The Elmslie-Trillat Operation: Comprehensive Surgical Guide

Key Takeaway
The Elmslie-Trillat operation is a highly specialized orthopedic procedure designed to realign the extensor mechanism by transferring the tibial tuberosity anteriorly and medially. It is primarily indicated for patients with recurrent patellar dislocations complicated by grade 3 or 4 chondromalacia. By optimizing patellofemoral tracking and reducing articular contact stress, this osteotomy provides a robust biomechanical solution for severe patellofemoral dysfunction.
Introduction to the Elmslie-Trillat Operation
The Elmslie-Trillat operation represents a cornerstone in the surgical management of complex patellofemoral instability and degenerative joint disease. Originally conceptualized to address extensor mechanism malalignment, the procedure has evolved through the contributions of Brown, Fulkerson, and others into a highly precise anteromedial transfer of the tibial tuberosity.
By altering the insertion vector of the patellar tendon, the Elmslie-Trillat procedure simultaneously corrects lateral patellar tracking and decompresses the patellofemoral articulation. This dual biomechanical advantage makes it an invaluable technique for orthopedic surgeons managing patients with recurrent dislocations superimposed on advanced chondral pathology. This comprehensive guide details the indications, biomechanical principles, preoperative planning, and step-by-step surgical execution of the Elmslie-Trillat operation.
Biomechanics of Tibial Tuberosity Transfer
Understanding the biomechanical interplay of the patellofemoral joint is critical for executing a successful Elmslie-Trillat procedure. The patella acts as a fulcrum, increasing the mechanical advantage of the quadriceps muscle. However, in the presence of a lateralized tibial tubercle (measured via the Tibial Tubercle-Trochlear Groove [TT-TG] distance), the lateral vector forces on the patella are exponentially increased during knee flexion.
Medialization and Anteriorization
The Elmslie-Trillat operation, particularly as modified by Brown et al., transfers the tuberosity both anteriorly and medially.
* Medialization: Corrects the abnormal Q-angle and normalizes the TT-TG distance, thereby eliminating the lateral subluxation vector that predisposes the patient to recurrent dislocations.
* Anteriorization: Elevates the extensor mechanism, which significantly increases the moment arm of the quadriceps while simultaneously decreasing the joint reaction forces across the patellofemoral articulation. This decompression is vital for preserving the remaining articular cartilage in the setting of advanced chondromalacia.
Clinical Pearl: Mechanical testing demonstrates that a flat (Elmslie-Trillat) osteotomy possesses significantly higher mean load-to-failure and total energy-to-failure rates compared to traditional oblique osteotomy techniques. This structural superiority provides a more stable construct for rigid internal fixation.
Indications and Patient Selection
Patient selection is the most critical determinant of success in tibial tuberosity osteotomies. The Elmslie-Trillat procedure is not a prophylactic operation; it is a salvage and realignment procedure for structurally compromised knees.
Primary Indications
- Recurrent Patellar Dislocations with Chondromalacia: The classic indication is recurrent lateral patellar dislocation associated with Outerbridge Grade 3 or 4 chondromalacia of the patella or trochlea.
- Patella Alta with Instability: In cases where recurrent dislocation is coupled with significant patella alta (defined by an Insall-Salvati index greater than 1.2), a modified Elmslie-Trillat incorporating a distal transfer is indicated.
- Severe Patellofemoral Degenerative Changes: Patients with isolated, severe patellofemoral osteoarthritis who are too young for a patellofemoral arthroplasty may benefit from the unloading characteristics of this osteotomy.
Contraindications
- High-Demand Athletes: Generally, this procedure is not indicated for competitive athletes due to the risk of stress fractures and the permanent alteration of extensor mechanism kinematics. It should be strictly reserved for patients with severe degenerative changes.
- Open Physes: Absolute contraindication. Performing this osteotomy in skeletally immature patients risks premature closure of the proximal tibial physis, leading to genu recurvatum.
- Isolated Medial Compartment Osteoarthritis: Anteriorization may inadvertently increase loads on the medial and lateral tibiofemoral compartments if not carefully calibrated.
Preoperative Planning and Imaging
Meticulous preoperative planning is required to quantify the exact degree of medial, anterior, and potentially distal transfer required.
Radiographic Evaluation
- Standard Knee Series: Weight-bearing anteroposterior (AP), true lateral (at 30 degrees of flexion), and axial (Merchant or Skyline) views.
- Insall-Salvati Ratio: Calculated on the true lateral radiograph to assess for patella alta. An index > 1.2 necessitates a distal transfer component during the osteotomy.
- Blumensaat’s Line: Used intraoperatively and preoperatively to ensure the inferior pole of the patella is not distalized excessively, which would create an iatrogenic patella baja.
- CT Scan (TT-TG Distance): Axial CT imaging superimposed over the femoral epicondyles and the tibial tubercle is the gold standard for quantifying lateralization. A TT-TG distance > 20 mm is highly pathologic and warrants medialization.
Surgical Technique: Step-by-Step
1. Positioning and Setup
The patient is placed supine on the operating table. A high thigh tourniquet is applied. The surgical limb is prepped and draped free to allow full range of motion (0 to 120 degrees) during the procedure. A bump may be placed under the ipsilateral hip to prevent external rotation of the limb.
2. Surgical Approach
A longitudinal incision is made just lateral to the anterior tibial crest, extending from the inferior pole of the patella to approximately 6 to 8 cm distal to the tibial tuberosity.
* Full-thickness fasciocutaneous flaps are elevated to preserve the vascular supply to the skin.
* The anterior compartment musculature is sharply elevated off the lateral aspect of the tibia to expose the proposed osteotomy site.
* The medial border of the patellar tendon and the tibial tuberosity are clearly defined.
3. Guide Pin Placement and Osteotomy Execution
Fulkerson et al. popularized the use of a specialized drill guide to ensure a perfectly planar cut.
- Pin Trajectory: Steinmann pins are placed through a guide to establish the cutting plane. The pins are angled from anteromedial (just deep to the anterior crest of the tibia) in a posterolateral direction.
- Depth Considerations: The depth of the cut dictates the amount of anteriorization. Making the cut deeper allows for a more pronounced anterior transfer of the tuberosity. However, a more superficial cut is often preferred as it avoids creating a massive stress riser effect, thereby reducing the risk of late postoperative fractures through the osteotomy site.
Surgical Warning: Care must be taken to protect the anterior tibial artery and the deep peroneal nerve, which lie in close proximity to the posterolateral exit point of the saw blade. Always use a retractor to protect the anterior compartment structures.
4. Osteotomy Trajectory and Biomechanical Adjustments
The angle of the osteotomy directly influences the final position of the tibial tuberosity. Figure 47-17 illustrates the cross-sectional variations of tibial tuberosity osteotomies.
Figure 47-17A: Transverse Osteotomy. A purely transverse cut allows for medialization but does not inherently elevate (anteriorize) or depress the origin of the tibial tuberosity.
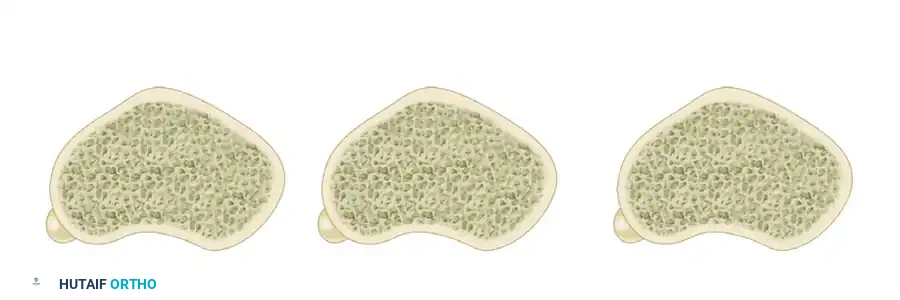
Figure 47-17B: Depressing Oblique Osteotomy. An oblique osteotomy angled steeply can inadvertently depress the tuberosity, which increases patellofemoral contact pressures and is generally contraindicated in the setting of chondromalacia.
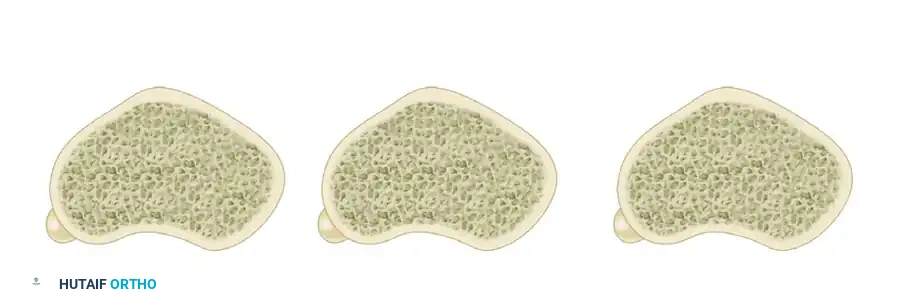
Figure 47-17C: Elevating Oblique Osteotomy (Fulkerson/Elmslie-Trillat Principle). An oblique osteotomy directed from anteromedial to posterolateral elevates the tuberosity as it is shifted medially. This is the desired trajectory for decompressing grade 3 or 4 chondromalacia.
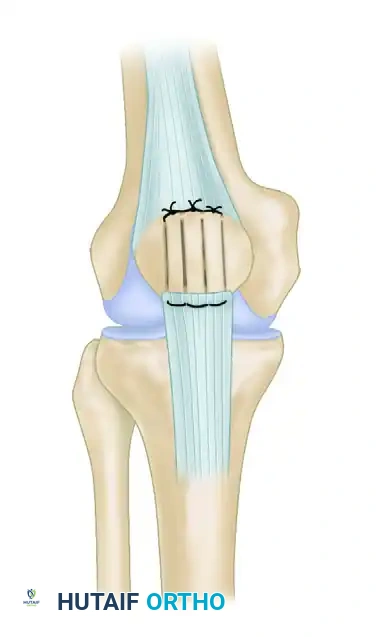
5. Management of Concomitant Patella Alta (Distal Transfer)
If preoperative imaging reveals an Insall-Salvati index > 1.2, a distal transfer must be incorporated.
1. The tuberosity is completely detached distally (unlike a purely hinged medialization).
2. Approximately 5 to 10 mm of bone is resected from the distal tip of the mobilized tuberosity block.
3. This resection creates a void, allowing the entire bone block to be translated distally.
4. Crucial Check: Before definitive fixation, a sterile radiopaque marker or intraoperative fluoroscopy must be used to reference Blumensaat's line. The inferior pole of the patella must not be placed distal to this line to prevent debilitating iatrogenic patella baja.
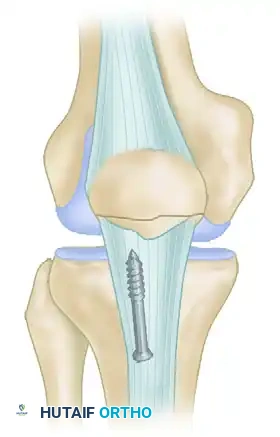
6. Fixation
Once the tuberosity is translated to the desired anteromedial (and potentially distal) position, it is temporarily held with Kirschner wires.
* Patellar tracking is assessed by taking the knee through a full range of motion. The patella should engage the trochlea centrally without lateral subluxation or excessive medial tightness.
* Definitive fixation is achieved using two or three 4.5 mm cortical lag screws directed from anterior to posterior.
* Screws must be countersunk to prevent symptomatic hardware prominence, and bicortical purchase is mandatory for rigid stability.
Complications and Pitfalls
While the Elmslie-Trillat operation yields 86% good to excellent results in properly selected patients, the complication profile must be respected.
- Stress Risers and Fractures: The most significant complication is a proximal tibial stress fracture. These can occur months after clinical and radiographic healing appear complete. The risk is mitigated by avoiding excessively deep osteotomy cuts and tapering the distal end of the osteotomy to prevent a sharp cortical step-off.
- Over-Medialization: Excessive medial transfer can lead to iatrogenic medial patellar instability or increased contact pressures on the medial patellar facet, accelerating medial-sided arthritis.
- Patella Baja: Overzealous distal transfer can permanently tether the extensor mechanism, leading to severe anterior knee pain, restricted flexion, and accelerated global patellofemoral arthrosis.
- Hardware Prominence: Due to the lack of subcutaneous fat over the anterior tibia, screw heads frequently become symptomatic, necessitating a secondary procedure for hardware removal once the osteotomy has fully united.
Postoperative Rehabilitation Protocol
A strict, phased rehabilitation protocol is essential to protect the osteotomy while restoring function.
Phase I: Maximum Protection (Weeks 0-4)
- Weight Bearing: Toe-touch weight-bearing (TTWB) or partial weight-bearing with crutches, depending on bone quality and fixation rigidity.
- Bracing: The knee is locked in full extension in a hinged knee brace during ambulation and sleep.
- Range of Motion (ROM): Passive and active-assisted ROM is initiated early (0 to 90 degrees) to prevent arthrofibrosis, but active knee extension is strictly prohibited to avoid avulsion of the osteotomy.
Phase II: Moderate Protection (Weeks 4-8)
- Weight Bearing: Progression to full weight-bearing (FWB) as tolerated, guided by radiographic evidence of early callus formation.
- Bracing: The brace is unlocked for ambulation once the patient demonstrates adequate quadriceps control (no extensor lag).
- Strengthening: Closed kinetic chain exercises (e.g., mini-squats, leg presses) are initiated. Open kinetic chain knee extension remains restricted.
Phase III: Return to Function (Weeks 8-16+)
- Radiographic Check: Confirmation of complete bony union before progressing to high-impact activities.
- Advanced Strengthening: Progression of closed-chain exercises, proprioceptive training, and stationary cycling.
- Return to Activity: Patients are counseled that return to heavy labor or low-impact sports may take 4 to 6 months. As noted, return to high-impact or competitive athletics is generally not recommended following this specific salvage procedure.
Conclusion
The Elmslie-Trillat operation remains a powerful surgical intervention for the treatment of recurrent patellar instability complicated by severe chondromalacia. By mastering the precise osteotomy angles, understanding the biomechanical implications of anteromedial transfer, and rigorously adhering to indications, orthopedic surgeons can provide significant pain relief and functional restoration to patients with complex patellofemoral pathology. Careful execution of the flat osteotomy technique, combined with vigilant postoperative rehabilitation, minimizes the risk of stress fractures and ensures long-term construct survivorship.
You Might Also Like