Masterclass in Patella Fractures: Surgical Techniques & Extensor Mechanism Repair
Key Takeaway
Patella fractures account for 1% of all skeletal injuries, threatening the continuity of the knee's extensor mechanism and patellofemoral congruity. Management hinges on restoring active extension and articular alignment. This guide details the biomechanics, clinical evaluation, and step-by-step surgical interventions—including modified tension band wiring and cannulated screw constructs—required to achieve stable fixation, permit early mobilization, and optimize functional outcomes in complex patellar trauma.
INTRODUCTION AND EPIDEMIOLOGY
Fractures of the patella constitute approximately 1% of all skeletal injuries. As the largest sesamoid bone in the human body, the patella serves a critical biomechanical function: it increases the moment arm of the quadriceps muscle, thereby enhancing the mechanical advantage of the extensor mechanism by up to 30%. The most significant clinical consequences of a patellar fracture are the loss of continuity of the extensor mechanism and the potential for severe incongruity of the patellofemoral articulation, which can lead to rapid-onset post-traumatic arthrosis.
Historically, the functional importance of the patella was debated. In 1937, Brooke proposed that the patella was not a functional organ and advocated for its routine excision following trauma. However, subsequent seminal biomechanical studies by Haxton (1945) and Kaufer definitively established the patella's indispensable role in knee kinematics, proving that patellectomy significantly decreases quadriceps strength and alters tibiofemoral joint reaction forces. Today, the preservation of the patella and the anatomic restoration of its articular surface remain the gold standards of care.
MECHANISM OF INJURY AND PATHOANATOMY
Patellar fractures result from direct trauma, indirect trauma, or a combination of both forces.
- Direct Trauma: The anterior, subcutaneous location of the patella makes it highly vulnerable to direct impact. Common scenarios include the knee striking the dashboard during a motor vehicle collision or a direct fall onto the flexed knee. These injuries typically produce comminuted or displaced fracture patterns and are frequently associated with severe chondral injuries to the patella or the opposing trochlea of the distal femur.
- Indirect Trauma: Fractures caused by indirect mechanisms typically result from a violent, eccentric contraction of the quadriceps muscle against a flexed knee (e.g., stumbling and attempting to prevent a fall). This tensile failure usually produces a transverse fracture pattern. Because the force is explosive, it is often associated with extensive tears of the medial and lateral retinacular expansions.
- Combined Mechanisms: Most clinical presentations involve a combination of direct impact and indirect tensile forces, leading to complex, displaced, and comminuted fracture patterns.
Clinical Pearl: The degree of fracture displacement is directly proportional to the extent of the retinacular tear. A widely displaced transverse fracture pathognomonically indicates severe disruption of the medial and lateral retinacula, necessitating meticulous surgical repair of these soft tissue envelopes alongside osseous fixation.
CLINICAL EVALUATION
Patients with patellar fractures typically present with an acute hemarthrosis, localized anterior knee pain, and tenderness.
Physical Examination
A comprehensive physical examination is paramount. In displaced fractures or those with concomitant retinacular tears, a palpable defect (gap) may be present between the fracture fragments.
The most critical component of the examination is assessing the integrity of the extensor mechanism. The inability of the patient to actively extend the affected knee against gravity, or to maintain an actively extended leg (straight leg raise), indicates a complete disruption of the extensor mechanism and a torn retinaculum. This is an absolute indication for surgical intervention.
Diagnostic Pitfall: Pain inhibition can occasionally mask the patient's true ability to extend the knee. If active extension is limited purely by pain, the hemarthrosis should be aspirated under strict sterile conditions, followed by an intraarticular injection of a local anesthetic (e.g., 1% Lidocaine or 0.5% Bupivacaine). Once analgesia is achieved, the patient's active knee extension must be reassessed.
Evaluation of Open Fractures
An open wound in the vicinity of a patellar fracture must be treated with a high index of suspicion for an open joint injury, which constitutes a surgical emergency. If there is uncertainty regarding whether the traumatic wound communicates with the knee joint, a saline load test should be performed.
* Technique: Inject 50 to 120 mL of sterile normal saline (often mixed with methylene blue) into the knee joint via a standard superolateral arthrocentesis approach, observing the traumatic wound for fluid extravasation.
* Warning: The saline load test is not 100% reliable. False negatives can occur in open fractures with very small traumatic arthrotomies or if the fluid tracks into adjacent fascial planes rather than exiting the skin wound.
RADIOGRAPHIC EVALUATION
A standard trauma radiographic series for the knee must include Anteroposterior (AP), Lateral, and Axial (Merchant or Sunrise) views.
- Lateral View: This is the most valuable projection for evaluating transverse fractures and quantifying the degree of superior-inferior displacement and articular step-off.
- Axial (Merchant) View: Essential for identifying vertical fractures, marginal fractures, osteochondral shear injuries, and subtle articular incongruities that may be missed on orthogonal views.
- AP View: Useful for assessing overall comminution and ruling out concurrent distal femur or proximal tibia fractures.
Radiographic Pearl: A comparison view of the contralateral knee is sometimes necessary to differentiate an acute, undisplaced fracture from a bipartite patella. A bipartite patella represents a failure of ossification center fusion, is typically located in the superolateral quadrant, has smooth, sclerotic margins, and is bilateral in up to 50% of patients.
CLASSIFICATION OF PATELLAR FRACTURES
Fractures of the patella are broadly classified as undisplaced or displaced, and are further subclassified according to their geometric configuration.
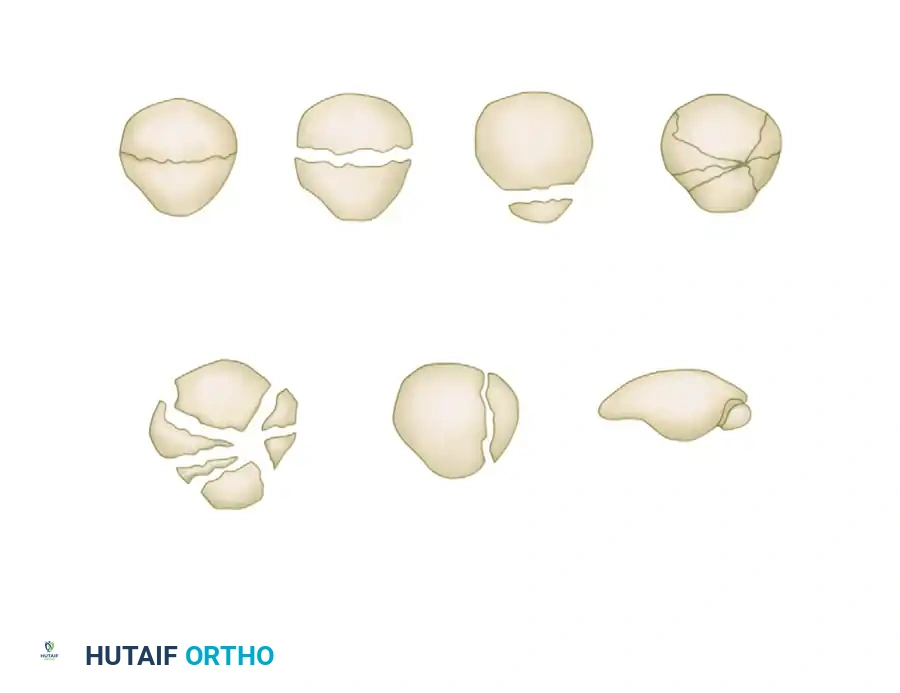
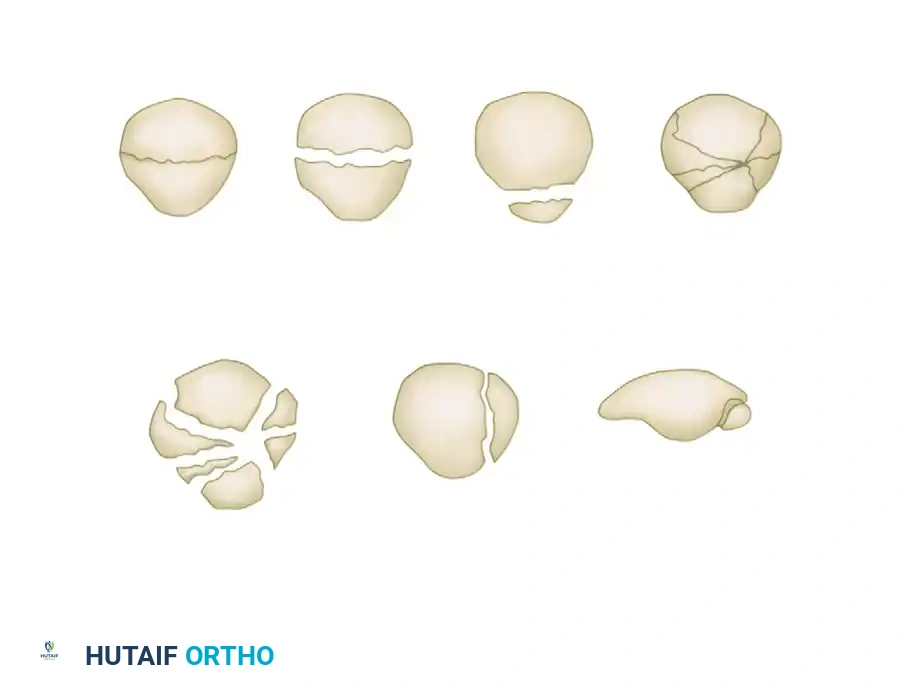
Morphological Subtypes
- Transverse Fractures: The most common pattern reported in the literature. They usually involve the central third of the patella but can occur at the proximal (apical) or distal (basal) poles. A variable amount of comminution may be present at the poles.
- Vertical Fractures: These typically involve the middle and lateral thirds of the patella. If only the extreme medial or lateral edge is affected, it is termed a marginal fracture. Vertical fractures are best visualized on axial radiographs. Because the fracture line runs parallel to the pull of the extensor mechanism, displacement and retinacular disruption rarely occur.
- Comminuted (Stellate) Fractures: Characterized by multiple fracture lines radiating from a central point, usually resulting from high-energy direct trauma. They are associated with a variable amount of displacement and severe chondral damage.
- Osteochondral Fractures: Often associated with patellar dislocations, these involve a shear injury to the articular cartilage and underlying subchondral bone.
INDICATIONS FOR SURGERY
Nonoperative Management
Indicated strictly for fractures that meet all the following criteria:
* Intact extensor mechanism (patient can perform a straight leg raise).
* Minimal displacement (< 2 to 3 mm of fragment separation).
* Minimal articular step-off (< 2 mm).
Operative Management
Absolute indications for surgical fixation include:
* Disruption of the extensor mechanism (inability to actively extend the knee).
* Displacement > 3 mm.
* Articular step-off > 2 mm.
* Open fractures.
* Osteochondral fractures with intraarticular loose bodies.
SURGICAL TECHNIQUES AND BIOMECHANICS
The primary goals of operative treatment are the anatomic restoration of the articular surface, rigid fixation to allow early range of motion, and the meticulous repair of the extensor retinaculum.
The Tension Band Principle
The anterior surface of the patella is subjected to massive tensile forces during knee flexion, while the articular surface is subjected to compressive forces. The tension band principle utilizes a construct (wire or heavy suture) placed on the anterior (tension) surface of the patella. When the knee flexes, the tensile forces are converted into compressive forces at the articular surface, dynamically stabilizing the fracture.
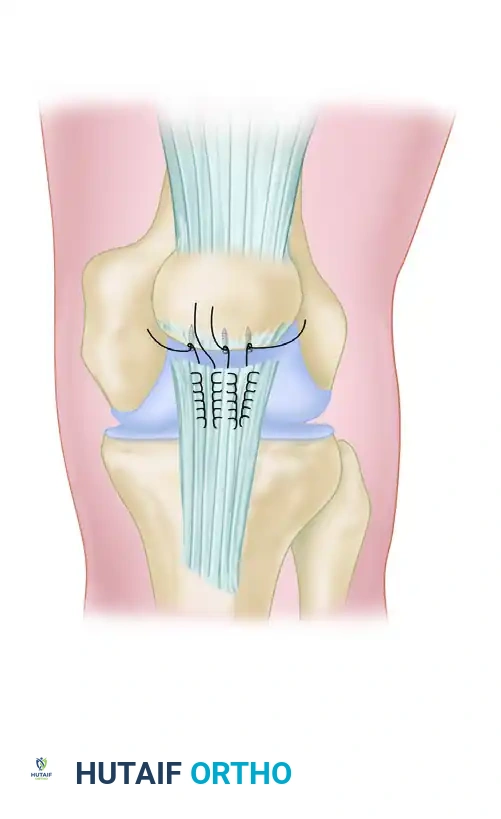
1. Modified Tension Band Wiring
Wiring techniques are the workhorse for transverse fractures. The most secure fixation, as demonstrated in experimental studies, is obtained with the modified tension band wiring technique (incorporating longitudinal Kirschner wires).
- Technique: Two parallel 2.0 mm K-wires are driven longitudinally across the reduced fracture. A flexible 18-gauge stainless steel wire is passed behind the K-wires at the superior and inferior poles in a figure-of-eight configuration over the anterior surface of the patella.
- Biomechanics: Weber et al. recommended anchoring the fixation wiring directly into the bone (via transosseous tunnels) rather than merely threading it through the soft tissue (quadriceps and patellar tendons) if early motion is to be initiated. Furthermore, adding a second tension band wire through the tendon has been shown to provide superior fixation.
- Outcomes: Results are generally favorable (81% good to excellent results reported by Lotke and Ecker). However, Smith et al. reported that 22% of fractures treated with tension band fixation displaced more than 2 mm, citing patient noncompliance and technical errors (e.g., loose wires, asymmetric tensioning) as the primary culprits.
2. Cannulated Screw Fixation with Tension Band
For fractures with large, robust fragments, two parallel screws alone can provide adequate fixation; however, biomechanical studies show slightly greater displacement with screws alone compared to tension band constructs.
- The Gold Standard Construct: Carpenter et al., in a landmark cadaveric study, demonstrated that specimens fixed with a tension band routed through parallel cannulated screws failed at the highest load.
- Berg's Technique: Berg described the fixation of displaced transverse fractures using a figure-of-eight wire passed through parallel cannulated compression screws.
- Advantages: This creates a low-profile construct that minimizes hardware prominence and subsequent soft-tissue irritation (a common complication of K-wires backing out). It permits early restricted motion and serves as an excellent salvage method after the failure of traditional tension band wiring.
3. Management of Comminution
If comminution is present, simple tension band wiring is insufficient.
* Lag Screw Conversion: Large comminuted fragments should first be lagged together with small fragment screws (2.7 mm or 3.5 mm) to convert the complex fracture into a simple transverse pattern, which is then neutralized with a tension band.
* Cerclage Wiring: A circumferential cerclage wire can be added around the equator of the patella to contain stellate comminution.
* Material Alternatives: Braided polyester and braided titanium cables have been utilized successfully and provide biomechanical fixation profiles similar to stainless steel wire, with potentially less hardware fatigue failure.
4. Arthroscopically Assisted Fixation
Arthroscopically assisted percutaneous screw fixation has been described for displaced transverse fractures. This minimally invasive approach preserves the anterior vascular supply and reduces soft-tissue morbidity, yielding good results in highly selected patients with simple fracture patterns and intact retinacula.
5. Partial and Total Patellectomy
If the degree of comminution and articular cartilage destruction is so severe that salvage of the patella is impossible, excision is warranted.
* Partial Patellectomy: Indicated for severe comminution localized to the superior or inferior pole. The comminuted fragments are excised, and the patellar or quadriceps tendon is reattached to the remaining healthy bone using transosseous tunnels or heavy suture anchors. It is critical to preserve as much of the patella as possible to maintain the mechanical advantage of the extensor mechanism.
* Total Patellectomy: Strictly a salvage procedure for irreparable, highly comminuted fractures. The entire patella is excised, and the quadriceps tendon is sutured directly to the patellar tendon. This results in a permanent reduction in extensor strength and alters knee kinematics, but provides pain relief in unsalvageable scenarios.
Surgical Warning: Following any patellar fixation or partial patellectomy, the medial and lateral retinacular tears MUST be meticulously repaired with heavy, non-absorbable sutures. The retinaculum provides crucial secondary stability to the extensor mechanism.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is dictated by the security of the surgical fixation and the quality of the patient's bone stock.
- Phase I (0 to 2 Weeks): The patient is placed in a hinged knee brace locked in full extension. Weight-bearing as tolerated (WBAT) is permitted with the brace locked in extension. Isometric quadriceps exercises (quad sets) and straight leg raises are initiated immediately to prevent muscle atrophy.
- Phase II (2 to 6 Weeks): If fixation is rigid (e.g., cannulated screws with tension band), controlled passive and active-assisted range of motion (ROM) is initiated. Flexion is typically advanced by 30 degrees every 1 to 2 weeks, depending on radiographic progression and clinical stability.
- Phase III (> 6 Weeks): Once radiographic consolidation is evident, the brace is discontinued. Progressive resistance exercises are introduced to restore quadriceps strength and endurance.
COMPLICATIONS
- Symptomatic Hardware: The most common complication following patellar fracture fixation. The anterior subcutaneous nature of the patella makes K-wires and wire knots highly prominent. Up to 30-50% of patients require a secondary surgery for hardware removal after fracture union.
- Loss of Fixation / Nonunion: Often due to technical errors (inadequate wire tensioning) or patient noncompliance with early weight-bearing in flexion. Requires revision fixation, often utilizing the Berg cannulated screw technique or partial patellectomy.
- Knee Stiffness: Arthrofibrosis and loss of terminal flexion are common, particularly if immobilization exceeds 3 to 4 weeks. Early, controlled mobilization is the best preventative measure.
- Post-Traumatic Osteoarthritis: Directly correlated with the severity of the initial chondral injury and the accuracy of the articular reduction. Even with anatomic reduction, the initial impact energy can cause chondrocyte apoptosis, leading to late-onset arthrosis.
You Might Also Like