Comprehensive Management of Ipsilateral Femoral Neck and Shaft Fractures

Key Takeaway
Ipsilateral femoral neck and shaft fractures occur in 1% to 9% of femoral shaft injuries. Because missed femoral neck fractures lead to catastrophic complications, a dedicated pelvic CT is mandatory for all blunt trauma femur fractures. Surgical priority dictates stabilizing the femoral neck first to ensure anatomic reduction, followed by shaft fixation. Postoperative protocols strictly limit patients to touch-down weight bearing for 10 to 12 weeks to optimize union.
Introduction and Epidemiology
Ipsilateral femoral neck fractures occur in association with femoral shaft fractures in approximately 1% to 9% of cases. These complex, high-energy injuries present a formidable challenge to the orthopedic surgeon. They are typically the result of severe blunt trauma, such as motor vehicle collisions or falls from a significant height, where an axial load is applied to a flexed and abducted thigh.
The timing of the diagnosis of the femoral neck fracture has a dramatic impact on patient outcomes. Historically, up to 30% of associated femoral neck fractures were missed at initial presentation. Late diagnosis of concomitant femoral neck fractures can lead to disastrous complications, including avascular necrosis (AVN), nonunion, varus collapse, and the need for early arthroplasty in young patients. Consequently, a high index of suspicion and a rigorous, standardized diagnostic protocol are paramount.
Diagnostic Protocols and Advanced Imaging
Radiographs must be carefully scrutinized to avoid missing an associated femoral neck fracture. The distracting nature of a grossly deformed femoral shaft fracture often draws the trauma team's attention away from the proximal femur. Furthermore, the femoral neck fracture in this setting is frequently nondisplaced or minimally displaced, and often vertically oriented (Pauwels type III), making it difficult to visualize on standard trauma bay plain films.
The standard radiographic evaluation of femoral fractures must include:
* Anteroposterior (AP) and lateral views of the entire femur.
* An AP view of the pelvis.
* A dedicated lateral view of the affected hip.
Clinical Pearl: Because a high-quality lateral image of the affected hip can be exceptionally difficult to obtain in a patient with a grossly unstable femoral shaft fracture, a pelvic CT scan is mandatory for every patient who sustains a femoral fracture caused by blunt trauma.
The pelvic CT scan should never be limited to standard axial images. It must include high-resolution coronal and sagittal reconstructed images to accurately assess the trabecular lines of the femoral neck and head.
Surgical Timing and Priorities
When an ipsilateral femoral neck and shaft fracture is diagnosed preoperatively, the fundamental principle of surgical management is clear: treatment of the femoral neck fracture is the absolute priority, followed by treatment of the femoral shaft.
The rationale for this sequence is biomechanical. Manipulating the lower extremity to reduce and nail a femoral shaft fracture generates significant rotational and translational forces across the hip joint. If the femoral shaft is addressed first, a nondisplaced femoral neck fracture can easily be displaced during reaming or nail insertion, drastically increasing the risk of avascular necrosis and compromising the blood supply derived from the medial femoral circumflex artery (MFCA).
Preoperative Planning and Patient Positioning
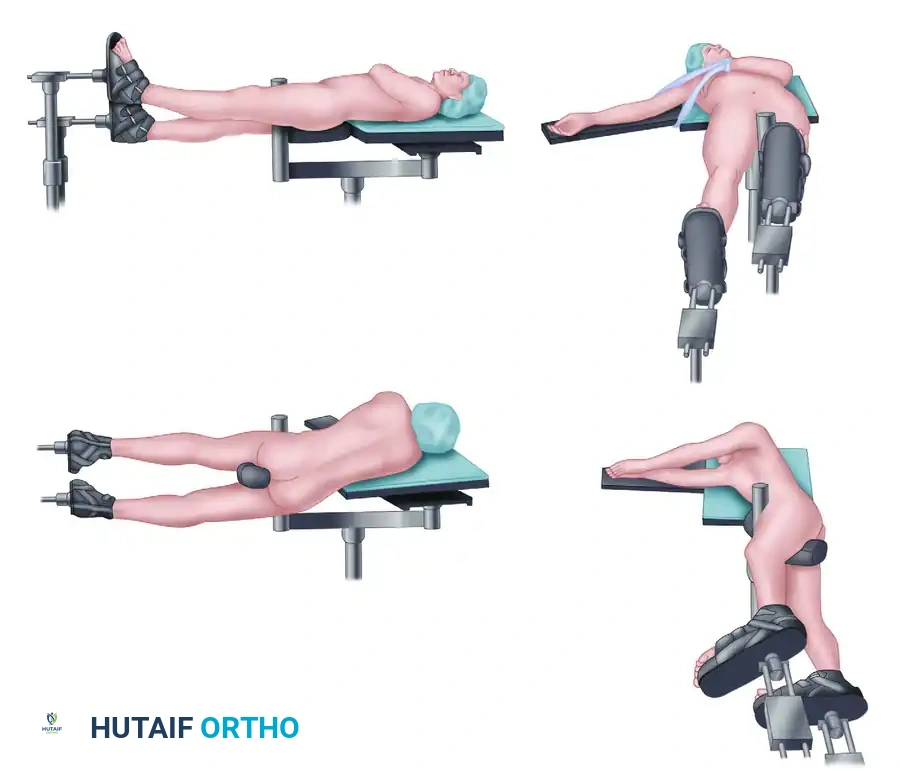
Reduction and fixation are optimally performed with the patient positioned on a radiolucent fracture table. This setup allows for the application of controlled traction and facilitates the highest quality orthogonal fluoroscopic imaging of the proximal femur without interference from the contralateral leg.
- Positioning: Supine on a fracture table with the contralateral leg placed in a hemilithotomy position or scissored posteriorly.
- Preparation: The entire affected limb, from the iliac crest to the toes, should be prepped and draped to allow for extensile approaches if necessary.
Surgical Approaches and Techniques
Management of the Displaced Femoral Neck
If the femoral neck is displaced, anatomic reduction is non-negotiable. Closed reduction should be attempted gently; however, if anatomic alignment is not achieved, open reduction is mandatory. Open reduction is typically performed through either a Smith-Petersen (anterior) or Watson-Jones (anterolateral) approach.
- Smith-Petersen Approach: Utilizes the internervous plane between the sartorius (femoral nerve) and tensor fasciae latae (superior gluteal nerve) superficially, and the rectus femoris (femoral nerve) and gluteus medius (superior gluteal nerve) deeply. This provides excellent direct visualization of the anterior femoral neck.
- Watson-Jones Approach: Utilizes the internervous plane between the tensor fasciae latae and the gluteus medius.
Once anatomic reduction is achieved and provisionally held with Kirschner wires, stabilization is obtained with either multiple cannulated screws or a compression hip screw (CHS).
Figure 55-62A: Preoperative radiograph demonstrating a displaced ipsilateral femoral neck and shaft fracture.
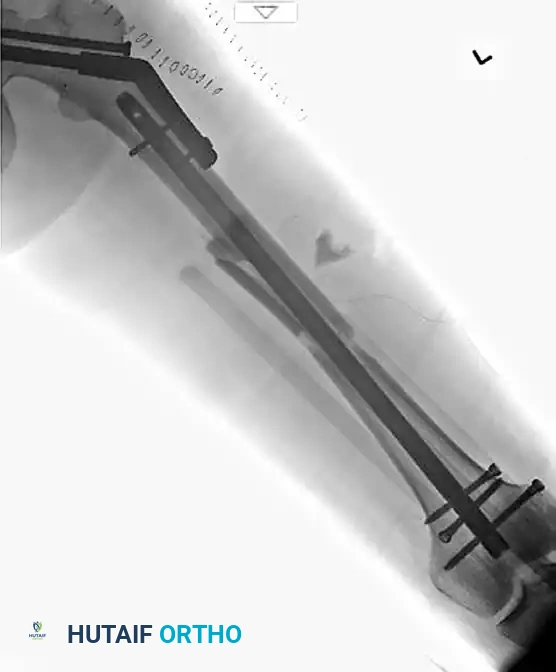
Figure 55-62B: Postoperative radiograph demonstrating fixation of the femoral neck with cannulated screws and the shaft with a retrograde intramedullary nail.

Figure 55-62C: Lateral postoperative radiograph confirming anatomic alignment and appropriate hardware placement.
Management of the Nondisplaced Femoral Neck
If the femoral neck is nondisplaced, it can be stabilized in situ. Fixation options include:
1. Cannulated Screws: Typically three 6.5mm or 7.3mm screws placed in an inverted triangle configuration. This is tissue-sparing but offers less biomechanical stability for vertically oriented shear fractures.
2. Compression Hip Screw (CHS): Provides superior biomechanical stability, particularly for basicervical or high-shear angle fractures, but requires a larger exposure.
Surgical Warning: A nondisplaced femoral neck fracture with an associated femoral shaft fracture can theoretically be treated with a single device, such as an antegrade reconstruction nail. However, this is technically difficult. Achieving the perfect starting point for the nail while simultaneously perfectly aligning the cephalomedullary screws into the femoral head often leads to malreduction of the neck. The potential complications (varus collapse, nonunion) are significantly greater with single-implant constructs compared to dual-implant constructs (e.g., cannulated screws for the neck and a retrograde nail for the shaft).
Intraoperative Protocols to Prevent Missed Fractures
Despite rigorous preoperative imaging, occult fractures can still be missed. To avoid leaving the operating room with an undiagnosed femoral neck fracture, a strict intraoperative fluoroscopic protocol must be adhered to.
After the placement of an intramedullary nail for the femoral shaft, the surgeon must obtain:
1. Live fluoroscopic images of the hip through a full range of motion.
2. A standard AP view of the pelvis with the extremities in internal rotation (to profile the femoral neck) while the patient is still under anesthesia.
Even with this exhaustive protocol, it is possible to miss a hairline femoral neck fracture. Therefore, repeat imaging of the hip (plain films or CT) is strictly indicated postoperatively if the patient has any new or persistent complaints of hip or groin pain.
Intraoperative Discovery of a Missed Neck Fracture
Discovering a femoral neck fracture after the placement of a femoral shaft intramedullary nail is a highly stressful intraoperative scenario. Treatment is dictated by the amount of fracture displacement and the specific design of the intramedullary nail system that has already been implanted.
If the femoral neck fracture has not been diagnosed until this point, it is highly likely that the fracture is nondisplaced or only minimally displaced.
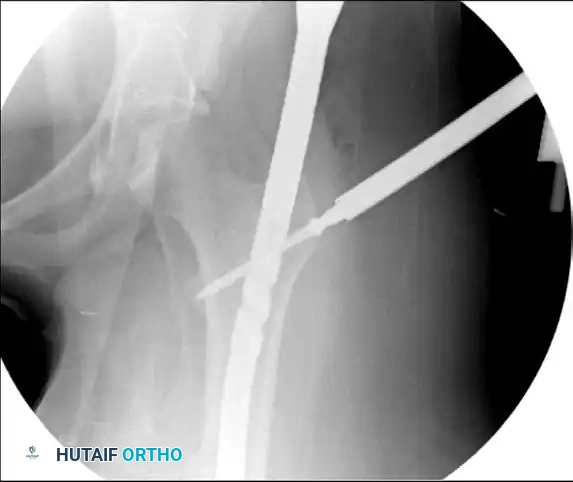
Figure 55-63A: Preoperative radiograph of a femoral shaft fracture. The subtle nondisplaced femoral neck fracture was initially missed.
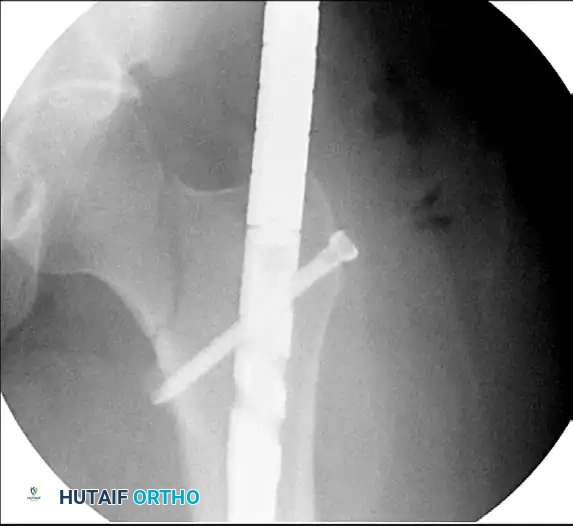
Figure 55-63B: Intraoperative fluoroscopic view after placement of an antegrade intramedullary nail. Note the appearance of the proximal femur.

Figure 55-63C: Intraoperative fluoroscopic view after range of motion of the hip under live fluoroscopy reveals the previously occult femoral neck fracture.
Salvage Techniques
Scenario A: The Nail System Has a Reconstruction Option
If the fracture is nondisplaced and the implanted nail system features a reconstruction option (holes designed for cephalomedullary screws), the surgeon can convert the construct.
1. The standard proximal transverse interlocking screw is removed.
2. Often, the nail position must be adjusted (tapped cephalad or caudad) to perfectly align the reconstruction holes with the center of the femoral neck and head.
3. Critical Step: If this adjustment is necessary, two provisional guide pins must be placed anteriorly across the femoral neck before moving the nail to prevent iatrogenic displacement of the fracture during nail manipulation.
4. Once aligned, two cephalomedullary screws are placed into the femoral head.

Figure 55-63D: Intraoperative fluoroscopic view after removal of the standard proximal interlocking screw, adjustment of the nail, and successful placement of reconstruction screws.
Scenario B: The Nail System Lacks a Reconstruction Option
If the nailing system does not allow for a reconstruction option, the surgeon must utilize a "miss-a-nail" technique. Multiple cannulated screws (typically 6.5mm or 5.0mm) are carefully placed around the intramedullary nail. This requires precise fluoroscopic guidance to ensure the screws pass anterior or posterior to the nail without compromising the fixation of either the neck or the shaft.
Complex Proximal Femoral Trauma: Associated Head and Acetabular Fractures
In the most severe high-energy trauma cases, ipsilateral femoral fractures may be complicated by concomitant injuries to the femoral head and acetabulum, such as a Pipkin IV fracture-dislocation. These require highly specialized, multidisciplinary orthopedic trauma management.
Surgical dislocation of the hip (Ganz approach) is often required to adequately address these complex intra-articular injuries. This approach allows for a 360-degree view of the femoral head and acetabulum while protecting the medial femoral circumflex artery.

Figure 55-61A: Preoperative radiograph demonstrating a complex Pipkin IV fracture (posterior wall acetabular fracture with an associated femoral head fracture).

Figure 55-61B: Postoperative radiograph following surgical dislocation of the hip, open reduction and internal fixation of the posterior wall acetabular fracture, and débridement of the infrafoveal femoral head fracture.
Figure 55-61C: Postoperative axial CT scan confirming concentric reduction and hardware placement.

Figure 55-61D: Postoperative coronal CT scan demonstrating restoration of the articular congruity.

Figure 55-61E: Postoperative AP pelvic radiograph showing the final construct.
Postoperative Rehabilitation and Protocols
The postoperative rehabilitation protocol for patients with ipsilateral femoral neck and shaft fractures is significantly more conservative than for isolated femoral shaft fractures.
Because the femoral neck fracture is the "weak link" in the construct and is highly susceptible to varus collapse and nonunion under cyclic loading, strict weight-bearing precautions are mandatory.
- Weight Bearing: Patients are allowed only touch-down weight bearing (TDWB) or flat-foot weight bearing (maximum 10-15 lbs of pressure) on the affected extremity for the first 10 to 12 weeks after surgery.
- Mobilization: Early range of motion of the hip and knee is encouraged to prevent arthrofibrosis and promote cartilage nutrition, provided the fracture fixation is deemed stable intraoperatively.
- Deep Vein Thrombosis (DVT) Prophylaxis: Given the high-energy nature of the trauma and the prolonged period of restricted weight bearing, aggressive chemical and mechanical DVT prophylaxis is required per institutional trauma guidelines.
- Follow-up: Serial radiographs are obtained at 2, 6, 12, and 24 weeks to monitor for fracture consolidation, hardware failure, or signs of avascular necrosis of the femoral head. Full weight bearing is only initiated once radiographic evidence of bridging callus is observed at both fracture sites.
You Might Also Like