Free Orthopedics Review | Dr Hutaif General Orthopedics -...
14 Apr 2026
59 min read
84 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Free Orthopedics Review | Dr Hutaif General O...
00:00
Start Quiz
Question 1High Yield
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The most likely complication in this child is:
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The most likely complication in this child is:
Explanation
Ulnar carpal translocation occurs due to the steep radial articular angulation that occurs due to the tethering effect of a shortened ulna and is already apparent in early stages in the first radiograph. While peroneal palsy is possible due to a proximal fibula lesion, it is less common. Malignant transformation occurs, risk varies with families.
Question 2High Yield
The accumulation of what metal was attributed to the 1996 episode of âbeer-drinkersâ cardiomyopathy:
Explanation
The accumulation of Co in the myocardium can induce cardiomyopathy, which was particularly evident after the 1996 episode of âbeer-drinkersâ cardiomyopathy, during which Co was used as a foam-stabilizing agent in beer
Question 3High Yield
Which of the following is not a common finding in cloacal exstrophy:
Explanation
Hydrocephalus is rare because most patients have lipomeningocele, not myelomeningocele.
Omphalocele is common in cloacal exstrophy.
Most patients with cloacal exstrophy have a lipomeningocele that is a form of spinal dysrhaphism. Many patients have malformations of the sacroiliac joints.
Approximately 25% of patients have dislocations of at least one hip.
Omphalocele is common in cloacal exstrophy.
Most patients with cloacal exstrophy have a lipomeningocele that is a form of spinal dysrhaphism. Many patients have malformations of the sacroiliac joints.
Approximately 25% of patients have dislocations of at least one hip.
Question 4High Yield
Patients with ankylosing spondylitis undergoing total knee arthroplasty are likely to experience which of the following complications?
Explanation
DISCUSSION: Patients with ankylosing spondylitis (AS) are likely to have achieved significant pain relief and improvement in function following total knee arthroplasty (TKA). These patients, however, are also likely to experience a higher incidence of complications, particularly stiffness and heterotopic ossification (HO). In one series, the incidence of HO following TKA in patients with AS was 20%.
REFERENCES: Parvizi J, Duffy GP, Trousdale RT: Total knee arthroplasty in patients with ankylosing spondylitis. J Bone Joint Surg Am 2001;83:1312-1316.
Fintersbush A, Amir D, Vatashki E, et al: Joint surgery in severe ankylosing spondylitis. Acta Orthop Scand 1988;59:491-496.
DISCUSSION: Patients with ankylosing spondylitis (AS) are likely to have achieved significant pain relief and improvement in function following total knee arthroplasty (TKA). These patients, however, are also likely to experience a higher incidence of complications, particularly stiffness and heterotopic ossification (HO). In one series, the incidence of HO following TKA in patients with AS was 20%.
REFERENCES: Parvizi J, Duffy GP, Trousdale RT: Total knee arthroplasty in patients with ankylosing spondylitis. J Bone Joint Surg Am 2001;83:1312-1316.
Fintersbush A, Amir D, Vatashki E, et al: Joint surgery in severe ankylosing spondylitis. Acta Orthop Scand 1988;59:491-496.
Question 5High Yield
Figures 1 through 3 are the radiographs of a 40-year-old patient with a history of posterior labral repair who presents with severe pain and stiffness in the shoulder. The pain interferes with activities of daily living and interrupts his sleep at night. He has tried corticosteroid injections, nonsteroidal anti-inflammatory drugs, and activity modification with only temporary benefit. He wishes to discuss definitive treatment options. How can you counsel the patient about treatment with a hemiarthroplasty?
10
10
Explanation
The patient has evidence of osteoarthritis with eccentric glenoid wear. Hemiarthroplasty outcomes are worse in patients with eccentric glenoid wear, as compared to those with a concentric joint. Additionally, hemiarthroplasty has been shown to have inferior functional outcomes compared to total shoulder arthroplasty, with low long-term satisfaction rates. Revision rates are equal to or greater than total shoulder arthroplasty at mid to long term follow-up, and glenoid erosion remains a problem.
Question 6High Yield
A 62-year-old man falls on his porch and sustains an elbow injury. A radiograph is provided in Figure A. Which of the following is the best treatment?

Explanation
The radiograph shows an olecranon fracture with articular comminution and depression of a large intra-articular fragment. This pattern is best treated with plate fixation to support the articular reduction.
Bailey et al reviewed 25 cases of olecranon fractures (simple and comminuted fracture patterns) treated with plate fixation. All 25 went on to union. There were no major complications reported. Twenty percent of patients underwent hardware removal at a later date for prominence.
Hak et al review the treatment options available for olecranon fractures. Simple intra-articular fractures without comminution are suitable for tension band fixation. Comminution of the articular surface is an indication for plate fixation and may benefit from bone graft to support depressed articular segments. Osteoporotic patients or fractures with severe comminution may do better with fragment excision and advancement of the triceps.
Bailey et al reviewed 25 cases of olecranon fractures (simple and comminuted fracture patterns) treated with plate fixation. All 25 went on to union. There were no major complications reported. Twenty percent of patients underwent hardware removal at a later date for prominence.
Hak et al review the treatment options available for olecranon fractures. Simple intra-articular fractures without comminution are suitable for tension band fixation. Comminution of the articular surface is an indication for plate fixation and may benefit from bone graft to support depressed articular segments. Osteoporotic patients or fractures with severe comminution may do better with fragment excision and advancement of the triceps.
Question 7High Yield
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.What is the most likely cause of this patient's pain?
Explanation
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown. The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. Ultrasonography may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasonography is not commonly used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has _important functions for hip stability and maintenance of the suction seal of the joint._
Question 8High Yield
..A 75-year-old woman sustained a 4-part fracture dislocation of the proximal humerus with a comminuted humeral head. You decide to perform a reverse total shoulder replacement because of her age and activity level. This will be your first reverse total shoulder replacement. It is common practice in your hospital for an industry representative to be present when new implants are brought into the operating room. What information are you required to disclose?
Explanation
- There will be an implant company representative in the room.
RESPONSES FOR QUESTIONS 101 THROUGH 104
RESPONSES FOR QUESTIONS 101 THROUGH 104
Question 9High Yield
-Pelvic packing for a hemodynamically unstable patient with a pelvic ring fracture is best described by which of the following techniques?
Explanation
No detailed explanation provided for this question.
Question 10High Yield
Which factor is most important when attempting to prevent interbody graft subsidence?
Explanation
Osteoporosis can affect all aspects of spinal stability and is the most critical factor regarding spinal implant failure. Burring of the end plates may decrease strength of the interface with the uncovering of "softer" cancellous bone. Increasing the surface contact area may help prevent subsidence but is not as important as bone quality. Stress shielding through rigid fixation may lead to construct failure.
RECOMMENDED READINGS
Benzel E (ed): Biomechanics of Spine Stabilization. Rolling Meadows, IL, American Association of Neurological Surgeons, 2001, pp 446-447.
[Goldhahn J, Reinhold M, Stauber M, Knop C, Frei R, Schneider E, Linke B. Improved anchorage in osteoporotic vertebrae with new implant designs. J Orthop Res. 2006 May;24(5):917-25. PubMed PMID: 16583445. ](http://www.ncbi.nlm.nih.gov/pubmed/16583445)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16583445)
RECOMMENDED READINGS
Benzel E (ed): Biomechanics of Spine Stabilization. Rolling Meadows, IL, American Association of Neurological Surgeons, 2001, pp 446-447.
[Goldhahn J, Reinhold M, Stauber M, Knop C, Frei R, Schneider E, Linke B. Improved anchorage in osteoporotic vertebrae with new implant designs. J Orthop Res. 2006 May;24(5):917-25. PubMed PMID: 16583445. ](http://www.ncbi.nlm.nih.gov/pubmed/16583445)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16583445)
Question 11High Yield
Which surgical procedure should be considered for treatment of chronic plantar fasciitis?
Explanation
Imaging studies in the evaluation of plantar fasciitis should always include weight-bearing foot radiographs to reveal alignment and exclude calcaneal stress fracture, tumor, subtalar arthritis, and insertional posterior spurs. MRI is occasionally indicated in problematic cases. Ultrasound can be helpful to evaluate thickening and disease in the proximal plantar fascia. Ultrasound is quick and much more cost effective than MRI. Laboratory screenings to evaluate inflammatory arthritis are indicated only for patients with bilateral heel pain who may be more likely to have systemic disease.
In the nonsurgical treatment of plantar fasciitis, high-impact loading exercises may make the condition worse. Corticosteroid injections may provide short-term relief only and can occasionally cause plantar fascia rupture. They should be used with caution. PRP injections are expensive and currently not covered by insurance. Studies have not demonstrated long-term pain relief with PRP. Plantar fascia-specific stretching has been shown more effective than Achilles tendon stretching alone.
Surgical treatment is indicated for fewer than 5% of patients. It is not necessary to resect the heel spur because the spur is not attached to the plantar fascia and rarely contributes to a patient's pain. The open extensile approach is associated with a much longer recovery than the open or endoscopic approaches and is no longer justified. Multiple studies have demonstrated the efficacy of endoscopic and open plantar fasciotomy techniques.
RECOMMENDED READINGS
Bader L, Park K, Gu Y, O'Malley MJ. Functional outcome of endoscopic plantar fasciotomy. Foot Ankle Int. 2012 Jan;33(1):37-43. doi: 10.3113/FAI.2012.0037. PubMed PMID:
[22381234.](http://www.ncbi.nlm.nih.gov/pubmed/22381234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22381234)
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133.](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
In the nonsurgical treatment of plantar fasciitis, high-impact loading exercises may make the condition worse. Corticosteroid injections may provide short-term relief only and can occasionally cause plantar fascia rupture. They should be used with caution. PRP injections are expensive and currently not covered by insurance. Studies have not demonstrated long-term pain relief with PRP. Plantar fascia-specific stretching has been shown more effective than Achilles tendon stretching alone.
Surgical treatment is indicated for fewer than 5% of patients. It is not necessary to resect the heel spur because the spur is not attached to the plantar fascia and rarely contributes to a patient's pain. The open extensile approach is associated with a much longer recovery than the open or endoscopic approaches and is no longer justified. Multiple studies have demonstrated the efficacy of endoscopic and open plantar fasciotomy techniques.
RECOMMENDED READINGS
Bader L, Park K, Gu Y, O'Malley MJ. Functional outcome of endoscopic plantar fasciotomy. Foot Ankle Int. 2012 Jan;33(1):37-43. doi: 10.3113/FAI.2012.0037. PubMed PMID:
[22381234.](http://www.ncbi.nlm.nih.gov/pubmed/22381234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22381234)
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133.](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
Question 12High Yield
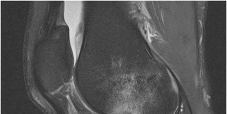
Figure 1 is the MRI scan of a 35-year-old female soccer player who injured her knee during a game. Given the findings of the scan, physical examination is most likely to reveal

Explanation
---
---
DISCUSSION:
The MRI scan clearly reveals bone bruises in the mid lateral femoral condyle and posterior tibial plateau. These MRI findings are commonly associated with acute anterior cruciate ligament injuries. Therefore, the preferred answer would be a positive pivot shift examination. A positive posterior drawer and positive quad active test are associated with posterior cruciate ligament injuries. A positive dial test would be suggestive of a posterolateral instability of the knee.
---
DISCUSSION:
The MRI scan clearly reveals bone bruises in the mid lateral femoral condyle and posterior tibial plateau. These MRI findings are commonly associated with acute anterior cruciate ligament injuries. Therefore, the preferred answer would be a positive pivot shift examination. A positive posterior drawer and positive quad active test are associated with posterior cruciate ligament injuries. A positive dial test would be suggestive of a posterolateral instability of the knee.
Question 13High Yield
Figures 5a through 5h
A B
C
6
D E F
G
H
A B
C
6
D E F
G
H







Explanation
- Calcaneonavicular (CN) coalition
Question 14High Yield
With a full-thickness articular cartilage injury, the body’s healing response produces cartilage mainly composed of what type of collagen?
Explanation
With a full-thickness articular cartilage injury, a healing response is initiated with hematoma, stem cell migration, and vascular ingrowth. This response produces type I collagen and resultant fibrous cartilage rather than desired hyaline cartilage as produced by chondrocytes. This repair cartilage has diminished resiliency, stiffness, poor wear characteristics, and the predilection for arthritis. Type I collagen is also found in the annulus of intervertebral disks, tendon, bone, meniscus, and skin. Type II is found in articular cartilage and nucleus pulposus of intervertebral disks. Type III is found in skin and blood vessels, type IV is found in basement membranes, and type X is found in the calcified layer of cartilage.
REFERENCES: Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Brinker M: Basic Science in Review of Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2000.
REFERENCES: Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Brinker M: Basic Science in Review of Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2000.
Question 15High Yield
..A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
Explanation
- Total elbow arthroplasty (TEA)
Question 16High Yield
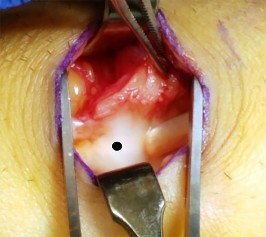
Figures 1 and 2 show the intraoperative photographs obtained during surgical treatment for de Quervain tendonitis. For orientation purposes, dorsal is at the top. Figure 1 is obtained just after the initial first extensor compartment release, and Figure 2 shows the floor of the first extensor compartment. If the structure marked by the black dot is not addressed, the most common postoperative problem would be

Explanation
The black dot identifies an accessory compartment of the extensor pollicis brevis (EPB) tendon. The incidence of accessory EPB compartment in patients undergoing surgical treatment for de Quervain syndrome ranges from 46% to 60%. Failure to release this compartment at the time of initial surgery can cause persistent postoperative pain. The patient would not experience altered sensation if this compartment were not released. Altered sensation would most commonly occur following injury to the dorsal radial sensory nerve branch during surgery. EPB tendon subluxation also would not occur should the accessory compartment not be released. For EPB tendon subluxation to occur, its own compartment would need to be released first. Finally, EPB tendon rupture would be an extremely uncommon complication of failure to release the accessory compartment.
Question 17High Yield
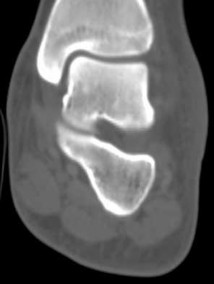
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of**
Explanation
The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present.
REFERENCES: Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Shaughnessy WJ, Bianco AJ: Osteochondritis dissecans, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 282-287.
REFERENCES: Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Shaughnessy WJ, Bianco AJ: Osteochondritis dissecans, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 282-287.
Question 18High Yield
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?
Explanation
Distraction interposition arthroplasty is indicated for the treatment of both rheumatoid and posttraumatic arthritis and is reserved for younger patients who are not suitable candidates for total elbow arthroplasty. Although less reliable than prosthetic replacement, distraction interposition arthroplasty is a useful option in the treatment of young, high-demand patients with elbow arthritis. It is rarely indicated in the presence of polyarticular inflammatory arthritis but may be of value in those patients in whom the disease is limited primarily to the elbow. Isolated radiocapitellar arthritis can be successfully treated with radial head resection, although caution should be exercised if there is evidence of instability. Osteoarthritis is best treated with ulnohumeral arthroplasty.
REFERENCES: Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Mansat P: Surgical treatment of the rheumatoid elbow. Joint Bone Spine 2001;68:198-210.
REFERENCES: Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Mansat P: Surgical treatment of the rheumatoid elbow. Joint Bone Spine 2001;68:198-210.
Question 19High Yield
What is the most appropriate indication for replantation in an otherwise healthy
35-year-old man?
35-year-old man?
Explanation
Vascular anastamoses are exceedingly difficult with amputations distal to the nail fold as the digital vessels bifurcate or trifurcate at this level, and little functional benefit is gained compared to other means of soft-tissue coverage. Single digit amputations, other than
the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy
active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time
of less than 6 hours.
the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy
active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time
of less than 6 hours.
Scientific References
- : Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Boulas HJ: Amputations of the fingers and hand: Indications for replantation. J Am Acad Orthop Surg 1998;6:100-105.
Question 20High Yield
A 72-year-old man has had right knee pain for 4 years that is worsening. Three years ago, he was walker-dependent and received knee injections without any relief (Figure
Explanation
Hip disease can present with knee pain in up to 47% of cases. The knee may be the only location of pain. Hip disease should be suspected as a cause of knee pain in patients who have pain and disability disproportionate to disease severity, especially with use of walkers and wheelchairs, symptoms nonresponsive to injections, surgical management, and with limbs fixed in external rotation making it difficult to obtain anteroposterior imaging. This patient has all of these features. His hip radiograph is shown in Figure 4.
33
33
Question 21High Yield
Which of the following treatments is not used for acute scapholunate ligament ruptures:
Explanation
Proximal row carpectomy is a salvage procedure for chronic instability with focal radioscaphoid arthritis. Open repair with sutures through bone tunnels, open repair with suture anchors, and arthroscopically assisted reduction and pinning have been used successfully in acute cases.
Question 22High Yield
A 42-year-old male sustains a closed, isolated ulna shaft fracture with 2mm displacement and 3 degrees valgus angulation. He is treated conservatively with early range of motion but presents at one year with a painful atrophic nonunion. What treatment is indicated at this time?
Explanation
Appropriate treatment of an atrophic nonunion of the ulna includes open reduction and internal fixation with autogenous bone grafting. The atrophic nature of the nonunion reveals that biology, and not necessarily stability, is the major issue of the nonunion. The referenced article by Ring et al reviews a case series of these patients and found that even in the face of significant preoperative bone resorption, good clinical outcomes and union rate is possible with open plating and grafting. The article by Street reviews intramedullary nailing/pinning of the forearm, and found a 7% nonunion rate with this technique.
Question 23High Yield
Figure 42 shows the radiograph of a 70-year-old woman who has had a painful near ankylosis of her dominant elbow for 1 year. Treatment should consist of
Explanation
The patient has arthritis and supracondylar nonunion of the elbow. Total elbow replacement has been shown to give almost immediate return of function as it can be performed while leaving the triceps intact and resecting the distal humerus fragment. Attempts at osteosynthesis are indicated in younger individuals with good joint surface. Resection arthroplasty yields poor function and is reserved as a salvage procedure.
REFERENCES: Ramsey ML, Morrey BF: Total elbow arthroplasty for nonunion and dysfunctional instability, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Sim FH, Morrey BF: Nonunion and delayed union of distal humeral fractures, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
REFERENCES: Ramsey ML, Morrey BF: Total elbow arthroplasty for nonunion and dysfunctional instability, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Sim FH, Morrey BF: Nonunion and delayed union of distal humeral fractures, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Question 24High Yield
Patients initially treated with intravenous (IV) antibiotics are at higher risk for failure of nonsurgical treatment in the setting of
Explanation
- diabetes.
Question 25High Yield
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?

Explanation
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
**Question 42of 100** Figure 1 shows an injury sustained by a 60-year-old man 4 weeks ago. Since that time he has had substantial pain and catching of his finger during attempts at range of motion. What is the most appropriate treatment at this point?
---
1. Tendon debridement
2. Release of the A2 pulley
3. Tendon repair with core sutures
4. Tendon repair with epitendinous sutures
PREFERRED RESPONSE: D
EXPLANATION:
Approximately 70% laceration of the flexor digitorum profundus tendon with active locking is best treated with epitendinous sutures. Performing this procedure under local anesthetic allows for better assessment
of whether the triggering has been resolved. Cyclic loading has been shown to increase with high-grade partial lacerations. Use of core sutures adds little strength to a partial laceration. Debridement alone is reserved for injuries involving less than 60% of the tendon diameter. Release of the A2 wouldcompromise _pulley function._
**Question 42of 100** Figure 1 shows an injury sustained by a 60-year-old man 4 weeks ago. Since that time he has had substantial pain and catching of his finger during attempts at range of motion. What is the most appropriate treatment at this point?
---
1. Tendon debridement
2. Release of the A2 pulley
3. Tendon repair with core sutures
4. Tendon repair with epitendinous sutures
PREFERRED RESPONSE: D
EXPLANATION:
Approximately 70% laceration of the flexor digitorum profundus tendon with active locking is best treated with epitendinous sutures. Performing this procedure under local anesthetic allows for better assessment
of whether the triggering has been resolved. Cyclic loading has been shown to increase with high-grade partial lacerations. Use of core sutures adds little strength to a partial laceration. Debridement alone is reserved for injuries involving less than 60% of the tendon diameter. Release of the A2 wouldcompromise _pulley function._
Question 26High Yield
**ORTHOPEDIC MCQS OB 20 BASIC7**
700. What method of spinal fixation requires the largest force to disrupt the bone-implant interface?
700. What method of spinal fixation requires the largest force to disrupt the bone-implant interface?
Explanation
concerning available
alternatives as well as the consequences of no treatment must also ensue. The explanation must be made in simple lay terms. 3) The participant must have the mental competency to comprehend the information. 4) There should be reasonable steps to ascertain that the subject understands all aspects of the discussion. 5) The subject actually makes a decision regarding participation.
708. What molecules have been shown to promote fibrosis during muscle injury?
1. Insulin growth factor 1 (IGF-1)
2. Basic fibroblast growth factor (bFGF)
3. Transforming growth factor beta 1 (TGF-ß1)
4. Bone morphogenetic protein
CORRECT answer: 3
A muscle's response to injury can be divided into 4 phases: necrosis, inflammation, repair, and fibrosis. Necrosis involves the degeneration of the muscle fibrils and death. The inflammatory cells then phagocytose the debris and secrete cytokines that promote vascularity. Muscle regeneration does not occur until phagocytic cells remove the debris. Consequently, anti- inflammatory drugs may have negative effects on muscle healing by inhibiting macrophage-induced phagocytosis. Muscle fibrosis occurs at the same time as muscle regeneration and has been shown to involve TGF-ß1. IGF-1 and bFGF are important trophic factors in muscle regeneration. Bone morphogenetic protein has several functions including bone and cartilage regeneration.
709. A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
1. case series.
2. case-control study.
3. cohort study.
4. randomized clinical trial.
CORRECT answer: 1
The type of study design in which a series of cases is presented with outcomes (without a control population or comparison group) is known as a case series. This type of study design, although frequently seen in orthopaedic literature, provides the lowest level of evidence. There is no control group and the population is usually poorly defined. This type of study can be helpful as a starting point for further analysis. A randomized trial provides the highest level of evidence in medical research, featuring a comparison group and
randomized (and usually blinded) placement of subjects into study groups. In case-control studies, cases are compared to a control group. The control group has not
been randomized, but may be a naturally occurring group of subjects who
have not had the same exposure or intervention as the case group. A cohort study can be retrospective or prospective and usually looks at a large group of people over time to assess exposures and incidence of disease.
710. What effect does intermittent administration of parathyroid hormone have on bone?
1. Anabolic
2. Catabolic
3. No effect
4. Decreased quantity
5. Decreased quality
CORRECT answer: 1
Treatment of osteoporosis centers on increasing bone mass by direct anabolic effect and/or inhibiting osteoclastic absorption. Bisphosphonates, selective estrogen receptor modulators, and calcitonin act to decrease bone resorption by inhibiting osteoclasts.
Parathyroid hormone causes both bone formation and resorption, depending on frequency of dosing. Osteoblasts are primary targets for PTH. Once activated, they secrete RANKL and IL-6, which causes osteoclast proliferation/maturation, leading to increased bone resorption. Because of this coupled remodeling process, several observations have been made:
1)intermittent PTH injections increase bone mass, 2) continous infusion lead to bone resorption, and 3) dosing should not continue past 2 yrs. Thus, intermittent parathyroid hormone is anabolic to bone and is used as a treatment of osteoporosis (forteo).
721. What dominant intracellular proteins become directly phosphorylated as a result of bone morphogenetic protein (BMP) binding to its receptors?
1. Myc
2. SMADs
3. Beta-catenin (ß-catenin)
4. Adenylate cyclase
CORRECT answer: 2
BMP proteins, which are part of the larger transforming growth factor-beta super family, bind to serine/threonine receptors on the cell surface. This binding causes phosphorylation of SMAD proteins, which in turn forms a complex that enters the nucleus and initiates the transcription of several genes involved in osteoblastic differentiation. Adenylate cyclase is
a transmembrane protein that acts intracellularly to activate the G protein pathways. Myc is a proto-oncogene that encodes for a transcription factor involved in numerous cell- activation pathways, but is not directly phosphorylated by BMP receptor.
ß-catenin is an intracellular molecule that plays a key role in the Wnt signaling pathway. This pathway is also involved in osteoblastic differentiation, but differs in target proteins within the cell.
722. A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is**
**positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness?
1. Ig antibodies at the neuromuscular (NM) junction
2. Decreased release of acetylcholine at the NM junction
3. Decrease in myelin sheath of axonal nerves with loss of NM junction
4. Absence of dystrophin with excess calcium at sarcolemma
CORRECT answer: 1
The patient has myasthenia gravis, which has its onset in middle age and causes progressive weakness because of the loss of acetylcholine receptors secondary to autoimmune antibodies at the NM junction. Rest periods allow uptake of acetylcholine and initial strength, but easy fatigability. Treatment is aimed at immunomodulation; acetyl cholinesterase inhibitors often coupled with thymectomy can control symptoms.
Decreased release of acetylcholine at the NM junction is the effect of a nondepolarizing drug or toxin botulinum. Patients with muscular dystrophy lack dystrophin that acts at the sarcolemma to regulate calcium channels, and onset of this condition occurs at a younger age. The decrease in myelin indicates Charcot-Marie-Tooth disease and is
often seen with long axon degeneration, such as in the feet and lower legs.
723. You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
1. Analysis of variance (ANOVA)
2. Regression analysis
3. Student t test
4. Mann-Whitney U test
CORRECT answer: 4
The Mann-Whitney U test is used when data are nonparametric, meaning either not normally distributed or variances are not equal among groups. Both the Student t test and ANOVA are used with parametric, normally distributed data. A regression analysis is a
statistical model that allows for control of potentially confounding variables. It is used to assess the relationship between a dependent variable and (usually) multiple independent variables.
724. Which of the following is the mechanism of action of aspirin?
1. Inhibition of vitamin K-dependent carboxylation
2. Inhibition of factor Xa through antithrombin binding
3. Binding of cyclooxygenase (COX)-1 and COX-2
4. Direct thrombin inhibition
5. Glycoprotein IIIb agonist binding
CORRECT answer: 3**
Aspirin works by the irreversible binding of cycloxygenase (COX). This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect. In addition, there is a decrease in the level of prostaglandin production due to the COX-1 binding.
Aspirin's effects and respective mechanisms of action vary with dose:
Low doses (typically 75 to 81 mg/day) are sufficient to irreversibly acetylate serine 530 of cyclooxygenase (COX)-1. This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect.
alternatives as well as the consequences of no treatment must also ensue. The explanation must be made in simple lay terms. 3) The participant must have the mental competency to comprehend the information. 4) There should be reasonable steps to ascertain that the subject understands all aspects of the discussion. 5) The subject actually makes a decision regarding participation.
708. What molecules have been shown to promote fibrosis during muscle injury?
1. Insulin growth factor 1 (IGF-1)
2. Basic fibroblast growth factor (bFGF)
3. Transforming growth factor beta 1 (TGF-ß1)
4. Bone morphogenetic protein
CORRECT answer: 3
A muscle's response to injury can be divided into 4 phases: necrosis, inflammation, repair, and fibrosis. Necrosis involves the degeneration of the muscle fibrils and death. The inflammatory cells then phagocytose the debris and secrete cytokines that promote vascularity. Muscle regeneration does not occur until phagocytic cells remove the debris. Consequently, anti- inflammatory drugs may have negative effects on muscle healing by inhibiting macrophage-induced phagocytosis. Muscle fibrosis occurs at the same time as muscle regeneration and has been shown to involve TGF-ß1. IGF-1 and bFGF are important trophic factors in muscle regeneration. Bone morphogenetic protein has several functions including bone and cartilage regeneration.
709. A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
1. case series.
2. case-control study.
3. cohort study.
4. randomized clinical trial.
CORRECT answer: 1
The type of study design in which a series of cases is presented with outcomes (without a control population or comparison group) is known as a case series. This type of study design, although frequently seen in orthopaedic literature, provides the lowest level of evidence. There is no control group and the population is usually poorly defined. This type of study can be helpful as a starting point for further analysis. A randomized trial provides the highest level of evidence in medical research, featuring a comparison group and
randomized (and usually blinded) placement of subjects into study groups. In case-control studies, cases are compared to a control group. The control group has not
been randomized, but may be a naturally occurring group of subjects who
have not had the same exposure or intervention as the case group. A cohort study can be retrospective or prospective and usually looks at a large group of people over time to assess exposures and incidence of disease.
710. What effect does intermittent administration of parathyroid hormone have on bone?
1. Anabolic
2. Catabolic
3. No effect
4. Decreased quantity
5. Decreased quality
CORRECT answer: 1
Treatment of osteoporosis centers on increasing bone mass by direct anabolic effect and/or inhibiting osteoclastic absorption. Bisphosphonates, selective estrogen receptor modulators, and calcitonin act to decrease bone resorption by inhibiting osteoclasts.
Parathyroid hormone causes both bone formation and resorption, depending on frequency of dosing. Osteoblasts are primary targets for PTH. Once activated, they secrete RANKL and IL-6, which causes osteoclast proliferation/maturation, leading to increased bone resorption. Because of this coupled remodeling process, several observations have been made:
1)intermittent PTH injections increase bone mass, 2) continous infusion lead to bone resorption, and 3) dosing should not continue past 2 yrs. Thus, intermittent parathyroid hormone is anabolic to bone and is used as a treatment of osteoporosis (forteo).
721. What dominant intracellular proteins become directly phosphorylated as a result of bone morphogenetic protein (BMP) binding to its receptors?
1. Myc
2. SMADs
3. Beta-catenin (ß-catenin)
4. Adenylate cyclase
CORRECT answer: 2
BMP proteins, which are part of the larger transforming growth factor-beta super family, bind to serine/threonine receptors on the cell surface. This binding causes phosphorylation of SMAD proteins, which in turn forms a complex that enters the nucleus and initiates the transcription of several genes involved in osteoblastic differentiation. Adenylate cyclase is
a transmembrane protein that acts intracellularly to activate the G protein pathways. Myc is a proto-oncogene that encodes for a transcription factor involved in numerous cell- activation pathways, but is not directly phosphorylated by BMP receptor.
ß-catenin is an intracellular molecule that plays a key role in the Wnt signaling pathway. This pathway is also involved in osteoblastic differentiation, but differs in target proteins within the cell.
722. A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is**
**positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness?
1. Ig antibodies at the neuromuscular (NM) junction
2. Decreased release of acetylcholine at the NM junction
3. Decrease in myelin sheath of axonal nerves with loss of NM junction
4. Absence of dystrophin with excess calcium at sarcolemma
CORRECT answer: 1
The patient has myasthenia gravis, which has its onset in middle age and causes progressive weakness because of the loss of acetylcholine receptors secondary to autoimmune antibodies at the NM junction. Rest periods allow uptake of acetylcholine and initial strength, but easy fatigability. Treatment is aimed at immunomodulation; acetyl cholinesterase inhibitors often coupled with thymectomy can control symptoms.
Decreased release of acetylcholine at the NM junction is the effect of a nondepolarizing drug or toxin botulinum. Patients with muscular dystrophy lack dystrophin that acts at the sarcolemma to regulate calcium channels, and onset of this condition occurs at a younger age. The decrease in myelin indicates Charcot-Marie-Tooth disease and is
often seen with long axon degeneration, such as in the feet and lower legs.
723. You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
1. Analysis of variance (ANOVA)
2. Regression analysis
3. Student t test
4. Mann-Whitney U test
CORRECT answer: 4
The Mann-Whitney U test is used when data are nonparametric, meaning either not normally distributed or variances are not equal among groups. Both the Student t test and ANOVA are used with parametric, normally distributed data. A regression analysis is a
statistical model that allows for control of potentially confounding variables. It is used to assess the relationship between a dependent variable and (usually) multiple independent variables.
724. Which of the following is the mechanism of action of aspirin?
1. Inhibition of vitamin K-dependent carboxylation
2. Inhibition of factor Xa through antithrombin binding
3. Binding of cyclooxygenase (COX)-1 and COX-2
4. Direct thrombin inhibition
5. Glycoprotein IIIb agonist binding
CORRECT answer: 3**
Aspirin works by the irreversible binding of cycloxygenase (COX). This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect. In addition, there is a decrease in the level of prostaglandin production due to the COX-1 binding.
Aspirin's effects and respective mechanisms of action vary with dose:
Low doses (typically 75 to 81 mg/day) are sufficient to irreversibly acetylate serine 530 of cyclooxygenase (COX)-1. This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect.
Question 27High Yield
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar
resurfacing is associated with
resurfacing is associated with
Explanation
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate
in patients with anterior knee pain.
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate
in patients with anterior knee pain.
Question 28High Yield
A 32-year-old soccer player presents with severe right ankle pain and inability to bear weight after sustaining a slide-tackle injury during a game. Radiographs are shown in Figures A and B. Given the nature of his injury, he is taken for surgical reduction and fixation. Following medial malleolar fixation, the syndesmosis is addressed. All of the following are true regarding the most appropriate intraoperative technique for anatomic syndesmotic reduction EXCEPT:




Explanation
When placing a clamp across the syndesmosis to facilitate reduction, the lateral tine should be placed directly on the lateral malleolar ridge. Placing the lateral tine either more anteriorly or posteriorly has been shown to result in sagittal malreduction from fibular translation.
Syndesmotic reduction has proven to be technically challenging, with reportedly greater than 50% of cases resulting in malreduction. Provisional reduction is most often attained via a pointed reduction clamp. Placement of the lateral tine is outlined above. The medial tine should be placed at the anatomic midportion of the medial tibia, which can be confirmed
fluoroscopically as the anterior third of the tibia on a true lateral view of the ankle. It is important to maintain the axis of the clamp parallel to the joint line and to the anatomic syndesmotic angle. The clamp should furthermore be maintained 1-2cm proximal to the mortise, at the level of the incisura, to avoid deformation or undue translation of the fibula. Lastly, over-compression of the syndesmosis has been demonstrated, though the clinical implications remain controversial.
Putnam et al. performed a radiographic analysis of the ideal orientation for placement of a syndesmotic reduction clamp. Based on the CT scans of uninjured adult ankles, the authors showed that the trans-syndesmotic axis could be most reliably paralleled by a reduction clamp by placing the lateral tine on the lateral malleolar ridge and the medial tine radiographically within the anterior third of the tibia, anatomically half-way between the anterior and posterior cortices. They further specified that the ideal location was within the central one-third of the distance from the anterior tibial cortex to the anterior fibular cortex.
Cosgrove et al. prospectively evaluated the effect of medial clamp tine positioning on the incidence of syndesmotic malreduction. The authors found that malreduction most often resulted from deviation of the clamp axis from the syndesmotic axis. With the clamp at 1-2cm proximal to the mortise and the lateral tine on the lateral malleolar ridge, the ideal position of the medial tine was within the anterior third of the tibia. The rate of sagittal malreduction increased substantially with increasingly posterior placement of the medial tine. The medial clamp position did not affect coronal plane malreduction.
Gardner et al. review the technical considerations in reduction and fixation of syndesmotic injuries. The authors stress careful positioning of the reduction clamp, advocating that the clamp should be placed from the lateral malleolar ridge to the center of the anteroposterior width of the medial tibia.
Additionally, they note that placement too proximal or distal results in coronal plane deformity of the fibula, and that over-compression of the syndesmosis is certainly possible.
Figure A is the AP radiograph of the left ankle demonstrating a displaced medial malleolar fracture and syndesmotic widening. Figure B is the lateral radiograph of the ipsilateral knee showing an associated proximal fibular fracture.
Illustration A shows the syndesmotic angle and anatomic trans-syndesmotic axis as compared to the AP and lateral fluoroscopic axes. Illustration B shows the ideal positioning of the medial tine within the anterior third of the tibia on a true lateral view of the ankle.
Incorrect answers:
Answer 1: The axis of the reduction camp should parallel that of the trans-syndesmotic axis.
Answer 3: The medial tine is ideally placed within the anterior third of the tibia, and moreover within the central third of the distance between the anterior tibial and fibular cortices on a true lateral view of the ankle.
Answer 4: The clamp is ideally placed 1-2cm proximal to the tibial plafond at the level of the incisura to avoid deformation of the fibula, which has been associated with placement too proximal or distal.
Answer 5: Over-compression of the syndesmosis has been demonstrated radiographically, though the effect on the range of motion and clinical outcomes remains unclear.
Syndesmotic reduction has proven to be technically challenging, with reportedly greater than 50% of cases resulting in malreduction. Provisional reduction is most often attained via a pointed reduction clamp. Placement of the lateral tine is outlined above. The medial tine should be placed at the anatomic midportion of the medial tibia, which can be confirmed
fluoroscopically as the anterior third of the tibia on a true lateral view of the ankle. It is important to maintain the axis of the clamp parallel to the joint line and to the anatomic syndesmotic angle. The clamp should furthermore be maintained 1-2cm proximal to the mortise, at the level of the incisura, to avoid deformation or undue translation of the fibula. Lastly, over-compression of the syndesmosis has been demonstrated, though the clinical implications remain controversial.
Putnam et al. performed a radiographic analysis of the ideal orientation for placement of a syndesmotic reduction clamp. Based on the CT scans of uninjured adult ankles, the authors showed that the trans-syndesmotic axis could be most reliably paralleled by a reduction clamp by placing the lateral tine on the lateral malleolar ridge and the medial tine radiographically within the anterior third of the tibia, anatomically half-way between the anterior and posterior cortices. They further specified that the ideal location was within the central one-third of the distance from the anterior tibial cortex to the anterior fibular cortex.
Cosgrove et al. prospectively evaluated the effect of medial clamp tine positioning on the incidence of syndesmotic malreduction. The authors found that malreduction most often resulted from deviation of the clamp axis from the syndesmotic axis. With the clamp at 1-2cm proximal to the mortise and the lateral tine on the lateral malleolar ridge, the ideal position of the medial tine was within the anterior third of the tibia. The rate of sagittal malreduction increased substantially with increasingly posterior placement of the medial tine. The medial clamp position did not affect coronal plane malreduction.
Gardner et al. review the technical considerations in reduction and fixation of syndesmotic injuries. The authors stress careful positioning of the reduction clamp, advocating that the clamp should be placed from the lateral malleolar ridge to the center of the anteroposterior width of the medial tibia.
Additionally, they note that placement too proximal or distal results in coronal plane deformity of the fibula, and that over-compression of the syndesmosis is certainly possible.
Figure A is the AP radiograph of the left ankle demonstrating a displaced medial malleolar fracture and syndesmotic widening. Figure B is the lateral radiograph of the ipsilateral knee showing an associated proximal fibular fracture.
Illustration A shows the syndesmotic angle and anatomic trans-syndesmotic axis as compared to the AP and lateral fluoroscopic axes. Illustration B shows the ideal positioning of the medial tine within the anterior third of the tibia on a true lateral view of the ankle.
Incorrect answers:
Answer 1: The axis of the reduction camp should parallel that of the trans-syndesmotic axis.
Answer 3: The medial tine is ideally placed within the anterior third of the tibia, and moreover within the central third of the distance between the anterior tibial and fibular cortices on a true lateral view of the ankle.
Answer 4: The clamp is ideally placed 1-2cm proximal to the tibial plafond at the level of the incisura to avoid deformation of the fibula, which has been associated with placement too proximal or distal.
Answer 5: Over-compression of the syndesmosis has been demonstrated radiographically, though the effect on the range of motion and clinical outcomes remains unclear.
Question 29High Yield
Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?
Explanation
Minimally displaced fractures of the proximal humerus have a good outcome if physical therapy is initiated within 2 weeks of the injury. Results are not affected by age, open reduction and internal fixation, or involvement of the greater tuberosity. Immobilization for longer than 3 weeks will often result in stiffness.
REFERENCES: Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Hodgson SA, Mawson SJ, Stanley D: Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 2003;85:419-422.
REFERENCES: Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Hodgson SA, Mawson SJ, Stanley D: Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 2003;85:419-422.
Question 30High Yield
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup?
---
---
---
---


Explanation
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding _scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis._
Question 31High Yield
Figure 35 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?

Explanation
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-a, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-ß, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
RECOMMENDED READINGS
Kim HT, Yoon ST, Jarrett C. Articular cartilage and intervertebral disk. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:23-33.
[Hoyland JA, Le Maitre C, Freemont AJ. Investigation of the role of IL-1 and TNF in matrix degradation in the intervertebral disc. Rheumatology (Oxford). 2008 Jun;47(6):809-14. doi: 10.1093/rheumatology/ken056. Epub 2008 Apr 8. PubMed PMID: 18397957. ](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[ ](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18397957)
[Gruber HE, Ingram JA, Hanley EN Jr. Immunolocalization of MMP-19 in the human intervertebral disc: implications for disc aging and degeneration. Biotech Histochem. 2005 May-Aug;80(3-4):157-62. PubMed PMID: 16298901. ](http://www.ncbi.nlm.nih.gov/pubmed/16298901)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16298901)
RECOMMENDED READINGS
Kim HT, Yoon ST, Jarrett C. Articular cartilage and intervertebral disk. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:23-33.
[Hoyland JA, Le Maitre C, Freemont AJ. Investigation of the role of IL-1 and TNF in matrix degradation in the intervertebral disc. Rheumatology (Oxford). 2008 Jun;47(6):809-14. doi: 10.1093/rheumatology/ken056. Epub 2008 Apr 8. PubMed PMID: 18397957. ](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[ ](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18397957)
[Gruber HE, Ingram JA, Hanley EN Jr. Immunolocalization of MMP-19 in the human intervertebral disc: implications for disc aging and degeneration. Biotech Histochem. 2005 May-Aug;80(3-4):157-62. PubMed PMID: 16298901. ](http://www.ncbi.nlm.nih.gov/pubmed/16298901)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16298901)
Question 32High Yield
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?
Explanation
Discoid menisci are rare causes of lateral knee pain in children. Various etiologies have been proposed, including failure of central absorption of the developing meniscus and hereditary transmission. Patients with discoid menisci have pain, clicking, and locking with a loss of active extension on range-of-motion testing. Classification of discoid menisci according to the Watanabe classification include complete, incomplete, and Wrisberg ligament type. The Wrisberg variant contains an abnormal posterior meniscal attachment. MRI is the diagnostic tool of choice, revealing a thick, flat meniscus generally seen in three consecutive MRI images. Symptomatic knees are often associated with a meniscal tear or degeneration and are managed with arthroscopic partial excision to a more normal shape (saucerization).
REFERENCES: Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Bellier G, Dupont JY, Larrain M, et al: Lateral discoid menisci in children. Arthroscopy 1989;5:52-56.
REFERENCES: Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Bellier G, Dupont JY, Larrain M, et al: Lateral discoid menisci in children. Arthroscopy 1989;5:52-56.
Question 33High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
What represents the best indication for surgical management of the humeral shaft fracture in this patient?
---
---
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
What represents the best indication for surgical management of the humeral shaft fracture in this patient?
---
---


Explanation
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 34High Yield
In the treatment of all magnitudes of bunionette deformities, what is the most common complication associated with lateral condylectomy of the fifth metatarsal head?
Explanation
When a lateral condylectomy alone is performed for all bunionette deformities, a high recurrence rate is expected. Lateral condylectomy should be used alone when the primary deformity is an enlarged lateral condyle of the fifth metatarsal head. In cases with significant divergence of the fifth metatarsal shaft in relationship to the fourth metatarsal shaft or with lateral bowing of the distal fifth metatarsal shaft, the lateral fifth metatarsal prominence will not be effectively reduced and recurrent symptoms and deformity are expected. Transfer metatarsalgia and/or dislocation of the metatarsophalangeal joint can infrequently occur with excessive metatarsal head excision. Arthrosis of the metatarsophalangeal joint has not been frequently reported.
REFERENCES: Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
Kelikian H: Deformities of the lesser toe, in Kelikian H (ed): Hallux Valgus, Allied Deformities of the Forefoot and Metatarsalgia. Philadelphia, PA, WB Saunders, 1965, pp 327-330.
Kitaoka HB, Holiday AD Jr: Lateral condylar resection for bunionette. Clin Orthop 1992;278:183-192.
REFERENCES: Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
Kelikian H: Deformities of the lesser toe, in Kelikian H (ed): Hallux Valgus, Allied Deformities of the Forefoot and Metatarsalgia. Philadelphia, PA, WB Saunders, 1965, pp 327-330.
Kitaoka HB, Holiday AD Jr: Lateral condylar resection for bunionette. Clin Orthop 1992;278:183-192.
Question 35High Yield
A 42-year-old construction worker sustains a crush injury to the hand at a job site. He has immediate pain and significant swelling, and is taken to the local emergency department for evaluation. Radiographs do not demonstrate any fracture or dislocation. On exam,
he experiences severe pain with passive motion at the metacarpal phalangeal joints and when the wrist is flexed and extended.
Otherwise he has intact sensation and appropriate capillary refill. What is the next best step in diagnosis or treatment?
he experiences severe pain with passive motion at the metacarpal phalangeal joints and when the wrist is flexed and extended.
Otherwise he has intact sensation and appropriate capillary refill. What is the next best step in diagnosis or treatment?

Explanation
This patient presents with compartment syndrome of the hand. A history and clinical exam are the best tools to identify the diagnosis, and the treatment consists of emergent fasciotomies.
Compartment syndrome of the hand may be secondary to trauma, burn, IV drug use, extravasation of IV fluids, or major limb revascularization. The diagnosis is usually made with pain out of proportion to exam, particularly with passive stretch of the digits. It is possible to have compartment syndrome without neurovascular changes (paresthesia, pallor, pulselessness), particularly earlier in the presentation. Compartment measurements may be obtained and are considered diagnostic with an absolute value greater than 30mmHg or when the compartment pressure is within 30mmHg of the patient's diastolic blood pressure. However pressure testing is not necessary in most cases, but may be particularly important in the patient who is obtunded, intubated, or who had a block, as the physical exam will be confounded. There are ten hand compartments: hypothenar, thenar, adductor pollicis, four dorsal interosseous, and three palmar interosseous; and emergent surgical release of all ten compartments is indicated.
Codding et al. comprehensively reviewed hand compartment syndrome. The authors identify the history and physical exam as the most critical aspect of the diagnosis. More specifically, they noted that pain with passive stretch of the MCPJ is the most sensitive clinical sign on physical exam. The authors conclude the short comings of the research on hand compartment syndrome, but note the potential morbidity of a missed diagnosis is so great that the threshold for surgical intervention should be very low.
Lipschitz et al. reviewed the measurement of compartment pressures in the hand. The authors discussed technical pearls including leveling the monitor at the level of the heart, using local analgesia on the skin only, inserting the needle perpendicular to the skin, and measuring all 10 hand compartments.
They noted that any measurement greater than 30mmHg or within 30mmHg of the diastolic blood pressure may be considered diagnostic.
Illustration A shows the standard incisions utilized to release all ten hand compartments. Incisions are generally placed directly overlaying the thenar musculature, hypothenar musculature, the carpal tunnel, and dorsally over the metacarpals. The radial and ulnar border of each metacarpal are incised through the dorsal incisions to release the interossei compartments.
Incorrect Answers:
Answer 1: Advanced imaging is not necessary in the diagnosis of compartment syndrome. It may delay treatment and should generally be avoided if compartment syndrome is suspected based on history and clinical exam.
Answer 2: Arterial Doppler is not necessary. Neurovascular changes occur very late in the process, and this patient has good perfusion on exam.
Answer 3: Admission overnight would delay emergent treatment and result in irreversible muscle and neurovascular damage.
Answer 5: The patient has clinical compartment syndrome. Pain control will mask the problem and delay emergent surgery.
Compartment syndrome of the hand may be secondary to trauma, burn, IV drug use, extravasation of IV fluids, or major limb revascularization. The diagnosis is usually made with pain out of proportion to exam, particularly with passive stretch of the digits. It is possible to have compartment syndrome without neurovascular changes (paresthesia, pallor, pulselessness), particularly earlier in the presentation. Compartment measurements may be obtained and are considered diagnostic with an absolute value greater than 30mmHg or when the compartment pressure is within 30mmHg of the patient's diastolic blood pressure. However pressure testing is not necessary in most cases, but may be particularly important in the patient who is obtunded, intubated, or who had a block, as the physical exam will be confounded. There are ten hand compartments: hypothenar, thenar, adductor pollicis, four dorsal interosseous, and three palmar interosseous; and emergent surgical release of all ten compartments is indicated.
Codding et al. comprehensively reviewed hand compartment syndrome. The authors identify the history and physical exam as the most critical aspect of the diagnosis. More specifically, they noted that pain with passive stretch of the MCPJ is the most sensitive clinical sign on physical exam. The authors conclude the short comings of the research on hand compartment syndrome, but note the potential morbidity of a missed diagnosis is so great that the threshold for surgical intervention should be very low.
Lipschitz et al. reviewed the measurement of compartment pressures in the hand. The authors discussed technical pearls including leveling the monitor at the level of the heart, using local analgesia on the skin only, inserting the needle perpendicular to the skin, and measuring all 10 hand compartments.
They noted that any measurement greater than 30mmHg or within 30mmHg of the diastolic blood pressure may be considered diagnostic.
Illustration A shows the standard incisions utilized to release all ten hand compartments. Incisions are generally placed directly overlaying the thenar musculature, hypothenar musculature, the carpal tunnel, and dorsally over the metacarpals. The radial and ulnar border of each metacarpal are incised through the dorsal incisions to release the interossei compartments.
Incorrect Answers:
Answer 1: Advanced imaging is not necessary in the diagnosis of compartment syndrome. It may delay treatment and should generally be avoided if compartment syndrome is suspected based on history and clinical exam.
Answer 2: Arterial Doppler is not necessary. Neurovascular changes occur very late in the process, and this patient has good perfusion on exam.
Answer 3: Admission overnight would delay emergent treatment and result in irreversible muscle and neurovascular damage.
Answer 5: The patient has clinical compartment syndrome. Pain control will mask the problem and delay emergent surgery.
Question 36High Yield
Haversian bone is composed of vascular channels surrounded circumferentially by lamellar bone. Which of the following terms is used to describe the unit of bone composed of a neurovascular channel surrounded by a cell-permeated layer of bone matrix:
Explanation
The osteon is a unique arrangement of bone cells and matrix surrounding a blood vessel. The osteon is an irregular branching, anastomosing cylinder composed of a centrally placed neurovascular canal surrounded by cell-permeated layers of bone matrix.
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
Question 37High Yield
A 40-year-old male sustains a fall from a height. He sustains the isolated injury shown in the radiograph and CT images seen in Figures A through C. Surgery is planned. Which of the following constructs is the most appropriate definitive fixation for this injury?


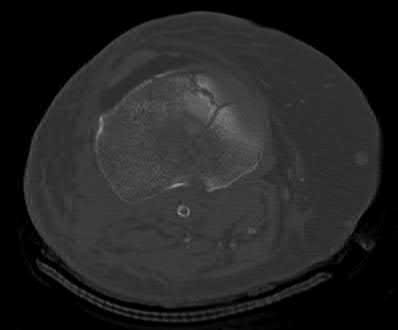
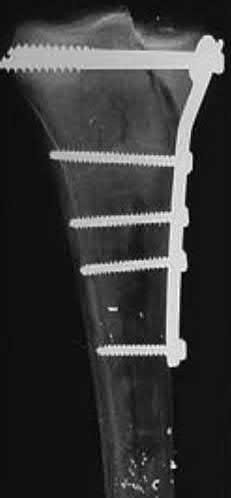
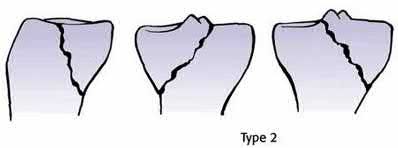
Explanation
This patient has a medial tibial plateau fracture. Medial buttress plating (MBP) is indicated.
Medial tibial plateau fractures (Schatzker IV, Hohl and Moore II) may represent fracture dislocations of the knee. Neurovascular injuries must be excluded. In these instances, the medial fragment represents the stable fragment, and the rest of the tibia is the fractured fragment, with the entire leg acting as the lever arm.
Berkson et al. reviewed high energy tibial plateau fractures. Medial fractures may be treated with a medial plate or external fixation. Open reduction may be necessary because of fracture line obliquity and propensity of the medial plateau to shorten and rotate in the sagittal plane. Meniscal injuries should be repaired and avulsed cruciates fixed early. Collateral ligaments should be reconstructed after obtaining bone healing and range of motion.
Ratcliff et al. compared the stability of lateral locked plates and medial buttress plates in a cadaver model. They found that the medial buttress plate had greater fixation strength/failure force (4136N) compared with the lateral locking plate (2895N), although maximum cyclic displacement and residual displacement results were not different. They concluded that for vertically
orientated medial tibial plateau fractures, medial buttress plates were more stable.
Figure A is a radiograph showing a medial tibial plateau fracture extending across the tibial eminence. This is also classified as a Hohl and Moore Type II fracture. Figures B and C are coronal and axial CT scan images confirming the medial tibial plateau fracture and excluding a bicondylar fracture. Illustration A shows a medial tibial plateau fracture fixed with a medial buttress plate (cadaveric model with fibula removed). Illustration B shows the Hohl and Moore Type II fracture involving the entire condyle.
Incorrect Answers:
Answer 1: Lateral locked plating is biomechanically inferior to medial buttress plating for medial tibial plateau fractures (see reference above).
Answer 2: Medial bridge plating is appropriate for segmental or comminuted fractures
Answer 4: Lag screw fixation alone is contraindicated because of the long lever arm of the leg may lead to implant failure.
Answer 5: Temporary spanning external fixation may be appropriate for extensive comminution or soft tissue injury/swelling. Definitive external fixation (non-joint spanning) with olive wires, monolateral half-pins or both (hybrid) are possible options but less preferred as wires <14mm from the articular surface risk joint capsule penetration and septic arthritis.
Medial tibial plateau fractures (Schatzker IV, Hohl and Moore II) may represent fracture dislocations of the knee. Neurovascular injuries must be excluded. In these instances, the medial fragment represents the stable fragment, and the rest of the tibia is the fractured fragment, with the entire leg acting as the lever arm.
Berkson et al. reviewed high energy tibial plateau fractures. Medial fractures may be treated with a medial plate or external fixation. Open reduction may be necessary because of fracture line obliquity and propensity of the medial plateau to shorten and rotate in the sagittal plane. Meniscal injuries should be repaired and avulsed cruciates fixed early. Collateral ligaments should be reconstructed after obtaining bone healing and range of motion.
Ratcliff et al. compared the stability of lateral locked plates and medial buttress plates in a cadaver model. They found that the medial buttress plate had greater fixation strength/failure force (4136N) compared with the lateral locking plate (2895N), although maximum cyclic displacement and residual displacement results were not different. They concluded that for vertically
orientated medial tibial plateau fractures, medial buttress plates were more stable.
Figure A is a radiograph showing a medial tibial plateau fracture extending across the tibial eminence. This is also classified as a Hohl and Moore Type II fracture. Figures B and C are coronal and axial CT scan images confirming the medial tibial plateau fracture and excluding a bicondylar fracture. Illustration A shows a medial tibial plateau fracture fixed with a medial buttress plate (cadaveric model with fibula removed). Illustration B shows the Hohl and Moore Type II fracture involving the entire condyle.
Incorrect Answers:
Answer 1: Lateral locked plating is biomechanically inferior to medial buttress plating for medial tibial plateau fractures (see reference above).
Answer 2: Medial bridge plating is appropriate for segmental or comminuted fractures
Answer 4: Lag screw fixation alone is contraindicated because of the long lever arm of the leg may lead to implant failure.
Answer 5: Temporary spanning external fixation may be appropriate for extensive comminution or soft tissue injury/swelling. Definitive external fixation (non-joint spanning) with olive wires, monolateral half-pins or both (hybrid) are possible options but less preferred as wires <14mm from the articular surface risk joint capsule penetration and septic arthritis.
Question 38High Yield
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
The histologic features of multiple myeloma are distinctive for this lesion. The plasma cells are round or oval and have an eccentric nucleus and prominent nucleolus. These characteristics and a clear area next to the eccentric nucleus representing the prominent Golgi center are pathognomonic for plasma cells. Lymphoma is in the differential diagnosis; the most frequent types that occur in bone are large cell or mixed small and large cell types. The histologic appearance of the specimen is not consistent with the other choices.
REFERENCE: Dorfman HD, Bodgan C: Immunohematopoietic tumors, in Dorfman HD, Bogdan C (eds): Bone Tumors. St Louis, MO, Mosby, 1998, Chapter 12.
REFERENCE: Dorfman HD, Bodgan C: Immunohematopoietic tumors, in Dorfman HD, Bogdan C (eds): Bone Tumors. St Louis, MO, Mosby, 1998, Chapter 12.
Question 39High Yield
A 43-year-old diabetic patient has had an ulcer on the plantar aspect of her foot for 9 months. She has no systemic symptoms. There is minimal drainage from the ulcer, and she has no pain in the foot. Initial management of this patient must include:
Explanation
This neuropathic ulcer is stable. There is minimal drainage and no clinical findings to suggest an active infection. C ulture of the ulcer yields multiple nonpathogenic organisms and antibiotic therapy is not indicated. Treatment is initiated with either a total contact cast or a total contact walker boot.
Question 40High Yield
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal- on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?

Explanation
DISCUSSION: This young patient has osteonecrosis of the femoral head with a large area of collapse.
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
1. ### distal femoral varus osteotomy.
2. ### osteoarticular transplant to the lateral femoral condyle.
3. ### unicondylar arthroplasty.
4. ### high tibial osteotomy.
5. ### Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
Figure 25a Figure 25b Figure 25c
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
1. ### distal femoral varus osteotomy.
2. ### osteoarticular transplant to the lateral femoral condyle.
3. ### unicondylar arthroplasty.
4. ### high tibial osteotomy.
5. ### Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
Figure 25a Figure 25b Figure 25c
Question 41High Yield
A 65-year-old woman sustains a hip fracture following a minor fall. Which of the following treatments should be considered:
Explanation
This patient has a new fracture. Because the fracture occurred following minor trauma, the physician should assume that this patient has an insufficiency fracture related to her osteoporosis.
Patients who sustain an osteoporotic hip fracture should be treated with antiresorptive therapy to lower the risk of a subsequent hip or vertebral fracture. A recent randomized trial showed the following:
A large prospective, randomized study showed a reduction in vertebral and nonvertebral fractures when patients were treated with intravenous (IV) zoledronic acid within 90 days of a hip fracture, followed up with annual treatment.
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months
C orrect Answer: Antiresorptive therapy
Patients who sustain an osteoporotic hip fracture should be treated with antiresorptive therapy to lower the risk of a subsequent hip or vertebral fracture. A recent randomized trial showed the following:
A large prospective, randomized study showed a reduction in vertebral and nonvertebral fractures when patients were treated with intravenous (IV) zoledronic acid within 90 days of a hip fracture, followed up with annual treatment.
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months
C orrect Answer: Antiresorptive therapy
Question 42High Yield
Marjolinâs ulcers are risk factors for which of the following tumors:
Explanation
Marjolinâs ulcers are malignant degenerations in chronic skin ulcers, sinuses, and burn scars and are risk factors for squamous cell carcinoma. Any patient with chronic, nonhealing ulcers should undergo biopsy for malignant degeneration. Basal cell carcinoma, malignant melanoma, synovial sarcoma, and osteosarcoma are not commonly associated with Marjolin's ulcer.
Question 43High Yield
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Based on the pathology noted, which finding may be found on plain knee radiographs?





Explanation
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment _of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair._
Question 44High Yield
A lateral transpsoas interbody fusion with percutaneous pedicle screws was performed. When compared with those undergoing open laminectomy and fusion, this patient can expect
Explanation
- higher risk for postoperative thigh pain.
Question 45High Yield
Slide 1 Slide 2 Slide 3
A patient with diabetes and severe peripheral neuropathy has been treated for a C harcot ankle deformity for 9 months (Slide 1, Slide 2, and Slide 3). An ankle foot orthosis has been used for 4 months. No skin breakdown occurred in the brace. Swelling is present but has decreased over the past month. Ankle range of motion is limited, and crepitus is present upon examination of the ankle. Which surgical procedure is most consistent with the future treatment of this patient:
A patient with diabetes and severe peripheral neuropathy has been treated for a C harcot ankle deformity for 9 months (Slide 1, Slide 2, and Slide 3). An ankle foot orthosis has been used for 4 months. No skin breakdown occurred in the brace. Swelling is present but has decreased over the past month. Ankle range of motion is limited, and crepitus is present upon examination of the ankle. Which surgical procedure is most consistent with the future treatment of this patient:
Explanation
The indication for surgery is intractable deformity, which is refractory to all forms of bracing. By refractory, one implies that skin breakdown or imminent infection is present. If surgery were performed, then it would consist of a tibiotalocalcaneal arthrodesis. There are no indications for this surgery in this patient. Once the neuropathic process has reached a stable point, a deformity is not likely to progress.
Question 46High Yield
What is the most appropriate diagnosis?
Explanation
- Charcot foot
Question 47High Yield
Which of the following most accurately approximates the estimated risk of a musculoskeletal allograft containing the human immunodeficiency virus (HIV) despite adequate screening?
Explanation
6,000,000
DISCUSSION: The calculated risk of a musculoskeletal allograft containing HIV despite adequate screening has been estimated to be approximately 1 in 1.6 million. This estimate is based on the risk of HIV in the population, projected population estimates, and current methods of donor screening.
REFERENCES: McAllister D, Joyce M, Mann B, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;2148-2158.
Buck B, Malinin T: Human bone and tissue allografts: Preparation and safety. Clin Orthop Relat Res 1994;303:8 -
17.
Buck B, Malinin T, Brown M: Bone transplantation and human immunodeficiency virus: An estimate of risk of acquired immunodeficiency syndrome (AIDS). Clin Orthop Relat Res 1989;240:129-136.
_A i;___
Figure 92
6,000,000
DISCUSSION: The calculated risk of a musculoskeletal allograft containing HIV despite adequate screening has been estimated to be approximately 1 in 1.6 million. This estimate is based on the risk of HIV in the population, projected population estimates, and current methods of donor screening.
REFERENCES: McAllister D, Joyce M, Mann B, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;2148-2158.
Buck B, Malinin T: Human bone and tissue allografts: Preparation and safety. Clin Orthop Relat Res 1994;303:8 -
17.
Buck B, Malinin T, Brown M: Bone transplantation and human immunodeficiency virus: An estimate of risk of acquired immunodeficiency syndrome (AIDS). Clin Orthop Relat Res 1989;240:129-136.
_A i;___
Figure 92
Question 48High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What type of screws should be available for stabilization of this injury?
---
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What type of screws should be available for stabilization of this injury?
---

Explanation
Coronal shear fractures of the distal end of the humerus are rare. Failure to recognize the fracture pattern can lead to poor patient outcomes secondary to poor surgical decision making. The double arc sign is considered a pathognomonic finding on the lateral elbow radiograph seen in Figure 2. This is created by the subchondral bone of the capitellum and lateral trochlear ridge. Excessive internal rotation of the fracture fragment or a subpar lateral radiograph can make recognition of this sign difficult.
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral
ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral
ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 49High Yield
Slide 1
A 56-year-old patient sustained an ankle fracture 3 years ago that was treated with closed reduction and cast immobilization. Since the injury, she has experienced pain upon ambulation and ankle stiffness. On examination, the range of motion of the ankle is 5° of dorsiflexion and 30° of plantarflexion. C repitus with motion is not present, but the patient does experience severe pain. A radiograph is presented (Slide). The recommended procedure to alleviate the patientâs pain and improve function is:
A 56-year-old patient sustained an ankle fracture 3 years ago that was treated with closed reduction and cast immobilization. Since the injury, she has experienced pain upon ambulation and ankle stiffness. On examination, the range of motion of the ankle is 5° of dorsiflexion and 30° of plantarflexion. C repitus with motion is not present, but the patient does experience severe pain. A radiograph is presented (Slide). The recommended procedure to alleviate the patientâs pain and improve function is:
Explanation
The arthritis in this joint is not severe, but there is joint malalignment associated with a short and externally rotated fibula. Joint malalignment is correctable with a lengthening and rotational (internal) osteotomy of the fibula with bone graft. Joint debridement, either open or arthroscopic, is not effective in the management of posttraumatic ankle arthritis. Arthrodesis and arthroplasty are not necessary at this stage.
Question 50High Yield
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel’s sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
Painful incisional neuromas after bunion surgery frequently involve the dorsomedial cutaneous branch of the superficial peroneal nerve. This is the medial branch of the superficial peroneal nerve that terminates as the dorsomedial cutaneous nerve to the hallux. Branches of the deep peroneal nerve to this area are rare, and no branches to this area exist from the sural nerve. The saphenous nerve branches are generally more proximal, and the medial plantar nerve lies plantarly.
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon