientific basis for this decision. A review of the available literature shows that the results were the same for patients who were observed as for those who underwent radial nerve exploration. The indications for surgical exploration include palsies associated with open fractures, irreducible closed fractures, and vascular injuries. The only other relative indication for surgical exploration is following manipulation of a Holstein-Lewis fracture (a distal third fracture of the humerus with a lateral spike). In this type of fracture, exploration may be necessary if a closed reduction leads to radial nerve palsy because the spike may lacerate or compress the nerve. Observation for return of nerve function may be appropriate for 3 months or longer prior to considering late exploration.
REFERENCES: Bostman O, Bakalim G, Vainionpaa S, Wilppula E, Patiala H, Rokkanen P: Radial palsy in shaft fracture of the humerus. Acta Orthop Scand 1986;57:316-319.
Shaz JJ, Bhatti NA: Radial nerve paralysis associated with the fractures of the humerus: A review of 62 cases. Clin Orthop 1983;172:171-176.
Holstein A, Lewis GB: Fractures of the humerus with radial nerve paralysis. J Bone Joint Surg Am 1963;458:1382-1388.
18/. A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
1- External fixation
2- Plate fixation
3- Unreamed unlocked intramedullary nailing
4- Reamed statically locked intramedullary nailing
5- Reamed unlocked nailing
PREFERRED RESPONSE: 1
DISCUSSION: A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient’s femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing.
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
19/. Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?
1- Distal femoral pin and 90-90 traction for 3 weeks, followed by a spica cast
2- Closed reduction and stabilization with an external fixator
3- Closed reduction and stabilization with an interlocking nail
4- Closed reduction and stabilization with multiple flexible intramedullary nails
5- Open reduction and stabilization with a plate and screws
PREFERRED RESPONSE: 4
DISCUSSION: Because the patient has a transverse midshaft fracture with no evidence of comminution, the treatment of choice is closed reduction and stabilization with flexible intramedullary nails. Transverse fractures treated with an external fixator heal with poor callus and have a high refracture rate. In addition, the pin tracks produce undesirable and excessive scarring. Femoral pin traction is safe and effective but results in considerable muscle wasting and a slow return to function. Interlocking nails run the risk of greater trochanteric growth disturbance and/or osteonecrosis of the femoral head in this age group. Plate fixation, while effective, requires considerable tissue dissection with large scar formation. It also requires a rather extensive dissection for later plate removal.
REFERENCES: Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Heinrich SD, Drvaric D, Darr K, MacEwen GD: Stabilization of pediatric diaphyseal femoral fractures with flexible intramedullary nails (a technique paper). J Orthop Trauma 1992;6:452-459.
20/. A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of
1- open reduction and internal fixation with bone grafting.
2- closed reduction and percutaneous pin fixation.
3- aspiration and steroid injection.
4- closed manipulation and a long arm cast.
5- in situ open bone grafting.
PREFERRED RESPONSE: 1
DISCUSSION: The patient has a scaphoid fracture with cystic resorption of the distal aspect of the midthird of the scaphoid. This fracture is unlikely to heal without intervention. Percutaneous pinning, closed manipulation, and bone grafting will not restore alignment. Treatment requires restoration of scaphoid length, bone grafting, and internal fixation to obtain healing with normal alignment.
REFERENCES: Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650.
Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737.
Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am
1988;70:982-991.
Feldman MD, Manske PR, Welch RL, Szerzinski JM: Evaluation of Herbert screw fixation for the treatment of displaced scaphoid nonunions. Orthopedics 1997;20:325-328.
21/. A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
1- Loss of reduction of the ulnar physis
2- Loss of reduction of the radial metaphysis
3- Physeal arrest of the distal radius
4- Physeal arrest of the distal ulna
5- Osteonecrosis of the ulnar epiphysis
PREFERRED RESPONSE: 4
DISCUSSION: While injury of the distal radial metaphysis is a rather common occurrence, the incidence of physeal arrest is only about 4% to 5% of patients. While injury of the distal physis of the ulna is rare, the incidence of physeal arrest is greater than 50% in fractures of this structure. These patients need to be followed closely both clinically and radiographically to look for the signs of distal ulnar/physeal arrest such as loss of the prominence of the ulna and ulnar deviation of the hand. Radiographically, progressive shortening of the ulna is observed.
REFERENCES: Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, pp 632-635.
22/. A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of
1- mobilization in a kinetic therapy bed for 8 weeks.
2- initiation of a steroid protocol.
3- immediate laminectomy of T7, T8, and T9.
4- application of a total contact orthosis.
5- open reduction and posterior segmental stabilization and grafting.
PREFERRED RESPONSE: 5
DISCUSSION: With a complete injury in the thoracic spinal cord, the likelihood of neurologic recovery is small. If possible, treatment should be planned to allow rapid mobilization and rehabilitation without the use of braces and their associated skin problems. The use of long segment fixation provides for rapid mobilization without having to use braces postoperatively. The use of steroid protocol is controversial and should be considered only if it can be started within 8 hours of the injury. Laminectomy is contraindicated because it will increase instability.
REFERENCE: Tasdemiroglu E, Tibbs PA: Long-term follow-up results of thoracolumbar fractures after posterior instrumentation. Spine 1995;20:1704-1708.
23/. A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of
1- skeletal tong traction for 6 weeks.
2- halo application.
3- immobilization in a rigid collar for 6 weeks.
4- open reduction posteriorly with interspinous wiring and bone grafting.
5- open reduction anteriorly with diskectomy, interbody grafting, and plating.
PREFERRED RESPONSE: 3
DISCUSSION: The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
REFERENCE: Clarke CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
24/. A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
1- Inflation of the abdominal portion of the PASG
2- Application of a pelvic clamp
3- Application of a pelvic external fixator
4- Rapid infusion of 4 more units of blood
5- Angiography and embolization
PREFERRED RESPONSE: 5
DISCUSSION: There is no identifiable thoracic, abdominal, or long bone source of ongoing bleeding. The patient has a lateral compression Burgess-Young type I pelvic ring injury. This injury does not increase the pelvic volume because it is not unstable in external rotation. Application of a PASG, a pelvic clamp, or an external fixator may be helpful if the patient has a pelvic injury that is unstable in external rotation or translation but would be of little use in this injury pattern. Persistent hemodynamic instability after administration of 4 units of blood is the decision point where most authors would recommend angiography and embolization. If the pelvis is unstable in external rotation or translation, inflation of the PASG trousers or application of an external fixator is recommended before angiography. Attributing the hemodynamic instability to the head injury before ruling out the pelvis as a source is not indicated.
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
25/. A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?
1- Visualization of the articular surface
2- Avoidance of an olecranon osteotomy
3- A muscle-sparing approach
4- The likelihood a total elbow arthroplasty will be performed
5- The likelihood that reconstruction of the anterior elbow joint will be performed
PREFERRED RESPONSE: 1
DISCUSSION: When managing a complex intra-articular fracture, it is imperative that there is adequate visualization of the joint; this usually means an extensile approach. At the elbow, this is usually through a transolecranon osteotomy. The recent addition of a muscle-sparing approach as described by Bryan and Morrey has gained popularity, but it is difficult to maintain soft-tissue viability and it may put the ulnar nerve at risk. A triceps-splitting approach, which can be used for simple single articular splits into the joint where extra-articular reduction is available, is possible and good results have been reported. To date, there is minimal data on these alternative approaches for comminuted intra-articular distal humeral fractures.
REFERENCES: McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522
McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop
2000;370:19-33.
Bryan RS, Morrey BF: Extensive posterior exposure of the elbow: A triceps-sparing approach. Clin Orthop 1982;166:188-192.
26/. The use of nasotracheal intubation for airway management is contraindicated in the acute multiply injured patient when the patient has
1- suspected cervical spine trauma.
2- head injuries and spontaneous respirations.
3- respiratory arrest.
4- a need for prolonged ventilatory support.
5- a hemopneumothorax.
PREFERRED RESPONSE: 3
DISCUSSION: The use of nasotracheal intubation is less desirable in patients with respiratory arrest because placement of the tube is most reliable when the patient is breathing. Nasotracheal intubation is advantageous in patients with suspected cervical spine trauma because it does not require hyperextension of the neck. A nasotracheal tube may be more comfortable than an orally placed tube because it is fixed at several points and moves less freely within the larynx, subglottic area, and trachea. The presence of a hemothorax or pneumothorax does not affect the choice of airway control but does require placement of a chest tube.
REFERENCES: Colice GL: Prolonged intubation versus tracheostomy in the adult. J Intern Care Med 1987;2:85.
Shackford S: Spine injury in the polytrauma patient: General surgical and orthopaedic considerations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 9-15.
27/. A 65-year man has right hip pain after a fall. Radiographs reveal a reverse oblique intertrochanteric femoral fracture. Treatment consists of reduction and internal fixation. Which of the following implants is most commonly associated with nonunion and hardware failure?
1- Sliding hip screw
2- Dynamic condylar screw
3- 95 blade plate
4- Cephalomedullary nail
5- Intramedullary hip screw
PREFERRED RESPONSE: 1
DISCUSSION: Reverse oblique intertrochanteric femoral fractures account for 5% of all intertrochanteric or subtrochanteric fractures. They are uncommon but not rare and will be encountered in practice. The sliding hip screw is associated with the most problems because of its design. When reverse oblique fractures are fixed with a sliding hip screw, the action of the construct causes medial displacement of the distal fragment rather than compression of the proximal and distal fragments. All of the other implants prevent medial displacement of the distal segment. It should not be assumed that simply using one of the other implants is reason for success. There is a significant failure rate for each of these implants with reverse oblique fractures. The implant must be ideally placed and the fracture must be reduced.
REFERENCES: Haidukewych GJ, Israel TA, Berry DB: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Baumgaertner MR, Chrostowski JH, Levy RN: Intertrochanteric hip fracture, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1833-1881.
28/. Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?
1- Wedge the cast to correct angulation.
2- Accept the present alignment and continue follow-up.
3- Perform open reduction and internal fixation of both the radius and ulna with plates and screws.
4- Perform open reduction and internal fixation of both the radius and ulna with intramedullary rods.
5- Remanipulate both the radius and ulna and stabilize with an external fixator.
PREFERRED RESPONSE: 2
DISCUSSION: Bayonet apposition of the radius and ulnar shafts is quite acceptable, as long as the angulation is less than 10 degrees. The rotation must be acceptable as well. This patient went on to full healing, with full supination and pronation of the forearm and no cosmetic deformity.
REFERENCES: Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Vittas D, Larsen E, Torp-Pedersen S: Angular remodeling of midshaft forearm fractures in children. Clin Orthop 1991;265:261-264.
29/. In Figure 14, the primary fracture line in a calcaneal fracture is best depicted by which of the following schematics?
1- A
2- B
3- C
4- D
5- E
PREFERRED RESPONSE: 1
DISCUSSION: The schematic labeled A best depicts the primary fracture line in a calcaneal fracture. The primary fracture line in an axial-loading fracture of the calcaneus occurs from superior-lateral to inferior-medial. This fracture line separates the calcaneus into sustentacular and tuberosity fragments and typically enters the subtalar joint through the posterior facet. Although additional fracture lines typically occur, the primary fracture line is almost always present. If surgical reduction is planned, reducing the primary fracture is always a key step.
REFERENCES: Macey LR, Benirschke SK, Sangeorzan BJ, Hansen ST: Acute calcaneal fractures: Treatment option and results. J Am Acad Orthop Surg 1994;2:36-43.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
30/. A 45-year-old man who sustains a medial subtalar dislocation while playing basketball undergoes immediate closed reduction. No fractures or osteochondral defects are noted on postreduction radiographs. The next most appropriate step in management should consist of
1- a long leg cast for 6 weeks.
2- an ankle support and return to activities.
3- a short leg cast for 4 weeks.
4- open repair of ligaments and active range of motion.
5- open repair of ligaments and casting for 6 weeks.
PREFERRED RESPONSE: 3
DISCUSSION: Most subtalar dislocations can be easily reduced by closed methods. If no fractures or defects are seen on the postreduction radiographs, then the success rate with cast immobilization is good. Medial dislocations have a better prognosis than lateral dislocations. Late instability is rare; therefore, the duration of immobilization should not be excessive. Most subtalar dislocations result in some stiffening of the hindfoot, and painful degenerative arthrosis is the most common serious complication.
REFERENCE: Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
31/. A 21-year-old woman sustained a minimally displaced traumatic spondylolisthesis of C2 (Hangman’s fracture) after striking the windshield with her forehead during a motor vehicle accident. Management should consist of
1- skeletal tong traction for 6 weeks.
2- anterior C2-3 diskectomy, grafting, and plate fixation.
3- halo application for 8 weeks.
4- a rigid collar for 4 to 6 weeks, followed by mobilization.
5- posterior stabilization with C2 pedicle screws.
PREFERRED RESPONSE: 4
DISCUSSION: According to the classification of Levine and Edwards, a type I Hangman’s fracture is minimally displaced without angulation and represents a stable injury. Good clinical success has been achieved with nonsurgical management consisting of use of a rigid collar until the patient reports pain relief, followed by quick mobilization.
REFERENCE: Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
32/. A 25-year-old patient who sustained multiple bilateral rib fractures, a pulmonary contusion, a left nondisplaced transtectal acetabular fracture, and a closed humerus fracture in a motor vehicle accident 2 weeks ago is transferred from another hospital. The humerus fracture has been surgically treated. There are no signs of infection, and the trauma surgeon wants to mobilize the patient as soon as possible. Radiographs are shown in Figures 15a and 15b. Management of the humerus fracture should consist of
1- open reduction and plate fixation.
2- a humeral fracture brace.
3- a locking intramedullary nail.
4- insertion of at least two additional pins.
5- removal of the pins and a long arm hanging cast.
PREFERRED RESPONSE: 1
DISCUSSION: The radiographs show a distal third humerus fracture that is angulated, rotated, and not rigidly fixed. Rigid fixation is needed because mobilization is highly desirable to improve pulmonary function. The acetabular fracture is through the weight-bearing dome but is nondisplaced. Nonsurgical management of the acetabular fracture requires at least 6 weeks of touchdown weight bearing to minimize the forces across the hip joint. Open reduction and plate fixation would achieve anatomic reduction and immediate mobilization. A single posterolateral 4.5-mm plate or two 3.5-mm plates at 90 degrees are possible alternatives. Immediate weight bearing on a plated humerus fracture with the use of crutches or a walker has been shown to be safe and would allow touchdown weight bearing, protecting the hip. None of the other options would achieve this goal for this distal fracture.
REFERENCE: Tingstad EM, Wolinsky PR, Shyr Y, Johnson KD: Effect of immediate weightbearing on plated fractures of the humeral shaft. J Trauma 2000;49:278-280.
33/. Figure 16 shows the radiograph of a 23-year-old man who has severe right shoulder pain after his motorcyle hit a bridge guardrail. He is neurologically intact. Nonsurgical management will most likely result in
1- nonunion of the clavicle or glenoid.
2- thoracic outlet syndrome.
3- less than 50% range of motion compared with the contralateral shoulder.
4- less than 50% strength compared with the contralateral shoulder.
5- high patient satisfaction and good shoulder function.
PREFERRED RESPONSE: 5
DISCUSSION: Internal fixation of the clavicle, glenoid, or both has been recommended for fractures of the clavicle and glenoid neck (floating shoulders). Recently, the inherent instability of these dual fractures has been questioned in a biomechanical model without further disruption of the coracoclavicular or acromioclavicular ligamentous structures. Nonsurgical management of the majority of combined scapular/glenoid fractures in patients with less than 10 mm of displacement has resulted in excellent shoulder function and will most likely achieve an excellent result in this patient.
REFERENCES: Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF: The floating shoulder: Clinical and functional results. J Bone Joint Surg Am 2001;83:1188-1194.
Williams GR Jr, Naranja J, Klimkiewicz J, et al: The floating shoulder: A biomechanical basis for classification and management. J Bone Joint Surg Am 2001;83:1182-1187.
Edwards SG, Whittle AP, Wood GW: Nonoperative treatment of ipsilateral fractures of the scapular and clavicle. J Bone Joint Surg Am 2000;82:774-779.
34/. An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
1- Unreamed intramedullary nail
2- Reamed statically locked intramedullary nail
3- External fixation
4- Plate fixation and interfragmentary compression
5- Bridge plate stabilization
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a simple fracture pattern that can be reduced anatomically and stabilized with absolute stability by interfragmental compression and protection plating. This will guarantee a 95% to 98% union rate with no radial nerve palsy. Intramedullary nailing does not equal these results in a simple fracture pattern in the humerus. Bridge plating is indicated for multifragmented fracture patterns when anatomic reduction and absolute stability cannot be achieved. External fixation is reserved for severe open fractures.
REFERENCES: Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
35/. A 28-year-old painter has had increasing pain in his hand and forearm after sustaining a paint injection wound to the tip of his left index finger 24 hours ago. Management should consist of
1- hospital admission and IV antibiotics.
2- emergent surgical debridement.
3- oral antibiotics, splinting, and elevation.
4- nonsteroidal anti-inflammatory drugs and splinting.
5- oral antibiotics and a tetanus shot.
PREFERRED RESPONSE: 2
DISCUSSION: The clinical presentation soon after injury may be surprisingly innocuous, but all high-pressure injection injuries of various materials are best treated by emergent surgical debridement of all foreign material from the flexor tendon sheath as well as the subcutaneous tissues. Subsequent hospital admission, IV antibiotics, and possible repeat debridements usually are necessary. The use of antibiotics alone is inadequate treatment of this severe injury.
REFERENCES: Pinto MR, Turkula-Pinto LE, Cooney WP, Wood MB, Dobyns JH: High-pressure injection injuries of the hand: Review of 25 patients managed by open wound technique. J Hand Surg Am 1993;18:125-130.
Urbaniak JR, Evans JP, Bright DS: Microvascular management of ring avulsion injuries. J Hand Surg Am 1981;6:25-30.
Tsai TM, Manstein C, DuBou R, Wolff T, Kutz JE, Kleinert HE: Primary microsurgical repair of ring avulsion amputation injuries. J Hand Surg Am 1984;9:68-72.
Kay S, Werntz J, Wolff T: Ring avulsion injuries: Classification and prognosis. J Hand Surg Am 1989;14:204-213.
Schnall SB, Mirzayan R: High-pressure injection injuries to the hand, in Kozin SH (ed): Hand Clinics: Upper Extremity Trauma. Philadelphia, PA, 1999, pp 245-248.
36/. A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?
1- Posterior tibial tendon
2- Impaction fracture of the head of the talus
3- Posterior tibial neurovascular bundle
4- Achilles tendon
5- Calcaneus fracture
PREFERRED RESPONSE: 2
DISCUSSION: The patient has a medial subtalar dislocation. These injuries should be reduced as soon as possible to minimize risk to the skin. Most often, this can be done easily, and further radiographic evaluation then can be performed as necessary. On rare occasions, closed reduction is not possible because of fractures of the articular surface of the talus, navicular, interposed extensor digitorum brevis, or transverse fibers of the cruciate crural ligament. The posterior tibial tendon is the most common obstruction to closed reduction in lateral subtalar dislocations, which are less common than medial dislocations. The majority of both injuries can be managed by closed reduction and immobilization.
REFERENCES: Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863.
Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
37/. A 27-year-old woman sustained a bilateral C5-6 facet subluxation in a motor vehicle accident. Neurologic evaluation reveals normal motor, sensory, and reflex functions. She is awake, alert, and cooperative. Initial management should consist of
1- halo application.
2- skeletal traction and attempted closed reduction.
3- a soft cervical collar.
4- immediate transfer to the operating room for closed reduction.
5- immediate transfer to the operating room for open reduction and
stabilization posteriorly.
PREFERRED RESPONSE: 2
DISCUSSION: As long as the patient is alert and cooperative, an attempt can be made to reduce the dislocation. This should not be attempted in a patient who is obtunded, comatose, or uncooperative. If any neurologic changes are noted during the reduction maneuver, the attempt should be stopped, appropriate radiographic studies obtained, and open reduction and stabilization planned in the operating room.
REFERENCE: Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case reports. J Bone Joint Surg Am 1991;73:1555-1560.
38/. A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of
1- indirect fracture reduction via traction and early mobilization.
2- volar plate arthroplasty.
3- open reduction and internal fixation.
4- closed reduction and percutaneous pin fixation.
5- cast immobilization.
PREFERRED RESPONSE: 1
DISCUSSION: This fracture, known as a pilon fracture, represents comminution of the base of the middle phalanx with both palmar and dorsal cortical disruption. The treatment method that allows the best function and fewest complications is indirect reduction achieved through specific dynamic splinting or the use of specifically designed proximal interphalangeal joint external fixators. Early mobilization can be achieved by either of these techniques. Volar plate arthroplasty is indicated for a simple fracture-dislocation of the proximal interphalangeal joint with comminution of the volar fracture fragment and dorsal dislocation of the remaining articular surface. Open reduction and internal fixation or percutaneous pinning adds surgical risks and scarring and typically will not provide added stability. Cast immobilization will not achieve the goal of early range of motion.
REFERENCES: Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Krakauer JD, Stern PJ: Hinged device for fractures involving the proximal interphalangeal joint. Clin Orthop 1996;327:29-37.
39/. Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of
1- early motion and muscle strengthening.
2- immobilization in a thumb spica cast with the thumb abducted.
3- open reduction and internal fixation through a volar approach.
4- open reduction and internal fixation through a dorsal approach.
5- closed reduction and percutaneous pin fixation.
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a Salter-Harris type III fracture of the proximal phalanx of the thumb. It is usually caused by an abduction injury where the ulnar collateral ligament avulses a fragment away from the proximal epiphysis and is the most common childhood gamekeeper’s injury. If there is greater than 1 mm of separation or a significant articular step-off, an open reduction, performed through an extensor aponeurosis-splitting approach, is required to reestablish joint congruity and stability. Percutaneous or closed methods of reduction are usually ineffective. The dorsal approach avoids the volar neurovascular structures. Since the ulnar collateral ligament is still attached, this area does not need to be visualized. The major goal is to reestablish joint congruity and bony stability. This can be easily performed via the dorsal approach.
REFERENCES: Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, p 668.
40/. Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of
1- a long arm cast.
2- immediate functional bracing.
3- closed reduction and percutaneous pin fixation.
4- percutaneous olecranon pin traction.
5- total elbow arthroplasty.
PREFERRED RESPONSE: 5
DISCUSSION: The radiographs reveal a severely comminuted distal humerus fracture. A long arm cast, functional bracing, and closed reduction and percutaneous pin fixation all have a poor outcome and could result in a nonunion that will be very difficult to treat. Open reduction and internal fixation is indicated in most supracondylar humerus fractures, but total elbow arthroplasty is a good alternative in elderly patients who have multiple medical problems and when the fracture pattern may preclude stable enough internal fixation to allow postoperative motion.
REFERENCES: Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Morrey BF: Fractures of the distal humerus: Role of elbow replacement. Orthop Clin North Am 2001;31:145-155.
41/. An 18-year-old man has acute respiratory distress after sustaining injuries in a motorcycle accident. He has a blood pressure of 80/60 mm Hg and a pulse rate of 110/min. Examination reveals chest tympany to percussion, distended neck veins, and deviation of the trachea away from his right hemithorax where the breath sounds are diminished. Heart sounds are regular and normal on auscultation. Initial management should consist of
1- administration of 2 L of saline solution.
2- subxiphoid pericardial aspiration.
3- rapid infusion of 500 mL of colloid solution.
4- insertion of a large-bore needle in the right third or fourth intercostal space.
5- intubation followed by mechanical ventilation.
PREFERRED RESPONSE: 4
DISCUSSION: Tension pneumothorax occurs when air trapped in the pleural space between the lung and chest wall achieves sufficient pressure to compress the lungs and shift the mediastinum. Urgent needle decompression of the pleural space air followed by definitive chest tube placement is the treatment of choice.
REFERENCE: Mattox KL, Feliciano DV, Moore EE (eds): Management of Shock, ed 4. New York, NY, McGraw Hill, 2000, p 215.
42/. A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?
1- Cruciate paralysis
2- Quadraplegia
3- Normal function
4- Absent bulbocavernosus reflex
5- Greater occipital nerve dysesthesia
PREFERRED RESPONSE: 3
DISCUSSION: The radiographic findings are consistent with a type II Hangman’s fracture or traumatic spondylolisthesis of C2. This occurs with more than 3 mm of displacement according to the classification of Levine and Edwards. Even though the radiograph reveals significant displacement, the overall space available for the neural elements is increased, therefore minimizing the risk of neural compromise. Neurologic injury is most frequently encountered in type III injuries that are associated with bilateral facet dislocations of C2 on C3 but is infrequent in type I (less than 3 mm displacement) and type II traumatic spondylolisthesis. When neurologic deficits are associated with type II injuries, it is usually the result of an associated head injury. Cruciate paralysis occurs as a result of the crossover of the motor and sensory tracts at different levels of the cord at the C1-C2 junction. This results in normal sensation but complete loss of motor function.
REFERENCES: Levine AM: Traumatic spondylolisthesis of the axis (Hangman’s fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R: Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313-318.
43/. After stabilizing a bimalleolar ankle fracture with a plate and lag screws for the fibula and two interfragmental compression screws for the medial malleolus, a syndesmosis screw is indicated in which of the following situations?
1- In all suprasyndesmotic fibular fractures
2- In all transsyndesmotic fibular fractures
3- When there is increased medial clear space with external rotation stress
4- If the deltoid ligament is ruptured
5- If the posterior malleolus is fractured
PREFERRED RESPONSE: 3
DISCUSSION: It is imperative to recognize the need for a position screw (syndesmosis screw) to hold the syndesmosis in proper alignment when surgically stabilizing an ankle fracture. Although many different fracture patterns are suspicious for a disrupted syndesmosis, the only sure way to assess the syndesmosis is to stress it with abduction and external rotation of the talus and attempt to displace the fibula from the incisura fibularis. Under fluoroscopy, the talus will move laterally and displace the fibula, show a valgus talar tilt, or show an increase in the medial clear space. If any or all of these signs occur, a syndesmosis screw is inserted after making sure that the fibula is reduced into the incisura fibularis. This screw may traverse three or four cortices but must not act as a lag screw. It usually is inserted with the ankle in maximal dorsiflexion, although this is probably not necessary because it is almost impossible to overcompress the syndesmosis. The diameter of the screw does not make any difference. It may or may not be removed but not before 3 months.
REFERENCES: Tornetta P III, Spoo JE, Reynolds FA, Lee C: Overtightening of the ankle syndesmosis: Is it really possible? J Bone Joint Surg Am 2001;83:489-492.
Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
44/. A 32-year-old man sustains multiple injuries in a motorcycle accident including ipsilateral open right femur and comminuted tibia fractures. He has acute abdominal distention and tenderness to palpation. The pelvis is stable to examination. He has a blood pressure of 70/40 mm Hg despite appropriate fluid resuscitation and a pulse rate of 120/min; the pulse is thready. Which of the following procedures is considered the highest priority in the management of this patient?
1- Emergent CT of the abdomen and pelvis
2- Insertion of a Swan-Ganz catheter to monitor the cardiac index
3- Administration of albumin solution
4- Emergent laparotomy in the operating room
5- Application of a pneumatic antishock garment
PREFERRED RESPONSE: 4
DISCUSSION: The patient is in hemorrhagic shock, and timely hemostasis in the operating room should be the highest priority. Further imaging and insertion of central lines carry the risk of further delays in arresting the source of the patient’s bleeding. Albumin (colloid) solutions have questionable indications, are expensive, and have been associated with increased mortality. Crystalloid solutions such as normal saline or lactated Ringer’s solution are the initial resuscitative fluid of choice until blood becomes available. Pneumatic antishock garments have been associated with higher mortality rates, particularly in patients with cardiac and thoracic vascular injuries.
REFERENCES: Krettek C, Simon RG, Tscherne H: Management priorities in patients with polytrauma. Langenbecks Arch Surg 1998;383:220-227.
Weigelt JA: Resuscitation and initial management. Crit Care Clin 1993;9:657-671.
45/. A 35-year-old man sustained an injury to his lower extremity after falling 10 feet from a ladder; initial management was nonsurgical. He now reports chronic hindfoot and anterior ankle pain. Radiographs are shown in Figures 22a and 22b. Surgical reconstruction of this painful process should consist of
1- talectomy and tibiocalcaneal arthrodesis.
2- in situ subtalar joint arthrodesis.
3- distraction bone block subtalar joint arthrodesis.
4- lateral wall exostectomy of the calcaneus.
5- tibiotalar joint arthrodesis.
PREFERRED RESPONSE: 3
DISCUSSION: The radiographs reveal a hindfoot deformity that developed following a severe, comminuted, intra-articular fracture of the calcaneus. There is deformity of the calcaneal body and collapse of the talus into the calcaneus, leading to dorsiflexion of the talus and anterior ankle joint impingement. Distraction bone block subtalar joint arthrodesis will assist with correction of the calcaneal height and will allow for an improved talar declination angle. With this procedure, care must be taken to avoid placing the hindfoot into further varus. A similar reconstruction option not listed would be a calcaneal osteotomy and arthrodesis as described by Romash. Talectomy and tibiocalcaneal arthrodesis are not warranted because the primary structure of the talus and ankle joint is well preserved. In situ subtalar joint arthrodesis will not correct the deformity, and symptoms about the ankle and hindfoot would most likely persist. Lateral wall calcaneal exostectomy may decrease pain from subfibular impingement but will not deal directly with subtalar joint arthrosis and deformity.
REFERENCES: Carr JB, Hansen ST , Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Romash MM: Reconstructive osteotomy of the calcaneus with subtalar arthrodesis for malunited calcaneal fractures. Clin Orthop 1993;290:157-167.
46/. An 8-year-old boy falls and injures his thumb. A radiograph is shown in Figure 23. Initial management should consist of
1- closed reduction.
2- closed reduction and percutaneous pinning.
3- open reduction through a volar approach.
4- open reduction through a dorsal approach.
5- splinting for comfort.
PREFERRED RESPONSE: 1
DISCUSSION: The radiograph shows a complete simple dislocation of the metacarpophalangeal joint. The clue to this injury is the perpendicular alignment of the proximal phalanx to the metacarpal on the lateral radiograph. This must be differentiated from the complete complex dislocation pattern that is irreducible because of the interposed volar plate. In lateral radiographs of these injuries, the long axes of the proximal phalanx and the metacarpal are parallel. Simple dislocations are amenable to closed reduction and casting. Some authors have recommended ulnar collateral ligament repair if instability is detected on examination after reduction.
REFERENCES: O’Brien ET: Part IV: Dislocations of hand and carpus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 429-431.
Bohart PC, Gelberman RH, Vardell RF, Solomon PB: Complex dislocations of the MCP joint. J Bone Joint Surg Am 1974;56:1459-1463.
47/. A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of
1- stretching of the forearm in pronation, wrist flexion, and splinting.
2- primary tendon repair of the flexor pollicis longus and flexor digitorum profundus to the index finger, followed by immobilization.
3- electrodiagnostic examination, followed by decompression of the anterior interosseous nerve within the next 2 to 3 weeks.
4- splinting followed by observation; surgical decompression of the median nerve may be required if no improvement in seen in 3 months.
5- splinting followed by observation; surgical decompression of the anterior interosseous nerve may be required if no improvement is seen in 6 months.
PREFERRED RESPONSE: 5
DISCUSSION: The patient has anterior interosseous nerve palsy. Initial management should consist of splinting followed by observation; surgical decompression may be required if there is no improvement in the functional deficit in 6 months. Anterior interosseous nerve palsy is classically described as an inability to flex the interphalangeal joint of the thumb because of flexor pollicis longus paralysis and a weakness or inability to flex the distal interphalangeal joint of the index finger because of weakness and/or paralysis of the flexor digitorum profundus to the index finger. There has been some controversy in the literature as to whether this represents a true peripheral compression neuropathy or neuritis. Recent recommendations have been to extend the period of observation from 3 to 6 months before surgical decompression, as most cases will resolve within 6 months.
REFERENCES: Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
Stern PJ, Fassler PR: Anterior interosseous nerve compression syndrome, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, 1991, vol 2, pp 983-1002.
48/. A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
1- a shoulder spica cast with the upper extremity in the salute position.
2- a sling and swathe for 3 weeks, followed by gradual motion and strengthening.
3- closed reduction and antegrade intramedullary pinning.
4- closed reduction and retrograde intramedullary nailing.
5- open reduction and internal fixation with small plates and screws.
