Free Orthopedics Review | Dr Hutaif General Orthopedics -...
14 Apr 2026
49 min read
88 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Free Orthopedics Review | Dr Hutaif General O...
00:00
Start Quiz
Question 1High Yield
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage
debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is

Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 2High Yield
At the time of arthroscopy, the posterior humeral head Hill-Sachs lesion substantially engages with the glenoid; CT and arthroscopic findings reveal minimal glenoid bone loss. In addition to arthroscopic Bankart repair, arthroscopic Hill-Sachs remplissage with suture anchors is performed. In combined Bankart repair with Hill-Sachs remplissage vs Bankart repair alone, which complication is of highest potential concern?
Explanation
- Loss of shoulder external rotation of approximately 10 degrees vs the uninjured shoulder_
Question 3High Yield
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The genetic pattern seen in patients with this type of presentation is:
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The genetic pattern seen in patients with this type of presentation is:
Explanation
Multiple hereditary exostoses is inherited in an autosomal-dominant manner with 90% penetrance.
Question 4High Yield
A functional nerve transfer involves
Explanation
Nerve transfer can provide some function to a functionless nerve. Typically, nerve transfer includes intrafascicular dissection; cutting of a functioning nerve fascicle; and suturing the
released, functioning nerve fascicle to a nonfunctioning nerve branch. A common application of nerve transfer in the upper extremity involves attachment of a functioning motor fascicle of the ulnar nerve to the nonfunctioning musculocutaneous branch to the biceps muscle to restore active elbow flexion in patients with nerve root avulsion brachial plexus injuries. Motor nerves can be transferred to other motor nerves, and sensory nerves can be transferred to other sensory nerves. Treatment of acute nerve gaps with nerve grafting, conduits, or nerve growth factors does not describe nerve transfer. Although implanting neuromas into neighboring muscle tissue can decrease symptoms related to the neuroma, this does not describe a nerve transfer, and a neuroma cannot reinnervate a muscle.
RECOMMENDED READINGS
10. Tung TH, Mackinnon SE. Nerve transfers: indications, techniques, and outcomes. J Hand Surg Am. 2010 Feb;35(2):332-41. doi: 10.1016/j.jhsa.2009.12.002. Review. PubMed PMID: 20141906.
11. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
released, functioning nerve fascicle to a nonfunctioning nerve branch. A common application of nerve transfer in the upper extremity involves attachment of a functioning motor fascicle of the ulnar nerve to the nonfunctioning musculocutaneous branch to the biceps muscle to restore active elbow flexion in patients with nerve root avulsion brachial plexus injuries. Motor nerves can be transferred to other motor nerves, and sensory nerves can be transferred to other sensory nerves. Treatment of acute nerve gaps with nerve grafting, conduits, or nerve growth factors does not describe nerve transfer. Although implanting neuromas into neighboring muscle tissue can decrease symptoms related to the neuroma, this does not describe a nerve transfer, and a neuroma cannot reinnervate a muscle.
RECOMMENDED READINGS
10. Tung TH, Mackinnon SE. Nerve transfers: indications, techniques, and outcomes. J Hand Surg Am. 2010 Feb;35(2):332-41. doi: 10.1016/j.jhsa.2009.12.002. Review. PubMed PMID: 20141906.
11. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
Question 5High Yield
Dupuytrenâs cord tissue is characterized by what change from normal:
Explanation
C ompared to normal palmar fascia, the fibrous bands in Dupuytrenâs disease have an increased ratio of type III to type I
collagen, and an overall increase in the amount of type III collagen.
collagen, and an overall increase in the amount of type III collagen.
Question 6High Yield
Figures 1 through 4 are the MRI scans and radiograph of a 48-year-old woman who has chronic neck pain and severe lower back pain. The pain is constant and seems to worsen at night. Other subjective complaints include: sleep disturbance, difficulty maintaining concentration, chronic fatigue, migraine headaches, morning stiffness, forgetfulness, and difficulty with balance. She also describes frequent episodes of bilateral lower extremity burning-like pain. On examination, she has normal motor and sensory function in upper and lower extremities. She does, however, have multiple sites of palpable tenderness scattered throughout her body. She has tried massage therapy and chiropractic management in the past with marginal results.
Imaging is provided. What is the most appropriate treatment?
Imaging is provided. What is the most appropriate treatment?

Explanation
■
The patient has a diagnosis of fibromyalgia, which the American College of Rheumatology defines as chronic widespread pain with at least 11 of 18 possible tender points. Etiology is multifactorial, but there is a genetic predisposition. Some associated factors include: history of widespread pain and hyperalgesia, sleep disorder, inactivity, functional disability, concomitant anxiety or mood disorder, and fear avoidance behavior. The most effective treatment for fibromyalgia is multimodal; however, pharmacologic neuromodulation (use of antiepileptic drugs, tricyclic antidepressants, selective serotonin-reuptake inhibitors, and serotonin norepinephrine reuptake inhibitors) has been found to be moderately successful in treating widespread pain and hyperalgesia. These medications are aimed at altering the neurochemistry of the central nervous system and diminishing the perception of pain. Other treatments include physical activity to address inactivity and functional disability, sleep quality improvement, interventions treating anxiety and mood disorders, and interventions targeting fear-avoidance behavior. Surgery, specifically fusion procedures, has not been found to be effective in such patients with discogenic changes only; without instability or stenosis. There is no high-level study showing efficacy of either lumbar or cervical epidural injection in patients with fibromyalgia who complain of neck or back pain without radiculopathy. The use of opiates and anxiolytics should be closely monitored because this patient population is especially at high risk for abuse and dependence.
The patient has a diagnosis of fibromyalgia, which the American College of Rheumatology defines as chronic widespread pain with at least 11 of 18 possible tender points. Etiology is multifactorial, but there is a genetic predisposition. Some associated factors include: history of widespread pain and hyperalgesia, sleep disorder, inactivity, functional disability, concomitant anxiety or mood disorder, and fear avoidance behavior. The most effective treatment for fibromyalgia is multimodal; however, pharmacologic neuromodulation (use of antiepileptic drugs, tricyclic antidepressants, selective serotonin-reuptake inhibitors, and serotonin norepinephrine reuptake inhibitors) has been found to be moderately successful in treating widespread pain and hyperalgesia. These medications are aimed at altering the neurochemistry of the central nervous system and diminishing the perception of pain. Other treatments include physical activity to address inactivity and functional disability, sleep quality improvement, interventions treating anxiety and mood disorders, and interventions targeting fear-avoidance behavior. Surgery, specifically fusion procedures, has not been found to be effective in such patients with discogenic changes only; without instability or stenosis. There is no high-level study showing efficacy of either lumbar or cervical epidural injection in patients with fibromyalgia who complain of neck or back pain without radiculopathy. The use of opiates and anxiolytics should be closely monitored because this patient population is especially at high risk for abuse and dependence.
Question 7High Yield
Schwannomas are differentiated from neurofibromas by all of the following except:
Explanation
Schwann cells contribute to schwannoma and neurofibroma.
Question 8High Yield
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?

Explanation
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.
Figure 56
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.
Figure 56
Question 9High Yield
A 16-year-old swimmer has right shoulder pain with activity. She describes the continued sensation that her shoulder is "loose." She has been in physical therapy for 7 months to work on strengthening the muscles around her shoulder and scapula. She denies being able to voluntarily dislocate her shoulder. Upon examination, you can feel the humeral head slide over the glenoid rim both anteriorly and posteriorly with the load and shift test. She has a grade III sulcus sign. What is the most appropriate next step?
Explanation
Nonsurgical treatment with activity modification and physical therapy is generally considered the first-line approach for young athletes with multidirectional instability (MDI) of the shoulder. Physical therapy focuses on exercises to strengthen the scapular stabilizers and rotator cuff muscles and restore scapulohumeral rhythm. Although a definitive length of time to assess physical therapy failure is not known, many surgeons believe that a patient with MDI should undergo at least 6 months of physical therapy and activity
36
modification before considering surgery. Although an open inferior capsular shift has historically been considered the gold standard for surgical treatment for MDI, studies have shown good success rates for arthroscopic capsulorrhaphy. Arthroscopy can allow a surgeon to assess all intra-articular structures and address a patient’s particular problem based on arthroscopic findings.
36
modification before considering surgery. Although an open inferior capsular shift has historically been considered the gold standard for surgical treatment for MDI, studies have shown good success rates for arthroscopic capsulorrhaphy. Arthroscopy can allow a surgeon to assess all intra-articular structures and address a patient’s particular problem based on arthroscopic findings.
Question 10High Yield
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as “gamekeeper’s thumb.” The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness.
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 11High Yield
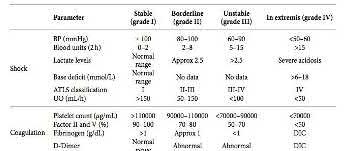
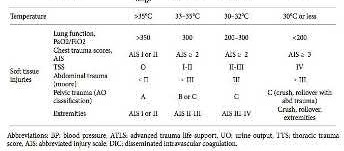
A previously healthy 22-year-old male presents to the hospital after a motor vehicle accident. His injuries include a closed head injury, flail chest, intra-abdominal bleed and right femoral shaft fracture. Which of the following conventional indicators would support the role for "damage control orthopaedics" as opposed to "early total care" in the clinical decision making process of his femur fracture management?
Explanation
Previously healthy, poly-trauma patients, presenting with platelet counts of
<70,000 will fall into the pathophysiological category of 'in extremis'. This will
support the role of damage control orthopaedics in the decision making process of this patients fracture management.
Damage control orthopaedics (DCO) is a staged approach for the management of polytrauma patients. It is most ideal for trauma patients that are clinically unstable or in extremis. In these patients, immediate surgery is thought to cause a “second hit” phenomenon, which may lead to ARDS, multi-organ failure, or even death. A patient is classified as 'unstable' or 'in extremis', if he or she meets the criteria in at least three of the four pathophysiological parameters; blood pressure <90mmHg, platelets count <70,000, temperature
<32°C and major soft tissue injuries.
Pape et al. (2005) described four classes of patients, based on their clinical status: stable, borderline, unstable, and in extremes. The term “borderline” was coined to describe a patient who is categorized as stable before surgery, but is at significant risk of unexpected deterioration and organ dysfunction postoperatively.
Pape et al. (2009) outlined that stable patient can undergo early definitive fracture fixation as necessary. In contrast, unstable patient should be resuscitated and adequately stabilized with temporary fixation before receiving definitive orthopaedic care.
Illustration A shows a table outlining the classification system used by Pape to classify patients into their clinical status of stable, borderline, unstable, and in extremes.
Incorrect Answers:
Answer 1: Lactate level = 1.9 mmol/L (normal range <2.5 mmol/L) would classify this patient into a stable category.
Answer 2: Fibrinogen = 1.1 g/dL (normal range >1 g/dL) would classify this patient into a stable category.
Answer 4: Urine output = 50 cc/hr (normal range >150 cc/hr)would classify this patient into a borderline category.
Answer 5: Base deficit = 2 mmol/L (normal range -2 to +2 mmol/L) would classify this patient into a stable category.
<70,000 will fall into the pathophysiological category of 'in extremis'. This will
support the role of damage control orthopaedics in the decision making process of this patients fracture management.
Damage control orthopaedics (DCO) is a staged approach for the management of polytrauma patients. It is most ideal for trauma patients that are clinically unstable or in extremis. In these patients, immediate surgery is thought to cause a “second hit” phenomenon, which may lead to ARDS, multi-organ failure, or even death. A patient is classified as 'unstable' or 'in extremis', if he or she meets the criteria in at least three of the four pathophysiological parameters; blood pressure <90mmHg, platelets count <70,000, temperature
<32°C and major soft tissue injuries.
Pape et al. (2005) described four classes of patients, based on their clinical status: stable, borderline, unstable, and in extremes. The term “borderline” was coined to describe a patient who is categorized as stable before surgery, but is at significant risk of unexpected deterioration and organ dysfunction postoperatively.
Pape et al. (2009) outlined that stable patient can undergo early definitive fracture fixation as necessary. In contrast, unstable patient should be resuscitated and adequately stabilized with temporary fixation before receiving definitive orthopaedic care.
Illustration A shows a table outlining the classification system used by Pape to classify patients into their clinical status of stable, borderline, unstable, and in extremes.
Incorrect Answers:
Answer 1: Lactate level = 1.9 mmol/L (normal range <2.5 mmol/L) would classify this patient into a stable category.
Answer 2: Fibrinogen = 1.1 g/dL (normal range >1 g/dL) would classify this patient into a stable category.
Answer 4: Urine output = 50 cc/hr (normal range >150 cc/hr)would classify this patient into a borderline category.
Answer 5: Base deficit = 2 mmol/L (normal range -2 to +2 mmol/L) would classify this patient into a stable category.
Question 12High Yield
Which key factor that induces osteoclastogenesis is secreted by osteoblasts in response to inflammatory stimuli?
Explanation
**
Osteoclasts are derived from cells of the monocyte/macrophage lineage. They are multinucleated and develop by fusion of mononuclear precursors, a process that requires receptor activator for nuclear factor kappa-B ligand (RANKL) and macrophage-colony stimulating factor (M-CSF). RANKL is secreted by osteoblasts in response to inflammatory signals and is a key component of inflammation-mediated osteolysis. OPG binds to and sequesters RANKL, thus inhibiting osteoclast differentiation and activity.
BMP and IGF-1 are potent regulators of osteoblast differentiation and activation. TNF is a cytokine secreted by macrophages and degranulating platelets infiltrated in the fracture site and impacts a variety of cells, not osteoclasts.
Osteoclasts are derived from cells of the monocyte/macrophage lineage. They are multinucleated and develop by fusion of mononuclear precursors, a process that requires receptor activator for nuclear factor kappa-B ligand (RANKL) and macrophage-colony stimulating factor (M-CSF). RANKL is secreted by osteoblasts in response to inflammatory signals and is a key component of inflammation-mediated osteolysis. OPG binds to and sequesters RANKL, thus inhibiting osteoclast differentiation and activity.
BMP and IGF-1 are potent regulators of osteoblast differentiation and activation. TNF is a cytokine secreted by macrophages and degranulating platelets infiltrated in the fracture site and impacts a variety of cells, not osteoclasts.
Question 13High Yield
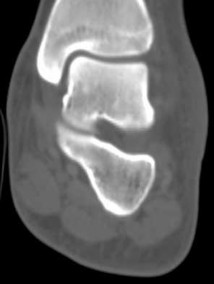
Figures 42a through 42c are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?



Explanation
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is
performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
RECOMMENDED READINGS
33. Moon ES, Dy CJ, Derman P, Vance MC, Carlson MG. Management of nonunion following surgical management of scaphoid fractures: current concepts. J Am Acad Orthop Surg. 2013 Sep;21(9):548-57. doi: 10.5435/JAAOS-21-09-548. Review. PubMed PMID: 23996986. View Abstract at PubMed
34. Kawamura K, Chung KC. Treatment of scaphoid fractures and nonunions. J Hand Surg Am. 2008 Jul-Aug;33(6):988-97. doi: 10.1016/j.jhsa.2008.04.026. Review. PubMed PMID: 18656779.
performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
RECOMMENDED READINGS
33. Moon ES, Dy CJ, Derman P, Vance MC, Carlson MG. Management of nonunion following surgical management of scaphoid fractures: current concepts. J Am Acad Orthop Surg. 2013 Sep;21(9):548-57. doi: 10.5435/JAAOS-21-09-548. Review. PubMed PMID: 23996986. View Abstract at PubMed
34. Kawamura K, Chung KC. Treatment of scaphoid fractures and nonunions. J Hand Surg Am. 2008 Jul-Aug;33(6):988-97. doi: 10.1016/j.jhsa.2008.04.026. Review. PubMed PMID: 18656779.
Question 14High Yield
A pantalar arthrodesis is described as a:
Explanation
A pantalar arthrodesis is the combination of an ankle and triple arthrodesis. It should not be confused with an ankle and subtalar arthrodesis (tibiotalocalcaneal).
Question 15High Yield
The most common soft tissue sarcoma of the foot and ankle is:
Explanation
Malignant melanoma is the most common soft tissue malignancy of the foot; however, synovial sarcoma is the most common soft tissue sarcoma. There may be a long duration of presence of the mass, with or without growth of the lesion. When one evaluates a patient with a small or large soft tissue mass on the foot, synovial sarcoma should be considered in the differential diagnosis.
Question 16High Yield
The examination suggests a neurologic deficit of which nerve?
Explanation
- Common peroneal nerve
Question 17High Yield
Figure 26 is the posteroranterior chest radiograph of a 76-year-old man with an atraumatic gradually enlarging mass overlying his left clavicle that has been present for 6 months. There are no changes in overlying skin. His only noteworthy medical history involves facial squamous cell carcinomas that have been successfully removed surgically.

Explanation
- MRI with and without contrast_
Question 18High Yield
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future?
Explanation
More than than 90% of preadolescent children who sustain a significant spinal cord injury subsequently develop scoliosis. Conversely, progressive paralytic spinal deformity is uncommon in the postadolescent patient. Bracing has not been shown to be effective in the prevention of scoliosis in the preadolescent patient with spinal cord injury.
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Dearolf WW III, Betz RR. Vogl LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Mehta S, Betz RR. Mulcahey MJ, et al: Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med 2004;27:S88-S92.
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Dearolf WW III, Betz RR. Vogl LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Mehta S, Betz RR. Mulcahey MJ, et al: Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med 2004;27:S88-S92.
Question 19High Yield
Figure 1 is the radiograph of a 12-year-old baseball player who has posterolateral elbow pain with throwing. The area of interest is designated by the black arrow. His range of motion and strength are full. No previous treatment has been provided. What is the most appropriate initial treatment?
Explanation
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
Question 20High Yield
Figure 37a is the initial radiograph of a 7-year-old boy who fell from monkey bars 4 hours ago. He has intact motor function in his fingers and normal capillary refill, but his radial pulse is not palpable. Figures 37b and 37c are the radiographs following closed reduction and pinning. This boy’s hand and fingers remain pink, but his radial pulse remains nonpalpable. What is the best next step?
Explanation
Figure 37a shows a completely displaced supracondylar humerus fracture. The first step in the situation described, which involves a pink pulseless hand, is to perform an urgent closed manipulation and pinning. The vascular examination should be reassessed following the reduction. When adequate reduction has been achieved and the pulse remains nonpalpable but the hand is pink and capillary refill is normal, the fracture may be splinted and the patient observed closely in the hospital. Arteriography is not useful and may delay revascularization or increase vessel spasm. Although some investigators have concluded that exploration of the brachial artery may be indicated, the algorithm that includes observation only is the most supported and the most commonly practiced treatment. The radiographs show adequate reduction and fixation without medial widening at the fracture site, which might indicate a site of brachial artery entrapment. Therefore, pin removal and fracture rereduction is not indicated.
RESPONSES FOR QUESTIONS 38 THROUGH 45
1. Sclerosis of the proximal femoral epiphysis with subchondral lucency
2. Abnormal femoral head-neck junction offset
3. Widening of the proximal femoral physis with normal femoral head-neck junction offset
4. Absence of the proximal femoral epiphysis secondary ossification center
For each clinical scenario below, select the most likely associated radiographic finding from the list above.
RESPONSES FOR QUESTIONS 38 THROUGH 45
1. Sclerosis of the proximal femoral epiphysis with subchondral lucency
2. Abnormal femoral head-neck junction offset
3. Widening of the proximal femoral physis with normal femoral head-neck junction offset
4. Absence of the proximal femoral epiphysis secondary ossification center
For each clinical scenario below, select the most likely associated radiographic finding from the list above.
Question 21High Yield
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to**
Explanation
Studies examining the impact of graded water debt have clearly shown that the magnitude of core temperature and heart rate increase accompanying work are proportional to the magnitude of water debt at the onset of exercise. Though added thermal burden from hot climates is a factor, it appears to be less significant.
REFERENCES: Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524.
Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Sawka MN, Young AJ, Francesconi RP, et al: Thermoregulatory and blood responses during exercise at graded hypohydration levels. J Appl Physiol 1985;59:1394-1401.
REFERENCES: Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524.
Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Sawka MN, Young AJ, Francesconi RP, et al: Thermoregulatory and blood responses during exercise at graded hypohydration levels. J Appl Physiol 1985;59:1394-1401.
Question 22High Yield
What is the most appropriate test to order at this time?
Explanation
_
_
_
Question 23High Yield
A 56-year-old woman presents with left hip pain and diminishing range of motion. Examination reveals pain with range of motion of the hip. Radiographs reveal multiple calcific lesions within the hip and well-preserved joint space. MRI scan shows thickened synovium nodular loose bodies with decreased signal on T1 and T2. What is the best next step?
Explanation
The patient has synovial chondromatosis, a benign metaplastic disorder of cartilagenous synovial nodules, often intra-articular. This condition is usually monoarticular, most commonly affecting the knee, followed by hip, elbow and shoulder. It occurs preferentially in men between the ages of 20 to 40. It may cause pain, mechanical or impingement symptoms and loss of motion, and may cause degenerative changes due to impingement. Synovectomy with excision of the cartilaginous nodules is the treatment of choice, and equally good results may be achieved with arthroscopic debridement and open debridement. Recurrence rates vary, reported from 0% to 22%. THA would not be indicated without the presence of arthritis.
Question 24High Yield
16A
B
C
Figures 16a through 16c are the postsurgical radiographs taken 3 months after surgical stabilization of the fracture and syndesmosis. The patient has no pain and symmetrical range of motion to the contralateral lower extremity. What is the most appropriate next step?
B
C
Figures 16a through 16c are the postsurgical radiographs taken 3 months after surgical stabilization of the fracture and syndesmosis. The patient has no pain and symmetrical range of motion to the contralateral lower extremity. What is the most appropriate next step?



Explanation
- Retention of hardware with progression of activity
Question 25High Yield
What is the best next step? 1- Knee aspiration
Explanation
- Blood cultures
Question 26High Yield
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?
Explanation
Use of systemic steroids has been implicated in the development of nontraumatic osteonecrosis of the humeral head. Staging of the disease is most relevant to prognosis and treatment. Cruess has described a widely accepted staging system. Several authors have shown that patients who have a lower stage of disease (ie, stage I or II) have a much less likely chance of progression compared with those who are in the later stages (IV and V).
REFERENCES: Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39.
Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Relationship of disease stage, extent, and cause to natural history. J Shoulder Elbow Surg 1999;8:559-564.
REFERENCES: Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39.
Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Relationship of disease stage, extent, and cause to natural history. J Shoulder Elbow Surg 1999;8:559-564.
Question 27High Yield
Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?
Explanation
The initial stages of posterior tibial tendon insufficiency, where the deformity remains supple, may be treated with bracing or an orthotic for pain relief. The Arizona brace was introduced in 1988, and assists in pain relief and deformity correction by minimizing hindfoot valgus alignment, lateral calcaneal displacement, and medial ankle collapse. It is particularly helpful in those patients with advanced disease that cannot tolerate an ankle-foot orthosis. All other choices are incorrect because of the addition of lateral posting, which is not advantageous in valgus deformities. The addition of medial posting to any of the above choices would render them correct alternatives. A heel lift is applicable in Achilles tendon disorders, not posterior tibial tendon disorders.
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
Question 28High Yield
A 35-year-old male sustains the fracture seen in Figures A and B. Which of the following substances has been shown to result in the least radiographic subsidence when combined with open reduction and internal fixation?


Explanation
Figures A and B show a plateau fracture with a lateral split and depression of the articular surface. In treating tibial plateau fractures, calcium phosphate has been shown to have the least amount of articular subsidence on follow-up examinations due to its high compressive strength.
The study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement. Welch and Zhang reproduced tibial plateau fractures in goats and compared cancellous autograft to calcium phosphate cement augmentation. At 24 hours, four of five specimens treated with autograft had subsidence of the fragment. Only two specimens from limbs treated with cement showed minimal subsidence; the remaining were congruent.
Yetkinler’s study compared cement to no cement treatment in a model of depressed plateau fractures. Calcium phosphate cement of high compressive
strength provided equivalent or better stability than conventional open reduction
and internal fixation with either auto/allograft bone which had both a lower compressive strength and reduced mechanical stability.
The study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement. Welch and Zhang reproduced tibial plateau fractures in goats and compared cancellous autograft to calcium phosphate cement augmentation. At 24 hours, four of five specimens treated with autograft had subsidence of the fragment. Only two specimens from limbs treated with cement showed minimal subsidence; the remaining were congruent.
Yetkinler’s study compared cement to no cement treatment in a model of depressed plateau fractures. Calcium phosphate cement of high compressive
strength provided equivalent or better stability than conventional open reduction
and internal fixation with either auto/allograft bone which had both a lower compressive strength and reduced mechanical stability.
Question 29High Yield
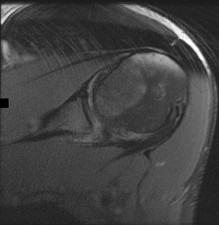
Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
Explanation
Historically, orthopaedic surgeons considered early range-of-motion programs following rotator cuff surgery secondary to concerns about potential postsurgical stiffness. Although this may have been a concern with primary open repair, arthroscopic surgery appears to substantially decrease this risk. More recently, investigators are reporting similar results in terms of range of motion, retear rate, and functional outcome scores among patients who undergo early versus delayed rehabilitation programs.
Question 30High Yield
Slide 1
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
Explanation
The extensor hallucis longus or the extensor hallucis brevis (rarely the abductor hallucis) may be used as a tendon transfer for correction. Arthrodesis of the hallux interphalangeal joint may be performed for correction of a fixed claw deformity of the interphalangeal joint, usually in conjunction with a tendon transfer. Arthrodesis of the metatarsophalangeal joint is a reasonable alternative provided there is no fixed deformity of the interphalangeal joint present and when arthritis or fixed deformity of the metatarsophalangeal joint is present.
Question 31High Yield
Figure 1 is the MRI scan of a 19-year-old man who has an acute anterior shoulder dislocation. The bony fragment occupies 10% of the glenoid articular surface. What is the most appropriate treatment?
---
---
Explanation
The MRI scan shows a bony Bankart lesion involving <20% of the glenoid joint surface. A recent series reported high success rates after arthroscopic treatment when the defect is incorporated into the repair. Anterior bony deficiencies occupying >25% to >30% of the glenoid joint surface treated with soft-tissue repair only are associated with high recurrence rates. In these patients, an open or arthroscopic coracoid transfer or structural iliac crest graft should be considered. Open reduction and internal fixation has been reported for treatment of large acute glenoid rim fractures but is not recommended for recurrent anterior shoulder instability in the setting of a 10% glenoid rim fracture.
Question 32High Yield
Figures 5a through 5h
A B
C
6
D E F
G
H
A B
C
6
D E F
G
H







Explanation
- Calcaneonavicular (CN) coalition
Question 33High Yield
Which inflammatory marker is most closely tied to a systemic inflammatory response following orthopaedic injury and treatment?


Explanation
No detailed explanation provided for this question.
Question 34High Yield
Which of the following is not associated with increased risk of stress fractures:
Explanation
Any history of frequent or prolonged corticosteroid use, hyperparathyroidism, rheumatoid arthritis, hyperthyroidism, celiaCsprue, previous stress fractures or overuse injuries as well as signs or symptoms of an eating disorder also should draw oneâs attention to the possibility of a reduced bone mass
Question 35High Yield
A 22-year-old male sustains the injury seen in Figures A and B as the result of a motor vehicle collision. He subsequently undergoes the procedure shown in Figures C and D with a 12 millimeter nail. When would full weight-bearing be allowed after surgery?




Explanation
Comminuted femoral shaft fractures treated with statically locked intramedullary nails of appropriate diameter can be treated with immediate weight-bearing, with little risk of nail/screw breakage or deformity. Immediate range of motion and weight-bearing can be extremely beneficial to short-term patient outcomes, especially in polytrauma patients.
Brumback et al.(1988) reviewed 133 dynamically locked femoral nails and report that 10.5% lost fixation and/or reduction postoperatively. They recommend reviewing high-quality radiographs to determine fracture characteristics, and note that dynamic fixation only be considered for transverse fracture patterns.
Brumback et al.(1988) performed a prospective series of 97 patients with statically locked femoral nails, and they report that 98% of these went on to successful union without additional procedures, and the 2% with nonunions were successfully treated with later conversion to dynamic interlocking. They also found that no implant failure or deformity occurred with early walking or weight-bearing.
Brumback et al.(1999) reviewed the biomechanics of immediate weightbearing after statically locked intramedullary nails are used in a segmental femur model, and they found that it would be safe. They then looked at immediate weight-bearing of these fractures after statically locked nail insertion in a series of 35 patients, and found no loss of reduction or implant failure with immediate weight-bearing.
Figures A and B show a comminuted, segmental femoral shaft fracture, while Figures C and D show the immediate postoperative radiographs of this patient after intramedullary nailing.
Incorrect Answers:
Answers 2-5: Delay in weight-bearing is not required for this injury pattern, if treated with an appropriate diameter statically locked intramedullary nail.
Brumback et al.(1988) reviewed 133 dynamically locked femoral nails and report that 10.5% lost fixation and/or reduction postoperatively. They recommend reviewing high-quality radiographs to determine fracture characteristics, and note that dynamic fixation only be considered for transverse fracture patterns.
Brumback et al.(1988) performed a prospective series of 97 patients with statically locked femoral nails, and they report that 98% of these went on to successful union without additional procedures, and the 2% with nonunions were successfully treated with later conversion to dynamic interlocking. They also found that no implant failure or deformity occurred with early walking or weight-bearing.
Brumback et al.(1999) reviewed the biomechanics of immediate weightbearing after statically locked intramedullary nails are used in a segmental femur model, and they found that it would be safe. They then looked at immediate weight-bearing of these fractures after statically locked nail insertion in a series of 35 patients, and found no loss of reduction or implant failure with immediate weight-bearing.
Figures A and B show a comminuted, segmental femoral shaft fracture, while Figures C and D show the immediate postoperative radiographs of this patient after intramedullary nailing.
Incorrect Answers:
Answers 2-5: Delay in weight-bearing is not required for this injury pattern, if treated with an appropriate diameter statically locked intramedullary nail.
Question 36High Yield
Which of the following is true concerning the repair of acute Achilles tendon ruptures:
Explanation
This meta-analysis showed:
Operative versus nonoperative (pooled rates):
Rerupture
Operative 3.5% (6/173) (relative risk 0.27) Nonoperative 12.6% (23/183)
Complications (adhesions, infection, disturbed sensibility)
Operative 34.1% (59/173) (relative risk 10.60) Nonoperative 2.7% (5/183)
Infection
Operative 4.0% (7/173) (relative risk 4.89) Nonoperative 0%
Operative versus nonoperative (pooled rates):
Rerupture
Operative 3.5% (6/173) (relative risk 0.27) Nonoperative 12.6% (23/183)
Complications (adhesions, infection, disturbed sensibility)
Operative 34.1% (59/173) (relative risk 10.60) Nonoperative 2.7% (5/183)
Infection
Operative 4.0% (7/173) (relative risk 4.89) Nonoperative 0%
Question 37High Yield
Which of the following zones of the articular cartilage most likely seals the cartilage off from the immune system:
Explanation
The superficial zone has a number of important characteristics: Thinnest articular cartilage layer
Two layers:
Most superficial – fine collagen fibrils (lamina splendens)
Deep layer – flattened fibroblast-like chondrocytes (parallel to joint surface) Forms a cartilage skin
Important chemical properties:
High collagen and low proteoglycan concentration
Fibronectin and water concentrations are highest in this zone
Great tensile stiffness and strength
Seals off the cartilage from the immune system
Two layers:
Most superficial – fine collagen fibrils (lamina splendens)
Deep layer – flattened fibroblast-like chondrocytes (parallel to joint surface) Forms a cartilage skin
Important chemical properties:
High collagen and low proteoglycan concentration
Fibronectin and water concentrations are highest in this zone
Great tensile stiffness and strength
Seals off the cartilage from the immune system
Question 38High Yield
Which of the following blood vessels supplies the majority of the scaphoid:
Explanation
Gelberman and Menon used injection studies to demonstrate that the majority of scaphoid blood flow stems from branches of the radial artery entering the scaphoid at the distal pole. Of these, the branch entering the dorsal ridge supplies 70% to 80% of the intraosseous vascularity of the scaphoid bone. The proximal pole is completely dependent on the intraosseous blood supply and is vulnerable to avascular necrosis when fracture disrupts this vascular source.
Question 39High Yield
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
With soft-tissue loss, local or free flap coverage may be necessary to treat exposed tendon and bone. However, a vacuum-assisted closure device is a good temporizing dressing. It prevents external contamination, reduces edema around the wound, increases oxygen tension in the wound, and promotes the formation of granulation tissue. The use of this negative pressure device has been described in both acute traumatic and in chronic wound scenarios. If sufficient granulation tissue forms, closure may be by split graft, avoiding a more complex coverage procedure. Immediate skin grafting over the exposed anterior tibial tendon and tibia would have a low likelihood of success. Dressing changes with sulfasalazine may be beneficial in a burn wound to assist with removal of skin slough; however, in a granulating wound, the material may be toxic to early epithelialization. Xenograft is a foreign body and should not be applied to an acute contaminated open wound. Historically, a cross-leg flap was a treatment alternative for lower extremity soft-tissue loss; however, its current applications are extremely limited.
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
Question 40High Yield
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
Explanation
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
1. Cortical thickening in the region of the lesion
2. Erosive metaphyseal lesion with loss of cortical integrity
3. Normal bony anatomy on radiographs
4. Diffuse articular erosion with loss of joint space
5. Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
6. Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
RESPONSES FOR QUESTIONS 57 THROUGH 62
1. Cortical thickening in the region of the lesion
2. Erosive metaphyseal lesion with loss of cortical integrity
3. Normal bony anatomy on radiographs
4. Diffuse articular erosion with loss of joint space
5. Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
6. Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
Question 41High Yield
Figures 1 through 4 show the radiographs and MRI scans of a 69-year-old woman with neck and upper extremity pain and progressive deformity of the cervical spine. What is the most likely diagnosis?

Explanation
■
Laminectomy without fusion for the treatment of cervical spondylotic myelopathy currently plays a minor role in the management of this disorder because of its many disadvantages. The actual incidence of postlaminectomy kyphosis is unknown, but is estimated to be between 11% and 47%. It can result in recurrent myelopathy if the spinal cord becomes draped over the kyphosis. In addition to the neurologic sequelae, the kyphosis itself can be a source of neck pain and deformity. Spondylolisthesis can develop, contributing to further cord compression. In this case, the patient had undergone a previous C4-5 anterior cervical diskectomy and fusion followed by a posterior laminectomy from C2 through C7, without fusion. This has resulted in severe kyphosis (i.e. postlaminectomy kyphosis) with grade IIIII spondylolisthesis at C3-4 and a grade I spondylolisthesis at C2-3. While ankylosing spondylitis can also result in a chin-on-chest deformity secondary to ankylosis, there is no evidence of marginal syndesmophytes in the imaging studies to suggest this diagnosis. The occiput is hyperextended on C1 on the lateral upright radiograph to compensate for the kyphosis in an attempt to maintain horizontal gaze. This results in an unusual appearing relationship on the imaging studies. However, there is no widening of the distance between C1 and the occiput and no evidence of soft-tissue injury on the MRI scans to suggest an acute injury. C3-4 demonstrates an unstable spondylolisthesis and was never intended to be included in the C4-5 fusion.
Laminectomy without fusion for the treatment of cervical spondylotic myelopathy currently plays a minor role in the management of this disorder because of its many disadvantages. The actual incidence of postlaminectomy kyphosis is unknown, but is estimated to be between 11% and 47%. It can result in recurrent myelopathy if the spinal cord becomes draped over the kyphosis. In addition to the neurologic sequelae, the kyphosis itself can be a source of neck pain and deformity. Spondylolisthesis can develop, contributing to further cord compression. In this case, the patient had undergone a previous C4-5 anterior cervical diskectomy and fusion followed by a posterior laminectomy from C2 through C7, without fusion. This has resulted in severe kyphosis (i.e. postlaminectomy kyphosis) with grade IIIII spondylolisthesis at C3-4 and a grade I spondylolisthesis at C2-3. While ankylosing spondylitis can also result in a chin-on-chest deformity secondary to ankylosis, there is no evidence of marginal syndesmophytes in the imaging studies to suggest this diagnosis. The occiput is hyperextended on C1 on the lateral upright radiograph to compensate for the kyphosis in an attempt to maintain horizontal gaze. This results in an unusual appearing relationship on the imaging studies. However, there is no widening of the distance between C1 and the occiput and no evidence of soft-tissue injury on the MRI scans to suggest an acute injury. C3-4 demonstrates an unstable spondylolisthesis and was never intended to be included in the C4-5 fusion.
Question 42High Yield
A 32-year-old professional skydiver lands awkwardly during a jump. He presents to the emergency room with bilateral knee injuries.
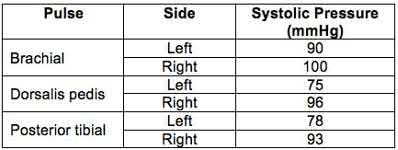
Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Explanation
The ankle-brachial index (ABI) of left and right limbs are 0.78 and 0.96 respectively. CT angiography (or conventional angiography) of the left lower extremity is indicated because of abnormal ABI <0.9. It is sufficient to observe the right lower extremity (ABI >0.9).
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI <0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Answer 1: If vascular exam is normal and ABI >0.9, neurovascular checks every 2-4 hours for 48 hours is appropriate. As ABI is abnormal on the left, CT angiogram is necessary.
Answer 2: Anticoagulation has not been shown to stop thrombus formation for non-flow limiting intimal flap tears.
Answer 3: CT angiography is indicated if ABI is abnormal post reduction. CT angiography for the right lower extremity is unnecessary as ABI >0.9.
Answer 5: Surgery is indicated if CT angiography (or conventional angiography) demonstrates intimal flap tears that are flow limiting (but not if the intimal flap is NOT flow limiting), if distal pulses are absent, or if distal ischemia, active hemorrhage, or expanding pulsatile hematoma are present.
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI <0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Answer 1: If vascular exam is normal and ABI >0.9, neurovascular checks every 2-4 hours for 48 hours is appropriate. As ABI is abnormal on the left, CT angiogram is necessary.
Answer 2: Anticoagulation has not been shown to stop thrombus formation for non-flow limiting intimal flap tears.
Answer 3: CT angiography is indicated if ABI is abnormal post reduction. CT angiography for the right lower extremity is unnecessary as ABI >0.9.
Answer 5: Surgery is indicated if CT angiography (or conventional angiography) demonstrates intimal flap tears that are flow limiting (but not if the intimal flap is NOT flow limiting), if distal pulses are absent, or if distal ischemia, active hemorrhage, or expanding pulsatile hematoma are present.
Question 43High Yield
A 35-year-old male presents 6 weeks following open reduction and internal fixation of the injury shown in Figures A and B performed through a sinus tarsi approach. He is a 1/2-pack-per-day smoker and his body mass index (BMI) is 25. He last presented 3 weeks ago at which time his wound appeared healed, and the sutures were removed. Physical therapy was also initiated for gentle range of motion exercises. He reports that his main surgical incision "opened up" a few days ago and has been draining. He denies fevers or chills at this time. On physical exam, he has a small, 1 cm area of wound dehiscence with no exposed hardware. His current radiograph is
shown in Figure C. Which of the following combines the risk factors this patient has for wound dehiscence with the next best step in treatment?
shown in Figure C. Which of the following combines the risk factors this patient has for wound dehiscence with the next best step in treatment?



Explanation
Smoking is a risk factor for wound dehiscence after open reduction and internal fixation (ORIF) of calcaneal fractures. Superficial wound dehiscence should initially be treated with cessation of physical therapy, immobilization, and nonsurgical wound management.
The most common complication associated with ORIF of calcaneus fractures is delayed wound healing. The extensile lateral approach is the most commonly used approach for treating these injuries and has been associated with wound breakdown in nearly 25% of patients. The sinus tarsi approach utilizes a much smaller incision and studies have shown fewer wound healing difficulties. Preoperative risk factors that predispose to wound breakdown include smoking, diabetes, open fractures, high BMI, and closure of the wound in a single layer. In the event of superficial wound breakdown, range of motion exercises should be stopped and a prophylactic course of antibiotics should be started with nonsurgical wound management. If purulence is encountered or the wound is found to be deep, hospitalization with serial debridements and antibiotics is required.
Clare et al. performed a review of how to manage complications of calcaneal fractures. They report that immobilization after wound breakdown should be performed with casting with a window over the wound to allow for wound care and wet-to-dry dressing changes. Once the wound is healed, range-of-motion exercises may be resumed.
Folk et al. performed a review of early wound complications of operative treatment of calcaneus fractures through the lateral extensile approach. They found that smoking, open fractures, and diabetes were risks for a wound complication. They recommend that patients with identifiable risk factors should be counseled of this potential complication.
Figure A is a lateral ankle radiograph demonstrating a displaced, intraarticular calcaneal fracture. Figure B is an axial CT image demonstrating the fracture and the sustentaculum tali. Figure C is a lateral ankle radiograph demonstrating fixation of the fracture with a plate and independent screws.
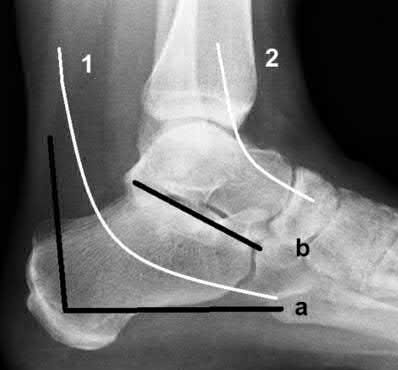
This fixation strategy is utilized along with a sinus tarsi approach. Illustration A is a radiograph illustrating the two approaches used to fix calcaneus fractures. The letter (a) represents the lateral extensile incision while (b) represents the sinus tarsi incision. The number (1) correlates to the location of the sural nerve, while (2) correlates with the superficial peroneal nerve.
Incorrect Answers:
Answer 1: This patient has a normal BMI and irrigation and debridement with removal of hardware is not indicated at this point as the fracture is not healed. Answer 2: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach. Irrigation and debridement with retention of hardware is not indicated at this point.
Answer 3: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach.
Answer 4: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach. Irrigation and debridement with retention of hardware is not indicated at this point.
The most common complication associated with ORIF of calcaneus fractures is delayed wound healing. The extensile lateral approach is the most commonly used approach for treating these injuries and has been associated with wound breakdown in nearly 25% of patients. The sinus tarsi approach utilizes a much smaller incision and studies have shown fewer wound healing difficulties. Preoperative risk factors that predispose to wound breakdown include smoking, diabetes, open fractures, high BMI, and closure of the wound in a single layer. In the event of superficial wound breakdown, range of motion exercises should be stopped and a prophylactic course of antibiotics should be started with nonsurgical wound management. If purulence is encountered or the wound is found to be deep, hospitalization with serial debridements and antibiotics is required.
Clare et al. performed a review of how to manage complications of calcaneal fractures. They report that immobilization after wound breakdown should be performed with casting with a window over the wound to allow for wound care and wet-to-dry dressing changes. Once the wound is healed, range-of-motion exercises may be resumed.
Folk et al. performed a review of early wound complications of operative treatment of calcaneus fractures through the lateral extensile approach. They found that smoking, open fractures, and diabetes were risks for a wound complication. They recommend that patients with identifiable risk factors should be counseled of this potential complication.
Figure A is a lateral ankle radiograph demonstrating a displaced, intraarticular calcaneal fracture. Figure B is an axial CT image demonstrating the fracture and the sustentaculum tali. Figure C is a lateral ankle radiograph demonstrating fixation of the fracture with a plate and independent screws.
This fixation strategy is utilized along with a sinus tarsi approach. Illustration A is a radiograph illustrating the two approaches used to fix calcaneus fractures. The letter (a) represents the lateral extensile incision while (b) represents the sinus tarsi incision. The number (1) correlates to the location of the sural nerve, while (2) correlates with the superficial peroneal nerve.
Incorrect Answers:
Answer 1: This patient has a normal BMI and irrigation and debridement with removal of hardware is not indicated at this point as the fracture is not healed. Answer 2: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach. Irrigation and debridement with retention of hardware is not indicated at this point.
Answer 3: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach.
Answer 4: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach. Irrigation and debridement with retention of hardware is not indicated at this point.
Question 44High Yield
Meleneyâs infection is a:
Explanation
Found in necrotizing fasciitis, Meleneyâs infection is a spreading ulcer rimmed with gangrenous skin. The affected area must be debrided immediately. C ultures are taken at the time of surgery to tailor antibiotic coverage. Amputation is not unusual to control the spread of the gangrenous infection.
Question 45High Yield
Slide 1 Slide 2 Slide 3 Slide 4
A 61-year-old woman presents for treatment of a painful ankle. She reports that 4 years ago, she sustained a fracture of her ankle that was treated with cast immobilization. She has experienced progressively worsening pain over the past 2 years. On examination, she has good range of motion of the ankle with crepitus and pain. Radiographs are presented (Slide 1 and Slide 2). All of the following are acceptable forms of surgical correction except:
A 61-year-old woman presents for treatment of a painful ankle. She reports that 4 years ago, she sustained a fracture of her ankle that was treated with cast immobilization. She has experienced progressively worsening pain over the past 2 years. On examination, she has good range of motion of the ankle with crepitus and pain. Radiographs are presented (Slide 1 and Slide 2). All of the following are acceptable forms of surgical correction except:
Explanation
Each of the alternatives presented is reasonable except for ankle arthroscopy because it has a limited role in the management of posttraumatic arthritis of the ankle. In this patient, there is a possibility to salvage the ankle before arthrodesis or joint replacement with an osteotomy of the tibia and or the fibula. Both have a definite role in management of ankle deformity and arthritis. A closing wedge osteotomy of the tibia was performed in this patient, and she remains asymptomatic 4 years later (Slide
3 and Slide 4).
3 and Slide 4).
Question 46High Yield
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect.
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocation. Am J Sports Med 1995;23:324-331.
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocation. Am J Sports Med 1995;23:324-331.
Question 47High Yield
An 18-month-old boy is brought to your office for a clawing deformity of his right hand. The parents inform you that he was born full term after a difficult delivery complicated by shoulder dystocia. The boy weighed 9½ lbs at birth. The child had a brief episode of apnea with an APGAR score of 5 at birth and needed resuscitation and admission to the natal intensive care unit. Parents recall having noted a bump on his right clavicle, which was tender and was diagnosed as clavicle fracture. They also noticed a week later that the child did not flex the fingers of his right hand. The neonatologist had informed them that the
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
Explanation
This is a case of obstetric brachial plexus injury involving the C 8, T1 roots (Klumpke Palsy). Erbâs palsy involves upper roots only. C ombined nerve injuries can present in a similar fashion; however, low ulnar and median nerve lesions will not have weakness of flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS).
History of large baby, shoulder dystocia and clavicle fracture point to a difficult labor. The most common type of brachial plexus injury related to birth is Erbâs palsy, which is usually associated with a breech presentation. Isolated Klumpkeâs palsy is rare, and involvement of C 8, T1 usually occurs as part of global plexus injury.
History of large baby, shoulder dystocia and clavicle fracture point to a difficult labor. The most common type of brachial plexus injury related to birth is Erbâs palsy, which is usually associated with a breech presentation. Isolated Klumpkeâs palsy is rare, and involvement of C 8, T1 usually occurs as part of global plexus injury.
Question 48High Yield
..A 61-year-old right-hand-dominant woman sustains a fall down 3 stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm.
What is the most appropriate treatment?
What is the most appropriate treatment?
Explanation
- Nonsurgical treatment with early passive range of motion
Question 49High Yield
What is the chief mechanism of action of parathyroid hormone (PTH) in the treatment of patients with osteoporosis?
Explanation
■
Recombinant human PTH benefits patients with osteoporosis by stimulating osteoblastic bone formation and reducing osteoblastic apoptosis. Treatment reduces vertebral fractures by 65%. PTH analogs act similarly and reduce vertebral fractures by 47%. Bisphosphonates reduce the resorptive activity of osteoclasts and cause a dissociation of bone formation and resorption that favors bone formation and reduce vertebral fractures by 50% to 70%. Selective estrogen receptor modulators inhibit bone resorption and reduce vertebral fractures by 35%. Humanized monoclonal antibodies inhibit osteoclast formation and reduce vertebral fractures by 68%.
Recombinant human PTH benefits patients with osteoporosis by stimulating osteoblastic bone formation and reducing osteoblastic apoptosis. Treatment reduces vertebral fractures by 65%. PTH analogs act similarly and reduce vertebral fractures by 47%. Bisphosphonates reduce the resorptive activity of osteoclasts and cause a dissociation of bone formation and resorption that favors bone formation and reduce vertebral fractures by 50% to 70%. Selective estrogen receptor modulators inhibit bone resorption and reduce vertebral fractures by 35%. Humanized monoclonal antibodies inhibit osteoclast formation and reduce vertebral fractures by 68%.
Question 50High Yield
An 8-year-old girl has asymmetry on a forward bend test of the spine. She is asymptomatic and has a normal clinical neurologic examination. Radiographs are shown in Figures 22a and 22b. What should be the next step in her work-up?


Explanation
DISCUSSION: There are several reasons to obtain an MRI of the entire spinal cord of this patient to evaluate for abnormalities. These include her young age and the presence of a left-sided curve. For juvenile scoliosis patients with more than a 20-degree Cobb angle, there is an approximately 20% prevalence of a neurologic abnormality. Therefore, recommendations for work-up include an MRI scan of the entire spine.
REFERENCES: Gillingham BL, Fan RA, Akbamia BA: Early onset idiopathic scoliosis. J Am Acad Orthop Surg 2006;14:101-112.
Gupta P, Lenke LG, Bridwell KH: Incidence of neural axis abnormalities in infantile and juvenile patients with spinal deformity: Is a magnetic resonance image screening necessary? Spine 1998;23:206-210.
**24 • American Academy of Orthopaedic Surgeons**
Figure 23a Figure 23b
REFERENCES: Gillingham BL, Fan RA, Akbamia BA: Early onset idiopathic scoliosis. J Am Acad Orthop Surg 2006;14:101-112.
Gupta P, Lenke LG, Bridwell KH: Incidence of neural axis abnormalities in infantile and juvenile patients with spinal deformity: Is a magnetic resonance image screening necessary? Spine 1998;23:206-210.
**24 • American Academy of Orthopaedic Surgeons**
Figure 23a Figure 23b
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon