Comprehensive Conservative Management and Radiographic Evaluation of Patellofemoral Instability

Key Takeaway
Conservative management of acute patellar dislocation focuses on immediate joint reduction, hemarthrosis aspiration, and structured rehabilitation. Initial treatment involves short-term immobilization and cryotherapy, rapidly progressing to closed-chain quadriceps strengthening. Advanced imaging, including axial radiographs and CT scans for TT-TG distance, dictates the necessity of surgical intervention in cases of recurrent subluxation or persistent patellofemoral malalignment.
INTRODUCTION TO PATELLOFEMORAL INSTABILITY
Patellofemoral instability encompasses a spectrum of pathologies ranging from subtle recurrent subluxation to acute, traumatic lateral dislocation of the patella. The stability of the patellofemoral joint relies on a complex interplay of static and dynamic restraints. The primary static stabilizers include the osseous geometry of the femoral trochlea and the medial patellofemoral ligament (MPFL), which provides 50% to 60% of the restraint against lateral patellar translation at 0 to 30 degrees of knee flexion. The dynamic stabilizers are primarily governed by the extensor mechanism, specifically the balanced vector forces of the vastus medialis obliquus (VMO) and the vastus lateralis.
When these stabilizing mechanisms fail—often due to a combination of traumatic force and underlying anatomic dysplasia—dislocation occurs. While surgical intervention is increasingly discussed in modern orthopedic literature, a meticulously structured conservative treatment protocol remains the cornerstone of management for first-time acute dislocations without intra-articular loose bodies, as well as for many cases of chronic patellofemoral malalignment.
ACUTE PATELLAR DISLOCATION AND SUBLUXATION
Initial Clinical Evaluation and Acute Management
The immediate management of an acute patellar dislocation or severe subluxation dictates a rapid, systematic approach to minimize joint morbidity and prevent long-term arthrofibrosis. Upon presentation, the knee is typically held in a flexed posture. If the patella has not spontaneously reduced, gentle extension of the knee with a medially directed force on the lateral patellar border will typically achieve reduction.
Following reduction, the presence of a tense hemarthrosis is a critical clinical finding. A massive hemarthrosis not only causes severe nociceptive pain but also leads to reflex arthrogenic muscle inhibition, profoundly affecting the quadriceps and VMO.
Clinical Pearl: If a tense hemarthrosis is present, causing significant pain and capsular tightness, aspiration under strict sterile conditions is highly indicated before the extremity is immobilized. The presence of fat globules in the aspirate (lipohaemarthrosis) is a pathognomonic sign of an osteochondral fracture, which may necessitate early surgical intervention rather than conservative care.
Once aspirated, the knee must be immobilized to allow the acutely torn medial structures (specifically the MPFL and medial retinaculum) to rest and begin the fibroblastic phase of healing. The knee is placed in a commercial knee immobilizer or a hinged brace locked in extension. This is supplemented with a Jones-type compressive dressing to control third-spacing and recurrent effusion. Crutches are prescribed for protected weight-bearing ambulation.
Phase I: Early Rehabilitation Protocol (Days 1 to 7)
Prolonged immobilization is detrimental to articular cartilage nutrition and exacerbates quadriceps atrophy. Therefore, the acute immobilization phase is strictly limited. The knee immobilizer and compressive wrap are typically discontinued at 3 to 5 days, contingent upon the resolution of the acute inflammatory reaction.
During this acute period, rehabilitation begins immediately:
* Quadriceps-Setting Exercises: Essential for mitigating arthrogenic muscle inhibition.
* Straight-Leg Raises (SLR): Three sets of 15 to 20 repetitions are performed four or five times a day. This maintains extensor mechanism tone without articulating the patella against the trochlea.
* Cryotherapy: Ice is applied for 20 minutes every 2 to 3 hours to induce local vasoconstriction, reduce capillary permeability, and manage swelling.
Crutches are discontinued when the patient demonstrates sufficient quadriceps control—specifically, the ability to perform straight-leg raises with a 5-lb ankle weight without an extensor lag, and the ability to ambulate with a near-normal, pain-free gait.
Phase II & III: Advanced Rehabilitation and Return to Play
Rehabilitation must transition from static to dynamic stabilization, emphasizing the functional integration of the extensor mechanism.
Surgical Warning: Open-chain quadriceps exercises (e.g., seated leg extensions) place maximal joint reaction forces on the patellofemoral articulation at terminal extension, precisely when the patella is least constrained by the bony trochlea. These must be strictly avoided in the early phases of instability rehabilitation.
Rehabilitation should heavily emphasize closed-kinetic-chain (CKC) exercises. CKC exercises increase tibiofemoral compressive forces, which paradoxically stabilizes the patellofemoral joint and recruits co-contraction of the hamstrings, thereby reducing anterior tibial translation and patellar tendon stress.
* Wall Sets (Mini-Squats): The patient squats to approximately 40 degrees of flexion while keeping the back flat against a wall, holding for 15 to 20 seconds, for a total of 10 to 15 repetitions.
* Step-Up Exercises: Side and forward step-ups using a 6- to 8-inch platform are initiated once the acute inflammatory reaction has completely resolved.
* Short Arc Leg Presses: Limited to the 0 to 45-degree arc to maximize VMO recruitment while minimizing patellofemoral joint reaction forces.
* Endurance Strengthening: Utilization of a stationary bicycle (with a high seat to minimize knee flexion angles) and a Stairmaster.
Return to Sports Criteria:
The patient may be cleared to return to athletic activity only when quadriceps and hamstring muscle strength is at least 85% of the contralateral, normal limb (verified via isokinetic testing if available), and sport-specific agility has been fully regained. Generally, a patellar stabilizing brace (featuring a lateral J-buttress) is prescribed for the first 6 to 8 weeks during active rehabilitation and is worn long-term during sports activity to provide proprioceptive feedback and mechanical medialization.
RADIOGRAPHIC EVALUATION OF THE PATELLOFEMORAL JOINT
A comprehensive radiographic evaluation is mandatory to assess the underlying osseous architecture, identify predisposing dysplastic factors, and rule out osteochondral shear fractures. Standard anteroposterior (AP) and lateral radiographs are routine, but specialized views are required to truly appreciate patellofemoral tracking and congruence.
Standard and Specialized Positioning Techniques
Proper patient positioning is paramount for obtaining reproducible and diagnostically accurate radiographs of the patellofemoral joint.
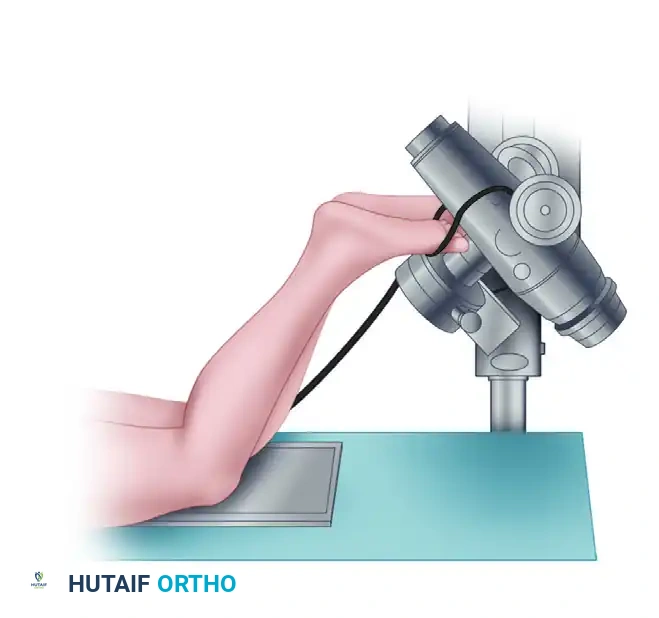
1. Infrapatellar View Positioning:
This technique is utilized to assess the inferior pole of the patella and the patellar tendon footprint.
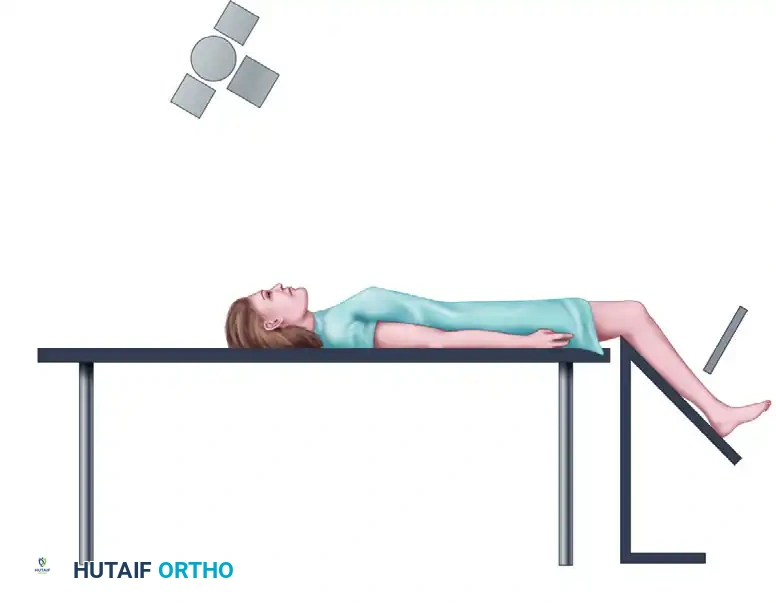
2. Axial View Positioning:
The axial view is critical for assessing the dynamic tracking of the patella within the trochlear groove. The knee is typically flexed to 30 or 45 degrees.
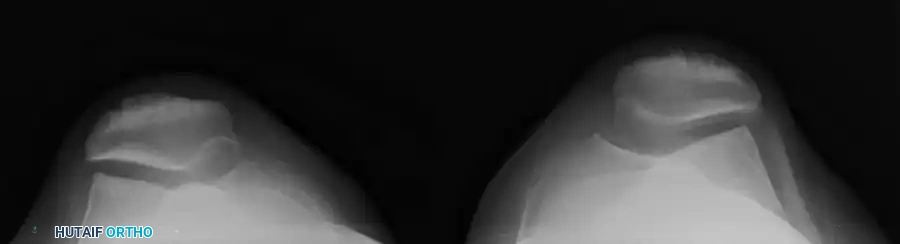
3. Skyline View Positioning:
The skyline view provides a tangential perspective of the patellofemoral articulation, allowing the surgeon to evaluate the medial and lateral facets, the depth of the trochlear sulcus, and the presence of marginal osteophytes.
Assessing Patellar Tilt and Sulcus Morphology
Once the appropriate views are obtained, the surgeon must analyze the images for signs of malalignment, tilt, and dysplasia.
Lateral Patellar Tilt:
On an axial or skyline view, the patella should sit symmetrically within the trochlea. A lateral tilt indicates tightness of the lateral retinaculum and potential insufficiency of the medial restraints.

Trochlear Dysplasia and Sulcus Angle:
The morphology of the femoral sulcus is a primary determinant of patellar stability. While complex classification systems (such as the Dejour classification) exist, under most circumstances, simply evaluating the radiographs is sufficient to differentiate a shallow, dysplastic sulcus from a normal, deep sulcus. The Merchant view is particularly useful for demonstrating a wide, flattened sulcus angle, which predisposes the patient to lateral subluxation.

Patellofemoral Congruence and Measurements
An analysis of patellofemoral congruence is highly indicated, especially when clinical subluxation is minimal or subtle. The measurements described by Merchant et al. remain the gold standard for quantifying patellar subluxation.
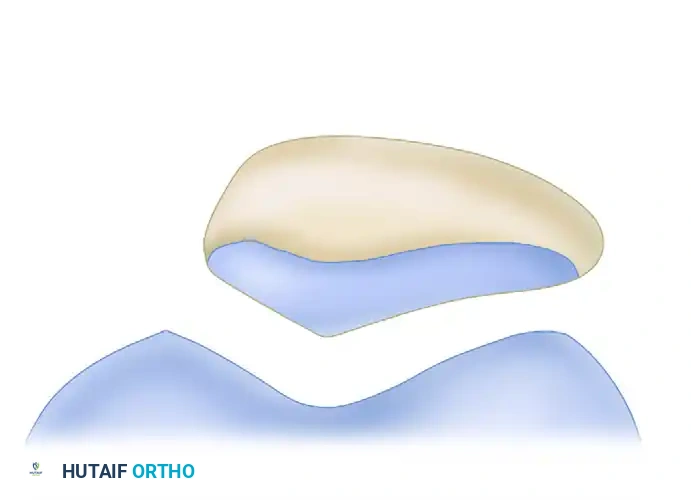
FIGURE 47-10: Measurements of patellofemoral congruence described by Merchant et al. F, facet; L, lateral condyle; M, medial condyle; P, patellar ridge; S, sulcus. Angle MSL is the sulcus angle (average, 137 degrees; standard deviation, 6 degrees). Line SO is the zero reference line bisecting the sulcus angle. Angle PSO is the congruence angle (average, −8 degrees; standard deviation, 6 degrees). Line PF (lateral facet) and line ML form the patellofemoral angle, which should diverge laterally.
Pitfall: A congruence angle greater than +16 degrees is highly indicative of pathologic lateral patellar subluxation. Failure to recognize an abnormal congruence angle may lead to inappropriate clearance for sports, resulting in recurrent dislocation and progressive chondral damage.
Advanced Cross-Sectional Imaging: CT and the TT-TG Distance
While plain radiographs provide excellent baseline data, Computed Tomography (CT) is the definitive modality for quantifying the lateralization of the tibial tubercle relative to the femoral trochlea—a critical metric known as the Tibial Tubercle-Trochlear Groove (TT-TG) distance.
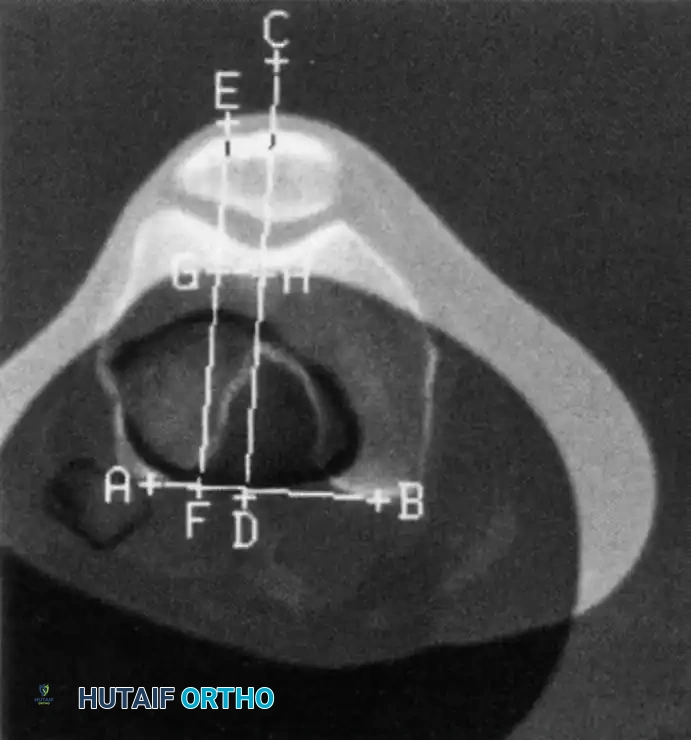
FIGURE 47-11: Lines used to calculate tibial tubercle lateralization using CT. A line is drawn on a superimposed image between the posterior margins of the femoral condyles (AB). Two lines are drawn perpendicular to this: one bisecting the femoral trochlear groove (CD) and one bisecting the anterior tibial tuberosity through a chosen point in the center of the patellar tendon insertion (EF). The distance between these two lines (GH) is measured in millimeters.
A normal TT-TG distance is typically less than 15 mm. A measurement approaching or exceeding 20 mm is considered highly abnormal and represents a significant biomechanical vector pulling the patella laterally. In the setting of recurrent instability, a TT-TG > 20 mm is a strong indication for a bony realignment procedure, such as a Fulkerson anteromedialization osteotomy.
PATELLOFEMORAL MALALIGNMENT AND RECURRENT PATELLAR SUBLUXATION
Chronic Conservative Management Strategies
It is a fundamental orthopedic principle that surgery is not needed in all patients with patellofemoral malalignment or recurrent subluxation of the patella. Good to excellent functional results have been consistently achieved with a rigorous, conservative exercise treatment program, particularly in moderately active individuals without severe underlying dysplasia.
A rehabilitation program designed to strengthen the quadriceps muscle—specifically targeting the VMO to counteract lateral tracking—is prime. A program similar to that followed after an acute dislocation is utilized, but with the addition of more advanced resistive exercises. This can be started early in the clinical course. Furthermore, a patellar stabilization brace can be worn during all high-risk activities to help prevent chronic recurrent subluxation and provide a sense of security for the patient.
Indications for Surgical Intervention
Conservative management is not universally successful. The surgeon must recognize when non-operative modalities have been exhausted to prevent irreversible patellofemoral osteoarthritis.
With failed conservative treatment in active, healthy surgical candidates—defined as those who experience recurrent instability episodes despite a minimum of 3 to 6 months of dedicated physical therapy—operative correction is necessary to help prevent joint deterioration.
Surgical decision-making is dictated by the specific pathoanatomy identified during the radiographic and clinical evaluation:
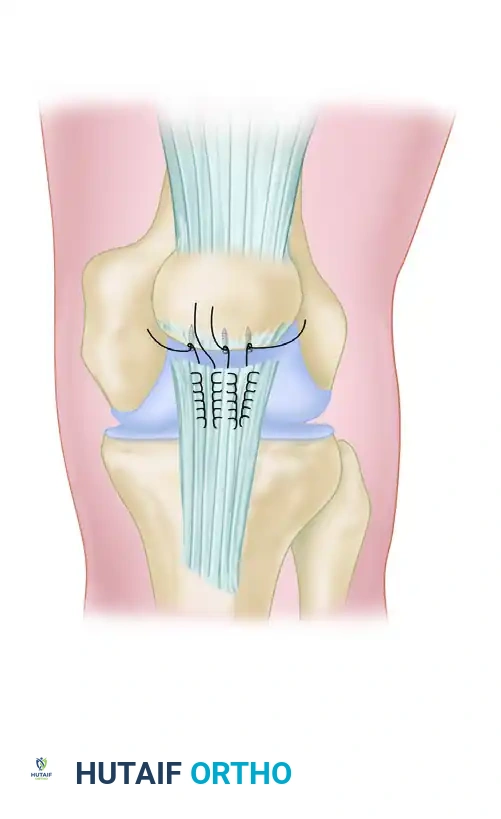
1. Medial Laxity: If the primary pathology is a torn or incompetent MPFL with a normal TT-TG distance, an MPFL reconstruction (often using a hamstring autograft or allograft) is indicated to restore the medial checkrein.
2. Bony Malalignment: If the TT-TG distance is > 20 mm, soft tissue procedures alone will fail due to the overwhelming lateral biomechanical vector. In these cases, a tibial tubercle transfer (osteotomy) is necessary to medialize the extensor mechanism, normalize the TT-TG distance, and decompress the lateral articular facets.
By meticulously combining conservative rehabilitation protocols with precise radiographic analysis, the orthopedic surgeon can optimize patient outcomes, reserving operative intervention strictly for those who demonstrate clear biomechanical failure.
Associated Surgical & Radiographic Imaging
You Might Also Like