PREFERRED RESPONSE: 2
DISCUSSION: In this age group, bayonet apposition can produce very good results. Healing occurs rapidly, and remodeling usually is complete in less than 1 year. All of the other methods have significant risks of complications and are unnecessary for this fracture.
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
49/. The cortical injury to the posterolateral distal fibula shown in Figure 25 indicates involvement of which of the following structures?
1- Deltoid ligament
2- Anterior talofibular ligament
3- Calcaneal fibular ligament
4- Superior peroneal retinaculum
5- Syndesmosis
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a rim avulsion fracture that is the result of a forceful twisting injury as the superior peroneal retinaculum is avulsed from its fibular attachment along with a small rim of bone. Injuries to the anterior talofibular ligament or calcaneal fibular ligament would show cortical avulsions more anteriorly or distally at the fibular tip. Deltoid ligament injuries would reveal medial radiographic changes. In a true injury to the syndesmosis, if osseous structures do show avulsion, it would be more directly posterior or anterior on the distal fibula or would occur on the tibial surface.
REFERENCES: Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
50/. A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
1- observation and splinting.
2- local wound drainage under local anesthesia.
3- incision and drainage, deep wound cultures, removal of the plates and screws, and cast application.
4- incision and drainage, deep wound cultures, and removal of the fixation only if it is loose.
5- incision and drainage, deep wound cultures, and bone grafting.
PREFERRED RESPONSE: 4
DISCUSSION: Deep infections after plating of closed fractures of the forearm are unusual. However, the risk increases with repeat surgeries. Debridement of all infected, nonviable tissue is the initial step in management. The fixation may be retained if it is stable, but if the plate and screws are loose, they should be removed and revision performed after removal of nonviable bone. Either external fixation or repeat plating may be performed. Late infections after fracture union may be treated with plate and screw removal, debridement, and IV antibiotics.
REFERENCES: Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63.
Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphysis of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
51/. A left-handed 23-year-old man who fell 5 feet from a ladder onto his left elbow sustained the closed injury shown in Figure 26. Management should consist of
1- percutaneous pin fixation.
2- a percutaneous 6.5-mm screw.
3- long arm casting in flexion.
4- open reduction and internal fixation with a tension band plate.
5- closed reduction and long arm casting in extension.
PREFERRED RESPONSE: 4
DISCUSSION: The radiographs reveal a displaced olecranon fracture. To maximize joint congruity of this intra-articular injury, open reduction and internal fixation is the treatment of choice. A tension band plate will assist with maintenance of the reduction and may aid in early range of motion because injuries to the elbow are prone to stiffness. The oblique fracture line is particularly well suited to plate fixation. Percutaneous pin fixation is unlikely to achieve anatomic joint reduction that can be obtained with open means. External immobilization will not accomplish joint reduction and will most likely lead to a nonunion.
REFERENCES: Hotchkiss RN: Fractures and dislocations of the elbow, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 929-1024.
Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Hume MC, Wiss DA: Olecranon fractures: A clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop 1992;285:229-235.
52/. Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
1- Progressive limb-length discrepancy
2- Contralateral ankle arthritis
3- Ipsilateral hindfoot and midfoot arthritis
4- Ipsilateral knee arthritis
5- Talar osteonecrosis
PREFERRED RESPONSE: 3
DISCUSSION: Ankle arthrodesis for posttraumatic ankle arthrosis provides reliable pain relief. However, the long-term sequela of joint arthrodesis is the development of arthrosis in the surrounding joints. Over time, following ankle arthrodesis, the ipsilateral hindfoot and midfoot joints show signs of joint space wear, and this may be symptomatic. With a stable ankle arthrodesis, progressive limb-length discrepancy or talar osteonecrosis is not expected. Ankle arthrodesis has not been definitively linked to ipsilateral knee arthritis or contralateral ankle arthritis.
REFERENCES: Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Mazur JM, Schwartz E, Simon SR: Ankle arthrodesis: Long-term follow-up with gait analysis. J Bone Joint Surg Am 1979;61:964-975.
53/. A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
1- limited weight bearing for 6 weeks, followed by a progressive return to activity.
2- no weight bearing for 6 weeks, followed by no running for 6 months.
3- no weight bearing for 2 weeks, followed by internal fixation if symptoms persist.
4- internal fixation at the time of diagnosis.
5- cessation of running for 6 weeks.
PREFERRED RESPONSE: 4
DISCUSSION: Unlike compression-side stress fractures, tension-side stress fractures on the superior side of the femoral neck are at a very high risk of displacement, even if the patient is not bearing weight. It is highly recommended to treat these fractures like acute fractures and to proceed with internal fixation emergently. Once the fracture has displaced, the prognosis is poor in terms of returning to sports, even when reduced and internally fixed. Nonsurgical management, such as limited weight bearing and low-impact activities, works very well for other lower extremity stress fractures. A training program evaluation (shoes, tracks, schedule) is always indicated for all patients with stress fractures.
REFERENCE: Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
54/. A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
1- Latent osteomyelitis from the percutaneous pins
2- Muscle weakness because of a lack of postinjury rehabilitation
3- Tardy ulnar nerve paralysis from injury by the medial pin
4- Osteonecrosis of the trochlea, producing joint incongruity
5- A new acute process
PREFERRED RESPONSE: 4
DISCUSSION: The patient sustained a very distal supracondylar fracture of the humerus. Fractures in this area can disrupt the blood vessels supplying the lateral ossification center of the trochlea. With disturbance of the blood supply in this area, local osteonecrosis occurs and disrupts the support for the overlying articular surface, producing joint incongruity and localized degenerative arthritis.
REFERENCES: Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
Morrissy RT, Wilkins KE: Deformities following distal humeral fracture in childhood. J Bone Joint Surg Am 1984;66:557-562.
55/. A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of
1- closed treatment and observation for return of nerve function.
2- closed treatment and immediate tendon transfer.
3- open nerve exploration without internal fixation of the fracture.
4- open nerve exploration with plating of the fracture.
5- open nerve exploration with intramedullary rodding of the fracture.
PREFERRED RESPONSE: 1
DISCUSSION: The patient has an isolated closed injury involving the humeral diaphysis. The lack of wrist and finger extension indicates injury to the radial nerve. Based on these findings, ongoing observation of the nerve is warranted with delayed exploration after 3 to 4 months if there are no signs of progressive return of nerve function. Treatment of the fracture should include external immobilization and fracture bracing. An indication for nerve exploration and surgical stabilization would be an open fracture.
REFERENCES: Zuckerman JD, Kovil KJ: Fractures of the shaft of the humerus, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1025-1053.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
56/. Examination of a 41-year-old man who was thrown from a motorcycle reveals that both legs appear externally rotated and there is bruising in the perineal area. He has a blood pressure of 80/40 mm Hg, a pulse rate of 140/min, a respiratory rate of 25/min, and he appears confused. Following administration of 4 L of saline solution and 2 units of packed red blood cells, he has a blood pressure of 80/40 mm Hg, a pulse rate of 160/min, and a respiratory rate of 25/min. The abdominal assessment for intraperitoneal blood is negative. An AP radiograph shows an anteroposterior compression injury with 7 cm of symphysis diastasis but no posterior displacement in the sacroiliac joints. What is the next most appropriate step in management?
1- Stabilization of the pelvis through noninvasive methods
2- Additional crystalloid solution replacement
3- External fixation in the operating room
4- Angiographic embolization
5- Continuing observation of vital signs
PREFERRED RESPONSE: 1
DISCUSSION: Because the patient has sustained a major high-energy injury to the pelvic ring, it can be assumed that there is serious bleeding or hemodynamic instability related to a pelvic vascular injury. The goal of intervention at this time is to assist in the resuscitative effort and to stop the bleeding. All attempts at providing fluid and blood are important, but without cessation of the bleeding continued loss occurs and significant problems can ensue such as coagulopathy and multiple organ failure. Noninvasive methods of stabilizating the pelvic ring should be used to stop the bleeding. These methods include wrapping a sheet around the pelvis or using commercially available belts, vacuum beanbags, or pneumatic shock garments. This will provide time to prepare for arteriography and/or external fixation. The next step is debatable but in view of negative findings for intra-abdominal blood, arteriography performed with the pelvis reduced using noninvasive methods would be ideal.
REFERENCES: Bassam D, Cephas GA, Ferguson KA, Beard LN, Young JS: A protocol for the initial management for unstable pelvic fractures. Am Surg 1998;64:862-867.
Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 217-226.
Mucha P Jr, Welch TJ: Hemorrhage in major pelvic fractures. Surg Clin North Am 1988;68:757-773.
57/. A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of
1- closed reduction and application of a long leg cast.
2- open reduction and internal fixation with plate and screw fixation.
3- percutaneous plate fixation.
4- spanning external fixation with delayed limited open reduction and internal fixation.
5- primary ankle arthrodesis.
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a severe high-energy injury from axial loading to the left ankle and distal tibia. This is a closed injury, but the soft tissues are injured and severely swollen. Initial treatment should focus on skeletal stabilization, and incisions directly over the fracture area should be avoided until soft-tissue stabilization has occurred. Immediate spanning external fixation with plans for a delayed reconstruction as needed for the joint surface is the treatment of choice. Closed reduction and application of a constrictive long leg cast may lead to increased risk of tissue necrosis. Immediate open procedures to internally fix the fracture add the risks of soft-tissue necrosis and are to be avoided. Percutaneous plating may be one of the delayed fixation options but should not be used immediately. Primary ankle arthrodesis is not indicated.
REFERENCES: Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
58/. Which of the following parameters is considered most important when assessing an acetabular fracture for surgical indications?
1- Age of the patient
2- Failure to maintain reduction of the head under the dome without traction
3- Presence of a femoral head impaction lesion
4- Direction of the femoral head displacement
5- Fragmentation of the fracture
PREFERRED RESPONSE: 2
DISCUSSION: The most important aspect in the decision for surgery in an acetabular fracture is the ability of the femoral head to remain concentrically reduced under the dome in AP and Judet oblique views of the pelvis. If this parameter is present, then the need for surgery is determined by other aspects such as fragmentation, age, incongruity, and displacement. If the head remains stable under the dome without traction, there is sufficient acetabular dome to provide stability, and nonsurgical treatment may be appropriate.
REFERENCES: Tile M: Assessment and management of acetabular fractures, in Tile M (ed): Pelvic and Acetabular Fractures, ed 2. Baltimore, MD, Williams and Wilkins, 1995, pp 305-354.
Letournel E: Acetabular fractures: Classification and management. Clin Orthop 1980;151:81-106.
Letournel E, Judet R: Fractures of the Acetabular, ed 2. Berlin, Springer-Verlag, 1993, pp 29-49.
59/. A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of
1- ankle arthrodesis.
2- modified Brostrom ligament reconstruction.
3- restoration of fibular length, alignment, and rotation.
4- cast immobilization.
5- tibial shortening osteotomy.
PREFERRED RESPONSE: 3
DISCUSSION: The radiographs reveal a malunited distal fibular fracture with shortening. Because there appears to be an adequate cartilage space within the ankle joint, the role of reconstruction would be to prevent arthrosis and the need for ankle arthrodesis, as well as to decrease symptoms. The treatment of choice is restoration of fibular length, alignment, and rotation with osteotomy plating, and bone grafting as needed. There is no indication for ligament reconstruction of a mechanically stable ankle, and tibial shortening osteotomy will not assist in correcting the deformity. Cast immobilization may assist with improvement of symptoms but will not correct the overall process. Determination of fibular length is best done by comparing the talocrural angle of the injured side with the uninjured side. The goal is to perfectly reduce the talus in the ankle mortise.
REFERENCES: Marti RK, Raaymakers EL, Nolte PA: Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-713.
Geissler W, Tsao A, Hughes J: Fractures and injuries of the ankle, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2201-2206.
Yablon IG, Leach RE: Reconstruction of malunited fractures of the lateral malleolus. J Bone Joint Surg Am 1989;71:521-527.
60/. A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
1- extensor digitorum brevis.
2- plantar fascia.
3- peroneus brevis.
4- peroneus longus.
5- syndesmosis.
PREFERRED RESPONSE: 4
DISCUSSION: The os peroneum is an accessory ossicle located within the peroneus longus tendon. It is typically located at the level of the cuboid groove in the lateral hindfoot and midfoot region. Proximal migration of the os peroneum indicates disruption of the peroneus longus tendon and is an important clue to diagnosis. This unusual condition can cause chronic lateral ankle pain, and surgical repair may be indicated. Active eversion indicates that the peroneus brevis is clinically intact. Disruption of the extensor digitorum brevis, plantar fascia, or syndesmosis would have no effect on the position of the os peroneum.
REFERENCES: Thompson FM, Patterson AH: Rupture of the peroneus longus tendon: Report of three cases. J Bone Joint Surg Am 1989;71:293-295.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
61/. A 24-year-old man sustained a grade IIIb open tibial fracture and an ipsilateral grade IIIa femoral fracture in a motorcycle accident. He is unresponsive, intubated, and has a Glasgow Coma Scale score of 8. He is resuscitated and taken to the operating room for definitive orthopaedic care. Which of the following intraoperative problems will most likely adversely affect his long-term outcome?
1- Blood loss during debridement
2- Prolonged tourniquet time
3- Failure to stabilize both fractures with intramedullary nails
4- Episodic hypotension
5- Loss of dorsalis pedis pulse
PREFERRED RESPONSE: 4
DISCUSSION: Traumatic brain injury is considered to be either primary or secondary. Primary injury is direct or impact damage to the brain, and secondary injury can have intracranial or systemic causes. While treatment has little impact on primary brain injury, secondary brain injury can be avoided. There are also many causes of intracranial secondary brain injury, including intracranial hypertension or cerebral edema. There are many causes of systemic secondary brain injury, but none has a greater impact on outcome than hypotension or hypoxia. In fact, the occurrence of hypotension postinjury causes a 10- to 15-fold increase in mortality. In a series by Pietropaoli and associates, the mortality rate for head-injured patients that were normotensive during surgery was 25%, but if they were hypotensive the mortality rate was 82%. In the same series, the number of patients with a Glasgow Coma Scale score of either 4 or 5 dropped from 58% in those patients that were normotensive during surgery to 6% in those patients that became hypotensive during surgery. Efforts to avoid hypotension postinjury and especially during surgery should be of primary importance.
REFERENCES: Chesnut RM, Marshall LF, Klauber MR, et al: The role of secondary brain injury in determining outcome from severe head injury. J Trauma 1993;34:216-222.
Pietropaoli JA, Rogers FB, Shackford SR, Wald SL, Schmoker JD, Zhuang J: The deleterious effects of intraoperative hypotension on outcome in patients with severe head injury. J Trauma 1992;33:403-407.
Schmeling GJ, Schwab JP: Polytrauma care: The effect of head injuries and timing of skeletal fixation. Clin Orthop 1995;318:106-116.
Townsend RN, Lheureau T, Protech J, Reimer B, Simon D: Timing fracture repair in patients with severe brain injury (Glascow Coma Scale score
J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
72/. A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?
1
Increased pitching activity in conjunction with aggressive physical therapy
2
Biopsy of the lesion in the proximal humerus
3
Complete rest with no activity
4
Immobilization in a shoulder spica cast in the salute position
5
Cessation of pitching and a vigorous program of muscle strengthening
The patient has a rotational stress fracture of the proximal humeral physis (Little Leaguer’s shoulder). The symptoms of increasing pain with activity and relief with rest are typical of a stress injury. Treatment should consist of cessation of throwing activity but rehabilitation of the shoulder girdle muscles. The pitching technique should be evaluated as well.
REFERENCES: Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in the adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
73/. A 36-year-old man sustains a traumatic spondylolisthesis of L5 on S1. Surgical stabilization requires pedicular fixation into the sacrum. If the screw is placed in a medial to lateral direction and penetrates the sacral ala, what nerve root is at risk?
1- L2
2- L3
3- L4
4- L5
5- S1
PREFERRED RESPONSE: 4
DISCUSSION: The L5 nerve root lies directly over the superior and anterior alae. If the screw is directed approximately 20 degrees laterally and bicortical purchase is achieved, there is the risk of injuring the L5 nerve root. If the screw is directed medially into the body of S1, there is little risk of injury. The same root is at risk during placement of an iliosacral screw.
REFERENCES: Ebraheim NA, et al: Lumbosacral nerve and dorsal screw placement. Orthopedics 2000;23:245-247.
Ebraheim NA, Mermer M, Xu R, Yeasting RA: Radiological evaluation of S1 dorsal screw placement. J Spinal Disord 1996;9:527-535.
Routt ML Jr, Nork SE, Mills WJ: Percutaneous fixation of pelvic ring disruptions. Clin Orthop 2000;375:15-29.
74/. A 25-year-old woman who fell on her outstretched hand reports chronic pain over the hypothenar eminence region and some dorsal ulnar wrist pain. She also notes difficulty playing golf and tennis. Plain radiographs of the hand and wrist are unremarkable. A CT scan is shown in Figure 36. What is the next most appropriate step in management?
1- Ultrasound therapy
2- MRI for further soft-tissue evaluation
3- Open reduction and internal fixation of the hook of the hamate
4- Excision of the hook of the hamate
5- Electrodiagnostic evaluation
PREFERRED RESPONSE: 4
DISCUSSION: The CT scan reveals a hook of the hamate nonunion with irregular resorption at the fracture site, which is at the base of the hamate. Symptomatic relief of the pain and discomfort has been well documented after excision of the hook of the hamate. Ultrasound therapy will not provide long-term symptomatic relief or induce nonunion healing. MRI for further soft-tissue evaluation is inappropriate because this is a bony problem; the bony architecture of the wrist is best visualized by CT. Open reduction and internal fixation of the hook of the hamate does not provide the symptomatic relief that is found with excision of the hook of the hamate. In addition, the technical difficulties and relative risk of persistent nonunion after open reduction and internal fixation are not merited when hamate excision can be effected easily and causes no long-term untoward effects. Electrodiagnostic evaluation is inappropriate because there is no history of the persistent numbness and tingling that is found in peripheral compression neuropathies.
REFERENCES: Stark HH, Chao EK, Zemel NP, Rickard TA, Ashworth CR: Fracture of the hook of the hamate. J Bone Joint Surg Am 1989;71:1206-1207.
Failla JM: Hook of hamate vascularity: Vulnerability to osteonecrosis and nonunion. J Hand Surg Am 1993;18:1075-1079.
Carter PR, Easton RG, Littler JW: Ununited fracture of the hook of the hamate. J Bone Joint Surg Am 1977;59:583-588.
Egawa M, Asai T: Fracture of the hook of the hamate: Report of six cases and the suitability of computerized tomography. J Hand Surg Am 1983;8:393-398.
75/. An active 72-year-old woman sustained a mid-diaphyseal right humerus fracture 16 months ago. History reveals that she was first treated with a brace for 7 months. Additional treatment consisted of intramedullary nailing 9 months ago. Recently the rod was removed, and the patient now reports pain and gross motion at the fracture site. Current radiographs are shown in Figures 37a and 37b. What is the next most appropriate step in management?
1- Electrical stimulation with an implanted coil
2- Ultrasound stimulation for 30 minutes per day
3- Locked intramedullary nailing with bone graft
4- Ilizarov external fixation with intermittent distraction and compression
5- Plate and screw fixation with bone graft
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a well-established nonunion in a very porotic bone. Electrical stimulation has been found effective in treating tibial nonunions, but there is very little data on humeral nonunions, especially chronic well-established ones. Ultrasound stimulation is effective in accelerating fracture healing, but there is little data concerning the treatment of nonunions. Intramedullary nailing with bone graft is an option, but it maybe difficult to obtain a rigid construct in a very porotic bone. An Ilizarov-type external fixator would be an alternative, but there is little clinical data for the humerus and it may be poorly tolerated. A plate and screw construct with bone graft combines rigidity with the biologic advantage of the bone graft. A recent series reported on the use of a plate combined with onlay allograft for recalitrant nonunions. Cement augmentation for screw fixation either in the canal or added to the screw holes may be helpful in select cases.
REFERENCES: Hornicek FJ, Zych GA, Hutson JJ, Malinin TI: Salvage of humeral nonunions with onlay bone plate allograft augmentation. Clin Orthop 2001;386:203-209.
Jupiter JB: The treatment of complex non-unions of the humeral shaft with a combination of surgical techniques. J Bone Joint Surg Am 1990;72:701-707.
76/. A 47-year-old man ruptured his left patellar tendon and twisted his right ankle in a fall. Initial radiographs of the ankle are unremarkable. One week following repair of the left patellar tendon, he reports increased pain with weight bearing in his right ankle. A follow-up radiograph is shown in Figure 38. Management of the ankle injury should consist of
1- functional rehabilitation with range of motion and strengthening.
2- reduction and screw fixation of the syndesmosis.
3- closed reduction and a long leg cast.
4- repair of the talofibular ligaments.
5- fibular osteotomy and plate fixation.
PREFERRED RESPONSE: 2
DISCUSSION: The radiograph reveals disruption of the syndesmosis with lateral displacement of the talus and widening of the medial ankle clear space. No fibular fracture is noted, although radiographs of the entire tibia and fibula are necessary to rule out a more proximal fibula fracture. There is clear instability of the syndesmosis, and surgical stabilization is needed, either by direct repair of the ligaments or more commonly with surgical stabilization of the fibula to the tibia with screws. Functional rehabilitation and early range of motion are indicated with anterior-lateral ankle sprains but not with true instability of the syndesmosis. In anterior syndesmotic injuries in which there are no signs of instability on plain radiographs or with stressing, cast immobilization and protected weight bearing until tenderness subsides is warranted. Long leg cast immobilization is unlikely to be adequate in maintaining reduction of the syndesmosis. Repair of the talofibular ligaments or fibular osteotomy does not address the pathology at the syndesmosis. Chronic syndesmotic disruption is likely to lead to chronic ankle pain and early arthrosis.
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Edwards GS Jr, DeLee JC: Ankle diastasis without fracture. Foot Ankle 1984;4:305-312.
77/. A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
1- open reduction and internal fixation.
2- percutaneous pin fixation.
3- excision of the fracture fragment.
4- primary calcaneocuboid joint arthrodesis.
5- a walking cast or removable cast boot.
PREFERRED RESPONSE: 5
DISCUSSION: The CT scans show a fracture of the anterior process of the calcaneus that involves less than 25% of the joint surface with minimal to no displacement. The preferred treatment is external immobilization in either a walking cast or, more typically, a removable cast boot. For larger fractures that involve more than 25% of the articular surface with joint incongruity, open reduction and internal fixation may be indicated. Primary calcaneocuboid joint arthrodesis is not warranted because symptoms are rare in most patients. Delayed excision of the fragment is a late reconstructive option if painful nonunion develops. Percutaneous pin fixation is not indicated beceause there tends to be inherent stability in this fracture.
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
78/. Which of the following complications occurs more commonly after antegrade femoral nail insertion when compared with retrograde insertion?
1- Increased blood loss
2- Decreased range of motion of the knee
3- Infection
4- Hip pain
5- Muscle weakness
PREFERRED RESPONSE: 4
DISCUSSION: There is no difference between the rates of union, malunion, range of motion of the hip or knee, muscle weakness, or infection for the two types of femoral nail insertion. The only difference is the location of the morbidity, which is around the insertion point of the rod. The antegrade technique has more morbidity about the hip, and the retrograde insertion technique has more morbidity about the knee.
REFERENCES: Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16.
Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R: Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161-169.
Ostrum RF, Agarwal A, Lakatos R, Poka A: Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496-501.
Tornetta P III, Tiburzi D: Antegrade or retrograde reamed femoral nailing: A prospective, randomized trial. J Bone Joint Surg Br 2000;82:652-654.
79/. A 24-year-old man has right forearm pain after sliding head first into home plate. Examination reveals that the arm is swollen, but there are no neurovascular deficits or skin lacerations. Radiographs reveal a both-bone forearm fracture. The ulna has an oblique fracture with a 30% butterfly fragment, and the radius is comminuted over 75% of its circumference. In addition to reduction and plate fixation of both bones, management should consist of
1- bone grafting the radius only.
2- bone grafting both the radius and ulna.
3- bone graft substitute for both the radius and ulna.
4- no additional grafting.
5- no additional grafting but postoperative electrical stimulation.
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a both-bone fracture with a comminuted radial shaft. Open reduction and internal fixation of both bones is the treatment of choice. In the past, Chapman and associates recommended bone grafting radial shaft fractures with more than 30% comminution of the circumference. This has remained the recommendation in most textbooks. More recent studies, where modern biologic plating techniques were used, found that the addition of bone graft to comminuted fractures was not necessary because the union rate did not differ from that of nongrafted comminuted fractures.
REFERENCES: Anderson LD, Sisk TD, Tooms RE, Park WI III: Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am 1975;57:287-297.
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
Wright RR, Schmeling GJ, Schwab JP: The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review. J Orthop Trauma 1997;11:288-294.
Wei SY, Born CT, Abene A, Ong A, Hayda R, Delong WG Jr: Diaphyseal forearm fractures treated with and without bone graft. J Trauma 1999;46:1045-1048.
80/. A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
1- Fracture comminution
2- Displacement of 1 mm at the fracture site
3- Involvement of the ischial facet
4- Femoral head subluxation during fluoroscopic examination
5- Presence of a bilateral pneumothorax
PREFERRED RESPONSE: 4
DISCUSSION: Fractures with a posterior wall fragment that makes up less than one third of the surface generally are stable. Conversely, fractures with a fragment making up more than 50% of the surface are unstable. Patients with an intermediate fracture fragment should undergo a fluoroscopic examination under sedation or anesthesia to determine if the fragment is truly stable. If so, the patient can be treated nonoperatively and safely mobilized.
REFERENCES: Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
Keith JE Jr, Brashear HR Jr, Guilford WB: Stability of posterior fracture-dislocations of the hip: Quantitative assessment using computed tomography. J Bone Joint Surg Am 1988;70:711-714.
81/. A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of
1- closed reduction and a short arm cast for 10 weeks.
2- closed reduction and a long arm cast for 10 weeks.
3- open reduction and internal fixation.
4- limited intercarpal fusion.
5- proximal row carpectomy.
PREFERRED RESPONSE: 3
DISCUSSION: The radiographs reveal a scaphoid fracture with displacement and comminution and an unstable fracture pattern. Treatment should consist of open reduction and internal fixation. In displaced scaphoid fractures and fractures with unstable fracture patterns, closed reduction is ineffective and is likely to lead to nonunion. Limited intercarpal fusion and proximal row carpectomy are used to correct a variety of traumatic and posttraumatic problems of the wrist.
REFERENCES: Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 809-823.
Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276.
Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
Szabo RM, Manske D: Displaced fractures of the scaphoid. Clin Orthop 1988;230:30-38.
82/. A 42-year-old woman reports that she has low back pain and had a transient loss of consciousness after falling off a horse. She denies having neck pain but notes that she was involved in a motor vehicle accident 2 years ago and had neck pain at that time. Examination reveals full range of motion of the neck and no localized tenderness. The neurologic examination is normal. A lateral radiograph of the cervical spine is obtained. Figures 41a and 41b show CT and MRI scans. What is the most likely diagnosis?
1- Cervical sprain
2- Atlas fracture
3- Acute displaced odontoid fracture
4- Odontoid nonunion
5- Hangman’s fracture
PREFERRED RESPONSE: 4
DISCUSSION: The examination findings do not correlate with an acute injury (full range of cervical motion and the absence of pain). Radiographically, the fracture appears old based on the smooth contour of the fracture fragments and the absence of soft-tissue swelling. Flexion-extension radiographs can be obtained to determine potential instability; if present, stabilization and fusion should be considered.
REFERENCES: Schatzker J, Rorabeck CH, Waddell JP: Non-union of the odontoid process: An experimental investigation. Clin Orthop 1975;108:127-137.
Clark CR, White AA III: Fractures of the dens: A multicenter study. J Bone Joint Surg Am 1985;67:1340-1348.
83/. What neurologic structure is most at risk when performing intramedullary screw fixation of a fifth metatarsal base fracture?
1- Saphenous nerve
2- First branch of the lateral plantar nerve
3- Superficial peroneal nerve
4- Sural nerve
5- Deep peroneal nerve
PREFERRED RESPONSE: 4
DISCUSSION: The sural nerve and its terminal branches course through the lateral hindfoot and midfoot area and are directly at risk in surgeries involving the peroneal tendon complex and the fifth metatarsal. The first branch of the lateral plantar nerve originates in the tarsal tunnel region and courses across the plantar heel area to innervate the abductor digiti minimi; it is not at direct risk with fifth metatarsal surgery. The saphenous, superficial peroneal, and deep peroneal nerves are not at risk anatomically with a lateral midfoot incision.
REFERENCES: Donley BG, McCollum MJ, Murphy GA, Richardson EG: Risk of sural nerve injury with intramedullary screw fixation of fifth metatarsal fractures: A cadaver study. Foot Ankle Int 1999;20:182-184.
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
84/. A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
1- bed rest only for 6 weeks.
2- mobilization in a kinetic therapy bed for 6 weeks, followed by a hyperextension brace.
3- a total contact thoracolumbosacral orthosis and rapid mobilization.
4- anterior decompression, vertebral reconstruction, and stabilization.
5- posterior reduction, stabilization, and grafting.
PREFERRED RESPONSE: 3
DISCUSSION: The patient has a stable fracture that can be initially treated with bed rest, followed by bracing and quick mobilization. The outcome is good and surgery is not required. These fractures can be treated nonsurgically if there is less than 50% compression, 15 degrees of angulation, and intact posterior structures.
REFERENCES: Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Rechtine GR II, Cahill D, Chrin AM: Treatment of thoracolumbar trauma: Comparison of complications of operative versus nonoperative treatment. J Spinal Disord 1999;12:406-409.
85/. A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
1- observation.
2- a rigid collar for 6 weeks.
3- halo vest application.
4- open reduction and posterior stabilization.
5- open reduction, diskectomy, grafting, and anterior plate stabilization.
PREFERRED RESPONSE: 2
DISCUSSION: The patient has a stable flexion-compression injury of the cervical spine. The fracture occurs as a result of compression failure of the vertebral body. If the force continues, a tension failure of the posterior structures occurs, leading to potential dislocation. Immobilization in a rigid cervical orthosis will allow this fracture to heal.
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Allen GL, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
86/. Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
1- external traction.
2- open reduction and internal stabilization.
3- repeat closed reduction under general anesthesia.
4- open reduction.
5- percutaneous pin fixation in the current position.
PREFERRED RESPONSE: 4
DISCUSSION: The radiographs show a complex dislocation of the little finger metacarpophalangeal joint. This is characterized by obvious dislocation on the AP and lateral views and a type of bayonet apposition best visualized on the lateral view. Irreducibility of this injury is caused by displacement of the volar plate that has been traumatically avulsed from its origin on the metacarpal, with subsequent displacement into the metacarpophalangeal joint. This abnormal position of the volar plate causes irreducibility that can be corrected only by open reduction. This can be effected either by dorsal or palmar approaches.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
87/. A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
1- repeat closed reduction and buddy taping.
2- closed reduction and percutaneous pin fixation, followed by casting.
3- open reduction and plate fixation, followed by casting.
4- open reduction and screw fixation, followed by splinting and early motion.
5- open reduction and intramedullary fixation with absorbable implants.
PREFERRED RESPONSE: 2
DISCUSSION: The patient has an unstable oblique fracture of the proximal phalanx that is easily reducible but unstable; therefore, the treatment of choice is closed reduction and percutaneous pin fixation, followed by casting. Closed reduction and percutaneous pin fixation offers a better functional result than open reduction and plate fixation. Repeat closed reduction and buddy taping is inadequate because of the inherently unstable fracture pattern. Buddy taping will allow the dislocation to recur. The other options represent more aggressive surgical techniques than are necessary to treat this fracture.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
88/. Figures 43a and 43b show the AP and lateral radiographs of the radius and ulna of a 9-year-old patient. The fracture is manipulated and placed in a long arm cast with the elbow flexed to 90 degrees and the forearm to neutral rotation. Figures 43c and 43d show the alignment of the fracture after the manipulation. What is the next most appropriate step in management?
1- Stabilize the present reduction internally with intramedullary pins.
2- Accept the present reduction and obtain follow-up radiographs in 1 week.
3- Remanipulate the fracture and place the forearm in pronation.
4- Remanipulate the fracture and place the forearm in supination.
5- Stabilize the present reduction with plates and screws.
PREFERRED RESPONSE: 4
DISCUSSION: By placing the forearm at neutral rotation, as shown in Figures 43c and 43d, the distal fragment has become malrotated by 90 degrees. This is evident by the fact that the bicipital tuberosity is rotated 90 degrees to the radial styloid. Normally, it should be directly opposite (180 degrees) to the radial styloid. The correct alignment was present in the original radiographs shown in Figures 43a and 43b. Another clue to the malrotation in the postreduction radiographs is the difference in the diameters of the opposing radial shafts. To correct this rotational malalignment, the distal fragment needs to be remanipulated into supination so that it is correctly aligned with the supinated proximal radius.
REFERENCES: Evans EM: Fractures of the radius and ulna. J Bone Joint Surg Br 1951;33:548-561.
Milch H: Roentgenographic differentiation between torsion and rotational fractures of the forearm. Bull Hosp Jt Dis 1949;10:216-225.
89/. Which of the following findings is an indication for adjunctive use of high-dose steroids?
1- C6 level injury secondary to a unilateral facet fracture-dislocation with weakness of wrist extension
2- C6 burst fracture with no neurologic deficit
3- L3 burst fracture with cauda equina syndrome
4- Incomplete spinal cord injury in a patient 24 hours after injury
5- Complete C6 level deficit in patient with spinal shock and a fracture-dislocation at C5 on C6 5 hours after injury
PREFERRED RESPONSE: 5
DISCUSSION: According to NASCIS III, the high-dose steroid protocol involves infusion of 30 mg/kg methylprednisolone followed by 5.4 mg/kg/h for 24 hours if the patient has sustained a spinal cord injury within the last 3 hours. The drip is continued for 48 hours if administration is started between 3 and 8 hours of the onset of neurologic deficit. No benefit has been conclusively demonstrated with steroids administered beginning 8 hours or longer after injury. Steroid use is not indicated for nerve root deficits, brachial plexus deficits, or gunshot wounds.
REFERENCES: Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 319-328.
Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury randomized controlled trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
90/. A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
1- Pulmonary embolism
2- Fat embolism syndrome
3- Sepsis
4- Pneumonia
5- Pneumothorax
PREFERRED RESPONSE: 2
DISCUSSION: The major criteria for the diagnosis of fat embolism syndrome include hypoxemia (PaO2 of less than 60 mm Hg), central nervous system depression, and a petechial rash that is most often located in the axillae, conjunctivae, and palate. The rash is often transient. Tachycardia, pyrexia, anemia, thrombocytopenia, and the presence of fat in the urine are all considered minor criteria. To establish the diagnosis of fat embolism syndrome, one major and four minor signs should be present. Pulmonary embolism, which is the major differential diagnosis, usually is not associated with conjunctival petechia or thrombocytopenia.
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
91/. Figure 45 shows the current radiograph of an 11-year-old girl who sustained a simple nondisplaced fracture of the distal radius 4 weeks ago. Management at the time of injury consisted of application of a short arm cast but no manipulation. What is the major concern at this time?
1- Stiffness of the wrist joint
2- Physeal growth arrest
3- Physeal overgrowth
4- Osteonecrosis of the metaphysis
5- Posttraumatic arthritis
PREFERRED RESPONSE: 2
DISCUSSION: The fracture pattern represents a Peterson type I physeal injury, which is a comminuted metaphyseal fracture in which the fracture lines extend up to the physis. Because there is no displacement of the physis and the fracture lines do not cross the physis, there may be a tendency to dismiss this injury as a simple metaphyseal fracture with no significant sequelae. A small percentage of patients (3% in Peterson’s series) experience growth arrest. In this patient, a disabling ulnar plus deformity, defined as increased ulnar length in relationship to the distal radius, developed.
REFERENCES: Peterson HA: Physeal fractures: Part 2. Two previously unclassified types. J Pediatr Orthop 1994;14:431-438.
Peterson HA: Physeal and apophyseal injuries, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 108-109.
92/. Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
1- Blood pressure
2- Urine output
3- Central venous pressure
4- Heart rate
5- Base deficit
PREFERRED RESPONSE: 5
DISCUSSION: The end point of resuscitation is adequate tissue perfusion and oxygenation. Blood lactate is the end point of anaerobic metabolism. The level of blood lactate reflects global hypoperfusion and is directly proportional to oxygen debt. Two separate prospective studies have verified a significant difference in mortality when blood lactate was used as a measure of resuscitation when compared to traditional parameters (mean arterial pressure, urine output, central venous pressure, and heart rate). Base deficit is a direct measure of metabolic acidosis and an indirect measure of blood lactate levels. It correlates well with organ dysfunction, mortality, and adequacy of resuscitation. It is easy to measure, can be obtained rapidly, and is an excellent assessment of the adequacy of resuscitation.
REFERENCES: Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Elliot DC: An evaluation of the end points of resuscitation. J Am Coll Surg 1998;187:536-547.
93/. A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
1- Immediately
2- When skin wrinkles are present and abrasions are epithelialized
3- Five days after injury
4- Following analysis of laser Doppler skin measurements
5- Following measurement of transcutaneous oxygen tension
PREFERRED RESPONSE: 2
DISCUSSION: Following any closed fracture, the most important determinant for the timing of surgery is the condition of the soft tissues and especially the skin. The best determinant of appropriate soft-tissue condition is the presence of wrinkling of the skin (wrinkle sign) at the site of the incision. A wrinkle sign is present when all the interstitial edema has left the skin; this may take up to 14 to 21 days of elevation. Any abrasion must be epithelialized so that there are no bacteria left at the site. To date, no other method of soft-tissue viability measurement has been shown to be of any clinical benefit.
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
94/. A 28-year-old woman sustained an injury to her dominant right arm after falling off her porch. Examination reveals a deformity at the elbow. She is neurovascularly intact. Figures 46a and 46b show the radiographs obtained before closed reduction, and postreduction radiographs are shown in Figure 46c and 46d. What is the most likely early complication?
1- Radial nerve injury
2- Intra-articular loose body causing a block to motion
3- Lack of active elbow flexion
4- Recurrent dislocation
5- Forearm compartment syndrome
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a complex fracture-dislocation of the elbow. The radial head is fractured, and there is a displaced coronoid fracture. These associated fractures indicate that the elbow is at high risk for recurrent instability after initial treatment. To prevent this complication, surgical treatment will most likely be required and will consist of some or all of the following: radial head open reduction and internal fixation or replacement, coronoid open reduction and internal fixation, medial and lateral ligament repairs, and even articulated external fixation. This patient was treated with open reduction and internal fixation of the radial head, and the elbow redislocated postoperatively.
REFERENCES: Ring D, Jupiter JB: Reconstruction of posttraumatic elbow instability. Clin Orthop 2000;370:44-56.
O’Driscoll SW: Classification and evaluation of recurrent instability of the elbow. Clin Orthop 2000;370:34-43.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxation and dislocation. Clin Orthop 1992;280:186-197.
95/. What is the most likely long-term sequela of the injury shown in Figures 47a and 47b?
1- Peroneal tendon instability
2- Ankle joint instability
3- Subtalar joint arthrosis
4- Ankle joint arthritis
5- Entrapment of the flexor hallucis longus tendon
PREFERRED RESPONSE: 3
DISCUSSION: The imaging studies show a comminuted lateral talar process fracture. This injury is often missed on plain radiographs; therefore, CT provides the best method of diagnostic evaluation. The most likely long-term sequela of this injury is subtalar joint arthrosis. Although this injury involves the fibular gutter region, progression to true ankle arthritis is unlikely. There does not appear to be any association with this injury and chronic mechanical instability of the ankle or disruption of the superior peroneal retinaculum and subsequent peroneal tendon instability. Entrapment of the flexor hallucis longus tendon may occur with fractures of the sustentaculum tali but not with injuries of the lateral talar process. Surgical management includes open reduction and internal fixation versus excision; the goal is preservation of the large articular surface fragments. In this patient, there is significant comminution and early fragment excision may be the best option for acute treatment.
REFERENCES: Tucker DJ, Feder JM, Boylan JP: Fractures of the lateral process of the talus: Two case reports and a comprehensive literature review. Foot Ankle Int 1998;19:641-646.
Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
96/. A 16-year-old high school football player has diffuse pain with attempted digital flexion after injuring the ring finger of the dominant hand 1 week ago. Examination reveals that he is unable to flex the distal interphalangeal joint. Management should consist of
1- surgical exploration and tendon reinsertion of the flexor digitorum profundis.
2- surgical exploration and tendon reinsertion of the flexor digitorum superficialis.
3- steroids and physical therapy.
4- surgical release of the anterior interosseous nerve.
5- surgical release of the median nerve.
PREFERRED RESPONSE: 1
DISCUSSION: The patient has an avulsion of the flexor digitorum profundus. Treatment should include surgical exploration and tendon reinsertion. This is not an avulsion of the flexor digitorum superficialis because the patient’s deficiency is the inability to flex the distal interphalangeal joint, not the proximal interphalangeal joint. Surgical release of the anterior interosseous nerve is not indicated because the flexor digitorum profundus of the ring finger is innervated by the ulnar nerve. A median nerve contusion causes wrist pain and/or numbness and tingling in the median nerve distribution.
REFERENCES: Strickland JW: Flexor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 1851-1897.
Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.
97/. A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. What type of injury pattern is shown?
1- Scaphoid fracture
2- Radiocarpal dislocation
3- Midcarpal dislocation
4- Transscaphoid dorsal perilunate dislocation
5- Volar lunate dislocation
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a transscaphoid dorsal perilunate dislocation. The radiographs clearly define a dorsal dislocation of the capitolunate joint, and the scaphoid fracture component is easily visible on the AP view. A scaphoid fracture alone is an unlikely diagnosis because of the midcarpal dislocation component. The radiocarpal joint is not dislocated because the lunate is sitting in the lunate fossa of the radius. Isolated radiocarpal dislocations are not associated with a midcarpal disruption. While a midcarpal dislocation is a component of a dorsal perilunate dislocation, this diagnosis does not address the scaphoid fracture. A volar lunate dislocation is not seen because the lunate is reduced in the lunate fossa of the distal radius. Volar lunate dislocations are in the spectrum of injury of perilunate dislocations and fracture-dislocations; however, the radiographs show a transscaphoid dorsal perilunate dislocation.
REFERENCES: Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
98/. A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of
1- closed reduction and a long arm cast.
2- closed reduction, percutaneous pin fixation, and a long arm cast.
3- closed reduction and an external fixator.
4- open reduction and internal fixation and soft-tissue repair.
5- proximal row carpectomy.
PREFERRED RESPONSE: 4
DISCUSSION: Open reduction and internal fixation is the treatment of choice for accurate reduction of the disrupted intercarpal ligaments. In addition, the displaced scaphoid fracture will require open reduction and internal fixation and possible bone grafting. Closed reduction and long arm casting will not allow accurate reduction of the dislocated intracarpal intervals, and it is unlikely to allow accurate reduction of the scaphoid. The maneuver required to effect closed reduction of a displaced scaphoid fracture will most likely cause the scaphoid lunate interval to displace. Closed reduction with percutaneous pin fixation or with an external fixator is unable to effect anatomic reduction of the injury. Proximal row carpectomy is used as a salvage procedure for a variety of degenerative and posttraumatic problems of the wrist.
REFERENCES: Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Sotereanos DG, Mitsionis GJ, Ginnakopoulos PN, Tomaino MM, Herndon JH: Perilunate dislocation and fracture dislocation: A critical analysis of the volar-dorsal approach. J Hand Surg Am 1997;22:49-56.
99/. A 17-year-old boy who fell on a pitchfork in a barn 1 day ago now has a painful, swollen forearm. Examination reveals erythema, exquisite tenderness, and crepitus to palpation of the forearm. He has a pulse rate of 110/min and a blood pressure of 80/60 mm Hg. Radiographs show subcutaneous air and no fractures. Gram stain of wound drainage reveals a gram-positive bacillus. The next most appropriate step in management should consist of
1- surgical debridement with wound closure and IV antibiotics.
2- surgical debridement with wound closure over suction drains and IV antibiotics.
3- surgical debridement with open wound management and IV antibiotics.
4- IV antibiotics alone.
5- hyperbaric oxygen therapy.
PREFERRED RESPONSE: 3
DISCUSSION: The successful treatment of necrotizing soft-tissue infections such as clostridial myonecrosis depends on prompt recognition and aggressive surgical debridement of all involved muscle, fascia, and soft tissue, resecting to a clearly normal healthy, viable margin. The effective antibiotic regimen for clostridial infection is high-dose penicillin; however, necrotizing infections are frequently polymicrobial so initially broad-spectrum antibiotics are indicated. Hyperbaric oxygen therapy may be used as an adjunct to surgical treatment but is insufficient as a primary therapy. Prolonged application of tourniquets and wound closure should be avoided.
REFERENCES: Pellegrini VD, Evarts CM: Complications, in Rockwood CA Jr, Green DP (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 365-370.
Gerding DN, Peterson LR: Infections caused by anaerobic bacteria, in Shulman ST, Phair JP, Peterson LR, Warren JR (eds): Infectious Diseases, ed 5. Philadelphia, PA, WB Saunders, 1997, pp 416-417.
Stephens DC: Myositis and fascitis, in Root RK (ed): Clinical Infectious Diseases, ed 1. Oxford, England, Oxford Press University, 1999, pp 769-770.
100. In the management of an open tibia fracture, what factor is considered most important in preventing deep infection?
1- Size of the skin lesion
2- Degree and the completeness of the debridement
3- Amount of contamination
4- Method of fixation
5- Cultures of the wound
PREFERRED RESPONSE: 2
DISCUSSION: The most important aspect of management of any open fracture, and in particular the tibia, is the degree and the completeness of the debridement of the soft tissue and most importantly, the muscle. The ultimate function is determined by the amount of muscle left, as well as the ability to heal. The amount of necrotic muscle left in the wound also determines the predisposition to infection. The method of fixation, the size of the wound, and the amount of contamination are controlled by the surgeon or the injury and have little to do with the long-term outcome. Initial wound cultures have little predictive value.
REFERENCES: Clifford P: Open fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 617-638.
Lee J: Efficacy of cultures in the management of open fractures. Clin Orthop 1997;339:71-75.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
REFERENCE: Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
3/. Figure 2 shows the lateral radiograph of an 8-year-old boy who sustained an acute injury to the elbow after falling down the stairs. Management should consist of
1- closed reduction, followed by a long arm cast in 120 degrees of flexion.
2- closed reduction, followed by percutaneous cross pin fixation.
3- open reduction and internal fixation using an oblique screw combined with an absorbable suture as a tension band.
4- a large intramedullary screw.
5- a long arm cast in full extension.
PREFERRED RESPONSE: 3
DISCUSSION: The patient has a flexion-type olecranon fracture, and the integrity of the extensor mechanism is disrupted. With this degree of displacement, closed reduction and extension casting would not be adequate. The strongest construct is an oblique screw across the fracture site, with a tension band. Healing is rapid in this age group; therefore one of the heavy absorbable sutures can be used as the tension band. Two parallel pins with the stainless steel tension band wire (AO technique) can be used but requires wire dissection for removal. Once the fracture is healed, the single screw can be removed easily with only a small incision. The presence of the screw, across the apophysis, has not been shown to produce any significant growth disturbance. Use of a large intramedullary screw would not be advisable because of the small size of the proximal fragment.
REFERENCES: Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Chambers HG, Wilkins KE: Part IV: Fractures of the proximal radius and ulna, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 629-630.
4/. A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of
1- open reduction and internal fixation via an anteromedial arthrotomy.
2- talectomy.
3- primary tibiotalocalcaneal arthrodesis.
4- open reduction and internal fixation via a medial malleolar osteotomy and limited anterior lateral arthrotomy.
5- closed reduction and a non-weight-bearing cast.
PREFERRED RESPONSE: 4
DISCUSSION: The radiographs show a comminuted talar body fracture. The goal of treatment is to minimize the risks of posttraumatic arthrosis of the ankle and subtalar joint and to maintain vascularity. Open reduction and internal fixation with an attempt at anatomic reduction will lead to improved outcomes. Attempting to repair this fracture via an arthrotomy only is extremely difficult, and the addition of a medial malleolar osteotomy is warranted. A limited anterior lateral arthrotomy with minimal soft-tissue stripping may assist with fixation of anterior-lateral and lateral fragments and allow better assessment of reduction of the major fracture line. Nonsurgical care would lead to inadequate reduction and increased risk of both ankle and hindfoot arthrosis. Talectomy and primary ankle and hindfoot arthrodesis should not be performed as primary surgical reconstructive options in this closed injury pattern.
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp
1465-1518.
Grob D, Simpson LA, Weber BG, Bray T: Operative treatment of displaced talus fractures. Clin Orthop 1985;199:88-96.
5/. Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?
1- Sacral fracture through the foramen
2- Sacral fracture through the ala
3- Sacroiliac joint dislocation
4- Reverse fracture-dislocation of the sacroiliac joint through the ilium
5- Iliac wing fracture
PREFERRED RESPONSE: 3
DISCUSSION: Although all of the above displaced injuries require reduction, the sacroiliac joint dislocation is a ligamentous injury. Without fixation, healing is unlikely and the result will be a painful dislocation. Both Holdsworth and Tile showed that the sacroiliac joint must be reduced anatomically and stabilized. The injuries through bone will unite fairly rapidly and, if reduced and stabilized with traction or external fixation, will generally result in an acceptable outcome unless modified by other associated problems such as neurologic injury.
REFERENCES: Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995.
Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
Henderson RC: The long-term results of nonoperatively treated major pelvic disruptions. J Orthop Trauma 1989;3:41-47.
6/. A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
1- Patellar sleeve fracture
2- Avulsion of the tibial tubercle
3- Avulsion of the anterior tibial spine
4- Osteochondral fracture of the femoral condyle
5- Osteochondral fracture of the patella
PREFERRED RESPONSE: 1
DISCUSSION: This is a typical patellar sleeve fracture. The patellar tendon avulses a portion of the distal bony patella, along with the retinaculum and articular cartilage from the inferior pole of the patella. It is common in children between ages 8 and 10 years. Anatomic reduction and repair of the extensor mechanism are mandatory to reestablish full knee extension.
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
7/. A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in
1- a painful nonunion.
2- asymptomatic nonunion.
3- chronic elbow instability.
4- tardy ulnar nerve palsy.
5- cubitus varus.
PREFERRED RESPONSE: 2
DISCUSSION: The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures.
REFERENCES: Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Farsetti P, Potenza V, Caterini R, Ippolito E: Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;83:1299-1305.
8/. Which of the following factors is considered most important when assessing an ankle fracture for surgical treatment?
1- Level of the fibular fracture
2- Displacement of the fibular fracture
3- Size of the posterior malleolus
4- Position of the talus in the mortise
5- Rupture of the deltoid ligament
PREFERRED RESPONSE: 4
DISCUSSION: Although all of these factors may influence the decision to perform surgery, the most important is the position of the talus in the mortise. The goal of treatment of ankle fractures is to maintain the talus centered in the mortise. If it is in this position, the other factors do not enter into the decision to intervene surgically.
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
9/. A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindfoot deformity. A lateral radiograph is shown in Figure 6. Surgical reconstruction is best accomplished with
1- calcaneal osteotomy.
2- subtalar joint arthrodesis.
3- triple arthrodesis.
4- pantalar arthrodesis.
5- distraction bone block arthrodesis.
PREFERRED RESPONSE: 2
DISCUSSION: The patient has posttraumatic subtalar joint arthrosis that developed following a calcaneal fracture. Because there is no hindfoot deformity, in situ subtalar joint arthrodesis is the treatment of choice. Calcaneal osteotomy or distraction bone block arthrodesis is beneficial in patients with severe talar dorsiflexion or malunion of the calcaneal body. Triple arthrodesis is not warranted without changes at the transverse tarsal joint, and typically even with injury into the calcaneocuboid joint, this joint is often asymptomatic. Pantalar arthrodesis is not indicated as the pathology is occurring at the subtalar joint and not in the ankle joint.
REFERENCES: Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 1422-1464.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Chandler JT, Bonar SK, Anderson RB, Davis WH: Results of in situ subtalar arthrodesis for late sequelae of calcaneus fractures. Foot Ankle Int 1999;20:18-24.
10/. Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?
1- Respiratory depression
2- Increased salivary secretion
3- Hypertension
4- Emergence phenomena
5- Cerebral vasoconstriction
PREFERRED RESPONSE: 2
DISCUSSION: The most common deleterious side effect of ketamine is increased salivation and tracheobronchial secretions. For this reason, an antisialagogue agent should be given. While lack of sufficient respiratory depression is one of the major advantages of using ketamine, apnea can occur if the drug is given too rapidly intravenously. Emergence phenomena is common in adults but relatively rare in children.
REFERENCES: Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63.
White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
McCarty EC, Mencio GA, Walker LA, Green NE: Ketamine sedation for the reduction of children’s fractures in the emergency department. J Bone Joint Surg Am 2000;82:912-918.
11/. Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Figure 7c. Following gradual progression of weight bearing, she reports that she slipped again and placed full weight on the extremity. She now notes a new onset of increased pain in her left thigh and hip region. Follow-up radiographs are shown in Figures 7d and 7e. Reconstruction should consist of
1- conversion to a longer side plate with the same compression screw and tube angle.
2- in situ bone grafting.
3- hardware removal and reconstruction with an intramedullary device that provides fixation into the femoral head and neck.
4- hardware removal and retrograde femoral nailing.
5- revision reconstruction with cerclage wiring.
PREFERRED RESPONSE: 3
DISCUSSION: The initial fracture was an unstable reverse oblique intertrochanteric fracture with subtrochanteric extension. Initial fixation with a high-angled screw and side plate construct may not provide stability as well as a 95 degree fixed-angle device or a intramedullary hip screw device. The follow-up radiographs show loss of fixation and further propagation of the fracture distally. Reconstruction would best be accomplished with hardware removal and conversion to a long intramedullary nail with femoral head fixation or a 95 degree angled plate and screw device. Conversion to a longer plate does not improve the biomechanical situation at the primary fracture site. In situ bone grafting would not provide any additional stability and would not correct the deformity. The proximal femoral fracture is not amenable to retrograde nailing. Cerclage wiring will not sufficiently enhance stability and is not indicated.
REFERENCES: Bridle SH, Patel AD, Bircher M, Calvert PT: Fixation of intertrochanteric fractures of the femur: A randomized prospective comparison of a gamma nail and dynamic hip screw. J Bone Joint Surg Br 1991;73:330-334.
DeLee JC: Fractures and dislocations of the hip, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1659-1825.
Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
12/. An intoxicated 68-year-old man fell at home. Examination reveals abrasions on his forehead, 2/5 weakness of his hand intrinsics and finger flexors, and 4/5 strength of the deltoid, biceps, and triceps bilaterally. Lower extremity motor function is 5/5. Sensory examination to pain and temperature is diminished in his hands but intact in his lower extremities. Deep tendon reflexes are depressed in all four extremities, but perianal sensation and rectal tone are intact. Foley catheterization yields 700 mL of urine. Radiographs of the cervical spine reveal multilevel spondylosis without fracture or subluxation. An MRI scan reveals high-intensity signal change within the cord substance at C5. What is the most likely diagnosis?
1- Brown-Sequard syndrome
2- Central cord syndrome
3- Anterior cord syndrome
4- Posterior cord syndrome
5- Bilateral brachial plexus palsy
PREFERRED RESPONSE: 2
DISCUSSION: Central cord syndrome is characterized by greater neurologic involvement of the upper extremities than the lower extremities. This is typically seen in older patients with cervical spondylosis without associated bony injury or joint subluxation. The prognosis for recovery is fair. Patients with Brown-Sequard syndrome have an ipsilateral motor deficit and contralateral loss of pain and temperature. Prognosis for recovery depends on the mechanism of injury, which is often of a penetrating nature. Anterior cord syndrome results from anterior compression such as occurs with a burst or teardrop fracture of the vertebral body; patients have bilateral motor loss, pain, and temperature loss with preservation of proprioception and vibratory sensation (posterior column function). The prognosis for recovery is generally poor. Posterior cord syndrome is rare and is associated with loss of posterior column function (proprioception and vibration).
REFERENCES: Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 541-549.
Schneider RC, Thompson JM, Rebin J: The syndrome of acute central cervical spinal cord injury. J Neurol Neurosurg Psychiatry 1958;21:216-227.
13/. A 23-year-old woman sustains an injury to her right hand after falling off her snowboard. Examination reveals that she has difficulty moving her fingers. A radiograph and a clinical photograph are shown in Figures 8a and Figure 8b. Management should consist of
1- closed reduction and buddy taping.
2- in situ pinning.
3- open reduction and internal fixation.
4- casting for 6 weeks.
5- dynamic extension splinting.
PREFERRED RESPONSE: 3
DISCUSSION: The radiograph reveals oblique fractures of the third and fourth metacarpals. The rotational component of the fracture displacement is well visualized on the clinical photograph, which shows scissoring of the middle finger over the ring finger. The fracture obliquity results in rotational deformity that cannot be adequately maintained and held by closed treatment. The treatment of choice is open reduction and internal fixation.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Freeland AE, Benoist LA, Melancon KP: Parallel miniature screw fixation of spiral and long oblique hand phalangeal fractures. Orthopedics 1994;17:199-200.
Freeland AE, Geissler WB: Plate fixation of metacarpal shaft fractures, in Blair WF (ed): Techniques in Hand Surgery. Baltimore, MD, Williams and Wilkins, 1996, pp 255-264.
14/. A 32-year-old man sustained an L1 burst fracture with 90% canal compromise, intact posterior elements, and kyphosis of 25% at the L1 level. He has an incomplete neurologic injury. Definitive management should consist of
1- bed rest for 8 weeks, followed by mobilization in a total contact thoracolumbosacral orthosis.
2- immediate laminectomy only.
3- anterior decompression, vertebral body reconstruction, and stabilization.
4- in situ posterior fusion.
5- short segment posterior fixation and fusion.
PREFERRED RESPONSE: 3
DISCUSSION: With an incomplete injury, the best chance for recovery occurs when the canal is cleared and the neural structures are decompressed. Anterior decompression, vertebral body reconstruction, and anterior stabilization have been shown to be highly effective in the treatment of burst-type injuries. Laminectomy alone is contraindicated because it increases the instability. Short segment posterior fixation has a high rate of failure in this type of injury at this level.
REFERENCES: Kaneda K, Abumi K: Burst fractures with neurologic deficits of the thoracolumbar spine. J Bone Joint Surg Am 1997;79:69-83.
McGuire R Jr: The role of anterior surgery in the treatment of thoracolumbar fractures. Orthopedics 1997;20:959-962.
15/. The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?
1- Anatomic alignment
2- Indirect reduction
3- Anatomic reduction of the fragments
4- Relatively stable fixation
5- Functional aftercare
PREFERRED RESPONSE: 3
DISCUSSION: Although the original concept of internal fixation was one of anatomic reduction and stable fixation, over the past 10 to 15 years there has been a change based on the advent of intramedullary nailing and bridge plating. It is now appreciated that in a multifragmentary diaphyseal fracture, particularly of the lower extremity, the achievement of axis alignment (mechanical and anatomic axis) is all that is required. Healing will occur by callus. Relatively stable fixation is achieved through intramedullary nailing or bridge plating, providing adequate pain relief for functional aftercare.
REFERENCES: Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000,
pp 7-32.
deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Mast J, Jakob R, Ganz R: Planning and Reduction Techniques in Fracture Surgery. Berlin, Springer-Verlag, 1989.
16/. A 68-year-old woman who sustained a closed distal tibia fracture 2 years ago was initially treated with an external fixator across the ankle for 12 weeks, followed by intramedullary nailing of the fibula and lag screw fixation of the tibia. She continued to report persistent pain so she was treated with a brace and a bone stimulator. She now reports pain in her ankle. Examination reveals ankle range of motion of 8 degrees of dorsiflexion to 25 degrees of plantar flexion. She is neurovascularly intact. Current radiographs are shown in Figures 9a through 9c. What is the next most appropriate step in management?
1- A cast and weight bearing as tolerated
2- A brace and an ultrasound bone stimulator
3- Intramedullary nailing
4- Open reduction and plate fixation with bone grafting
5- Fibular osteotomy
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a nonunion of the distal fifth of the tibia. The nonunion appears to be oligotrophic, somewhere between atrophic and hypertrophic. Management requires stabilization and stimulation of the local biology, which can be accomplished with open reduction and internal fixation with bone grafting. Bracing or casting does not provide enough stability. Ultrasound bone stimulation has been shown to speed fresh fracture repair but is not indicated in nonunions. The distal segment is too short for intramedullary nailing. A fibular osteotomy alone would increase instability and, even with prolonged casting, would be unlikely to lead to successful repair.
REFERENCES: Carpenter CA, Jupiter JB: Blade plate reconstruction of metaphyseal nonunion of the tibia. Clin Orthop 1996;332:23-28.
Lonner JH, Siliski JM, Jupiter JB, Lhowe DW: Posttraumatic nonunion of the proximal tibial metaphysis. Am J Orthop 1999;28:523-528.
Stevenson S: Enhancement of fracture healing with autogenous and allogeneic bone grafts. Clin Orthop 1998;355:S239-S246.
Wiss DA, Johnson DL, Miao M: Compression plating for non-union after failed external fixation of open tibial fractures. J Bone Joint Surg Am 1992;74:1279-1285.
17/. A patient has a displaced midshaft transverse fracture of the humerus and is neurologically intact. Following closed reduction and application of a coaptation splint, the patient cannot dorsiflex the wrist or the fingers at the metacarpophalangeal joints of the hand. What is the next most appropriate step in management?
1- Observation with a high expectation for recovery
2- Observation for 1 week, followed by exploration if recovery is not evident
3- Immediate exploration of the radial nerve and fracture fixation
4- Immediate exploration of the radial nerve without fracture fixation
5- Removal of the coaptation splint and repeat reduction
PREFERRED RESPONSE: 1
DISCUSSION: The answer to this question is controversial. All of the standard textbooks state that development of a radial nerve palsy during initial fracture management may represent a laceration or injury of the nerve by bone fragments at the time of manipulation; therefore, surgery should be considered. However, it appears that there is no scientific basis for this decision. A review of the available literature shows that the results were the same for patients who were observed as for those who underwent radial nerve exploration. The indications for surgical exploration include palsies associated with open fractures, irreducible closed fractures, and vascular injuries. The only other relative indication for surgical exploration is following manipulation of a Holstein-Lewis fracture (a distal third fracture of the humerus with a lateral spike). In this type of fracture, exploration may be necessary if a closed reduction leads to radial nerve palsy because the spike may lacerate or compress the nerve. Observation for return of nerve function may be appropriate for 3 months or longer prior to considering late exploration.
REFERENCES: Bostman O, Bakalim G, Vainionpaa S, Wilppula E, Patiala H, Rokkanen P: Radial palsy in shaft fracture of the humerus. Acta Orthop Scand 1986;57:316-319.
Shaz JJ, Bhatti NA: Radial nerve paralysis associated with the fractures of the humerus: A review of 62 cases. Clin Orthop 1983;172:171-176.
Holstein A, Lewis GB: Fractures of the humerus with radial nerve paralysis. J Bone Joint Surg Am 1963;458:1382-1388.
18/. A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
1- External fixation
2- Plate fixation
3- Unreamed unlocked intramedullary nailing
4- Reamed statically locked intramedullary nailing
5- Reamed unlocked nailing
PREFERRED RESPONSE: 1
DISCUSSION: A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient’s femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing.
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
19/. Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?
1- Distal femoral pin and 90-90 traction for 3 weeks, followed by a spica cast
2- Closed reduction and stabilization with an external fixator
3- Closed reduction and stabilization with an interlocking nail
4- Closed reduction and stabilization with multiple flexible intramedullary nails
5- Open reduction and stabilization with a plate and screws
PREFERRED RESPONSE: 4
DISCUSSION: Because the patient has a transverse midshaft fracture with no evidence of comminution, the treatment of choice is closed reduction and stabilization with flexible intramedullary nails. Transverse fractures treated with an external fixator heal with poor callus and have a high refracture rate. In addition, the pin tracks produce undesirable and excessive scarring. Femoral pin traction is safe and effective but results in considerable muscle wasting and a slow return to function. Interlocking nails run the risk of greater trochanteric growth disturbance and/or osteonecrosis of the femoral head in this age group. Plate fixation, while effective, requires considerable tissue dissection with large scar formation. It also requires a rather extensive dissection for later plate removal.
REFERENCES: Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Heinrich SD, Drvaric D, Darr K, MacEwen GD: Stabilization of pediatric diaphyseal femoral fractures with flexible intramedullary nails (a technique paper). J Orthop Trauma 1992;6:452-459.
20/. A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of
1- open reduction and internal fixation with bone grafting.
2- closed reduction and percutaneous pin fixation.
3- aspiration and steroid injection.
4- closed manipulation and a long arm cast.
5- in situ open bone grafting.
PREFERRED RESPONSE: 1
DISCUSSION: The patient has a scaphoid fracture with cystic resorption of the distal aspect of the midthird of the scaphoid. This fracture is unlikely to heal without intervention. Percutaneous pinning, closed manipulation, and bone grafting will not restore alignment. Treatment requires restoration of scaphoid length, bone grafting, and internal fixation to obtain healing with normal alignment.
REFERENCES: Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650.
Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737.
Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am
1988;70:982-991.
Feldman MD, Manske PR, Welch RL, Szerzinski JM: Evaluation of Herbert screw fixation for the treatment of displaced scaphoid nonunions. Orthopedics 1997;20:325-328.
21/. A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
1- Loss of reduction of the ulnar physis
2- Loss of reduction of the radial metaphysis
3- Physeal arrest of the distal radius
4- Physeal arrest of the distal ulna
5- Osteonecrosis of the ulnar epiphysis
PREFERRED RESPONSE: 4
DISCUSSION: While injury of the distal radial metaphysis is a rather common occurrence, the incidence of physeal arrest is only about 4% to 5% of patients. While injury of the distal physis of the ulna is rare, the incidence of physeal arrest is greater than 50% in fractures of this structure. These patients need to be followed closely both clinically and radiographically to look for the signs of distal ulnar/physeal arrest such as loss of the prominence of the ulna and ulnar deviation of the hand. Radiographically, progressive shortening of the ulna is observed.
REFERENCES: Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, pp 632-635.
22/. A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of
1- mobilization in a kinetic therapy bed for 8 weeks.
2- initiation of a steroid protocol.
3- immediate laminectomy of T7, T8, and T9.
4- application of a total contact orthosis.
5- open reduction and posterior segmental stabilization and grafting.
PREFERRED RESPONSE: 5
DISCUSSION: With a complete injury in the thoracic spinal cord, the likelihood of neurologic recovery is small. If possible, treatment should be planned to allow rapid mobilization and rehabilitation without the use of braces and their associated skin problems. The use of long segment fixation provides for rapid mobilization without having to use braces postoperatively. The use of steroid protocol is controversial and should be considered only if it can be started within 8 hours of the injury. Laminectomy is contraindicated because it will increase instability.
REFERENCE: Tasdemiroglu E, Tibbs PA: Long-term follow-up results of thoracolumbar fractures after posterior instrumentation. Spine 1995;20:1704-1708.
23/. A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of
1- skeletal tong traction for 6 weeks.
2- halo application.
3- immobilization in a rigid collar for 6 weeks.
4- open reduction posteriorly with interspinous wiring and bone grafting.
5- open reduction anteriorly with diskectomy, interbody grafting, and plating.
PREFERRED RESPONSE: 3
DISCUSSION: The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
REFERENCE: Clarke CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
24/. A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
1- Inflation of the abdominal portion of the PASG
2- Application of a pelvic clamp
3- Application of a pelvic external fixator
4- Rapid infusion of 4 more units of blood
5- Angiography and embolization
PREFERRED RESPONSE: 5
DISCUSSION: There is no identifiable thoracic, abdominal, or long bone source of ongoing bleeding. The patient has a lateral compression Burgess-Young type I pelvic ring injury. This injury does not increase the pelvic volume because it is not unstable in external rotation. Application of a PASG, a pelvic clamp, or an external fixator may be helpful if the patient has a pelvic injury that is unstable in external rotation or translation but would be of little use in this injury pattern. Persistent hemodynamic instability after administration of 4 units of blood is the decision point where most authors would recommend angiography and embolization. If the pelvis is unstable in external rotation or translation, inflation of the PASG trousers or application of an external fixator is recommended before angiography. Attributing the hemodynamic instability to the head injury before ruling out the pelvis as a source is not indicated.
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
25/. A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?
1- Visualization of the articular surface
2- Avoidance of an olecranon osteotomy
3- A muscle-sparing approach
4- The likelihood a total elbow arthroplasty will be performed
5- The likelihood that reconstruction of the anterior elbow joint will be performed
PREFERRED RESPONSE: 1
DISCUSSION: When managing a complex intra-articular fracture, it is imperative that there is adequate visualization of the joint; this usually means an extensile approach. At the elbow, this is usually through a transolecranon osteotomy. The recent addition of a muscle-sparing approach as described by Bryan and Morrey has gained popularity, but it is difficult to maintain soft-tissue viability and it may put the ulnar nerve at risk. A triceps-splitting approach, which can be used for simple single articular splits into the joint where extra-articular reduction is available, is possible and good results have been reported. To date, there is minimal data on these alternative approaches for comminuted intra-articular distal humeral fractures.
REFERENCES: McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522
McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop
2000;370:19-33.
Bryan RS, Morrey BF: Extensive posterior exposure of the elbow: A triceps-sparing approach. Clin Orthop 1982;166:188-192.
26/. The use of nasotracheal intubation for airway management is contraindicated in the acute multiply injured patient when the patient has
1- suspected cervical spine trauma.
2- head injuries and spontaneous respirations.
3- respiratory arrest.
4- a need for prolonged ventilatory support.
5- a hemopneumothorax.
PREFERRED RESPONSE: 3
DISCUSSION: The use of nasotracheal intubation is less desirable in patients with respiratory arrest because placement of the tube is most reliable when the patient is breathing. Nasotracheal intubation is advantageous in patients with suspected cervical spine trauma because it does not require hyperextension of the neck. A nasotracheal tube may be more comfortable than an orally placed tube because it is fixed at several points and moves less freely within the larynx, subglottic area, and trachea. The presence of a hemothorax or pneumothorax does not affect the choice of airway control but does require placement of a chest tube.
REFERENCES: Colice GL: Prolonged intubation versus tracheostomy in the adult. J Intern Care Med 1987;2:85.
Shackford S: Spine injury in the polytrauma patient: General surgical and orthopaedic considerations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 9-15.
27/. A 65-year man has right hip pain after a fall. Radiographs reveal a reverse oblique intertrochanteric femoral fracture. Treatment consists of reduction and internal fixation. Which of the following implants is most commonly associated with nonunion and hardware failure?
1- Sliding hip screw
2- Dynamic condylar screw
3- 95 blade plate
4- Cephalomedullary nail
5- Intramedullary hip screw
PREFERRED RESPONSE: 1
DISCUSSION: Reverse oblique intertrochanteric femoral fractures account for 5% of all intertrochanteric or subtrochanteric fractures. They are uncommon but not rare and will be encountered in practice. The sliding hip screw is associated with the most problems because of its design. When reverse oblique fractures are fixed with a sliding hip screw, the action of the construct causes medial displacement of the distal fragment rather than compression of the proximal and distal fragments. All of the other implants prevent medial displacement of the distal segment. It should not be assumed that simply using one of the other implants is reason for success. There is a significant failure rate for each of these implants with reverse oblique fractures. The implant must be ideally placed and the fracture must be reduced.
REFERENCES: Haidukewych GJ, Israel TA, Berry DB: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Baumgaertner MR, Chrostowski JH, Levy RN: Intertrochanteric hip fracture, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1833-1881.
28/. Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?
1- Wedge the cast to correct angulation.
2- Accept the present alignment and continue follow-up.
3- Perform open reduction and internal fixation of both the radius and ulna with plates and screws.
4- Perform open reduction and internal fixation of both the radius and ulna with intramedullary rods.
5- Remanipulate both the radius and ulna and stabilize with an external fixator.
PREFERRED RESPONSE: 2
DISCUSSION: Bayonet apposition of the radius and ulnar shafts is quite acceptable, as long as the angulation is less than 10 degrees. The rotation must be acceptable as well. This patient went on to full healing, with full supination and pronation of the forearm and no cosmetic deformity.
REFERENCES: Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Vittas D, Larsen E, Torp-Pedersen S: Angular remodeling of midshaft forearm fractures in children. Clin Orthop 1991;265:261-264.
29/. In Figure 14, the primary fracture line in a calcaneal fracture is best depicted by which of the following schematics?
1- A
2- B
3- C
4- D
5- E
PREFERRED RESPONSE: 1
DISCUSSION: The schematic labeled A best depicts the primary fracture line in a calcaneal fracture. The primary fracture line in an axial-loading fracture of the calcaneus occurs from superior-lateral to inferior-medial. This fracture line separates the calcaneus into sustentacular and tuberosity fragments and typically enters the subtalar joint through the posterior facet. Although additional fracture lines typically occur, the primary fracture line is almost always present. If surgical reduction is planned, reducing the primary fracture is always a key step.
REFERENCES: Macey LR, Benirschke SK, Sangeorzan BJ, Hansen ST: Acute calcaneal fractures: Treatment option and results. J Am Acad Orthop Surg 1994;2:36-43.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
30/. A 45-year-old man who sustains a medial subtalar dislocation while playing basketball undergoes immediate closed reduction. No fractures or osteochondral defects are noted on postreduction radiographs. The next most appropriate step in management should consist of
1- a long leg cast for 6 weeks.
2- an ankle support and return to activities.
3- a short leg cast for 4 weeks.
4- open repair of ligaments and active range of motion.
5- open repair of ligaments and casting for 6 weeks.
PREFERRED RESPONSE: 3
DISCUSSION: Most subtalar dislocations can be easily reduced by closed methods. If no fractures or defects are seen on the postreduction radiographs, then the success rate with cast immobilization is good. Medial dislocations have a better prognosis than lateral dislocations. Late instability is rare; therefore, the duration of immobilization should not be excessive. Most subtalar dislocations result in some stiffening of the hindfoot, and painful degenerative arthrosis is the most common serious complication.
REFERENCE: Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
31/. A 21-year-old woman sustained a minimally displaced traumatic spondylolisthesis of C2 (Hangman’s fracture) after striking the windshield with her forehead during a motor vehicle accident. Management should consist of
1- skeletal tong traction for 6 weeks.
2- anterior C2-3 diskectomy, grafting, and plate fixation.
3- halo application for 8 weeks.
4- a rigid collar for 4 to 6 weeks, followed by mobilization.
5- posterior stabilization with C2 pedicle screws.
PREFERRED RESPONSE: 4
DISCUSSION: According to the classification of Levine and Edwards, a type I Hangman’s fracture is minimally displaced without angulation and represents a stable injury. Good clinical success has been achieved with nonsurgical management consisting of use of a rigid collar until the patient reports pain relief, followed by quick mobilization.
REFERENCE: Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
32/. A 25-year-old patient who sustained multiple bilateral rib fractures, a pulmonary contusion, a left nondisplaced transtectal acetabular fracture, and a closed humerus fracture in a motor vehicle accident 2 weeks ago is transferred from another hospital. The humerus fracture has been surgically treated. There are no signs of infection, and the trauma surgeon wants to mobilize the patient as soon as possible. Radiographs are shown in Figures 15a and 15b. Management of the humerus fracture should consist of
1- open reduction and plate fixation.
2- a humeral fracture brace.
3- a locking intramedullary nail.
4- insertion of at least two additional pins.
5- removal of the pins and a long arm hanging cast.
PREFERRED RESPONSE: 1
DISCUSSION: The radiographs show a distal third humerus fracture that is angulated, rotated, and not rigidly fixed. Rigid fixation is needed because mobilization is highly desirable to improve pulmonary function. The acetabular fracture is through the weight-bearing dome but is nondisplaced. Nonsurgical management of the acetabular fracture requires at least 6 weeks of touchdown weight bearing to minimize the forces across the hip joint. Open reduction and plate fixation would achieve anatomic reduction and immediate mobilization. A single posterolateral 4.5-mm plate or two 3.5-mm plates at 90 degrees are possible alternatives. Immediate weight bearing on a plated humerus fracture with the use of crutches or a walker has been shown to be safe and would allow touchdown weight bearing, protecting the hip. None of the other options would achieve this goal for this distal fracture.
REFERENCE: Tingstad EM, Wolinsky PR, Shyr Y, Johnson KD: Effect of immediate weightbearing on plated fractures of the humeral shaft. J Trauma 2000;49:278-280.
33/. Figure 16 shows the radiograph of a 23-year-old man who has severe right shoulder pain after his motorcyle hit a bridge guardrail. He is neurologically intact. Nonsurgical management will most likely result in
1- nonunion of the clavicle or glenoid.
2- thoracic outlet syndrome.
3- less than 50% range of motion compared with the contralateral shoulder.
4- less than 50% strength compared with the contralateral shoulder.
5- high patient satisfaction and good shoulder function.
PREFERRED RESPONSE: 5
DISCUSSION: Internal fixation of the clavicle, glenoid, or both has been recommended for fractures of the clavicle and glenoid neck (floating shoulders). Recently, the inherent instability of these dual fractures has been questioned in a biomechanical model without further disruption of the coracoclavicular or acromioclavicular ligamentous structures. Nonsurgical management of the majority of combined scapular/glenoid fractures in patients with less than 10 mm of displacement has resulted in excellent shoulder function and will most likely achieve an excellent result in this patient.
REFERENCES: Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF: The floating shoulder: Clinical and functional results. J Bone Joint Surg Am 2001;83:1188-1194.
Williams GR Jr, Naranja J, Klimkiewicz J, et al: The floating shoulder: A biomechanical basis for classification and management. J Bone Joint Surg Am 2001;83:1182-1187.
Edwards SG, Whittle AP, Wood GW: Nonoperative treatment of ipsilateral fractures of the scapular and clavicle. J Bone Joint Surg Am 2000;82:774-779.
34/. An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
1- Unreamed intramedullary nail
2- Reamed statically locked intramedullary nail
3- External fixation
4- Plate fixation and interfragmentary compression
5- Bridge plate stabilization
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a simple fracture pattern that can be reduced anatomically and stabilized with absolute stability by interfragmental compression and protection plating. This will guarantee a 95% to 98% union rate with no radial nerve palsy. Intramedullary nailing does not equal these results in a simple fracture pattern in the humerus. Bridge plating is indicated for multifragmented fracture patterns when anatomic reduction and absolute stability cannot be achieved. External fixation is reserved for severe open fractures.
REFERENCES: Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
35/. A 28-year-old painter has had increasing pain in his hand and forearm after sustaining a paint injection wound to the tip of his left index finger 24 hours ago. Management should consist of
1- hospital admission and IV antibiotics.
2- emergent surgical debridement.
3- oral antibiotics, splinting, and elevation.
4- nonsteroidal anti-inflammatory drugs and splinting.
5- oral antibiotics and a tetanus shot.
PREFERRED RESPONSE: 2
DISCUSSION: The clinical presentation soon after injury may be surprisingly innocuous, but all high-pressure injection injuries of various materials are best treated by emergent surgical debridement of all foreign material from the flexor tendon sheath as well as the subcutaneous tissues. Subsequent hospital admission, IV antibiotics, and possible repeat debridements usually are necessary. The use of antibiotics alone is inadequate treatment of this severe injury.
REFERENCES: Pinto MR, Turkula-Pinto LE, Cooney WP, Wood MB, Dobyns JH: High-pressure injection injuries of the hand: Review of 25 patients managed by open wound technique. J Hand Surg Am 1993;18:125-130.
Urbaniak JR, Evans JP, Bright DS: Microvascular management of ring avulsion injuries. J Hand Surg Am 1981;6:25-30.
Tsai TM, Manstein C, DuBou R, Wolff T, Kutz JE, Kleinert HE: Primary microsurgical repair of ring avulsion amputation injuries. J Hand Surg Am 1984;9:68-72.
Kay S, Werntz J, Wolff T: Ring avulsion injuries: Classification and prognosis. J Hand Surg Am 1989;14:204-213.
Schnall SB, Mirzayan R: High-pressure injection injuries to the hand, in Kozin SH (ed): Hand Clinics: Upper Extremity Trauma. Philadelphia, PA, 1999, pp 245-248.
36/. A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?
1- Posterior tibial tendon
2- Impaction fracture of the head of the talus
3- Posterior tibial neurovascular bundle
4- Achilles tendon
5- Calcaneus fracture
PREFERRED RESPONSE: 2
DISCUSSION: The patient has a medial subtalar dislocation. These injuries should be reduced as soon as possible to minimize risk to the skin. Most often, this can be done easily, and further radiographic evaluation then can be performed as necessary. On rare occasions, closed reduction is not possible because of fractures of the articular surface of the talus, navicular, interposed extensor digitorum brevis, or transverse fibers of the cruciate crural ligament. The posterior tibial tendon is the most common obstruction to closed reduction in lateral subtalar dislocations, which are less common than medial dislocations. The majority of both injuries can be managed by closed reduction and immobilization.
REFERENCES: Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863.
Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
37/. A 27-year-old woman sustained a bilateral C5-6 facet subluxation in a motor vehicle accident. Neurologic evaluation reveals normal motor, sensory, and reflex functions. She is awake, alert, and cooperative. Initial management should consist of
1- halo application.
2- skeletal traction and attempted closed reduction.
3- a soft cervical collar.
4- immediate transfer to the operating room for closed reduction.
5- immediate transfer to the operating room for open reduction and
stabilization posteriorly.
PREFERRED RESPONSE: 2
DISCUSSION: As long as the patient is alert and cooperative, an attempt can be made to reduce the dislocation. This should not be attempted in a patient who is obtunded, comatose, or uncooperative. If any neurologic changes are noted during the reduction maneuver, the attempt should be stopped, appropriate radiographic studies obtained, and open reduction and stabilization planned in the operating room.
REFERENCE: Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case reports. J Bone Joint Surg Am 1991;73:1555-1560.
38/. A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of
1- indirect fracture reduction via traction and early mobilization.
2- volar plate arthroplasty.
3- open reduction and internal fixation.
4- closed reduction and percutaneous pin fixation.
5- cast immobilization.
PREFERRED RESPONSE: 1
DISCUSSION: This fracture, known as a pilon fracture, represents comminution of the base of the middle phalanx with both palmar and dorsal cortical disruption. The treatment method that allows the best function and fewest complications is indirect reduction achieved through specific dynamic splinting or the use of specifically designed proximal interphalangeal joint external fixators. Early mobilization can be achieved by either of these techniques. Volar plate arthroplasty is indicated for a simple fracture-dislocation of the proximal interphalangeal joint with comminution of the volar fracture fragment and dorsal dislocation of the remaining articular surface. Open reduction and internal fixation or percutaneous pinning adds surgical risks and scarring and typically will not provide added stability. Cast immobilization will not achieve the goal of early range of motion.
REFERENCES: Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Krakauer JD, Stern PJ: Hinged device for fractures involving the proximal interphalangeal joint. Clin Orthop 1996;327:29-37.
39/. Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of
1- early motion and muscle strengthening.
2- immobilization in a thumb spica cast with the thumb abducted.
3- open reduction and internal fixation through a volar approach.
4- open reduction and internal fixation through a dorsal approach.
5- closed reduction and percutaneous pin fixation.
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a Salter-Harris type III fracture of the proximal phalanx of the thumb. It is usually caused by an abduction injury where the ulnar collateral ligament avulses a fragment away from the proximal epiphysis and is the most common childhood gamekeeper’s injury. If there is greater than 1 mm of separation or a significant articular step-off, an open reduction, performed through an extensor aponeurosis-splitting approach, is required to reestablish joint congruity and stability. Percutaneous or closed methods of reduction are usually ineffective. The dorsal approach avoids the volar neurovascular structures. Since the ulnar collateral ligament is still attached, this area does not need to be visualized. The major goal is to reestablish joint congruity and bony stability. This can be easily performed via the dorsal approach.
REFERENCES: Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, p 668.
40/. Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of
1- a long arm cast.
2- immediate functional bracing.
3- closed reduction and percutaneous pin fixation.
4- percutaneous olecranon pin traction.
5- total elbow arthroplasty.
PREFERRED RESPONSE: 5
DISCUSSION: The radiographs reveal a severely comminuted distal humerus fracture. A long arm cast, functional bracing, and closed reduction and percutaneous pin fixation all have a poor outcome and could result in a nonunion that will be very difficult to treat. Open reduction and internal fixation is indicated in most supracondylar humerus fractures, but total elbow arthroplasty is a good alternative in elderly patients who have multiple medical problems and when the fracture pattern may preclude stable enough internal fixation to allow postoperative motion.
REFERENCES: Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Morrey BF: Fractures of the distal humerus: Role of elbow replacement. Orthop Clin North Am 2001;31:145-155.
41/. An 18-year-old man has acute respiratory distress after sustaining injuries in a motorcycle accident. He has a blood pressure of 80/60 mm Hg and a pulse rate of 110/min. Examination reveals chest tympany to percussion, distended neck veins, and deviation of the trachea away from his right hemithorax where the breath sounds are diminished. Heart sounds are regular and normal on auscultation. Initial management should consist of
1- administration of 2 L of saline solution.
2- subxiphoid pericardial aspiration.
3- rapid infusion of 500 mL of colloid solution.
4- insertion of a large-bore needle in the right third or fourth intercostal space.
5- intubation followed by mechanical ventilation.
PREFERRED RESPONSE: 4
DISCUSSION: Tension pneumothorax occurs when air trapped in the pleural space between the lung and chest wall achieves sufficient pressure to compress the lungs and shift the mediastinum. Urgent needle decompression of the pleural space air followed by definitive chest tube placement is the treatment of choice.
REFERENCE: Mattox KL, Feliciano DV, Moore EE (eds): Management of Shock, ed 4. New York, NY, McGraw Hill, 2000, p 215.
42/. A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?
1- Cruciate paralysis
2- Quadraplegia
3- Normal function
4- Absent bulbocavernosus reflex
5- Greater occipital nerve dysesthesia
PREFERRED RESPONSE: 3
DISCUSSION: The radiographic findings are consistent with a type II Hangman’s fracture or traumatic spondylolisthesis of C2. This occurs with more than 3 mm of displacement according to the classification of Levine and Edwards. Even though the radiograph reveals significant displacement, the overall space available for the neural elements is increased, therefore minimizing the risk of neural compromise. Neurologic injury is most frequently encountered in type III injuries that are associated with bilateral facet dislocations of C2 on C3 but is infrequent in type I (less than 3 mm displacement) and type II traumatic spondylolisthesis. When neurologic deficits are associated with type II injuries, it is usually the result of an associated head injury. Cruciate paralysis occurs as a result of the crossover of the motor and sensory tracts at different levels of the cord at the C1-C2 junction. This results in normal sensation but complete loss of motor function.
REFERENCES: Levine AM: Traumatic spondylolisthesis of the axis (Hangman’s fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R: Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313-318.
43/. After stabilizing a bimalleolar ankle fracture with a plate and lag screws for the fibula and two interfragmental compression screws for the medial malleolus, a syndesmosis screw is indicated in which of the following situations?
1- In all suprasyndesmotic fibular fractures
2- In all transsyndesmotic fibular fractures
3- When there is increased medial clear space with external rotation stress
4- If the deltoid ligament is ruptured
5- If the posterior malleolus is fractured
PREFERRED RESPONSE: 3
DISCUSSION: It is imperative to recognize the need for a position screw (syndesmosis screw) to hold the syndesmosis in proper alignment when surgically stabilizing an ankle fracture. Although many different fracture patterns are suspicious for a disrupted syndesmosis, the only sure way to assess the syndesmosis is to stress it with abduction and external rotation of the talus and attempt to displace the fibula from the incisura fibularis. Under fluoroscopy, the talus will move laterally and displace the fibula, show a valgus talar tilt, or show an increase in the medial clear space. If any or all of these signs occur, a syndesmosis screw is inserted after making sure that the fibula is reduced into the incisura fibularis. This screw may traverse three or four cortices but must not act as a lag screw. It usually is inserted with the ankle in maximal dorsiflexion, although this is probably not necessary because it is almost impossible to overcompress the syndesmosis. The diameter of the screw does not make any difference. It may or may not be removed but not before 3 months.
REFERENCES: Tornetta P III, Spoo JE, Reynolds FA, Lee C: Overtightening of the ankle syndesmosis: Is it really possible? J Bone Joint Surg Am 2001;83:489-492.
Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
44/. A 32-year-old man sustains multiple injuries in a motorcycle accident including ipsilateral open right femur and comminuted tibia fractures. He has acute abdominal distention and tenderness to palpation. The pelvis is stable to examination. He has a blood pressure of 70/40 mm Hg despite appropriate fluid resuscitation and a pulse rate of 120/min; the pulse is thready. Which of the following procedures is considered the highest priority in the management of this patient?
1- Emergent CT of the abdomen and pelvis
2- Insertion of a Swan-Ganz catheter to monitor the cardiac index
3- Administration of albumin solution
4- Emergent laparotomy in the operating room
5- Application of a pneumatic antishock garment
PREFERRED RESPONSE: 4
DISCUSSION: The patient is in hemorrhagic shock, and timely hemostasis in the operating room should be the highest priority. Further imaging and insertion of central lines carry the risk of further delays in arresting the source of the patient’s bleeding. Albumin (colloid) solutions have questionable indications, are expensive, and have been associated with increased mortality. Crystalloid solutions such as normal saline or lactated Ringer’s solution are the initial resuscitative fluid of choice until blood becomes available. Pneumatic antishock garments have been associated with higher mortality rates, particularly in patients with cardiac and thoracic vascular injuries.
REFERENCES: Krettek C, Simon RG, Tscherne H: Management priorities in patients with polytrauma. Langenbecks Arch Surg 1998;383:220-227.
Weigelt JA: Resuscitation and initial management. Crit Care Clin 1993;9:657-671.
45/. A 35-year-old man sustained an injury to his lower extremity after falling 10 feet from a ladder; initial management was nonsurgical. He now reports chronic hindfoot and anterior ankle pain. Radiographs are shown in Figures 22a and 22b. Surgical reconstruction of this painful process should consist of
1- talectomy and tibiocalcaneal arthrodesis.
2- in situ subtalar joint arthrodesis.
3- distraction bone block subtalar joint arthrodesis.
4- lateral wall exostectomy of the calcaneus.
5- tibiotalar joint arthrodesis.
PREFERRED RESPONSE: 3
DISCUSSION: The radiographs reveal a hindfoot deformity that developed following a severe, comminuted, intra-articular fracture of the calcaneus. There is deformity of the calcaneal body and collapse of the talus into the calcaneus, leading to dorsiflexion of the talus and anterior ankle joint impingement. Distraction bone block subtalar joint arthrodesis will assist with correction of the calcaneal height and will allow for an improved talar declination angle. With this procedure, care must be taken to avoid placing the hindfoot into further varus. A similar reconstruction option not listed would be a calcaneal osteotomy and arthrodesis as described by Romash. Talectomy and tibiocalcaneal arthrodesis are not warranted because the primary structure of the talus and ankle joint is well preserved. In situ subtalar joint arthrodesis will not correct the deformity, and symptoms about the ankle and hindfoot would most likely persist. Lateral wall calcaneal exostectomy may decrease pain from subfibular impingement but will not deal directly with subtalar joint arthrosis and deformity.
REFERENCES: Carr JB, Hansen ST , Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Romash MM: Reconstructive osteotomy of the calcaneus with subtalar arthrodesis for malunited calcaneal fractures. Clin Orthop 1993;290:157-167.
46/. An 8-year-old boy falls and injures his thumb. A radiograph is shown in Figure 23. Initial management should consist of
1- closed reduction.
2- closed reduction and percutaneous pinning.
3- open reduction through a volar approach.
4- open reduction through a dorsal approach.
5- splinting for comfort.
PREFERRED RESPONSE: 1
DISCUSSION: The radiograph shows a complete simple dislocation of the metacarpophalangeal joint. The clue to this injury is the perpendicular alignment of the proximal phalanx to the metacarpal on the lateral radiograph. This must be differentiated from the complete complex dislocation pattern that is irreducible because of the interposed volar plate. In lateral radiographs of these injuries, the long axes of the proximal phalanx and the metacarpal are parallel. Simple dislocations are amenable to closed reduction and casting. Some authors have recommended ulnar collateral ligament repair if instability is detected on examination after reduction.
REFERENCES: O’Brien ET: Part IV: Dislocations of hand and carpus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 429-431.
Bohart PC, Gelberman RH, Vardell RF, Solomon PB: Complex dislocations of the MCP joint. J Bone Joint Surg Am 1974;56:1459-1463.
47/. A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of
1- stretching of the forearm in pronation, wrist flexion, and splinting.
2- primary tendon repair of the flexor pollicis longus and flexor digitorum profundus to the index finger, followed by immobilization.
3- electrodiagnostic examination, followed by decompression of the anterior interosseous nerve within the next 2 to 3 weeks.
4- splinting followed by observation; surgical decompression of the median nerve may be required if no improvement in seen in 3 months.
5- splinting followed by observation; surgical decompression of the anterior interosseous nerve may be required if no improvement is seen in 6 months.
PREFERRED RESPONSE: 5
DISCUSSION: The patient has anterior interosseous nerve palsy. Initial management should consist of splinting followed by observation; surgical decompression may be required if there is no improvement in the functional deficit in 6 months. Anterior interosseous nerve palsy is classically described as an inability to flex the interphalangeal joint of the thumb because of flexor pollicis longus paralysis and a weakness or inability to flex the distal interphalangeal joint of the index finger because of weakness and/or paralysis of the flexor digitorum profundus to the index finger. There has been some controversy in the literature as to whether this represents a true peripheral compression neuropathy or neuritis. Recent recommendations have been to extend the period of observation from 3 to 6 months before surgical decompression, as most cases will resolve within 6 months.
REFERENCES: Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
Stern PJ, Fassler PR: Anterior interosseous nerve compression syndrome, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, 1991, vol 2, pp 983-1002.
48/. A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
1- a shoulder spica cast with the upper extremity in the salute position.
2- a sling and swathe for 3 weeks, followed by gradual motion and strengthening.
3- closed reduction and antegrade intramedullary pinning.
4- closed reduction and retrograde intramedullary nailing.
5- open reduction and internal fixation with small plates and screws.
PREFERRED RESPONSE: 2
DISCUSSION: In this age group, bayonet apposition can produce very good results. Healing occurs rapidly, and remodeling usually is complete in less than 1 year. All of the other methods have significant risks of complications and are unnecessary for this fracture.
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
49/. The cortical injury to the posterolateral distal fibula shown in Figure 25 indicates involvement of which of the following structures?
1- Deltoid ligament
2- Anterior talofibular ligament
3- Calcaneal fibular ligament
4- Superior peroneal retinaculum
5- Syndesmosis
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a rim avulsion fracture that is the result of a forceful twisting injury as the superior peroneal retinaculum is avulsed from its fibular attachment along with a small rim of bone. Injuries to the anterior talofibular ligament or calcaneal fibular ligament would show cortical avulsions more anteriorly or distally at the fibular tip. Deltoid ligament injuries would reveal medial radiographic changes. In a true injury to the syndesmosis, if osseous structures do show avulsion, it would be more directly posterior or anterior on the distal fibula or would occur on the tibial surface.
REFERENCES: Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
50/. A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
1- observation and splinting.
2- local wound drainage under local anesthesia.
3- incision and drainage, deep wound cultures, removal of the plates and screws, and cast application.
4- incision and drainage, deep wound cultures, and removal of the fixation only if it is loose.
5- incision and drainage, deep wound cultures, and bone grafting.
PREFERRED RESPONSE: 4
DISCUSSION: Deep infections after plating of closed fractures of the forearm are unusual. However, the risk increases with repeat surgeries. Debridement of all infected, nonviable tissue is the initial step in management. The fixation may be retained if it is stable, but if the plate and screws are loose, they should be removed and revision performed after removal of nonviable bone. Either external fixation or repeat plating may be performed. Late infections after fracture union may be treated with plate and screw removal, debridement, and IV antibiotics.
REFERENCES: Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63.
Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphysis of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
51/. A left-handed 23-year-old man who fell 5 feet from a ladder onto his left elbow sustained the closed injury shown in Figure 26. Management should consist of
1- percutaneous pin fixation.
2- a percutaneous 6.5-mm screw.
3- long arm casting in flexion.
4- open reduction and internal fixation with a tension band plate.
5- closed reduction and long arm casting in extension.
PREFERRED RESPONSE: 4
DISCUSSION: The radiographs reveal a displaced olecranon fracture. To maximize joint congruity of this intra-articular injury, open reduction and internal fixation is the treatment of choice. A tension band plate will assist with maintenance of the reduction and may aid in early range of motion because injuries to the elbow are prone to stiffness. The oblique fracture line is particularly well suited to plate fixation. Percutaneous pin fixation is unlikely to achieve anatomic joint reduction that can be obtained with open means. External immobilization will not accomplish joint reduction and will most likely lead to a nonunion.
REFERENCES: Hotchkiss RN: Fractures and dislocations of the elbow, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 929-1024.
Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Hume MC, Wiss DA: Olecranon fractures: A clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop 1992;285:229-235.
52/. Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
1- Progressive limb-length discrepancy
2- Contralateral ankle arthritis
3- Ipsilateral hindfoot and midfoot arthritis
4- Ipsilateral knee arthritis
5- Talar osteonecrosis
PREFERRED RESPONSE: 3
DISCUSSION: Ankle arthrodesis for posttraumatic ankle arthrosis provides reliable pain relief. However, the long-term sequela of joint arthrodesis is the development of arthrosis in the surrounding joints. Over time, following ankle arthrodesis, the ipsilateral hindfoot and midfoot joints show signs of joint space wear, and this may be symptomatic. With a stable ankle arthrodesis, progressive limb-length discrepancy or talar osteonecrosis is not expected. Ankle arthrodesis has not been definitively linked to ipsilateral knee arthritis or contralateral ankle arthritis.
REFERENCES: Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Mazur JM, Schwartz E, Simon SR: Ankle arthrodesis: Long-term follow-up with gait analysis. J Bone Joint Surg Am 1979;61:964-975.
53/. A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
1- limited weight bearing for 6 weeks, followed by a progressive return to activity.
2- no weight bearing for 6 weeks, followed by no running for 6 months.
3- no weight bearing for 2 weeks, followed by internal fixation if symptoms persist.
4- internal fixation at the time of diagnosis.
5- cessation of running for 6 weeks.
PREFERRED RESPONSE: 4
DISCUSSION: Unlike compression-side stress fractures, tension-side stress fractures on the superior side of the femoral neck are at a very high risk of displacement, even if the patient is not bearing weight. It is highly recommended to treat these fractures like acute fractures and to proceed with internal fixation emergently. Once the fracture has displaced, the prognosis is poor in terms of returning to sports, even when reduced and internally fixed. Nonsurgical management, such as limited weight bearing and low-impact activities, works very well for other lower extremity stress fractures. A training program evaluation (shoes, tracks, schedule) is always indicated for all patients with stress fractures.
REFERENCE: Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
54/. A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
1- Latent osteomyelitis from the percutaneous pins
2- Muscle weakness because of a lack of postinjury rehabilitation
3- Tardy ulnar nerve paralysis from injury by the medial pin
4- Osteonecrosis of the trochlea, producing joint incongruity
5- A new acute process
PREFERRED RESPONSE: 4
DISCUSSION: The patient sustained a very distal supracondylar fracture of the humerus. Fractures in this area can disrupt the blood vessels supplying the lateral ossification center of the trochlea. With disturbance of the blood supply in this area, local osteonecrosis occurs and disrupts the support for the overlying articular surface, producing joint incongruity and localized degenerative arthritis.
REFERENCES: Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
Morrissy RT, Wilkins KE: Deformities following distal humeral fracture in childhood. J Bone Joint Surg Am 1984;66:557-562.
55/. A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of
1- closed treatment and observation for return of nerve function.
2- closed treatment and immediate tendon transfer.
3- open nerve exploration without internal fixation of the fracture.
4- open nerve exploration with plating of the fracture.
5- open nerve exploration with intramedullary rodding of the fracture.
PREFERRED RESPONSE: 1
DISCUSSION: The patient has an isolated closed injury involving the humeral diaphysis. The lack of wrist and finger extension indicates injury to the radial nerve. Based on these findings, ongoing observation of the nerve is warranted with delayed exploration after 3 to 4 months if there are no signs of progressive return of nerve function. Treatment of the fracture should include external immobilization and fracture bracing. An indication for nerve exploration and surgical stabilization would be an open fracture.
REFERENCES: Zuckerman JD, Kovil KJ: Fractures of the shaft of the humerus, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1025-1053.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
56/. Examination of a 41-year-old man who was thrown from a motorcycle reveals that both legs appear externally rotated and there is bruising in the perineal area. He has a blood pressure of 80/40 mm Hg, a pulse rate of 140/min, a respiratory rate of 25/min, and he appears confused. Following administration of 4 L of saline solution and 2 units of packed red blood cells, he has a blood pressure of 80/40 mm Hg, a pulse rate of 160/min, and a respiratory rate of 25/min. The abdominal assessment for intraperitoneal blood is negative. An AP radiograph shows an anteroposterior compression injury with 7 cm of symphysis diastasis but no posterior displacement in the sacroiliac joints. What is the next most appropriate step in management?
1- Stabilization of the pelvis through noninvasive methods
2- Additional crystalloid solution replacement
3- External fixation in the operating room
4- Angiographic embolization
5- Continuing observation of vital signs
PREFERRED RESPONSE: 1
DISCUSSION: Because the patient has sustained a major high-energy injury to the pelvic ring, it can be assumed that there is serious bleeding or hemodynamic instability related to a pelvic vascular injury. The goal of intervention at this time is to assist in the resuscitative effort and to stop the bleeding. All attempts at providing fluid and blood are important, but without cessation of the bleeding continued loss occurs and significant problems can ensue such as coagulopathy and multiple organ failure. Noninvasive methods of stabilizating the pelvic ring should be used to stop the bleeding. These methods include wrapping a sheet around the pelvis or using commercially available belts, vacuum beanbags, or pneumatic shock garments. This will provide time to prepare for arteriography and/or external fixation. The next step is debatable but in view of negative findings for intra-abdominal blood, arteriography performed with the pelvis reduced using noninvasive methods would be ideal.
REFERENCES: Bassam D, Cephas GA, Ferguson KA, Beard LN, Young JS: A protocol for the initial management for unstable pelvic fractures. Am Surg 1998;64:862-867.
Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 217-226.
Mucha P Jr, Welch TJ: Hemorrhage in major pelvic fractures. Surg Clin North Am 1988;68:757-773.
57/. A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of
1- closed reduction and application of a long leg cast.
2- open reduction and internal fixation with plate and screw fixation.
3- percutaneous plate fixation.
4- spanning external fixation with delayed limited open reduction and internal fixation.
5- primary ankle arthrodesis.
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a severe high-energy injury from axial loading to the left ankle and distal tibia. This is a closed injury, but the soft tissues are injured and severely swollen. Initial treatment should focus on skeletal stabilization, and incisions directly over the fracture area should be avoided until soft-tissue stabilization has occurred. Immediate spanning external fixation with plans for a delayed reconstruction as needed for the joint surface is the treatment of choice. Closed reduction and application of a constrictive long leg cast may lead to increased risk of tissue necrosis. Immediate open procedures to internally fix the fracture add the risks of soft-tissue necrosis and are to be avoided. Percutaneous plating may be one of the delayed fixation options but should not be used immediately. Primary ankle arthrodesis is not indicated.
REFERENCES: Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
58/. Which of the following parameters is considered most important when assessing an acetabular fracture for surgical indications?
1- Age of the patient
2- Failure to maintain reduction of the head under the dome without traction
3- Presence of a femoral head impaction lesion
4- Direction of the femoral head displacement
5- Fragmentation of the fracture
PREFERRED RESPONSE: 2
DISCUSSION: The most important aspect in the decision for surgery in an acetabular fracture is the ability of the femoral head to remain concentrically reduced under the dome in AP and Judet oblique views of the pelvis. If this parameter is present, then the need for surgery is determined by other aspects such as fragmentation, age, incongruity, and displacement. If the head remains stable under the dome without traction, there is sufficient acetabular dome to provide stability, and nonsurgical treatment may be appropriate.
REFERENCES: Tile M: Assessment and management of acetabular fractures, in Tile M (ed): Pelvic and Acetabular Fractures, ed 2. Baltimore, MD, Williams and Wilkins, 1995, pp 305-354.
Letournel E: Acetabular fractures: Classification and management. Clin Orthop 1980;151:81-106.
Letournel E, Judet R: Fractures of the Acetabular, ed 2. Berlin, Springer-Verlag, 1993, pp 29-49.
59/. A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of
1- ankle arthrodesis.
2- modified Brostrom ligament reconstruction.
3- restoration of fibular length, alignment, and rotation.
4- cast immobilization.
5- tibial shortening osteotomy.
PREFERRED RESPONSE: 3
DISCUSSION: The radiographs reveal a malunited distal fibular fracture with shortening. Because there appears to be an adequate cartilage space within the ankle joint, the role of reconstruction would be to prevent arthrosis and the need for ankle arthrodesis, as well as to decrease symptoms. The treatment of choice is restoration of fibular length, alignment, and rotation with osteotomy plating, and bone grafting as needed. There is no indication for ligament reconstruction of a mechanically stable ankle, and tibial shortening osteotomy will not assist in correcting the deformity. Cast immobilization may assist with improvement of symptoms but will not correct the overall process. Determination of fibular length is best done by comparing the talocrural angle of the injured side with the uninjured side. The goal is to perfectly reduce the talus in the ankle mortise.
REFERENCES: Marti RK, Raaymakers EL, Nolte PA: Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-713.
Geissler W, Tsao A, Hughes J: Fractures and injuries of the ankle, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2201-2206.
Yablon IG, Leach RE: Reconstruction of malunited fractures of the lateral malleolus. J Bone Joint Surg Am 1989;71:521-527.
60/. A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
1- extensor digitorum brevis.
2- plantar fascia.
3- peroneus brevis.
4- peroneus longus.
5- syndesmosis.
PREFERRED RESPONSE: 4
DISCUSSION: The os peroneum is an accessory ossicle located within the peroneus longus tendon. It is typically located at the level of the cuboid groove in the lateral hindfoot and midfoot region. Proximal migration of the os peroneum indicates disruption of the peroneus longus tendon and is an important clue to diagnosis. This unusual condition can cause chronic lateral ankle pain, and surgical repair may be indicated. Active eversion indicates that the peroneus brevis is clinically intact. Disruption of the extensor digitorum brevis, plantar fascia, or syndesmosis would have no effect on the position of the os peroneum.
REFERENCES: Thompson FM, Patterson AH: Rupture of the peroneus longus tendon: Report of three cases. J Bone Joint Surg Am 1989;71:293-295.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
61/. A 24-year-old man sustained a grade IIIb open tibial fracture and an ipsilateral grade IIIa femoral fracture in a motorcycle accident. He is unresponsive, intubated, and has a Glasgow Coma Scale score of 8. He is resuscitated and taken to the operating room for definitive orthopaedic care. Which of the following intraoperative problems will most likely adversely affect his long-term outcome?
1- Blood loss during debridement
2- Prolonged tourniquet time
3- Failure to stabilize both fractures with intramedullary nails
4- Episodic hypotension
5- Loss of dorsalis pedis pulse
PREFERRED RESPONSE: 4
DISCUSSION: Traumatic brain injury is considered to be either primary or secondary. Primary injury is direct or impact damage to the brain, and secondary injury can have intracranial or systemic causes. While treatment has little impact on primary brain injury, secondary brain injury can be avoided. There are also many causes of intracranial secondary brain injury, including intracranial hypertension or cerebral edema. There are many causes of systemic secondary brain injury, but none has a greater impact on outcome than hypotension or hypoxia. In fact, the occurrence of hypotension postinjury causes a 10- to 15-fold increase in mortality. In a series by Pietropaoli and associates, the mortality rate for head-injured patients that were normotensive during surgery was 25%, but if they were hypotensive the mortality rate was 82%. In the same series, the number of patients with a Glasgow Coma Scale score of either 4 or 5 dropped from 58% in those patients that were normotensive during surgery to 6% in those patients that became hypotensive during surgery. Efforts to avoid hypotension postinjury and especially during surgery should be of primary importance.
REFERENCES: Chesnut RM, Marshall LF, Klauber MR, et al: The role of secondary brain injury in determining outcome from severe head injury. J Trauma 1993;34:216-222.
Pietropaoli JA, Rogers FB, Shackford SR, Wald SL, Schmoker JD, Zhuang J: The deleterious effects of intraoperative hypotension on outcome in patients with severe head injury. J Trauma 1992;33:403-407.
Schmeling GJ, Schwab JP: Polytrauma care: The effect of head injuries and timing of skeletal fixation. Clin Orthop 1995;318:106-116.
Townsend RN, Lheureau T, Protech J, Reimer B, Simon D: Timing fracture repair in patients with severe brain injury (Glascow Coma Scale score
J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
72/. A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?
1
Increased pitching activity in conjunction with aggressive physical therapy
2
Biopsy of the lesion in the proximal humerus
3
Complete rest with no activity
4
Immobilization in a shoulder spica cast in the salute position
5
Cessation of pitching and a vigorous program of muscle strengthening
The patient has a rotational stress fracture of the proximal humeral physis (Little Leaguer’s shoulder). The symptoms of increasing pain with activity and relief with rest are typical of a stress injury. Treatment should consist of cessation of throwing activity but rehabilitation of the shoulder girdle muscles. The pitching technique should be evaluated as well.
REFERENCES: Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in the adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
73/. A 36-year-old man sustains a traumatic spondylolisthesis of L5 on S1. Surgical stabilization requires pedicular fixation into the sacrum. If the screw is placed in a medial to lateral direction and penetrates the sacral ala, what nerve root is at risk?
1- L2
2- L3
3- L4
4- L5
5- S1
PREFERRED RESPONSE: 4
DISCUSSION: The L5 nerve root lies directly over the superior and anterior alae. If the screw is directed approximately 20 degrees laterally and bicortical purchase is achieved, there is the risk of injuring the L5 nerve root. If the screw is directed medially into the body of S1, there is little risk of injury. The same root is at risk during placement of an iliosacral screw.
REFERENCES: Ebraheim NA, et al: Lumbosacral nerve and dorsal screw placement. Orthopedics 2000;23:245-247.
Ebraheim NA, Mermer M, Xu R, Yeasting RA: Radiological evaluation of S1 dorsal screw placement. J Spinal Disord 1996;9:527-535.
Routt ML Jr, Nork SE, Mills WJ: Percutaneous fixation of pelvic ring disruptions. Clin Orthop 2000;375:15-29.
74/. A 25-year-old woman who fell on her outstretched hand reports chronic pain over the hypothenar eminence region and some dorsal ulnar wrist pain. She also notes difficulty playing golf and tennis. Plain radiographs of the hand and wrist are unremarkable. A CT scan is shown in Figure 36. What is the next most appropriate step in management?
1- Ultrasound therapy
2- MRI for further soft-tissue evaluation
3- Open reduction and internal fixation of the hook of the hamate
4- Excision of the hook of the hamate
5- Electrodiagnostic evaluation
PREFERRED RESPONSE: 4
DISCUSSION: The CT scan reveals a hook of the hamate nonunion with irregular resorption at the fracture site, which is at the base of the hamate. Symptomatic relief of the pain and discomfort has been well documented after excision of the hook of the hamate. Ultrasound therapy will not provide long-term symptomatic relief or induce nonunion healing. MRI for further soft-tissue evaluation is inappropriate because this is a bony problem; the bony architecture of the wrist is best visualized by CT. Open reduction and internal fixation of the hook of the hamate does not provide the symptomatic relief that is found with excision of the hook of the hamate. In addition, the technical difficulties and relative risk of persistent nonunion after open reduction and internal fixation are not merited when hamate excision can be effected easily and causes no long-term untoward effects. Electrodiagnostic evaluation is inappropriate because there is no history of the persistent numbness and tingling that is found in peripheral compression neuropathies.
REFERENCES: Stark HH, Chao EK, Zemel NP, Rickard TA, Ashworth CR: Fracture of the hook of the hamate. J Bone Joint Surg Am 1989;71:1206-1207.
Failla JM: Hook of hamate vascularity: Vulnerability to osteonecrosis and nonunion. J Hand Surg Am 1993;18:1075-1079.
Carter PR, Easton RG, Littler JW: Ununited fracture of the hook of the hamate. J Bone Joint Surg Am 1977;59:583-588.
Egawa M, Asai T: Fracture of the hook of the hamate: Report of six cases and the suitability of computerized tomography. J Hand Surg Am 1983;8:393-398.
75/. An active 72-year-old woman sustained a mid-diaphyseal right humerus fracture 16 months ago. History reveals that she was first treated with a brace for 7 months. Additional treatment consisted of intramedullary nailing 9 months ago. Recently the rod was removed, and the patient now reports pain and gross motion at the fracture site. Current radiographs are shown in Figures 37a and 37b. What is the next most appropriate step in management?
1- Electrical stimulation with an implanted coil
2- Ultrasound stimulation for 30 minutes per day
3- Locked intramedullary nailing with bone graft
4- Ilizarov external fixation with intermittent distraction and compression
5- Plate and screw fixation with bone graft
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a well-established nonunion in a very porotic bone. Electrical stimulation has been found effective in treating tibial nonunions, but there is very little data on humeral nonunions, especially chronic well-established ones. Ultrasound stimulation is effective in accelerating fracture healing, but there is little data concerning the treatment of nonunions. Intramedullary nailing with bone graft is an option, but it maybe difficult to obtain a rigid construct in a very porotic bone. An Ilizarov-type external fixator would be an alternative, but there is little clinical data for the humerus and it may be poorly tolerated. A plate and screw construct with bone graft combines rigidity with the biologic advantage of the bone graft. A recent series reported on the use of a plate combined with onlay allograft for recalitrant nonunions. Cement augmentation for screw fixation either in the canal or added to the screw holes may be helpful in select cases.
REFERENCES: Hornicek FJ, Zych GA, Hutson JJ, Malinin TI: Salvage of humeral nonunions with onlay bone plate allograft augmentation. Clin Orthop 2001;386:203-209.
Jupiter JB: The treatment of complex non-unions of the humeral shaft with a combination of surgical techniques. J Bone Joint Surg Am 1990;72:701-707.
76/. A 47-year-old man ruptured his left patellar tendon and twisted his right ankle in a fall. Initial radiographs of the ankle are unremarkable. One week following repair of the left patellar tendon, he reports increased pain with weight bearing in his right ankle. A follow-up radiograph is shown in Figure 38. Management of the ankle injury should consist of
1- functional rehabilitation with range of motion and strengthening.
2- reduction and screw fixation of the syndesmosis.
3- closed reduction and a long leg cast.
4- repair of the talofibular ligaments.
5- fibular osteotomy and plate fixation.
PREFERRED RESPONSE: 2
DISCUSSION: The radiograph reveals disruption of the syndesmosis with lateral displacement of the talus and widening of the medial ankle clear space. No fibular fracture is noted, although radiographs of the entire tibia and fibula are necessary to rule out a more proximal fibula fracture. There is clear instability of the syndesmosis, and surgical stabilization is needed, either by direct repair of the ligaments or more commonly with surgical stabilization of the fibula to the tibia with screws. Functional rehabilitation and early range of motion are indicated with anterior-lateral ankle sprains but not with true instability of the syndesmosis. In anterior syndesmotic injuries in which there are no signs of instability on plain radiographs or with stressing, cast immobilization and protected weight bearing until tenderness subsides is warranted. Long leg cast immobilization is unlikely to be adequate in maintaining reduction of the syndesmosis. Repair of the talofibular ligaments or fibular osteotomy does not address the pathology at the syndesmosis. Chronic syndesmotic disruption is likely to lead to chronic ankle pain and early arthrosis.
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Edwards GS Jr, DeLee JC: Ankle diastasis without fracture. Foot Ankle 1984;4:305-312.
77/. A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
1- open reduction and internal fixation.
2- percutaneous pin fixation.
3- excision of the fracture fragment.
4- primary calcaneocuboid joint arthrodesis.
5- a walking cast or removable cast boot.
PREFERRED RESPONSE: 5
DISCUSSION: The CT scans show a fracture of the anterior process of the calcaneus that involves less than 25% of the joint surface with minimal to no displacement. The preferred treatment is external immobilization in either a walking cast or, more typically, a removable cast boot. For larger fractures that involve more than 25% of the articular surface with joint incongruity, open reduction and internal fixation may be indicated. Primary calcaneocuboid joint arthrodesis is not warranted because symptoms are rare in most patients. Delayed excision of the fragment is a late reconstructive option if painful nonunion develops. Percutaneous pin fixation is not indicated beceause there tends to be inherent stability in this fracture.
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
78/. Which of the following complications occurs more commonly after antegrade femoral nail insertion when compared with retrograde insertion?
1- Increased blood loss
2- Decreased range of motion of the knee
3- Infection
4- Hip pain
5- Muscle weakness
PREFERRED RESPONSE: 4
DISCUSSION: There is no difference between the rates of union, malunion, range of motion of the hip or knee, muscle weakness, or infection for the two types of femoral nail insertion. The only difference is the location of the morbidity, which is around the insertion point of the rod. The antegrade technique has more morbidity about the hip, and the retrograde insertion technique has more morbidity about the knee.
REFERENCES: Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16.
Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R: Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161-169.
Ostrum RF, Agarwal A, Lakatos R, Poka A: Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496-501.
Tornetta P III, Tiburzi D: Antegrade or retrograde reamed femoral nailing: A prospective, randomized trial. J Bone Joint Surg Br 2000;82:652-654.
79/. A 24-year-old man has right forearm pain after sliding head first into home plate. Examination reveals that the arm is swollen, but there are no neurovascular deficits or skin lacerations. Radiographs reveal a both-bone forearm fracture. The ulna has an oblique fracture with a 30% butterfly fragment, and the radius is comminuted over 75% of its circumference. In addition to reduction and plate fixation of both bones, management should consist of
1- bone grafting the radius only.
2- bone grafting both the radius and ulna.
3- bone graft substitute for both the radius and ulna.
4- no additional grafting.
5- no additional grafting but postoperative electrical stimulation.
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a both-bone fracture with a comminuted radial shaft. Open reduction and internal fixation of both bones is the treatment of choice. In the past, Chapman and associates recommended bone grafting radial shaft fractures with more than 30% comminution of the circumference. This has remained the recommendation in most textbooks. More recent studies, where modern biologic plating techniques were used, found that the addition of bone graft to comminuted fractures was not necessary because the union rate did not differ from that of nongrafted comminuted fractures.
REFERENCES: Anderson LD, Sisk TD, Tooms RE, Park WI III: Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am 1975;57:287-297.
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
Wright RR, Schmeling GJ, Schwab JP: The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review. J Orthop Trauma 1997;11:288-294.
Wei SY, Born CT, Abene A, Ong A, Hayda R, Delong WG Jr: Diaphyseal forearm fractures treated with and without bone graft. J Trauma 1999;46:1045-1048.
80/. A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
1- Fracture comminution
2- Displacement of 1 mm at the fracture site
3- Involvement of the ischial facet
4- Femoral head subluxation during fluoroscopic examination
5- Presence of a bilateral pneumothorax
PREFERRED RESPONSE: 4
DISCUSSION: Fractures with a posterior wall fragment that makes up less than one third of the surface generally are stable. Conversely, fractures with a fragment making up more than 50% of the surface are unstable. Patients with an intermediate fracture fragment should undergo a fluoroscopic examination under sedation or anesthesia to determine if the fragment is truly stable. If so, the patient can be treated nonoperatively and safely mobilized.
REFERENCES: Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
Keith JE Jr, Brashear HR Jr, Guilford WB: Stability of posterior fracture-dislocations of the hip: Quantitative assessment using computed tomography. J Bone Joint Surg Am 1988;70:711-714.
81/. A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of
1- closed reduction and a short arm cast for 10 weeks.
2- closed reduction and a long arm cast for 10 weeks.
3- open reduction and internal fixation.
4- limited intercarpal fusion.
5- proximal row carpectomy.
PREFERRED RESPONSE: 3
DISCUSSION: The radiographs reveal a scaphoid fracture with displacement and comminution and an unstable fracture pattern. Treatment should consist of open reduction and internal fixation. In displaced scaphoid fractures and fractures with unstable fracture patterns, closed reduction is ineffective and is likely to lead to nonunion. Limited intercarpal fusion and proximal row carpectomy are used to correct a variety of traumatic and posttraumatic problems of the wrist.
REFERENCES: Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 809-823.
Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276.
Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
Szabo RM, Manske D: Displaced fractures of the scaphoid. Clin Orthop 1988;230:30-38.
82/. A 42-year-old woman reports that she has low back pain and had a transient loss of consciousness after falling off a horse. She denies having neck pain but notes that she was involved in a motor vehicle accident 2 years ago and had neck pain at that time. Examination reveals full range of motion of the neck and no localized tenderness. The neurologic examination is normal. A lateral radiograph of the cervical spine is obtained. Figures 41a and 41b show CT and MRI scans. What is the most likely diagnosis?
1- Cervical sprain
2- Atlas fracture
3- Acute displaced odontoid fracture
4- Odontoid nonunion
5- Hangman’s fracture
PREFERRED RESPONSE: 4
DISCUSSION: The examination findings do not correlate with an acute injury (full range of cervical motion and the absence of pain). Radiographically, the fracture appears old based on the smooth contour of the fracture fragments and the absence of soft-tissue swelling. Flexion-extension radiographs can be obtained to determine potential instability; if present, stabilization and fusion should be considered.
REFERENCES: Schatzker J, Rorabeck CH, Waddell JP: Non-union of the odontoid process: An experimental investigation. Clin Orthop 1975;108:127-137.
Clark CR, White AA III: Fractures of the dens: A multicenter study. J Bone Joint Surg Am 1985;67:1340-1348.
83/. What neurologic structure is most at risk when performing intramedullary screw fixation of a fifth metatarsal base fracture?
1- Saphenous nerve
2- First branch of the lateral plantar nerve
3- Superficial peroneal nerve
4- Sural nerve
5- Deep peroneal nerve
PREFERRED RESPONSE: 4
DISCUSSION: The sural nerve and its terminal branches course through the lateral hindfoot and midfoot area and are directly at risk in surgeries involving the peroneal tendon complex and the fifth metatarsal. The first branch of the lateral plantar nerve originates in the tarsal tunnel region and courses across the plantar heel area to innervate the abductor digiti minimi; it is not at direct risk with fifth metatarsal surgery. The saphenous, superficial peroneal, and deep peroneal nerves are not at risk anatomically with a lateral midfoot incision.
REFERENCES: Donley BG, McCollum MJ, Murphy GA, Richardson EG: Risk of sural nerve injury with intramedullary screw fixation of fifth metatarsal fractures: A cadaver study. Foot Ankle Int 1999;20:182-184.
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
84/. A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
1- bed rest only for 6 weeks.
2- mobilization in a kinetic therapy bed for 6 weeks, followed by a hyperextension brace.
3- a total contact thoracolumbosacral orthosis and rapid mobilization.
4- anterior decompression, vertebral reconstruction, and stabilization.
5- posterior reduction, stabilization, and grafting.
PREFERRED RESPONSE: 3
DISCUSSION: The patient has a stable fracture that can be initially treated with bed rest, followed by bracing and quick mobilization. The outcome is good and surgery is not required. These fractures can be treated nonsurgically if there is less than 50% compression, 15 degrees of angulation, and intact posterior structures.
REFERENCES: Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Rechtine GR II, Cahill D, Chrin AM: Treatment of thoracolumbar trauma: Comparison of complications of operative versus nonoperative treatment. J Spinal Disord 1999;12:406-409.
85/. A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
1- observation.
2- a rigid collar for 6 weeks.
3- halo vest application.
4- open reduction and posterior stabilization.
5- open reduction, diskectomy, grafting, and anterior plate stabilization.
PREFERRED RESPONSE: 2
DISCUSSION: The patient has a stable flexion-compression injury of the cervical spine. The fracture occurs as a result of compression failure of the vertebral body. If the force continues, a tension failure of the posterior structures occurs, leading to potential dislocation. Immobilization in a rigid cervical orthosis will allow this fracture to heal.
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Allen GL, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
86/. Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
1- external traction.
2- open reduction and internal stabilization.
3- repeat closed reduction under general anesthesia.
4- open reduction.
5- percutaneous pin fixation in the current position.
PREFERRED RESPONSE: 4
DISCUSSION: The radiographs show a complex dislocation of the little finger metacarpophalangeal joint. This is characterized by obvious dislocation on the AP and lateral views and a type of bayonet apposition best visualized on the lateral view. Irreducibility of this injury is caused by displacement of the volar plate that has been traumatically avulsed from its origin on the metacarpal, with subsequent displacement into the metacarpophalangeal joint. This abnormal position of the volar plate causes irreducibility that can be corrected only by open reduction. This can be effected either by dorsal or palmar approaches.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
87/. A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
1- repeat closed reduction and buddy taping.
2- closed reduction and percutaneous pin fixation, followed by casting.
3- open reduction and plate fixation, followed by casting.
4- open reduction and screw fixation, followed by splinting and early motion.
5- open reduction and intramedullary fixation with absorbable implants.
PREFERRED RESPONSE: 2
DISCUSSION: The patient has an unstable oblique fracture of the proximal phalanx that is easily reducible but unstable; therefore, the treatment of choice is closed reduction and percutaneous pin fixation, followed by casting. Closed reduction and percutaneous pin fixation offers a better functional result than open reduction and plate fixation. Repeat closed reduction and buddy taping is inadequate because of the inherently unstable fracture pattern. Buddy taping will allow the dislocation to recur. The other options represent more aggressive surgical techniques than are necessary to treat this fracture.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
88/. Figures 43a and 43b show the AP and lateral radiographs of the radius and ulna of a 9-year-old patient. The fracture is manipulated and placed in a long arm cast with the elbow flexed to 90 degrees and the forearm to neutral rotation. Figures 43c and 43d show the alignment of the fracture after the manipulation. What is the next most appropriate step in management?
1- Stabilize the present reduction internally with intramedullary pins.
2- Accept the present reduction and obtain follow-up radiographs in 1 week.
3- Remanipulate the fracture and place the forearm in pronation.
4- Remanipulate the fracture and place the forearm in supination.
5- Stabilize the present reduction with plates and screws.
PREFERRED RESPONSE: 4
DISCUSSION: By placing the forearm at neutral rotation, as shown in Figures 43c and 43d, the distal fragment has become malrotated by 90 degrees. This is evident by the fact that the bicipital tuberosity is rotated 90 degrees to the radial styloid. Normally, it should be directly opposite (180 degrees) to the radial styloid. The correct alignment was present in the original radiographs shown in Figures 43a and 43b. Another clue to the malrotation in the postreduction radiographs is the difference in the diameters of the opposing radial shafts. To correct this rotational malalignment, the distal fragment needs to be remanipulated into supination so that it is correctly aligned with the supinated proximal radius.
REFERENCES: Evans EM: Fractures of the radius and ulna. J Bone Joint Surg Br 1951;33:548-561.
Milch H: Roentgenographic differentiation between torsion and rotational fractures of the forearm. Bull Hosp Jt Dis 1949;10:216-225.
89/. Which of the following findings is an indication for adjunctive use of high-dose steroids?
1- C6 level injury secondary to a unilateral facet fracture-dislocation with weakness of wrist extension
2- C6 burst fracture with no neurologic deficit
3- L3 burst fracture with cauda equina syndrome
4- Incomplete spinal cord injury in a patient 24 hours after injury
5- Complete C6 level deficit in patient with spinal shock and a fracture-dislocation at C5 on C6 5 hours after injury
PREFERRED RESPONSE: 5
DISCUSSION: According to NASCIS III, the high-dose steroid protocol involves infusion of 30 mg/kg methylprednisolone followed by 5.4 mg/kg/h for 24 hours if the patient has sustained a spinal cord injury within the last 3 hours. The drip is continued for 48 hours if administration is started between 3 and 8 hours of the onset of neurologic deficit. No benefit has been conclusively demonstrated with steroids administered beginning 8 hours or longer after injury. Steroid use is not indicated for nerve root deficits, brachial plexus deficits, or gunshot wounds.
REFERENCES: Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 319-328.
Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury randomized controlled trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
90/. A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
1- Pulmonary embolism
2- Fat embolism syndrome
3- Sepsis
4- Pneumonia
5- Pneumothorax
PREFERRED RESPONSE: 2
DISCUSSION: The major criteria for the diagnosis of fat embolism syndrome include hypoxemia (PaO2 of less than 60 mm Hg), central nervous system depression, and a petechial rash that is most often located in the axillae, conjunctivae, and palate. The rash is often transient. Tachycardia, pyrexia, anemia, thrombocytopenia, and the presence of fat in the urine are all considered minor criteria. To establish the diagnosis of fat embolism syndrome, one major and four minor signs should be present. Pulmonary embolism, which is the major differential diagnosis, usually is not associated with conjunctival petechia or thrombocytopenia.
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
91/. Figure 45 shows the current radiograph of an 11-year-old girl who sustained a simple nondisplaced fracture of the distal radius 4 weeks ago. Management at the time of injury consisted of application of a short arm cast but no manipulation. What is the major concern at this time?
1- Stiffness of the wrist joint
2- Physeal growth arrest
3- Physeal overgrowth
4- Osteonecrosis of the metaphysis
5- Posttraumatic arthritis
PREFERRED RESPONSE: 2
DISCUSSION: The fracture pattern represents a Peterson type I physeal injury, which is a comminuted metaphyseal fracture in which the fracture lines extend up to the physis. Because there is no displacement of the physis and the fracture lines do not cross the physis, there may be a tendency to dismiss this injury as a simple metaphyseal fracture with no significant sequelae. A small percentage of patients (3% in Peterson’s series) experience growth arrest. In this patient, a disabling ulnar plus deformity, defined as increased ulnar length in relationship to the distal radius, developed.
REFERENCES: Peterson HA: Physeal fractures: Part 2. Two previously unclassified types. J Pediatr Orthop 1994;14:431-438.
Peterson HA: Physeal and apophyseal injuries, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 108-109.
92/. Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
1- Blood pressure
2- Urine output
3- Central venous pressure
4- Heart rate
5- Base deficit
PREFERRED RESPONSE: 5
DISCUSSION: The end point of resuscitation is adequate tissue perfusion and oxygenation. Blood lactate is the end point of anaerobic metabolism. The level of blood lactate reflects global hypoperfusion and is directly proportional to oxygen debt. Two separate prospective studies have verified a significant difference in mortality when blood lactate was used as a measure of resuscitation when compared to traditional parameters (mean arterial pressure, urine output, central venous pressure, and heart rate). Base deficit is a direct measure of metabolic acidosis and an indirect measure of blood lactate levels. It correlates well with organ dysfunction, mortality, and adequacy of resuscitation. It is easy to measure, can be obtained rapidly, and is an excellent assessment of the adequacy of resuscitation.
REFERENCES: Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Elliot DC: An evaluation of the end points of resuscitation. J Am Coll Surg 1998;187:536-547.
93/. A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
1- Immediately
2- When skin wrinkles are present and abrasions are epithelialized
3- Five days after injury
4- Following analysis of laser Doppler skin measurements
5- Following measurement of transcutaneous oxygen tension
PREFERRED RESPONSE: 2
DISCUSSION: Following any closed fracture, the most important determinant for the timing of surgery is the condition of the soft tissues and especially the skin. The best determinant of appropriate soft-tissue condition is the presence of wrinkling of the skin (wrinkle sign) at the site of the incision. A wrinkle sign is present when all the interstitial edema has left the skin; this may take up to 14 to 21 days of elevation. Any abrasion must be epithelialized so that there are no bacteria left at the site. To date, no other method of soft-tissue viability measurement has been shown to be of any clinical benefit.
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
94/. A 28-year-old woman sustained an injury to her dominant right arm after falling off her porch. Examination reveals a deformity at the elbow. She is neurovascularly intact. Figures 46a and 46b show the radiographs obtained before closed reduction, and postreduction radiographs are shown in Figure 46c and 46d. What is the most likely early complication?
1- Radial nerve injury
2- Intra-articular loose body causing a block to motion
3- Lack of active elbow flexion
4- Recurrent dislocation
5- Forearm compartment syndrome
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a complex fracture-dislocation of the elbow. The radial head is fractured, and there is a displaced coronoid fracture. These associated fractures indicate that the elbow is at high risk for recurrent instability after initial treatment. To prevent this complication, surgical treatment will most likely be required and will consist of some or all of the following: radial head open reduction and internal fixation or replacement, coronoid open reduction and internal fixation, medial and lateral ligament repairs, and even articulated external fixation. This patient was treated with open reduction and internal fixation of the radial head, and the elbow redislocated postoperatively.
REFERENCES: Ring D, Jupiter JB: Reconstruction of posttraumatic elbow instability. Clin Orthop 2000;370:44-56.
O’Driscoll SW: Classification and evaluation of recurrent instability of the elbow. Clin Orthop 2000;370:34-43.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxation and dislocation. Clin Orthop 1992;280:186-197.
95/. What is the most likely long-term sequela of the injury shown in Figures 47a and 47b?
1- Peroneal tendon instability
2- Ankle joint instability
3- Subtalar joint arthrosis
4- Ankle joint arthritis
5- Entrapment of the flexor hallucis longus tendon
PREFERRED RESPONSE: 3
DISCUSSION: The imaging studies show a comminuted lateral talar process fracture. This injury is often missed on plain radiographs; therefore, CT provides the best method of diagnostic evaluation. The most likely long-term sequela of this injury is subtalar joint arthrosis. Although this injury involves the fibular gutter region, progression to true ankle arthritis is unlikely. There does not appear to be any association with this injury and chronic mechanical instability of the ankle or disruption of the superior peroneal retinaculum and subsequent peroneal tendon instability. Entrapment of the flexor hallucis longus tendon may occur with fractures of the sustentaculum tali but not with injuries of the lateral talar process. Surgical management includes open reduction and internal fixation versus excision; the goal is preservation of the large articular surface fragments. In this patient, there is significant comminution and early fragment excision may be the best option for acute treatment.
REFERENCES: Tucker DJ, Feder JM, Boylan JP: Fractures of the lateral process of the talus: Two case reports and a comprehensive literature review. Foot Ankle Int 1998;19:641-646.
Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
96/. A 16-year-old high school football player has diffuse pain with attempted digital flexion after injuring the ring finger of the dominant hand 1 week ago. Examination reveals that he is unable to flex the distal interphalangeal joint. Management should consist of
1- surgical exploration and tendon reinsertion of the flexor digitorum profundis.
2- surgical exploration and tendon reinsertion of the flexor digitorum superficialis.
3- steroids and physical therapy.
4- surgical release of the anterior interosseous nerve.
5- surgical release of the median nerve.
PREFERRED RESPONSE: 1
DISCUSSION: The patient has an avulsion of the flexor digitorum profundus. Treatment should include surgical exploration and tendon reinsertion. This is not an avulsion of the flexor digitorum superficialis because the patient’s deficiency is the inability to flex the distal interphalangeal joint, not the proximal interphalangeal joint. Surgical release of the anterior interosseous nerve is not indicated because the flexor digitorum profundus of the ring finger is innervated by the ulnar nerve. A median nerve contusion causes wrist pain and/or numbness and tingling in the median nerve distribution.
REFERENCES: Strickland JW: Flexor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 1851-1897.
Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.
97/. A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. What type of injury pattern is shown?
1- Scaphoid fracture
2- Radiocarpal dislocation
3- Midcarpal dislocation
4- Transscaphoid dorsal perilunate dislocation
5- Volar lunate dislocation
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a transscaphoid dorsal perilunate dislocation. The radiographs clearly define a dorsal dislocation of the capitolunate joint, and the scaphoid fracture component is easily visible on the AP view. A scaphoid fracture alone is an unlikely diagnosis because of the midcarpal dislocation component. The radiocarpal joint is not dislocated because the lunate is sitting in the lunate fossa of the radius. Isolated radiocarpal dislocations are not associated with a midcarpal disruption. While a midcarpal dislocation is a component of a dorsal perilunate dislocation, this diagnosis does not address the scaphoid fracture. A volar lunate dislocation is not seen because the lunate is reduced in the lunate fossa of the distal radius. Volar lunate dislocations are in the spectrum of injury of perilunate dislocations and fracture-dislocations; however, the radiographs show a transscaphoid dorsal perilunate dislocation.
REFERENCES: Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
98/. A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of
1- closed reduction and a long arm cast.
2- closed reduction, percutaneous pin fixation, and a long arm cast.
3- closed reduction and an external fixator.
4- open reduction and internal fixation and soft-tissue repair.
5- proximal row carpectomy.
PREFERRED RESPONSE: 4
DISCUSSION: Open reduction and internal fixation is the treatment of choice for accurate reduction of the disrupted intercarpal ligaments. In addition, the displaced scaphoid fracture will require open reduction and internal fixation and possible bone grafting. Closed reduction and long arm casting will not allow accurate reduction of the dislocated intracarpal intervals, and it is unlikely to allow accurate reduction of the scaphoid. The maneuver required to effect closed reduction of a displaced scaphoid fracture will most likely cause the scaphoid lunate interval to displace. Closed reduction with percutaneous pin fixation or with an external fixator is unable to effect anatomic reduction of the injury. Proximal row carpectomy is used as a salvage procedure for a variety of degenerative and posttraumatic problems of the wrist.
REFERENCES: Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Sotereanos DG, Mitsionis GJ, Ginnakopoulos PN, Tomaino MM, Herndon JH: Perilunate dislocation and fracture dislocation: A critical analysis of the volar-dorsal approach. J Hand Surg Am 1997;22:49-56.
99/. A 17-year-old boy who fell on a pitchfork in a barn 1 day ago now has a painful, swollen forearm. Examination reveals erythema, exquisite tenderness, and crepitus to palpation of the forearm. He has a pulse rate of 110/min and a blood pressure of 80/60 mm Hg. Radiographs show subcutaneous air and no fractures. Gram stain of wound drainage reveals a gram-positive bacillus. The next most appropriate step in management should consist of
1- surgical debridement with wound closure and IV antibiotics.
2- surgical debridement with wound closure over suction drains and IV antibiotics.
3- surgical debridement with open wound management and IV antibiotics.
4- IV antibiotics alone.
5- hyperbaric oxygen therapy.
PREFERRED RESPONSE: 3
DISCUSSION: The successful treatment of necrotizing soft-tissue infections such as clostridial myonecrosis depends on prompt recognition and aggressive surgical debridement of all involved muscle, fascia, and soft tissue, resecting to a clearly normal healthy, viable margin. The effective antibiotic regimen for clostridial infection is high-dose penicillin; however, necrotizing infections are frequently polymicrobial so initially broad-spectrum antibiotics are indicated. Hyperbaric oxygen therapy may be used as an adjunct to surgical treatment but is insufficient as a primary therapy. Prolonged application of tourniquets and wound closure should be avoided.
REFERENCES: Pellegrini VD, Evarts CM: Complications, in Rockwood CA Jr, Green DP (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 365-370.
Gerding DN, Peterson LR: Infections caused by anaerobic bacteria, in Shulman ST, Phair JP, Peterson LR, Warren JR (eds): Infectious Diseases, ed 5. Philadelphia, PA, WB Saunders, 1997, pp 416-417.
Stephens DC: Myositis and fascitis, in Root RK (ed): Clinical Infectious Diseases, ed 1. Oxford, England, Oxford Press University, 1999, pp 769-770.
100. In the management of an open tibia fracture, what factor is considered most important in preventing deep infection?
1- Size of the skin lesion
2- Degree and the completeness of the debridement
3- Amount of contamination
4- Method of fixation
5- Cultures of the wound
PREFERRED RESPONSE: 2
DISCUSSION: The most important aspect of management of any open fracture, and in particular the tibia, is the degree and the completeness of the debridement of the soft tissue and most importantly, the muscle. The ultimate function is determined by the amount of muscle left, as well as the ability to heal. The amount of necrotic muscle left in the wound also determines the predisposition to infection. The method of fixation, the size of the wound, and the amount of contamination are controlled by the surgeon or the injury and have little to do with the long-term outcome. Initial wound cultures have little predictive value.
REFERENCES: Clifford P: Open fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 617-638.
Lee J: Efficacy of cultures in the management of open fractures. Clin Orthop 1997;339:71-75.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 37High Yield
A 34-year-old man sustained a tibial fracture in a motorcycle accident. What perioperative variable is associated with the greatest relative risk for reoperation to achieve bone union?
Explanation
In a recent analysis of 200 patients with tibial fractures, Bhandari and associates attempted to identify variables that were predictive of reoperation. The variables in the study were type of injury (fracture pattern), degree of open injury, mechanism of injury, cortical bone contact, postoperative complications, polytrauma, anti-inflammatory drug use, nail insertion technique (reamed versus nonreamed), smoking history, alcohol use, diabetes mellitus, peripheral vascular disease, age, disability status pre-injury, gender, surgeon, time to surgery, steroid use, phenytoin use, antibiotic use, anticoagulant use, and type of fixation used. Three variables were statistically significant predictors of reoperation to achieve bone union in the first postinjury year: transverse fracture pattern, open fracture, and cortical contact of 50% or less. Using these three variables, four reoperation risk groups were identified based on the number of these three variables present: 0, 1, 2, or 3. The risk for reoperation was 0%, 18%, 47%, and 94%, respectively. The authors concluded that these statistics can provide prognostic information to patients and help identify those high-risk patients where early intervention to achieve union is indicated. In addition, the data highlights the significance of achieving cortical contact at the time of initial fixation.
REFERENCE: Bhandari M, Tornetta P III, Sprague S, et al: Predictors of reoperation following operative management of fractures of the tibial shaft. J Orthop Trauma 2003;17:353-361.
REFERENCE: Bhandari M, Tornetta P III, Sprague S, et al: Predictors of reoperation following operative management of fractures of the tibial shaft. J Orthop Trauma 2003;17:353-361.
Question 38High Yield
-are the radiographs of a 45-year-old man who fell into a ditch and sustained a twisting injury to the left lower extremity. Examination in the emergency department reveals normal neurologic function, no skin compromise, and palpable pedal pulses. The patient has no other complaints and has an otherwise normal examination. What additional imaging study is recommended?
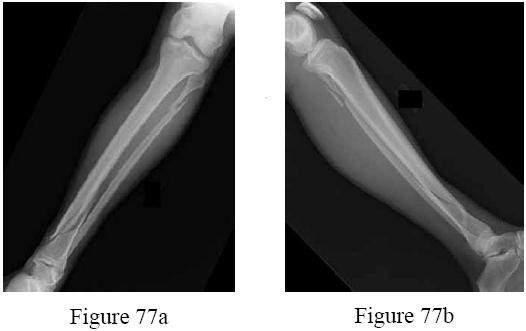
Explanation
No detailed explanation provided for this question.
Question 39High Yield
All of the following are risk factors for malignant melanoma except:
Explanation
Sun exposure is the most important risk factor for melanoma. Family history, atypical nevi, and an immunosuppressive state increases an individual's risk for developing melanoma. It is unknown if tanning lotions cause malignant melanomas.
Question 40High Yield
A hockey player had a puck hit his foot. Radiographs taken immediately after the game were negative. He still has persistent pain 5 days after the injury and difficulty weight bearing. What is the best next step?
Explanation
Ice hockey injuries demand a thorough assessment because they have the potential to be significant. In hockey players, bone injuries in the foot and ankle can be missed or improperly diagnosed through routine radiographic imaging. MRI can display bone injuries that are not found radiographically; this is because _some fractures and contusions involve the medial ankle and midfoot bones._
Question 41High Yield
What is the most important factor in determining recovery after surgical repair of a complete laceration of a nerve at the wrist?
Explanation
All other factors being equal, a patient’s age is the most important factor in determining outcome after peripheral nerve injury. Repair of a nerve laceration within the first 2 weeks is generally considered appropriate. Fascicular repair may be of benefit in larger proximal nerves to reapproximate appropriate nerve bundles; distally perineural or epineural repair is sufficient. Use of a fibrin tissue sealant for nerve repair does not result in improved outcomes over suture repair. Nerve conduits have shown promise in digital nerves but do not have proven benefit in larger caliber nerves.
REFERENCES: Sunderland S: Nerve Injuries and Their Repair: A Critical Appraisal. New York, NY, Churchill Livingstone, 1991.
Wilgis ES, Brushart TM: Nerve repair and grafting, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1325.
Narakas A: The use of fibrin glue in repair of peripheral nerves. Orthop Clin North Am 1988;19:187-199.
Weber RA, Breidenbach WC, Brown RE, et al: A randomized prospective study of
polyglycolic acid conduits for digital nerve reconstruction in humans. Plast Reconstr Surg 2000;106:1036-1045.
REFERENCES: Sunderland S: Nerve Injuries and Their Repair: A Critical Appraisal. New York, NY, Churchill Livingstone, 1991.
Wilgis ES, Brushart TM: Nerve repair and grafting, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1325.
Narakas A: The use of fibrin glue in repair of peripheral nerves. Orthop Clin North Am 1988;19:187-199.
Weber RA, Breidenbach WC, Brown RE, et al: A randomized prospective study of
polyglycolic acid conduits for digital nerve reconstruction in humans. Plast Reconstr Surg 2000;106:1036-1045.
Question 42High Yield
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees
Explanation
DISCUSSION: The history, physical examination, and laboratory studies suggest a septic hip. Recent studies indicate that a child with elevated ESR, a WBC count of greater than 12,000/mm3, a temperature of greater than 38.5 degrees, and unwillingness to walk is very likely to have septic arthritis of the hip versus toxic synovitis. The best way to confirm the diagnosis is by hip aspiration. No medications should be started until a diagnosis is made. Toxic synovitis is common, but significantly less likely if three of the above criteria are present. This condition usually responds well to ibuprofen, but requires close observation. Septic hips are considered urgent conditions and therefore a repeat evaluation in 2 weeks is inappropriate.
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
DISCUSSION: The history, physical examination, and laboratory studies suggest a septic hip. Recent studies indicate that a child with elevated ESR, a WBC count of greater than 12,000/mm3, a temperature of greater than 38.5 degrees, and unwillingness to walk is very likely to have septic arthritis of the hip versus toxic synovitis. The best way to confirm the diagnosis is by hip aspiration. No medications should be started until a diagnosis is made. Toxic synovitis is common, but significantly less likely if three of the above criteria are present. This condition usually responds well to ibuprofen, but requires close observation. Septic hips are considered urgent conditions and therefore a repeat evaluation in 2 weeks is inappropriate.
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 43High Yield
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
1. [Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. ](http://www.ncbi.nlm.nih.gov/pubmed/21823110)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21823110)
2. Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. _Enzinger & Weiss’s Soft Tissue Tumors_. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
3. [Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/27267143)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/27267143)
4. [Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. ](http://www.ncbi.nlm.nih.gov/pubmed/26222558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26222558)
5. [Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.](http://www.ncbi.nlm.nih.gov/pubmed/24898549)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24898549)
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
1. [Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. ](http://www.ncbi.nlm.nih.gov/pubmed/21823110)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21823110)
2. Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. _Enzinger & Weiss’s Soft Tissue Tumors_. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
3. [Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/27267143)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/27267143)
4. [Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. ](http://www.ncbi.nlm.nih.gov/pubmed/26222558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26222558)
5. [Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.](http://www.ncbi.nlm.nih.gov/pubmed/24898549)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24898549)
Question 44High Yield
Which two quadrants of the acetabulum are most at risk for injury by screws during fixation of total hip arthroplasty (THA):
Explanation
The acetabular quadrant system described by Wasielewski and colleagues is useful for determining the location of planned acetabular screw fixation in THA to avoid neurovascular complications. The quadrants are formed by drawing a line from the anterior-superior iliaCspine through the center of the acetabulum and bisecting that line at the center of the acetabulum to form four equal quadrants. The line from the anterior-superior iliaCspine to the center of the acetabulum serves as the dividing line between anterior and posterior, and the bisecting line as the division between superior and inferior.
In cadaver studies, the posterior-superior and posterior-inferior quadrants were shown to have the thickest bone and best potential for obtaining secure fixation with the least risk for injury to vessels. The anterior-superior quadrant (the quadrant of death) and the anterior-inferior quadrant were shown to be the most dangerous quadrants for fixation due to the thin bone and close proximity of the vessels to bone in that region
In cadaver studies, the posterior-superior and posterior-inferior quadrants were shown to have the thickest bone and best potential for obtaining secure fixation with the least risk for injury to vessels. The anterior-superior quadrant (the quadrant of death) and the anterior-inferior quadrant were shown to be the most dangerous quadrants for fixation due to the thin bone and close proximity of the vessels to bone in that region
Question 45High Yield
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B




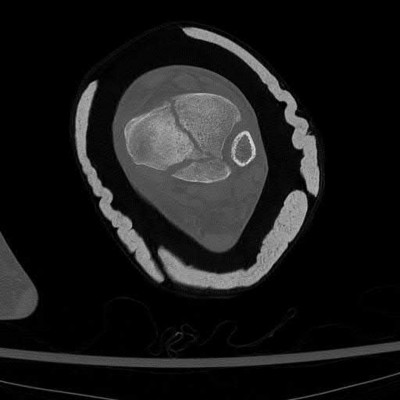








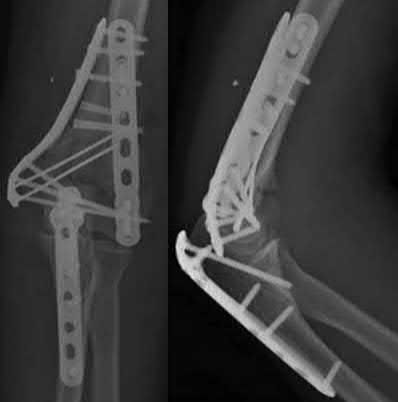
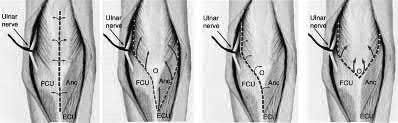
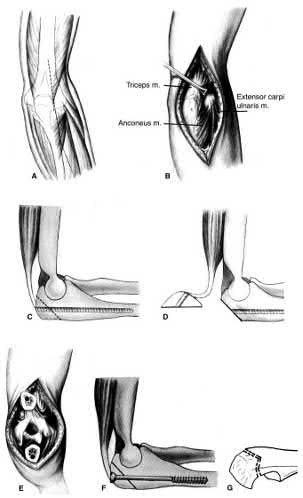







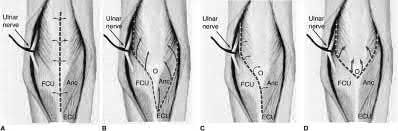











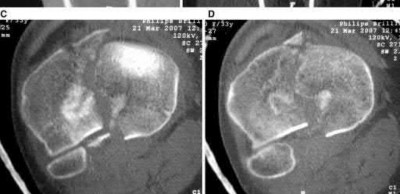






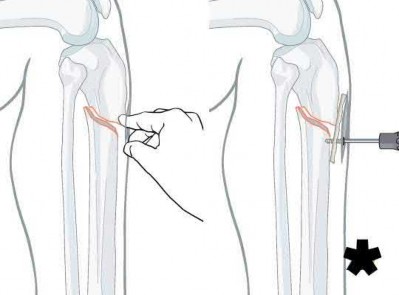


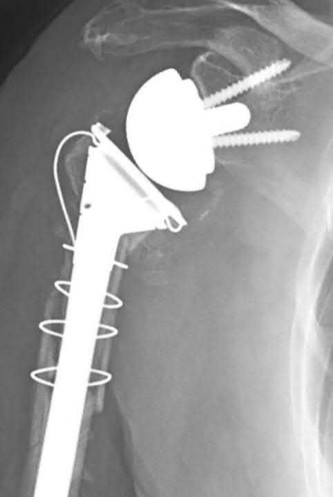
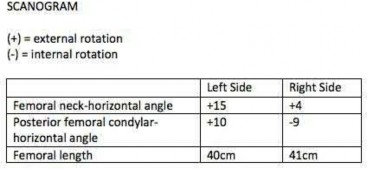

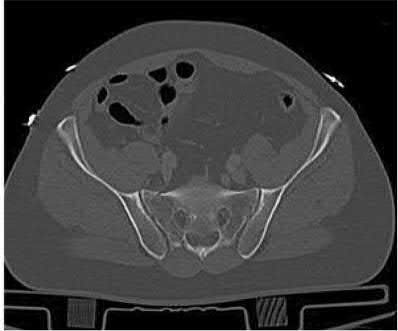
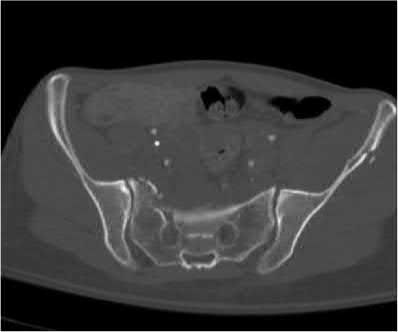
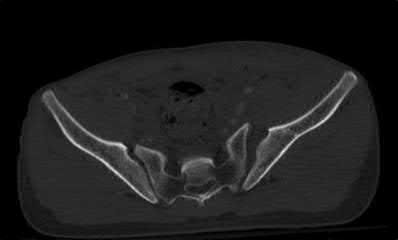
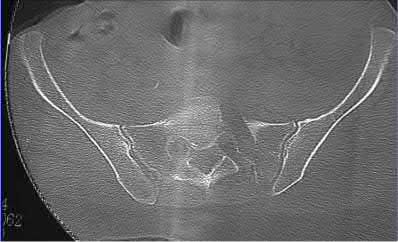



Explanation
This patient has a posterior knee dislocation with an ischemic limb that does not reverse following reduction. Emergent vascular exploration and reconstruction is indicated.
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours.
Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
: The limb remains ischemic. Splinting and observation alone are inappropriate.
Answer 3: External fixation is appropriate for immobilization following reduction, especially for very obese patients (BMI>50) where casting/splinting is not possible, and especially to protect a vascular reconstruction. However, the MOST important next step is vascular exploration to attempt revascularization.
Answers 4 and 5: CT angiography and standard angiography will only serve to delay vascular exploration of the ischemic limb. On-table angiograms will be performed during the surgery, obviating the need for preoperative angiography outside the operating room (OR).
A 51-year-old carpenter presents with a distal humerus nonunion (Figures A and B). After repair of the nonunion, he is lost to follow up for 3 months and then presents to your clinic pain-free and with evidence of fracture union. On examination the elbow arc of motion is 10-80 degrees. Following a brief failed trial of conservative management, you recommend:
1) Open release of the posterior bundle of the MCL and excision of osteophytes
2) Complete open release of the MCL and LCL complexes with radiation for heterotopic ossification prophylaxis
3) Arthroscopic release of the anterior capsule with removal of hardware
4) Removal of hardware and dome osteotomy
5) Functional bracing and recommendation for job retraining
Limited flexion outside a functional range of motion (30-130 degrees) can be quite debilitating, and it is often addressed with open release of the posterior bundle of the MCL and posterior capsule and excision of osteophytes.
A frequent complication of distal humerus fractures is post-traumatic stiffness. This patient has had multiple procedures about the distal humerus, and the question stem implies that he did not complete a structured range of motion protocol following the repair of his nonunion. Beyond a trial of conservative management, there are many techniques described for capsule and soft tissue releases as well as bony resections if heterotopic ossification is present. This patient's severely limited flexion would best be addressed with a release of the posterior bundle of the MCL, and with flexion
A 51-year-old female presents with an acute inability to extend her thumb, four months after she was treated with cast immobilization for a minimally-displaced distal radius fracture. What is the most appropriate treatment at this time?
1) Occupational therapy for strengthening
2) Extensor carpi radialis longus transfer to extensor pollicus longus
3) Extensor pollicis brevis transfer to extensor pollicus longus
4) Extensor indicis proprius transfer to extensor pollicus longus
5) Primary repair of extensor pollicus longus
A rare complication of non-displaced or minimally displaced fractures of the distal radius treated with a cast is a delayed rupture of the extensor pollicis longus (EPL) tendon. The EPL is the primary extensor of the interphalangeal joint of the thumb and also assists with metacarpophalangeal extension.
Extensor indicis proprius transfer to the EPL is the most widely used and reported treatment for this condition.
Magnussen et al. reviewed results of EIP transfer following ruptures of the EPL, with 19/21 good results. None of the cases had any loss of independent index finger extension although index extensor strength reduced to half of that of the contralateral side.
Hove et al. reported a similar satisfaction rate following treatment of 15 patients. In his series of 4,400 distal radius fractures treated over a 5 year period, the incidence of delayed tendon rupture following distal radius fracture was 0.3 percent.
A 25-year-old female is involved in a motor vehicle collision. She presents with the isolated injury seen in Figures A through D. Her leg is swollen but her skin is intact. She has no clinical signs of compartment syndrome. Which of the following treatment options will allow for maintenance of fracture alignment and minimize the risk of soft tissue complications?
1) Closed reduction and long-leg non-weight bearing cast
2) Immediate open reduction of the tibia through an anterolateral approach
3) Percutaneous fixation of the articular surface and intramedullary nailing
4) Definitive uniplanar external fixator
5) Immediate open reduction of the tibia through an anteromedial approach
The patient presents with a closed distal third metaphyseal-diaphyseal distal tibia fracture with simple intra-articular extension. Immediate intramedullary nailing along with percutaneous fixation of the articular component provides appropriate restoration of length, rotation and alignment and minimizes the risk of wound complication.
Displaced distal third tibia fractures may be associated with simple intraarticular extension. Operative treatment of intra-articular distal tibia fractures has historically been performed with open reduction and internal fixation. Early open reduction and plate fixation of pilon fractures has been associated with high rates of infection and wound complication. In select patterns with simple articular extension, percutaneous screw fixation and medullary nailing may provide appropriate reduction with minimal soft-tissue risk.
Marcus et al. evaluated the outcomes of immediate intramedullary nailing and percutaneous fixation of simple intra-articular distal tibia fractures (AO/OTA 43 C1 and C2). The authors found excellent rates of union and alignment, however caution against broad application of this technique until more rigorous randomized studies can be performed.
Sirkin et al. retrospectively evaluated the results of a staged approach to management of intra-articular distal tibia fractures with temporary bridging external fixation followed by open reduction and internal fixation (ORIF). The authors found decreased rates of wound complication and infection compared with prior studies.
Figures A and B demonstrate a distal third tibial shaft fracture with simple intra-articular extension. The axial and coronal CT cuts in Figures C and D further clarify the articular injury. Illustrations A and B demonstrate a comminuted distal third tibial fracture with simple intra-articular extension. Illustrations C and D are fluoroscopic images of the same injury after intramedullary nailing and percutaneous fixation of the articular component.
Incorrect Answers:
Answer 1: Closed reduction and casting of this injury results in increased rates of malalignment
Answers 2 and 5: Immediate open reduction of pilon fractures has historically been associated with high rates of infection and wound complications
Answer 4: This fracture pattern would be difficult to control with a uniplanar fixator. A circular or multiplanar fixator would be a potential treatment option
A 24-year-old woman is thrown from her motorcycle and sustains the closed injury shown in Figures A through C. Open reduction and internal fixation is planned. What surgical technique will best allow visualization of the joint surface and allow early range of motion?
1) Bryan-Morrey approach and parallel plating
2) Triceps reflecting anconeus pedicle approach and parallel plating
3) Triceps reflecting anconeus pedicle approach and orthogonal plating on the posteromedial and lateral surfaces
4) Olecranon osteotomy and parallel plating
5) Olecranon osteotomy and orthogonal plating on the posteromedial and lateral surfaces
Access to complex intra-articular fractures is best achieved by an olecranon osteotomy (OO). Fixation can be with parallel plating or orthogonal plating.
Bicolumnar fixation of distal humerus fractures should follow the principles outlined by O'Driscoll: Distal fragments should be held by as many screws as possible; every screw in the distal fragments should pass through a plate; each screw should engage as many articular fragments as possible.
Galano et al. review treatment for bicolumnar distal humerus fractures. They note that the olecranon osteotomy, Alonso-Llames triceps sparing and Campbell triceps splitting approaches expose 57%, 46% and 35% of the articular surface, respectively. The OO and paratricipital (triceps sparing)
approaches allow for early ROM. Protected motion is required for the O'Driscoll TRAP and Bryan-Morrey approaches for tendon-to-bone healing.
Coles et al. retrospectively reviewed the OO in fixation of 70 fractures. Osteotomy fixation was with an intramedullary screw and dorsal ulnar wiring, or with a plate. The rate of OO increased with fracture difficulty (from AO type C1-C3). There was 1 delayed union but no nonunions.
Figures A and B show a AO/OTA type C2 intraarticular distal humerus fracture. Figure C is a coronal CT scan showing intraarticular comminution. Illustration A shows fixation of the fracture with bicolumnar plating through an olecranon osteotomy approach. Illustration B shows the various approaches to the distal humerus (left, Campbell triceps splitting; center left, O'Driscoll triceps reflecting anconeus pedicle; center right, Bryan-Morrey approach, leaving the triceps attached laterally to the fasciocutaneous flap, but elevating it off the ulna; right, olecranon osteotomy). Illustration C shows 3 methods of olecranon osteotomy (A and B, Intra-articular transverse; C-F, Extra-articular oblique; G, Intra-articular chevron).
Incorrect Answers:
Answer 1: The Bryan-Morrey approach provides excellent medial exposure, but inadequate lateral exposure. The triceps is lifted subperiosteally, and the anconeus is released subperiosteally. Triceps repair depends on tendon-bone healing.
Answer 2: The O'Driscoll TRAP approach detaches triceps and anconeus from their distal insertions in a V-shaped flap that is reflected proximally. Repair to bone is via drill holes in the ulna. Early mobilization is not recommended.
Answers 3 and 5: Orthogonal plating is performed on the POSTEROLATERAL and MEDIAL surfaces.
A 31-year-old male sustains an isolated handgun injury shown in Figure A. On physical examination, he has a 0.5 cm wound over the anteromedial aspect of his thigh, with no gross contamination of the skin edges. He is neurovascularly intact. The patient has received tetanus prophylaxis and antibiotics in the emergency department.
What would next best step in treatment?
1) External fixation and IV antibiotics for 6 weeks
2) Irrigation and debridement of wound and external fixation for 6 weeks
3) Reamed antegrade or retrograde intramedullary nail
4) Irrigation and debridement of wound, reamed antegrade nail and IV antibiotics for 6 weeks
5) Irrigation and debridement of wound, reamed retrograde nail and IV antibiotics for 6 weeks
This patient has sustained a low-velocity gunshot to the right femoral diaphysis. The next best step in treatment would be insertion of a reamed antegrade or retrograde intramedullary nail. During surgery, the gunshot wound could be closed primarily if it was considered clean, or allowed to heal by secondary intention if it was there was any concern.
Low-velocity gunshot wounds are typically treated as closed fractures, since the risk of osteomyelitis is very low. These are typically bullets from handguns that travel 600 meters per second). The timing and direction (e.g. antegrade or retrograde) of nail insertion has not shown to
affect outcomes.
Cannada et al. reviewed 74 cases of femoral diaphyseal fractures caused by gunshots. All were treated with reamed, retrograde, statically locked intramedullary nailing, without formal irrigation and debridement in the operating room. Outcomes showed low incidence of shortening, angular deformity and infection rate.
Dougherty et al. compared retrograde vs. antegrade intramedullary nailing for the treatment of gunshot diaphyseal femur fractures. No significant differences were found between groups with regards to operative time, blood loss, or radiographic union. They conclude that immediate retrograde or antegrade nailing is safe for the early treatment of gunshot femur fractures.
Figure A shows an AP radiograph of the right femur. There is a gunshot fracture in the proximal femoral shaft with retained bullet fragments. The leg has been placed in temporary traction.
Incorrect Answers:
Answer 1: External fixation would be considered for treatment of femur fractures in damage control orthopaedics.
Answer 2: IV antibiotics for 6 weeks would not be necessary with low velocity gunshot wounds with clean wounds.
Answer 4 and 5: The direction of nail entry does not seem to affect outcomes with these fractures. Irrigation and debridement of wound, as well as IV antibiotics, wound not be necessary, aforementioned.
Figure A shows a radiograph of a 19-year-old male with an isolated shotgun injury. On physical examination, he has a 3 cm wound over the posterolateral aspect of his arm. In addition, he has weakness with wrist and finger extension, but no sensory deficits. The patient has received tetanus prophylaxis and antibiotics in the emergency department. What would be the next best steps in treatment?
1) Urgent open reduction internal fixation and fibular osteoseptocutaneous flap
2) Irrigation and debridement and external fixation
3) Irrigation and debridement, repair of the radial nerve and retrograde intramedullary nail
4) CT scan, urgent open reduction internal fixation and IV antibiotics for 6 weeks
5) Closed reduction, CT scan, immobilization in a coaptation splint
This patient has sustained a shotgun blast to the midshaft humerus. The next best step would be irrigation and debridement, and external fixation of the fracture.
Shotgun injuries are typically treated as open fractures, whereas low-energy gunshot wounds are treated as closed fractures. The initial operative treatment of shotgun wounds should include irrigation and debridement and stabilization with external fixation. The goal of treatment is to stabilize the severe soft-tissue injury and bone loss, as well as to aggressively debride devitalized tissue and gross contamination.
Dougherty et al. reviewed gunshot fractures to the humerus. They report that
peripheral nerve injuries are relatively common with these injuries, with a more common incidence in distal injuries than proximal.
Joshi et al. looked at low velocity gunshot fractures to the humerus. They found that these injuries can be safely treated as closed fractures with local wound care, fracture brace and oral antibiotics. The time to union was similar in the non-operative and open treatment group.
Berick et al. examined the indications for nerve exploration with humerus gunshot fractures. They recommend continued observation of isolated nerve palsies associated with gunshot fractures of the humerus. However, consider early nerve exploration of palsies when associated with a concomitant vascular injury.
Figure A shows a high velocity shotgun fracture to the left humerus with retained buck fragments. Illustration A shows a similar injury stabilized with external fixation.
Incorrect Answers:
Answer 1: Due to the severity of soft tissue injury, external fixation should be considered for initial stabilization. Vascularized fibular grafts has been expanded to an osteoseptocutaneous flap by including a cutaneous flap on the lateral aspect of the lower leg. These are not typically used in the acute setting.
Answer 3: Retrograde intramedullary nail would not be the ideal implant for this injury, acutely.
Answer 4 and 5: There is no indication for a CT scan or prolonged antibiotics. The fracture and soft-tissue injury should be initially stabilized with external fixation. Coaptation splinting will interfere with soft tissue care.
A 34-year-old male sustains the closed injury seen in Figure A as a result of a high-speed motor vehicle collision. What is the most appropriate next step in treatment?
1) Open reduction and internal fixation
2) Spanning external fixation
3) Percutaneous internal fixation
4) Closed reduction and cast placement
5) Ankle arthrodesis
The radiograph shows a comminuted pilon fracture, which is associated with high-energy trauma and significant soft tissue injury. The tested concept here is the importance of avoiding definitive reduction and fixation of this high-energy injury, which has been shown to be associated with an increased risk of wound complications and deep infections (as compared to staged treatment with usage of a spanning external fixator).
Patterson et al. reviewed 23 consecutive patients with comminuted distal tibia fractures. They showed 0% infections or wound-healing problems in their patient population treated with a two-staged protocol. Their protocol involved fibula fixation with an intramedullary implant and application of a medial external fixator to to regain length and restore anatomic alignment. Reevaluation of the limb occurred ten to fourteen days later for definitive fixation.
Sirkin et al. retrospectively reviewed 40 closed and 17 open pilon fractures (AO types 43A-C) that were treated with staged surgical management (avg. time from ext. fix. to formal reconstruction was 14 days (range 4 to 31) They reported 17% post-operative wound complication in the closed group and 11% post-operative wound complication in the open group (Gustilo Type I-III). They suggest the technique was successful in both closed and open pilon fractures.
A 72-year-old woman falls down stairs and sustains the injury shown in Figure A. Additional radiographs are performed in Figure B to help assess the fracture pattern. These additional radiographs represent which of the following?
1) Oblique radiographs
2) In-situ radiographs under anesthesia
3) Traction radiographs
4) Fracture flexion radiographs
5) Fracture extension radiographs
Additional traction radiographs are performed in distal humerus fractures to better understand the fracture configuration.
Traction radiographs help align the fracture fragments for better visualization. This is useful in comminuted fractures where distal fragments are telescoped or flexed on the proximal fragments, making CT scan visualization difficult.
Proper visualization can help determine (1) the approach to the distal humerus, (2) whether to perform ORIF or total elbow arthroplasty (in select patients), (3) whether to add a 3rd plate (lateral column), (4) whether to add tricortical bone graft to augment distal fixation and restore trochlear width.
Doornberg et al. examined whether 3D CT improved fracture characterization. They found that 3D CT improved interobserver and intraobserver reliability for fracture characterization and classification. It also improved intraobserver accuracy for fracture characteristics, but not interobserver accuracy. They concluded that 3D CT is helpful for preoperative planning.
Galano et al. reviewed treatment strategies for bicolumnar distal humerus fractures. They state that 3D CT compensates for oblique scans from formatting in an incorrect plane, and allows for subtraction of the radius/ulna to properly demonstrate articular incongruity, degree of comminution and column involvement.
Figures A and B show a distal humerus fracture without traction (A) and with traction (B) applied. Illustration A shows the same fracture after bicolumnar plating. Illustration B shows the different surgical approaches to the distal humerus (A, Campbell triceps splitting; B, O'Driscoll triceps reflecting anconeus pedicle [TRAP]; C, Bryan-Morrey triceps reflecting; D, olecranon osteotomy)
Incorrect Answers:
Answer 1: These radiographs aren't oblique images.
Answer 2: Radiographs under anesthesia do not add further information unless traction is applied.
Answers 4 and 5: Flexion and extension will further impact and displaced fragments and will not improve alignment.
Mirror therapy is indicated for which of the following clinical conditions?
1) Impaired proprioception after lower extremity injury
2) Two-stage flexor tendon reconstruction
3) Plumbism
4) Anterior cruciate ligament reconstruction
5) Phantom pain
Mirror therapy is a useful technique to improve phantom pain in amputees. Phantom limb pain is a painful sensation that is perceived within a body part that no longer exists.
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Answer 1: Mirror therapy is not indicated for proprioception training. Answer 2: Mirror therapy is not indicated for flexor tendon injuries. Answer 3: Mirror therapy is not indicated for lead poisoning.
Answer 4: Mirror therapy is not indicated for ACL reconstruction.
A patient presents to the emergency department with the injury seen in Figure A. Which of the following is true about radial nerve palsies associated with isolated humeral shaft fractures after low velocity gunshot wounds?
1) The initial treatment involves debridement, irrigation, nerve exploration, and osteosynthesis.
2) The radial nerve palsy is often a result of neurotmesis.
3) Initial treatment involves splinting and observation for return of neurologic function.
4) Electrophysiologic testing for radial nerve palsies is indicated after 2-3 weeks without improvement.
5) The radial nerve palsy will not resolve regardless of attempted interventions.
When a patient sustains an isolated humeral shaft fracture and radial nerve palsy from a GSW, the initial treatment involves splinting with observation.
The majority of humeral shaft fractures are treated initially with a coaptation splint and then transitioned to a functional brace. Absolute surgical indications for operative management include: open fracture, brachial plexus injury, compartment syndrome, floating elbow, or vascular injury. A radial nerve palsy is not an indication for surgical management of an isolated humeral shaft fracture. Radial nerve injury from a low-velocity GSW is similar to that of blunt force trauma and thus, immediate exploration is not necessary. Instead, nerve function should be observed. Seventy percent of these nerve injuries will resolve spontaneously. Additionally, the patient should receive a short course of antibiotics as any low velocity GSW would be treated.
Guo et al retrospectively reviewed the electrophysiologic data for 40 radial nerve palsies caused by GSWs and blunt trauma. After characterizing the palsies by level of injury, completeness of nerve injury, and other associated nerves injured, they found there to be no difference in any of these variables between GSW induced radial nerve palsies and blunt trauma induced palsies.
Vaidya et al retrospectively reviewed the outcomes of 54 patients with humeral shaft fractures resulting from low velocity GSWs comparing operative and nonoperative treatments. They found that patients receiving non-operative management did well and that 70% of radial nerve palsies in the non-operative treatment group resolved on their own. They recommended non-operative treatment for the majority of isolated humeral shaft fractures resulting from civilian gunshot wounds.
Figure A is a radiograph of a humeral shaft fracture after a GSW. Illustration A is a radiograph of a humeral shaft fracture with a coaptation in place.
Illustration B is an example of a functional brace.
Incorrect answers:
Answer 1: This is the initial treatment for an open humeral shaft fracture associated with an radial nerve palsy.
Answer 2: Radial nerve palsy from a low velocity GSW is usually axonotmesis. Neurotmesis the most common injury in open fractures.
Answer 4:EMG testing is not indicated until 3-4 months of radial nerve palsy with no neural recovery.
Answer 5: Seventy percent of radial nerve palsies will spontaneously resolve
A 76-year-old male community ambulatory presented to clinic complaining of pain in the left groin that has been persistent for the last 8 months. Radiographs obtained from clinic are seen in Figure A. You suspect a femoral neck nonunion and obtain a CT scan which confirmed it. Which of the following statements is true?
1) Total hip arthroplasty will provide patient with the best long term outcomes
2) Valgus malreduction is closely correlated with failure of fixation after reduction and cannulated screw fixation
3) The patient's best outcome would be with an open reduction, bone grafting, and changing to an inverted triangle configuration of screws
4) The most appropriate treatment is a valgus osteotomy to correct malreduction
5) Providing this patient with a hemiarthroplasty increases rates of postoperative dislocation when comparing to total hip arthroplasty
A total hip arthroplasty (THA) after nonunion of a femoral neck fracture would provide the best long term outcomes in a 76-year-old male who is a community ambulator.
After nonunion of a femoral neck fracture, hemiarthroplasty and THA are good salvage option for the physiologically older patients. When deciding between these two options, THA is better for active and cognitively intact patients. THA is also indicated in patients with radiographic evidence of degenerative disease about the acetabulum. Hemiarthroplasty is advocated for patients who are older and less active.
Yang et al. retrospectively investigated the risk factors for nonunion in patients treated with cannulated screws. They reviewed 202 patients who had femoral neck fractures and were treated with internal fixation with cannulated screws. They identified that triangle configuration, displaced fracture, borderline or unacceptable reduction, and increased screw shaft subchondral purchase over the femoral neck were all risk factors for nonunion after internal fixation.
Inverted triangle configuration was found to increase rate of union.
Archibeck et al. retrospectively reviewed the outcomes of 102 THAs after failed internal fixation for a hip fracture (including both femoral neck and intertrochanteric). They concluded that the conversion of failed hip internal fixation has elevated risks compared to a primary THA, however, it may still be successful. The biggest concern for these patients postoperatively are periprosthetic fracture and dislocation.
Figures and Illustrations:
Figure A is an AP pelvic radiograph demonstrating a nonunion of a femoral neck fracture after suboptimal fixation with 3 cannulated screws in a triangle configuration.
Illustration A is an AP radiograph of the left hip in this patient following conversion to THA.
Illustration B is a radiograph demonstrating a valgus osteotomy. Illustration C shows an example of a femoral neck nonunion with varus malreduction.
Incorrect Answers:
Answer 2: Varus reduction is closely correlated with failure in this fixation method.
Answer 3: The patient's best outcome would be with THA.
Answer 4: This would be a good option in a younger patient, but given age and functional capacity, the best option is THA.
Answer 5: Patients with hemiarthroplasty have lower rates of dislocation.
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?
1) Non-operative managment, but arrange for early follow-up in clinic
2) Intra-compartmental pressure measurements
3) Ankle-brachial index measurements
4) Knee spanning external fixation
5) Open reduction internal fixation
This patient presents with a Schatzker IV tibia plateau fracture with lower extremity neurologic deficits. The next best step would be to investigate for an acute vascular injury with ankle-brachial index measurements.
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
1) Splint until swelling subsides, then long-arm cast
2) Excision of fracture fragments
3) Closed reduction and percutaneous pinning
4) Open reduction and internal fixation (ORIF)
5) Radial head replacement
This patient has Mason II radial head fracture. ORIF will give the best results.
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF
group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
Answer 1: Nonoperative management is indicated for non-/minimally displaced fractures.
Answer 2: Excision is an option for small partial articular fragments = 3 fragments.
When placing an intramedullary nail for closed distal tibia shaft fractures, all of the following methods are described techniques to aid anatomic reduction EXCEPT:
1) Plating of a concomitant fibula fracture
2) Percutaneous placement of reduction foreceps at the fracture site
3) Placing a Poller screw
4) Placing a small-fragment plate at the fracture site
5) Placing syndesmotic fixation
Of the choices above, syndesmotic fixation would not help anatomically reduce these fractures.
Fractures of the distal tibia are challenging fractures to achieve an anatomic reduction. The medullary canals at either end of the tibia are capacious compared to the mid-diaphysis thus inhibiting an endosteal fit. These fractures have a tendency to become mal-aligned unless certain steps are taken to ensure restoration of the length, alignment, and rotation. Using a Poller or blocking screw can function to narrow the space available for the nail to guide the nail or correct deformity. The use of large pointed-reduction forceps or a small frag plate may also be used for provisional fixation. Additionally, plating concomitant fibula fractures may help indirectly restore length and reduce the tibia fracture. Concomitant syndesmotic injuries are not commonly seen and fixation for these is not required unless stress exam clearly demonstrates it.
Casstevens et al. reviewed the surgical management of distal tibia fractures using either plates/screws or intramedullary nails. Current literature shows near equivalence of either technique regarding union and alignment. They recommend treating each fracture on a case-by-case basis with consideration of the soft tissues and fracture pattern when determining fixation choices.
Tejwani et al. reviewed surgical techniques for managing metaphyseal and meta-diaphysial tibia fractures. Advances in tibial nail design have helped tremendously in negotiating these fractures. Though current supporting literature is based mostly on case series, the use of suprapatellar entry intramedullary nails may help avoid the common deformity of procurvatum and valgus seen with proximal tibia fractures.
Egol et al. retrospectively reviewed distal tibial shaft fracture undergoing intramedullary nailing, with and without concomitant fibula fracture plate fixation. They found fractures with fibular fixation maintained better alignment beyond 12 week post-operatively than those without fixation. Given these findings they recommended fibular plating for all distal tibial shaft fractures.
Illustration A shows a fibula fracture that was plated prior to tibia IMN placement. Illustrations B and C show the use of pointed reduction forceps placed percutaneously to reduce the fracture. Illustration D shows the use of a blocking screw (denoted by the arrow) to keep the nail lateralized and the fracture out of valgus. Illustration E shows the use of a plate to reduce the fracture prior to nail placement.
Incorrect Answers:
Answers 1, 2, 3, and 4: All of these have been described in the literature to help aid in reducing these fractures
A 70-year-old woman falls down a flight of stairs and sustains the injury shown in Figures A and B to her dominant upper extremity. She lives alone and has no other medical history. Which of the following surgical options is best to minimize complications for this fracture pattern?
1) Open reduction and internal fixation with a long locking plate
2) Uncemented reverse total shoulder arthroplasty with tuberosity repair
3) Cemented reverse total shoulder arthroplasty without tuberosity repair
4) Cemented reverse total shoulder arthroplasty with tuberosity repair
5) Proximal humeral resection with endoprosthetic replacement
This patient has a complex proximal humerus fracture with metaphyseal comminution and poor bone stock. Cemented reverse total shoulder arthroplasty (rTSA) using a long stem prosthesis and tuberosity repair is indicated.
Proximal humerus fragility fractures are hard to treat because of comminution and poor bone stock. AVN is common with glenohumeral fracture-dislocation. Hemiarthroplasty (and standard total shoulder arthroplasty, TSA) is unreliable because of dependence on tuberosity healing. rTSA is recommended for fractures in patients >70 years with severely comminuted fractures, high likelihood of head AVN, and poor tuberosity bone quality (osteoporosis or comminution).
Bufquin et al. retrospectively reviewed the use of rTSA for treatment of 43 patients with 3- and 4-part proximal humerus fractures. They found satisfactory elevation (97°), ER in abduction (30°), constant scores (44) and modified Constant scores (66%). Complications included calcification (90%), tuberosity displacement (53%) and scapular notching (25%). They concluded that rTSA was a good procedure because it provides pain relief and easier functional recovery in spite of failed tuberosity healing.
Anakwenze et al. systematically reviewed acute proximal humerus fractures. Frequency weighted range of motion was flexion 122°, abduction 97°, ER at neutral 18°. Tuberosity repair yielded higher ER compared to no repair.
Scapular notching was the most common complication (32%). They concluded that rTSA patients tended to be elderly women with 4-part fractures, had good pain control but residual dysfunction.
Jobin et al. reviewed rTSA for management of proximal humerus 3- and 4-part fractures. They note >50% of cases have tuberosity resorption. They recommend repairing the greater tuberosity to restore infraspinatus/teres minor function which improves external rotation strength. Greater tuberosity malunion is not a result of secondary displacement, but rather, from intraoperative malreduction. Lesser tuberosity repair should be performed if there is significant bone loss or intraoperative anterior instability.
Figures A and B are AP radiograph and 3D reformatted CT scan showing comminuted proximal humerus fracture dislocation. Illustration A shows rTSA performed with distal cementation of a long stem prosthesis and cerclage fixation of the proximal shaft and the tuberosity fragments.
Incorrect Answers:
Answer 1: ORIF has potential complications of screw cut out, AVN, fracture collapse, tuberosity resorption and loss of fixation. The risk of AVN (and resultant screw cut out) is high because of comminuted fracture-dislocation. Answer 2: Cementing is indicated because metaphyseal fracture bone loss compromises stem fixation.
Answer 3: Greater tuberosity repair improves external rotation strength. Lesser tuberosity repair adds to anterior stability.
Answer 5: Proximal humeral replacement is only necessary for tumor or unreconstructable fractures. They have poorer outcomes because of loss of rotator cuff function.
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-
operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
1) Observation and close follow-up
2) Dynamization of the intramedullary nail
3) Revision surgery, internally rotate distal fragment by 19 degrees
4) Revision surgery, externally rotate distal fragment by 8 degrees
5) Revision surgery, internally rotate proximal fragment by 11 degrees
The CT scanogram shows the operative left femur is 8 degrees externally rotated compared to the native right femur. No correction is required unless malalignment is >15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles.
This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH - PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs.
Therefore 15 degrees and symptomatic.
Which of the following images shows an injury pattern most consistent with a lateral compression type 3 pelvic ring injury?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure C is an axial CT scan of a lateral compression type 3 (LC3) pelvic ring injury.
Classically, LC3 injuries demonstrate an ipsilateral lateral compression and a contralateral APC (windswept pelvis) fracture pattern. The most common mechanism of injury in these cases is a rollover MVC or pedestrian vs. auto. LC1 injuries are characterized by an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture, while LC2 injuries consist of a rami fracture and ipsilateral posterior ilium fracture dislocation (crescent fracture). While LC1 injuries can often initially be managed conservatively with protected weight-bearing and close observation, LC2 and LC3 pelvic ring injuries are almost universally operative.
Pennal et al. discuss a radiologic technique for assessing the forces producing pelvic disruption and its use in logically classifying pelvic injury. Based on this radiologic assessment and along with some biomechanical studies, they propose a classification system involving three major forces producing injury that can also be helpful in the management of these patients.
Young et al. performed a retrospective analysis of the plain radiographs of 142 cases of pelvic fractures and identified four patterns of force that presented with distinctive, recognizable radiographic appearances. They describe a classification system for pelvic fractures based on radiographic and clinical findings that correlates with associated injury to soft-tissue structures and enables the surgeon to begin corrective procedures rapidly.
Incorrect Answers:
Answer 1: This represents a lateral compression type 2 injury. Answer 2: This represents a lateral compression type 1 injury.
Answer 4: This represents an anterior posterior compression type 2 injury. Answer 5: This represents an anterior posterior compression type 3 injury.
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?
1) Length of hospital stay
2) Association with neurological deficit(s)
3) Length of intensive care stay
4) Cardiac collapse
5) Mortality
Unstable pelvic fractures can be devastating injuries often resulting in significant morbidity and even death.
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (24 hours).
Incorrect Answers: Choices 1-4 do not correlate with increased blood transfusions to the extent of Option 5.
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
1) Reduced radial artery pulse
2) Double break in the ipsilateral superior shoulder suspensory complex
3) Elevated hemidiaphragm
4) Musculocutaneous nerve deficit
5) Drooping of the left eyelid
Drooping of the left eyelid is a presenting feature of Horner's syndrome. Horner's syndrome represents a disruption of the sympathetic chain via C8 and/or T1 root avulsion after trauma.
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity = 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Answer 1, 2: The superior shoulder suspensory complex (SSSC) is located in close proximity to the brachial plexus. Disruption of the SSSC may affect the local anatomy and cause local brachial plexus or vascular injury.
Answer 3: Elevated hemidiaphragm (Phrenic nerve C3,4,5) may be suggestive an upper brachial plexus root avulsion, e.g. C5, C6 injury.
Answer 4: Musculocutaneous nerve deficiency (C5 deficiency) results in weakness to the biceps.
A 46-year-old competitive cyclist falls while racing and suffers an isolated fracture as seen in Figure A. He is positioned on a fracture table and a closed reduction maneuver is attempted, unsuccessfully.
Which of the following treatment plans is most appropriate?
1) Obtain a CT scan intraoperatively to reassess the quality of reduction
2) Perform additional closed reduction maneuvers until the reduction is adequate for percutaneous fixation
3) As long as the stepoff is less than 7mm in any plane of imaging, it is appropriate to proceed with percutaneous fixation
4) Perform an open reduction and internal fixation using a sliding hip screw
5) Perform an acute total hip arthroplasty through a direct anterior approach since the patient is on the fracture table
When standard closed reduction maneuvers using a traction table are unsuccessful, displaced femoral neck fracture in young adults (10 degrees varus/valgus or anteversion/retroversion) or has
significant displacement (5 mm or more in ANY view) is unacceptable, and an open reduction should be performed. Of course, this can be very difficult to assess in the operating room, where uncalibrated fluoroscopy with difficult to obtain tangential imaging is heavily relied upon to make this assessment.
Accordingly, when the quality of closed reduction is questionable, the best treatment plan is to obtain a better reduction with direct visualization of the femoral neck prior to fixation.
A systematic review of the literature by Pauyo, et al. cites numerous studies showing a higher incidence of osteonecrosis of the femoral head in patients with displaced femoral neck fractures treated with unsatisfactory reductions. Furthermore, performing multiple closed reduction attempts is also associated with a higher risk of osteonecrosis.
Upadhyay et al. performed a randomized controlled trial of 102 patients with femoral neck fractures treated with closed or open reductions, which were randomized. The groups had similar rates of nonunions and osteonecrosis of the femoral head; however, subanalysis revealed a "poor" reduction was the highest predictor of poor outcome, whether the reduction was attempted open or closed. Interestingly, the quality of reduction was more important than the implant used or the timing of surgery (including surgeries performed > 48h after injury).
Figure A shows a pre-operative AP x-ray of the patient's high-energy femoral neck fracture. Illustrations A and B are intraoperative fluoroscopic and postoperative CT scans of this same patient, highlighting that fluoroscopy may "hide" the degree of residual displacement.
Incorrect Answers:
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours.
Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
: The limb remains ischemic. Splinting and observation alone are inappropriate.
Answer 3: External fixation is appropriate for immobilization following reduction, especially for very obese patients (BMI>50) where casting/splinting is not possible, and especially to protect a vascular reconstruction. However, the MOST important next step is vascular exploration to attempt revascularization.
Answers 4 and 5: CT angiography and standard angiography will only serve to delay vascular exploration of the ischemic limb. On-table angiograms will be performed during the surgery, obviating the need for preoperative angiography outside the operating room (OR).
A 51-year-old carpenter presents with a distal humerus nonunion (Figures A and B). After repair of the nonunion, he is lost to follow up for 3 months and then presents to your clinic pain-free and with evidence of fracture union. On examination the elbow arc of motion is 10-80 degrees. Following a brief failed trial of conservative management, you recommend:
1) Open release of the posterior bundle of the MCL and excision of osteophytes
2) Complete open release of the MCL and LCL complexes with radiation for heterotopic ossification prophylaxis
3) Arthroscopic release of the anterior capsule with removal of hardware
4) Removal of hardware and dome osteotomy
5) Functional bracing and recommendation for job retraining
Limited flexion outside a functional range of motion (30-130 degrees) can be quite debilitating, and it is often addressed with open release of the posterior bundle of the MCL and posterior capsule and excision of osteophytes.
A frequent complication of distal humerus fractures is post-traumatic stiffness. This patient has had multiple procedures about the distal humerus, and the question stem implies that he did not complete a structured range of motion protocol following the repair of his nonunion. Beyond a trial of conservative management, there are many techniques described for capsule and soft tissue releases as well as bony resections if heterotopic ossification is present. This patient's severely limited flexion would best be addressed with a release of the posterior bundle of the MCL, and with flexion
A 51-year-old female presents with an acute inability to extend her thumb, four months after she was treated with cast immobilization for a minimally-displaced distal radius fracture. What is the most appropriate treatment at this time?
1) Occupational therapy for strengthening
2) Extensor carpi radialis longus transfer to extensor pollicus longus
3) Extensor pollicis brevis transfer to extensor pollicus longus
4) Extensor indicis proprius transfer to extensor pollicus longus
5) Primary repair of extensor pollicus longus
A rare complication of non-displaced or minimally displaced fractures of the distal radius treated with a cast is a delayed rupture of the extensor pollicis longus (EPL) tendon. The EPL is the primary extensor of the interphalangeal joint of the thumb and also assists with metacarpophalangeal extension.
Extensor indicis proprius transfer to the EPL is the most widely used and reported treatment for this condition.
Magnussen et al. reviewed results of EIP transfer following ruptures of the EPL, with 19/21 good results. None of the cases had any loss of independent index finger extension although index extensor strength reduced to half of that of the contralateral side.
Hove et al. reported a similar satisfaction rate following treatment of 15 patients. In his series of 4,400 distal radius fractures treated over a 5 year period, the incidence of delayed tendon rupture following distal radius fracture was 0.3 percent.
A 25-year-old female is involved in a motor vehicle collision. She presents with the isolated injury seen in Figures A through D. Her leg is swollen but her skin is intact. She has no clinical signs of compartment syndrome. Which of the following treatment options will allow for maintenance of fracture alignment and minimize the risk of soft tissue complications?
1) Closed reduction and long-leg non-weight bearing cast
2) Immediate open reduction of the tibia through an anterolateral approach
3) Percutaneous fixation of the articular surface and intramedullary nailing
4) Definitive uniplanar external fixator
5) Immediate open reduction of the tibia through an anteromedial approach
The patient presents with a closed distal third metaphyseal-diaphyseal distal tibia fracture with simple intra-articular extension. Immediate intramedullary nailing along with percutaneous fixation of the articular component provides appropriate restoration of length, rotation and alignment and minimizes the risk of wound complication.
Displaced distal third tibia fractures may be associated with simple intraarticular extension. Operative treatment of intra-articular distal tibia fractures has historically been performed with open reduction and internal fixation. Early open reduction and plate fixation of pilon fractures has been associated with high rates of infection and wound complication. In select patterns with simple articular extension, percutaneous screw fixation and medullary nailing may provide appropriate reduction with minimal soft-tissue risk.
Marcus et al. evaluated the outcomes of immediate intramedullary nailing and percutaneous fixation of simple intra-articular distal tibia fractures (AO/OTA 43 C1 and C2). The authors found excellent rates of union and alignment, however caution against broad application of this technique until more rigorous randomized studies can be performed.
Sirkin et al. retrospectively evaluated the results of a staged approach to management of intra-articular distal tibia fractures with temporary bridging external fixation followed by open reduction and internal fixation (ORIF). The authors found decreased rates of wound complication and infection compared with prior studies.
Figures A and B demonstrate a distal third tibial shaft fracture with simple intra-articular extension. The axial and coronal CT cuts in Figures C and D further clarify the articular injury. Illustrations A and B demonstrate a comminuted distal third tibial fracture with simple intra-articular extension. Illustrations C and D are fluoroscopic images of the same injury after intramedullary nailing and percutaneous fixation of the articular component.
Incorrect Answers:
Answer 1: Closed reduction and casting of this injury results in increased rates of malalignment
Answers 2 and 5: Immediate open reduction of pilon fractures has historically been associated with high rates of infection and wound complications
Answer 4: This fracture pattern would be difficult to control with a uniplanar fixator. A circular or multiplanar fixator would be a potential treatment option
A 24-year-old woman is thrown from her motorcycle and sustains the closed injury shown in Figures A through C. Open reduction and internal fixation is planned. What surgical technique will best allow visualization of the joint surface and allow early range of motion?
1) Bryan-Morrey approach and parallel plating
2) Triceps reflecting anconeus pedicle approach and parallel plating
3) Triceps reflecting anconeus pedicle approach and orthogonal plating on the posteromedial and lateral surfaces
4) Olecranon osteotomy and parallel plating
5) Olecranon osteotomy and orthogonal plating on the posteromedial and lateral surfaces
Access to complex intra-articular fractures is best achieved by an olecranon osteotomy (OO). Fixation can be with parallel plating or orthogonal plating.
Bicolumnar fixation of distal humerus fractures should follow the principles outlined by O'Driscoll: Distal fragments should be held by as many screws as possible; every screw in the distal fragments should pass through a plate; each screw should engage as many articular fragments as possible.
Galano et al. review treatment for bicolumnar distal humerus fractures. They note that the olecranon osteotomy, Alonso-Llames triceps sparing and Campbell triceps splitting approaches expose 57%, 46% and 35% of the articular surface, respectively. The OO and paratricipital (triceps sparing)
approaches allow for early ROM. Protected motion is required for the O'Driscoll TRAP and Bryan-Morrey approaches for tendon-to-bone healing.
Coles et al. retrospectively reviewed the OO in fixation of 70 fractures. Osteotomy fixation was with an intramedullary screw and dorsal ulnar wiring, or with a plate. The rate of OO increased with fracture difficulty (from AO type C1-C3). There was 1 delayed union but no nonunions.
Figures A and B show a AO/OTA type C2 intraarticular distal humerus fracture. Figure C is a coronal CT scan showing intraarticular comminution. Illustration A shows fixation of the fracture with bicolumnar plating through an olecranon osteotomy approach. Illustration B shows the various approaches to the distal humerus (left, Campbell triceps splitting; center left, O'Driscoll triceps reflecting anconeus pedicle; center right, Bryan-Morrey approach, leaving the triceps attached laterally to the fasciocutaneous flap, but elevating it off the ulna; right, olecranon osteotomy). Illustration C shows 3 methods of olecranon osteotomy (A and B, Intra-articular transverse; C-F, Extra-articular oblique; G, Intra-articular chevron).
Incorrect Answers:
Answer 1: The Bryan-Morrey approach provides excellent medial exposure, but inadequate lateral exposure. The triceps is lifted subperiosteally, and the anconeus is released subperiosteally. Triceps repair depends on tendon-bone healing.
Answer 2: The O'Driscoll TRAP approach detaches triceps and anconeus from their distal insertions in a V-shaped flap that is reflected proximally. Repair to bone is via drill holes in the ulna. Early mobilization is not recommended.
Answers 3 and 5: Orthogonal plating is performed on the POSTEROLATERAL and MEDIAL surfaces.
A 31-year-old male sustains an isolated handgun injury shown in Figure A. On physical examination, he has a 0.5 cm wound over the anteromedial aspect of his thigh, with no gross contamination of the skin edges. He is neurovascularly intact. The patient has received tetanus prophylaxis and antibiotics in the emergency department.
What would next best step in treatment?
1) External fixation and IV antibiotics for 6 weeks
2) Irrigation and debridement of wound and external fixation for 6 weeks
3) Reamed antegrade or retrograde intramedullary nail
4) Irrigation and debridement of wound, reamed antegrade nail and IV antibiotics for 6 weeks
5) Irrigation and debridement of wound, reamed retrograde nail and IV antibiotics for 6 weeks
This patient has sustained a low-velocity gunshot to the right femoral diaphysis. The next best step in treatment would be insertion of a reamed antegrade or retrograde intramedullary nail. During surgery, the gunshot wound could be closed primarily if it was considered clean, or allowed to heal by secondary intention if it was there was any concern.
Low-velocity gunshot wounds are typically treated as closed fractures, since the risk of osteomyelitis is very low. These are typically bullets from handguns that travel 600 meters per second). The timing and direction (e.g. antegrade or retrograde) of nail insertion has not shown to
affect outcomes.
Cannada et al. reviewed 74 cases of femoral diaphyseal fractures caused by gunshots. All were treated with reamed, retrograde, statically locked intramedullary nailing, without formal irrigation and debridement in the operating room. Outcomes showed low incidence of shortening, angular deformity and infection rate.
Dougherty et al. compared retrograde vs. antegrade intramedullary nailing for the treatment of gunshot diaphyseal femur fractures. No significant differences were found between groups with regards to operative time, blood loss, or radiographic union. They conclude that immediate retrograde or antegrade nailing is safe for the early treatment of gunshot femur fractures.
Figure A shows an AP radiograph of the right femur. There is a gunshot fracture in the proximal femoral shaft with retained bullet fragments. The leg has been placed in temporary traction.
Incorrect Answers:
Answer 1: External fixation would be considered for treatment of femur fractures in damage control orthopaedics.
Answer 2: IV antibiotics for 6 weeks would not be necessary with low velocity gunshot wounds with clean wounds.
Answer 4 and 5: The direction of nail entry does not seem to affect outcomes with these fractures. Irrigation and debridement of wound, as well as IV antibiotics, wound not be necessary, aforementioned.
Figure A shows a radiograph of a 19-year-old male with an isolated shotgun injury. On physical examination, he has a 3 cm wound over the posterolateral aspect of his arm. In addition, he has weakness with wrist and finger extension, but no sensory deficits. The patient has received tetanus prophylaxis and antibiotics in the emergency department. What would be the next best steps in treatment?
1) Urgent open reduction internal fixation and fibular osteoseptocutaneous flap
2) Irrigation and debridement and external fixation
3) Irrigation and debridement, repair of the radial nerve and retrograde intramedullary nail
4) CT scan, urgent open reduction internal fixation and IV antibiotics for 6 weeks
5) Closed reduction, CT scan, immobilization in a coaptation splint
This patient has sustained a shotgun blast to the midshaft humerus. The next best step would be irrigation and debridement, and external fixation of the fracture.
Shotgun injuries are typically treated as open fractures, whereas low-energy gunshot wounds are treated as closed fractures. The initial operative treatment of shotgun wounds should include irrigation and debridement and stabilization with external fixation. The goal of treatment is to stabilize the severe soft-tissue injury and bone loss, as well as to aggressively debride devitalized tissue and gross contamination.
Dougherty et al. reviewed gunshot fractures to the humerus. They report that
peripheral nerve injuries are relatively common with these injuries, with a more common incidence in distal injuries than proximal.
Joshi et al. looked at low velocity gunshot fractures to the humerus. They found that these injuries can be safely treated as closed fractures with local wound care, fracture brace and oral antibiotics. The time to union was similar in the non-operative and open treatment group.
Berick et al. examined the indications for nerve exploration with humerus gunshot fractures. They recommend continued observation of isolated nerve palsies associated with gunshot fractures of the humerus. However, consider early nerve exploration of palsies when associated with a concomitant vascular injury.
Figure A shows a high velocity shotgun fracture to the left humerus with retained buck fragments. Illustration A shows a similar injury stabilized with external fixation.
Incorrect Answers:
Answer 1: Due to the severity of soft tissue injury, external fixation should be considered for initial stabilization. Vascularized fibular grafts has been expanded to an osteoseptocutaneous flap by including a cutaneous flap on the lateral aspect of the lower leg. These are not typically used in the acute setting.
Answer 3: Retrograde intramedullary nail would not be the ideal implant for this injury, acutely.
Answer 4 and 5: There is no indication for a CT scan or prolonged antibiotics. The fracture and soft-tissue injury should be initially stabilized with external fixation. Coaptation splinting will interfere with soft tissue care.
A 34-year-old male sustains the closed injury seen in Figure A as a result of a high-speed motor vehicle collision. What is the most appropriate next step in treatment?
1) Open reduction and internal fixation
2) Spanning external fixation
3) Percutaneous internal fixation
4) Closed reduction and cast placement
5) Ankle arthrodesis
The radiograph shows a comminuted pilon fracture, which is associated with high-energy trauma and significant soft tissue injury. The tested concept here is the importance of avoiding definitive reduction and fixation of this high-energy injury, which has been shown to be associated with an increased risk of wound complications and deep infections (as compared to staged treatment with usage of a spanning external fixator).
Patterson et al. reviewed 23 consecutive patients with comminuted distal tibia fractures. They showed 0% infections or wound-healing problems in their patient population treated with a two-staged protocol. Their protocol involved fibula fixation with an intramedullary implant and application of a medial external fixator to to regain length and restore anatomic alignment. Reevaluation of the limb occurred ten to fourteen days later for definitive fixation.
Sirkin et al. retrospectively reviewed 40 closed and 17 open pilon fractures (AO types 43A-C) that were treated with staged surgical management (avg. time from ext. fix. to formal reconstruction was 14 days (range 4 to 31) They reported 17% post-operative wound complication in the closed group and 11% post-operative wound complication in the open group (Gustilo Type I-III). They suggest the technique was successful in both closed and open pilon fractures.
A 72-year-old woman falls down stairs and sustains the injury shown in Figure A. Additional radiographs are performed in Figure B to help assess the fracture pattern. These additional radiographs represent which of the following?
1) Oblique radiographs
2) In-situ radiographs under anesthesia
3) Traction radiographs
4) Fracture flexion radiographs
5) Fracture extension radiographs
Additional traction radiographs are performed in distal humerus fractures to better understand the fracture configuration.
Traction radiographs help align the fracture fragments for better visualization. This is useful in comminuted fractures where distal fragments are telescoped or flexed on the proximal fragments, making CT scan visualization difficult.
Proper visualization can help determine (1) the approach to the distal humerus, (2) whether to perform ORIF or total elbow arthroplasty (in select patients), (3) whether to add a 3rd plate (lateral column), (4) whether to add tricortical bone graft to augment distal fixation and restore trochlear width.
Doornberg et al. examined whether 3D CT improved fracture characterization. They found that 3D CT improved interobserver and intraobserver reliability for fracture characterization and classification. It also improved intraobserver accuracy for fracture characteristics, but not interobserver accuracy. They concluded that 3D CT is helpful for preoperative planning.
Galano et al. reviewed treatment strategies for bicolumnar distal humerus fractures. They state that 3D CT compensates for oblique scans from formatting in an incorrect plane, and allows for subtraction of the radius/ulna to properly demonstrate articular incongruity, degree of comminution and column involvement.
Figures A and B show a distal humerus fracture without traction (A) and with traction (B) applied. Illustration A shows the same fracture after bicolumnar plating. Illustration B shows the different surgical approaches to the distal humerus (A, Campbell triceps splitting; B, O'Driscoll triceps reflecting anconeus pedicle [TRAP]; C, Bryan-Morrey triceps reflecting; D, olecranon osteotomy)
Incorrect Answers:
Answer 1: These radiographs aren't oblique images.
Answer 2: Radiographs under anesthesia do not add further information unless traction is applied.
Answers 4 and 5: Flexion and extension will further impact and displaced fragments and will not improve alignment.
Mirror therapy is indicated for which of the following clinical conditions?
1) Impaired proprioception after lower extremity injury
2) Two-stage flexor tendon reconstruction
3) Plumbism
4) Anterior cruciate ligament reconstruction
5) Phantom pain
Mirror therapy is a useful technique to improve phantom pain in amputees. Phantom limb pain is a painful sensation that is perceived within a body part that no longer exists.
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Answer 1: Mirror therapy is not indicated for proprioception training. Answer 2: Mirror therapy is not indicated for flexor tendon injuries. Answer 3: Mirror therapy is not indicated for lead poisoning.
Answer 4: Mirror therapy is not indicated for ACL reconstruction.
A patient presents to the emergency department with the injury seen in Figure A. Which of the following is true about radial nerve palsies associated with isolated humeral shaft fractures after low velocity gunshot wounds?
1) The initial treatment involves debridement, irrigation, nerve exploration, and osteosynthesis.
2) The radial nerve palsy is often a result of neurotmesis.
3) Initial treatment involves splinting and observation for return of neurologic function.
4) Electrophysiologic testing for radial nerve palsies is indicated after 2-3 weeks without improvement.
5) The radial nerve palsy will not resolve regardless of attempted interventions.
When a patient sustains an isolated humeral shaft fracture and radial nerve palsy from a GSW, the initial treatment involves splinting with observation.
The majority of humeral shaft fractures are treated initially with a coaptation splint and then transitioned to a functional brace. Absolute surgical indications for operative management include: open fracture, brachial plexus injury, compartment syndrome, floating elbow, or vascular injury. A radial nerve palsy is not an indication for surgical management of an isolated humeral shaft fracture. Radial nerve injury from a low-velocity GSW is similar to that of blunt force trauma and thus, immediate exploration is not necessary. Instead, nerve function should be observed. Seventy percent of these nerve injuries will resolve spontaneously. Additionally, the patient should receive a short course of antibiotics as any low velocity GSW would be treated.
Guo et al retrospectively reviewed the electrophysiologic data for 40 radial nerve palsies caused by GSWs and blunt trauma. After characterizing the palsies by level of injury, completeness of nerve injury, and other associated nerves injured, they found there to be no difference in any of these variables between GSW induced radial nerve palsies and blunt trauma induced palsies.
Vaidya et al retrospectively reviewed the outcomes of 54 patients with humeral shaft fractures resulting from low velocity GSWs comparing operative and nonoperative treatments. They found that patients receiving non-operative management did well and that 70% of radial nerve palsies in the non-operative treatment group resolved on their own. They recommended non-operative treatment for the majority of isolated humeral shaft fractures resulting from civilian gunshot wounds.
Figure A is a radiograph of a humeral shaft fracture after a GSW. Illustration A is a radiograph of a humeral shaft fracture with a coaptation in place.
Illustration B is an example of a functional brace.
Incorrect answers:
Answer 1: This is the initial treatment for an open humeral shaft fracture associated with an radial nerve palsy.
Answer 2: Radial nerve palsy from a low velocity GSW is usually axonotmesis. Neurotmesis the most common injury in open fractures.
Answer 4:EMG testing is not indicated until 3-4 months of radial nerve palsy with no neural recovery.
Answer 5: Seventy percent of radial nerve palsies will spontaneously resolve
A 76-year-old male community ambulatory presented to clinic complaining of pain in the left groin that has been persistent for the last 8 months. Radiographs obtained from clinic are seen in Figure A. You suspect a femoral neck nonunion and obtain a CT scan which confirmed it. Which of the following statements is true?
1) Total hip arthroplasty will provide patient with the best long term outcomes
2) Valgus malreduction is closely correlated with failure of fixation after reduction and cannulated screw fixation
3) The patient's best outcome would be with an open reduction, bone grafting, and changing to an inverted triangle configuration of screws
4) The most appropriate treatment is a valgus osteotomy to correct malreduction
5) Providing this patient with a hemiarthroplasty increases rates of postoperative dislocation when comparing to total hip arthroplasty
A total hip arthroplasty (THA) after nonunion of a femoral neck fracture would provide the best long term outcomes in a 76-year-old male who is a community ambulator.
After nonunion of a femoral neck fracture, hemiarthroplasty and THA are good salvage option for the physiologically older patients. When deciding between these two options, THA is better for active and cognitively intact patients. THA is also indicated in patients with radiographic evidence of degenerative disease about the acetabulum. Hemiarthroplasty is advocated for patients who are older and less active.
Yang et al. retrospectively investigated the risk factors for nonunion in patients treated with cannulated screws. They reviewed 202 patients who had femoral neck fractures and were treated with internal fixation with cannulated screws. They identified that triangle configuration, displaced fracture, borderline or unacceptable reduction, and increased screw shaft subchondral purchase over the femoral neck were all risk factors for nonunion after internal fixation.
Inverted triangle configuration was found to increase rate of union.
Archibeck et al. retrospectively reviewed the outcomes of 102 THAs after failed internal fixation for a hip fracture (including both femoral neck and intertrochanteric). They concluded that the conversion of failed hip internal fixation has elevated risks compared to a primary THA, however, it may still be successful. The biggest concern for these patients postoperatively are periprosthetic fracture and dislocation.
Figures and Illustrations:
Figure A is an AP pelvic radiograph demonstrating a nonunion of a femoral neck fracture after suboptimal fixation with 3 cannulated screws in a triangle configuration.
Illustration A is an AP radiograph of the left hip in this patient following conversion to THA.
Illustration B is a radiograph demonstrating a valgus osteotomy. Illustration C shows an example of a femoral neck nonunion with varus malreduction.
Incorrect Answers:
Answer 2: Varus reduction is closely correlated with failure in this fixation method.
Answer 3: The patient's best outcome would be with THA.
Answer 4: This would be a good option in a younger patient, but given age and functional capacity, the best option is THA.
Answer 5: Patients with hemiarthroplasty have lower rates of dislocation.
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?
1) Non-operative managment, but arrange for early follow-up in clinic
2) Intra-compartmental pressure measurements
3) Ankle-brachial index measurements
4) Knee spanning external fixation
5) Open reduction internal fixation
This patient presents with a Schatzker IV tibia plateau fracture with lower extremity neurologic deficits. The next best step would be to investigate for an acute vascular injury with ankle-brachial index measurements.
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
1) Splint until swelling subsides, then long-arm cast
2) Excision of fracture fragments
3) Closed reduction and percutaneous pinning
4) Open reduction and internal fixation (ORIF)
5) Radial head replacement
This patient has Mason II radial head fracture. ORIF will give the best results.
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF
group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
Answer 1: Nonoperative management is indicated for non-/minimally displaced fractures.
Answer 2: Excision is an option for small partial articular fragments = 3 fragments.
When placing an intramedullary nail for closed distal tibia shaft fractures, all of the following methods are described techniques to aid anatomic reduction EXCEPT:
1) Plating of a concomitant fibula fracture
2) Percutaneous placement of reduction foreceps at the fracture site
3) Placing a Poller screw
4) Placing a small-fragment plate at the fracture site
5) Placing syndesmotic fixation
Of the choices above, syndesmotic fixation would not help anatomically reduce these fractures.
Fractures of the distal tibia are challenging fractures to achieve an anatomic reduction. The medullary canals at either end of the tibia are capacious compared to the mid-diaphysis thus inhibiting an endosteal fit. These fractures have a tendency to become mal-aligned unless certain steps are taken to ensure restoration of the length, alignment, and rotation. Using a Poller or blocking screw can function to narrow the space available for the nail to guide the nail or correct deformity. The use of large pointed-reduction forceps or a small frag plate may also be used for provisional fixation. Additionally, plating concomitant fibula fractures may help indirectly restore length and reduce the tibia fracture. Concomitant syndesmotic injuries are not commonly seen and fixation for these is not required unless stress exam clearly demonstrates it.
Casstevens et al. reviewed the surgical management of distal tibia fractures using either plates/screws or intramedullary nails. Current literature shows near equivalence of either technique regarding union and alignment. They recommend treating each fracture on a case-by-case basis with consideration of the soft tissues and fracture pattern when determining fixation choices.
Tejwani et al. reviewed surgical techniques for managing metaphyseal and meta-diaphysial tibia fractures. Advances in tibial nail design have helped tremendously in negotiating these fractures. Though current supporting literature is based mostly on case series, the use of suprapatellar entry intramedullary nails may help avoid the common deformity of procurvatum and valgus seen with proximal tibia fractures.
Egol et al. retrospectively reviewed distal tibial shaft fracture undergoing intramedullary nailing, with and without concomitant fibula fracture plate fixation. They found fractures with fibular fixation maintained better alignment beyond 12 week post-operatively than those without fixation. Given these findings they recommended fibular plating for all distal tibial shaft fractures.
Illustration A shows a fibula fracture that was plated prior to tibia IMN placement. Illustrations B and C show the use of pointed reduction forceps placed percutaneously to reduce the fracture. Illustration D shows the use of a blocking screw (denoted by the arrow) to keep the nail lateralized and the fracture out of valgus. Illustration E shows the use of a plate to reduce the fracture prior to nail placement.
Incorrect Answers:
Answers 1, 2, 3, and 4: All of these have been described in the literature to help aid in reducing these fractures
A 70-year-old woman falls down a flight of stairs and sustains the injury shown in Figures A and B to her dominant upper extremity. She lives alone and has no other medical history. Which of the following surgical options is best to minimize complications for this fracture pattern?
1) Open reduction and internal fixation with a long locking plate
2) Uncemented reverse total shoulder arthroplasty with tuberosity repair
3) Cemented reverse total shoulder arthroplasty without tuberosity repair
4) Cemented reverse total shoulder arthroplasty with tuberosity repair
5) Proximal humeral resection with endoprosthetic replacement
This patient has a complex proximal humerus fracture with metaphyseal comminution and poor bone stock. Cemented reverse total shoulder arthroplasty (rTSA) using a long stem prosthesis and tuberosity repair is indicated.
Proximal humerus fragility fractures are hard to treat because of comminution and poor bone stock. AVN is common with glenohumeral fracture-dislocation. Hemiarthroplasty (and standard total shoulder arthroplasty, TSA) is unreliable because of dependence on tuberosity healing. rTSA is recommended for fractures in patients >70 years with severely comminuted fractures, high likelihood of head AVN, and poor tuberosity bone quality (osteoporosis or comminution).
Bufquin et al. retrospectively reviewed the use of rTSA for treatment of 43 patients with 3- and 4-part proximal humerus fractures. They found satisfactory elevation (97°), ER in abduction (30°), constant scores (44) and modified Constant scores (66%). Complications included calcification (90%), tuberosity displacement (53%) and scapular notching (25%). They concluded that rTSA was a good procedure because it provides pain relief and easier functional recovery in spite of failed tuberosity healing.
Anakwenze et al. systematically reviewed acute proximal humerus fractures. Frequency weighted range of motion was flexion 122°, abduction 97°, ER at neutral 18°. Tuberosity repair yielded higher ER compared to no repair.
Scapular notching was the most common complication (32%). They concluded that rTSA patients tended to be elderly women with 4-part fractures, had good pain control but residual dysfunction.
Jobin et al. reviewed rTSA for management of proximal humerus 3- and 4-part fractures. They note >50% of cases have tuberosity resorption. They recommend repairing the greater tuberosity to restore infraspinatus/teres minor function which improves external rotation strength. Greater tuberosity malunion is not a result of secondary displacement, but rather, from intraoperative malreduction. Lesser tuberosity repair should be performed if there is significant bone loss or intraoperative anterior instability.
Figures A and B are AP radiograph and 3D reformatted CT scan showing comminuted proximal humerus fracture dislocation. Illustration A shows rTSA performed with distal cementation of a long stem prosthesis and cerclage fixation of the proximal shaft and the tuberosity fragments.
Incorrect Answers:
Answer 1: ORIF has potential complications of screw cut out, AVN, fracture collapse, tuberosity resorption and loss of fixation. The risk of AVN (and resultant screw cut out) is high because of comminuted fracture-dislocation. Answer 2: Cementing is indicated because metaphyseal fracture bone loss compromises stem fixation.
Answer 3: Greater tuberosity repair improves external rotation strength. Lesser tuberosity repair adds to anterior stability.
Answer 5: Proximal humeral replacement is only necessary for tumor or unreconstructable fractures. They have poorer outcomes because of loss of rotator cuff function.
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-
operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
1) Observation and close follow-up
2) Dynamization of the intramedullary nail
3) Revision surgery, internally rotate distal fragment by 19 degrees
4) Revision surgery, externally rotate distal fragment by 8 degrees
5) Revision surgery, internally rotate proximal fragment by 11 degrees
The CT scanogram shows the operative left femur is 8 degrees externally rotated compared to the native right femur. No correction is required unless malalignment is >15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles.
This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH - PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs.
Therefore 15 degrees and symptomatic.
Which of the following images shows an injury pattern most consistent with a lateral compression type 3 pelvic ring injury?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure C is an axial CT scan of a lateral compression type 3 (LC3) pelvic ring injury.
Classically, LC3 injuries demonstrate an ipsilateral lateral compression and a contralateral APC (windswept pelvis) fracture pattern. The most common mechanism of injury in these cases is a rollover MVC or pedestrian vs. auto. LC1 injuries are characterized by an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture, while LC2 injuries consist of a rami fracture and ipsilateral posterior ilium fracture dislocation (crescent fracture). While LC1 injuries can often initially be managed conservatively with protected weight-bearing and close observation, LC2 and LC3 pelvic ring injuries are almost universally operative.
Pennal et al. discuss a radiologic technique for assessing the forces producing pelvic disruption and its use in logically classifying pelvic injury. Based on this radiologic assessment and along with some biomechanical studies, they propose a classification system involving three major forces producing injury that can also be helpful in the management of these patients.
Young et al. performed a retrospective analysis of the plain radiographs of 142 cases of pelvic fractures and identified four patterns of force that presented with distinctive, recognizable radiographic appearances. They describe a classification system for pelvic fractures based on radiographic and clinical findings that correlates with associated injury to soft-tissue structures and enables the surgeon to begin corrective procedures rapidly.
Incorrect Answers:
Answer 1: This represents a lateral compression type 2 injury. Answer 2: This represents a lateral compression type 1 injury.
Answer 4: This represents an anterior posterior compression type 2 injury. Answer 5: This represents an anterior posterior compression type 3 injury.
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?
1) Length of hospital stay
2) Association with neurological deficit(s)
3) Length of intensive care stay
4) Cardiac collapse
5) Mortality
Unstable pelvic fractures can be devastating injuries often resulting in significant morbidity and even death.
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (24 hours).
Incorrect Answers: Choices 1-4 do not correlate with increased blood transfusions to the extent of Option 5.
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
1) Reduced radial artery pulse
2) Double break in the ipsilateral superior shoulder suspensory complex
3) Elevated hemidiaphragm
4) Musculocutaneous nerve deficit
5) Drooping of the left eyelid
Drooping of the left eyelid is a presenting feature of Horner's syndrome. Horner's syndrome represents a disruption of the sympathetic chain via C8 and/or T1 root avulsion after trauma.
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity = 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Answer 1, 2: The superior shoulder suspensory complex (SSSC) is located in close proximity to the brachial plexus. Disruption of the SSSC may affect the local anatomy and cause local brachial plexus or vascular injury.
Answer 3: Elevated hemidiaphragm (Phrenic nerve C3,4,5) may be suggestive an upper brachial plexus root avulsion, e.g. C5, C6 injury.
Answer 4: Musculocutaneous nerve deficiency (C5 deficiency) results in weakness to the biceps.
A 46-year-old competitive cyclist falls while racing and suffers an isolated fracture as seen in Figure A. He is positioned on a fracture table and a closed reduction maneuver is attempted, unsuccessfully.
Which of the following treatment plans is most appropriate?
1) Obtain a CT scan intraoperatively to reassess the quality of reduction
2) Perform additional closed reduction maneuvers until the reduction is adequate for percutaneous fixation
3) As long as the stepoff is less than 7mm in any plane of imaging, it is appropriate to proceed with percutaneous fixation
4) Perform an open reduction and internal fixation using a sliding hip screw
5) Perform an acute total hip arthroplasty through a direct anterior approach since the patient is on the fracture table
When standard closed reduction maneuvers using a traction table are unsuccessful, displaced femoral neck fracture in young adults (10 degrees varus/valgus or anteversion/retroversion) or has
significant displacement (5 mm or more in ANY view) is unacceptable, and an open reduction should be performed. Of course, this can be very difficult to assess in the operating room, where uncalibrated fluoroscopy with difficult to obtain tangential imaging is heavily relied upon to make this assessment.
Accordingly, when the quality of closed reduction is questionable, the best treatment plan is to obtain a better reduction with direct visualization of the femoral neck prior to fixation.
A systematic review of the literature by Pauyo, et al. cites numerous studies showing a higher incidence of osteonecrosis of the femoral head in patients with displaced femoral neck fractures treated with unsatisfactory reductions. Furthermore, performing multiple closed reduction attempts is also associated with a higher risk of osteonecrosis.
Upadhyay et al. performed a randomized controlled trial of 102 patients with femoral neck fractures treated with closed or open reductions, which were randomized. The groups had similar rates of nonunions and osteonecrosis of the femoral head; however, subanalysis revealed a "poor" reduction was the highest predictor of poor outcome, whether the reduction was attempted open or closed. Interestingly, the quality of reduction was more important than the implant used or the timing of surgery (including surgeries performed > 48h after injury).
Figure A shows a pre-operative AP x-ray of the patient's high-energy femoral neck fracture. Illustrations A and B are intraoperative fluoroscopic and postoperative CT scans of this same patient, highlighting that fluoroscopy may "hide" the degree of residual displacement.
Incorrect Answers:
Question 46High Yield
If a metacarpal shaft fracture shortens 4 mm, what will the theoretical amount of extensor lag be at the metacarpophalangeal joint:
Explanation
For each 2 mm of shortening, a 7° extensor lag exists. Thus, with 4 mm of shortening, there will be a 14° extensor lag at the metacarpophalangeal joint.
Question 47High Yield
A closed reduction of a volar thumb metacarpophalangeal (MP) joint dislocation is less likely to be successful with
Explanation
A volar thumb MP joint dislocation is an uncommon injury, occurring much less often than dorsal dislocation. Thumb volar MP dislocations often necessitate an open reduction because of interposed tissue including the EPL, extensor pollicis brevis (EPB), dorsal capsule, or volar plate. Several presurgical factors are associated with failure of a closed reduction. A closed reduction is less likely to be successful with no palpable EPL, displacement of the EPL or EPB, interposed sesamoids on radiographs, and paradoxical MP joint flexion and interphalangeal joint extension on attempting MP extension. The dorsal capsule is often noted to be disrupted following the injury, but this does not necessarily lead to an irreducible joint. The APL tendon inserts on the base of the thumb metacarpal and is not involved in the pathoanatomy of an irreducible MP dislocation. A collateral ligament injury is often associated with a volar thumb MP dislocation regardless of the ability to perform a closed reduction.
RECOMMENDED READINGS
24. Beck JD, Klena JC. Closed reduction and treatment of 2 volar thumb metacarpophalangeal dislocations: report of 2 cases. J Hand Surg Am. 2011 Apr;36(4):665-9. doi: 10.1016/j.jhsa.2010.12.006. Epub 2011 Feb 25. PubMed PMID: 21353397.
25. Hirata H, Takegami K, Nagakura T, Tsujii M, Uchida A. Irreducible volar subluxation of the metacarpophalangeal joint of the thumb. J Hand Surg Am. 2004 Sep;29(5):921-4. PubMed PMID: 15465245.
RECOMMENDED READINGS
24. Beck JD, Klena JC. Closed reduction and treatment of 2 volar thumb metacarpophalangeal dislocations: report of 2 cases. J Hand Surg Am. 2011 Apr;36(4):665-9. doi: 10.1016/j.jhsa.2010.12.006. Epub 2011 Feb 25. PubMed PMID: 21353397.
25. Hirata H, Takegami K, Nagakura T, Tsujii M, Uchida A. Irreducible volar subluxation of the metacarpophalangeal joint of the thumb. J Hand Surg Am. 2004 Sep;29(5):921-4. PubMed PMID: 15465245.
Question 48High Yield
Figures 1 and 2 are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?

Explanation
■
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
Question 49High Yield
While experts disagree whether the postpolio syndrome is caused by a reactivation of the dormant virus or by an attritional aging phenomena of muscles that have been overworked over a period of time, both groups recommend which of the following guidelines for optimizing function in this population?
Explanation
Most leaders in orthopaedic surgery support Jacqueline Perry’s theory that the postpolio syndrome is an attritional degenerative process that is the result of overuse of muscles and joints that are unable to adequately tolerate overload, and have little functional reserve. For that reason, aerobic conditioning and exercise are important. Overload and exhaustion of involved muscles should be avoided.
REFERENCE: Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
REFERENCE: Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Question 50High Yield
A 7 5-year-old man who sustained an intertrochanteric hip fracture underwent open reduction and internal fixation with a sliding hip screw. Six months after the procedure, the patient has shortening and external rotation of the extremity and progressively severe groin pain with ambulation. Radiographs are shown in Figures 5a and 5b. What is the most appropriate management?

Explanation
DISCUSSION: The patient has an intertrochanteric fracture malunion with protrusion of the hardware and penetration into the acetabulum. To restore leg length and relieve pain, total hip arthroplasty is necessary. Valgus osteotomy is appropriate for fracture nonunion with an intact femoral head with no signs of osteonecrosis. Bipolar hemiarthroplasty with acetabular erosion will most likely lead to pain as will removal of the hardware with or without physical therapy.
REFERENCE: Said GZ, Farouk O, El-Sayed A, et al: Salvage of failed dynamic hip screw fixation of intertrochanteric fractures. Injury 2006;37:194-202.
Figure 6
DISCUSSION: The patient has an intertrochanteric fracture malunion with protrusion of the hardware and penetration into the acetabulum. To restore leg length and relieve pain, total hip arthroplasty is necessary. Valgus osteotomy is appropriate for fracture nonunion with an intact femoral head with no signs of osteonecrosis. Bipolar hemiarthroplasty with acetabular erosion will most likely lead to pain as will removal of the hardware with or without physical therapy.
REFERENCE: Said GZ, Farouk O, El-Sayed A, et al: Salvage of failed dynamic hip screw fixation of intertrochanteric fractures. Injury 2006;37:194-202.
Figure 6
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon