Disorders of the Peroneal Tendons: Comprehensive Diagnosis and Surgical Management

Key Takeaway
Peroneal tendon disorders encompass tendinitis, subluxation, and attritional ruptures, frequently presenting in athletes or patients with cavovarus foot deformities. Accurate diagnosis relies on clinical examination and advanced imaging like MRI or ultrasound. Management ranges from conservative immobilization to surgical tenosynovectomy, tubularization, or tenodesis. This guide details the evidence-based evaluation, Krause and Brodsky classification, and step-by-step operative techniques for optimal functional recovery.
Introduction to Peroneal Tendon Disorders
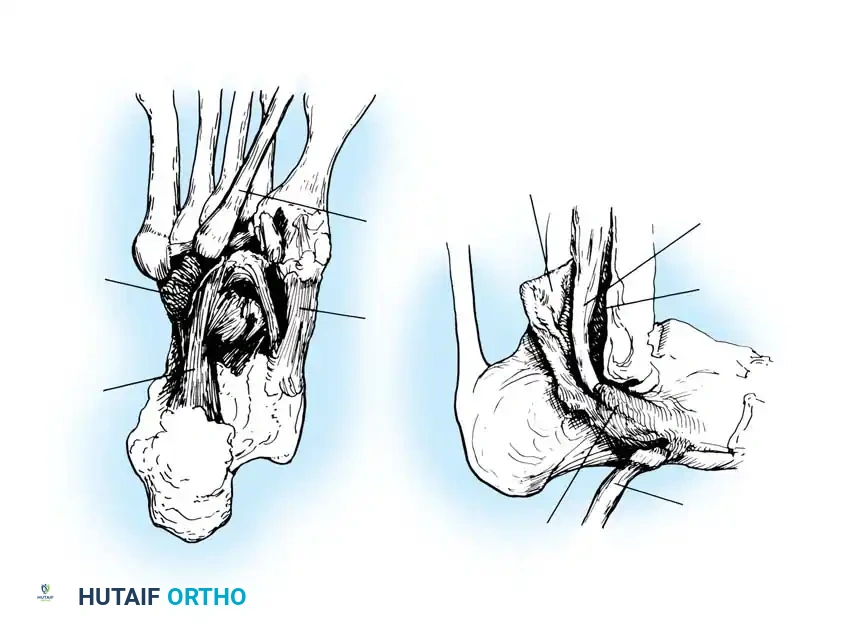
Disorders of the peroneal tendons represent a complex spectrum of pathology that can cause significant lateral hindfoot pain, instability, and functional impairment. The peroneus longus and peroneus brevis tendons are critical dynamic stabilizers of the lateral ankle and primary evertors of the foot. The peroneus brevis inserts onto the base of the fifth metatarsal, while the peroneus longus courses through the cuboid groove to insert onto the plantar aspect of the medial cuneiform and the base of the first metatarsal, acting as a vital plantarflexor of the first ray.
Pathology within this tendon complex is frequently misdiagnosed as chronic lateral ankle sprains. A thorough understanding of the regional anatomy, biomechanics, and associated osseous deformities—particularly the cavovarus foot—is essential for the orthopedic surgeon to formulate an effective treatment algorithm.
Pathoanatomic Classification
Disorders of the peroneal tendons fall primarily into three distinct clinical entities, each with unique demographic and biomechanical profiles:
1. Primary Peroneal Tendinitis Without Subluxation
This condition is characterized by tenosynovitis and potential attritional tearing without demonstrable instability of the tendons within the retromalleolar groove. It is most frequently observed in middle-aged athletes. Patients typically present with localized swelling, effusion within the peroneal tendon sheath, and pain exacerbated by activity. Manual examination reveals stable tendons without subluxation over the lateral malleolus.
2. Peroneal Tendinitis with Instability
The second type involves tendinitis associated with instability of the peroneal tendons at the level of the superior peroneal retinaculum (SPR). This may occur with or without an acute rupture or avulsion of the SPR. It is highly correlated with chronic lateral ankle instability and is frequently seen in younger athletes following acute inversion or dorsiflexion trauma. The incompetence of the SPR allows the tendons to subluxate anteriorly over the fibula, leading to mechanical attrition and longitudinal split tears, predominantly of the peroneus brevis.
3. Stenosing Tenosynovitis of the Peroneus Longus
The third variant is stenosing tenosynovitis specifically affecting the peroneus longus tendon. This is often associated with distinct anatomical anomalies, including:
* A painful or hypertrophic os peroneum.
* An enlarged peroneal tubercle on the lateral calcaneus.
* Pathological changes at the calcaneocuboid joint.
* Complete encasement of the peroneus longus tendon within a bony tunnel at the level of the cuboid.
Clinical Pearl: Associated physical findings in stenosing tenosynovitis often include a high arch (cavus) or varus hindfoot. Limitation of subtalar motion in eversion is also a frequent concomitant finding. As emphasized by Redfern and Myerson, comprehensive treatment must include the correction of underlying bony deformities (e.g., lateralizing calcaneal osteotomy) and ligamentous instability; otherwise, isolated soft-tissue repair is doomed to fail.

Clinical Evaluation and Diagnosis
The diagnosis of peroneal tendinitis and tearing is primarily clinical, supplemented by targeted advanced imaging.
History and Physical Examination
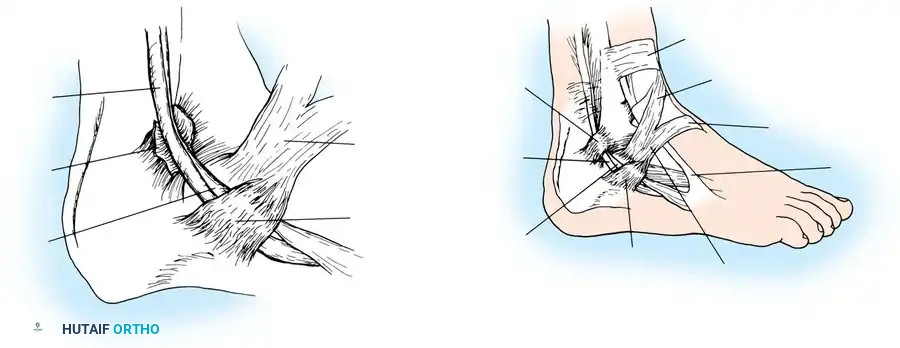
Patients typically report posterolateral ankle pain, swelling, and occasionally a snapping sensation. Presenting symptoms of tenosynovitis include tenderness, grating, and crepitance—which may even be audible—just posterior to the lateral malleolus as the two tendons (longus lateral to brevis) course beneath the SPR. In severe cases, the tendon sheaths become so thickened and excursion so reduced that peroneal spasm develops.
Evaluation must be performed with the patient in a standing position. The examiner should view the foot from behind to determine biomechanical abnormalities of the hindfoot, specifically looking for a varus (or less commonly, valgus) alignment.
Manual testing of eversion strength is necessary, though it remains intact in most patients due to compensatory mechanisms. Selective testing of the peroneus longus is performed by placing the ankle in forced active eversion while the examiner pushes up on the medial column at the level of the first metatarsal head. Areas of maximal tenderness suggest zones of rupture or synovitis, particularly at the superior and inferior peroneal retinacula, or just proximal to the base of the fifth metatarsal.
Imaging Modalities
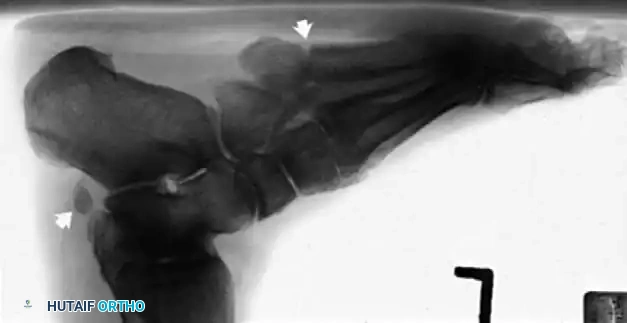
Radiographic examination is indicated to assess for instability, osseous avulsions, and structural alignment. Plain films must be inspected carefully for bone densities in adjacent soft tissues, such as a "fleck sign" indicating SPR avulsion, or proximal migration of the os peroneum indicating a peroneus longus rupture.
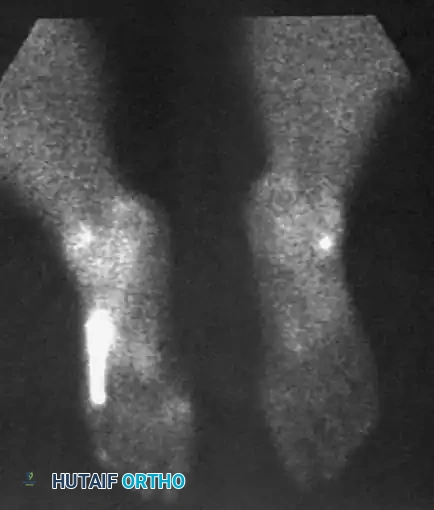
While bone scans and computed tomography (CT) can be helpful for osseous pathology, Magnetic Resonance Imaging (MRI) and dynamic ultrasound are the gold standards for soft tissue evaluation. Grant et al. demonstrated the high sensitivity and specificity of ultrasound for evaluating peroneal tendon tears, allowing for dynamic assessment of subluxation. MRI provides excellent visualization of tenosynovitis, tendon morphology, and longitudinal split tears.

Krause and Brodsky Classification
Surgical decision-making for peroneus brevis tears is heavily guided by the intraoperative assessment of tendon viability. Krause and Brodsky classified tears of the peroneus brevis into two distinct types:
* Grade I: Involves 50% or less of the cross-sectional area of the peroneus brevis tendon.
* Grade II: Involves more than 50% of the cross-sectional area of the tendon.
This classification directly dictates whether the tendon can be salvaged via tubularization (Grade I) or requires excision and tenodesis (Grade II).
Nonoperative Management
Peroneal tendinitis occurring as an isolated entity without observable subluxation is uncommon. However, conservative treatment can be highly effective, particularly if MRI or ultrasound confirms the absence of significant intratendinous tearing.
Initial management includes:
* Immobilization: Cast or controlled ankle motion (CAM) boot immobilization for 4 to 6 weeks to reduce mechanical stress.
* Pharmacotherapy: Oral anti-inflammatory medications (NSAIDs).
* Corticosteroid Injection: Careful, ultrasound-guided injection of corticosteroid into the peroneal tendon sheath may relieve acute inflammation. Warning: Intratendinous injection must be strictly avoided to prevent iatrogenic rupture.
* Biomechanical Correction: For long-term benefit, underlying biomechanical faults must be addressed. This generally involves custom orthoses (e.g., lateral heel wedge for a varus hindfoot) or an ankle brace for 4 to 6 months following the resolution of acute symptoms.
Surgical Management: Indications and Preoperative Planning
For patients who fail conservative management, surgical intervention consisting of debridement, repair, and tenosynovectomy is indicated. Preoperative MRI or ultrasound is invaluable for anticipating the extent of debridement and the exact location of pathological changes.
Surgical Warning: Intraoperative findings often reveal more extensive pathology than suggested by preoperative imaging. The surgeon must be prepared to perform a tenodesis or tendon transfer if the tendons are found to be non-viable. Furthermore, any concomitant varus hindfoot deformity must be corrected (e.g., via a Dwyer or lateralizing calcaneal osteotomy) to prevent recurrent failure of the repaired tendons.


Operative Technique: Synovectomy and Repair of Peroneal Tendons (Technique 85-9)
1. Patient Positioning and Anesthesia
The procedure is performed under general or regional anesthesia. The patient is placed in the lateral decubitus position, or supine with a large bolster beneath the ipsilateral hip to internally rotate the leg, allowing excellent access to the lateral ankle. The foot is held in equinovalgus to relax the peroneal tendons. A thigh tourniquet is applied and inflated after exsanguination.
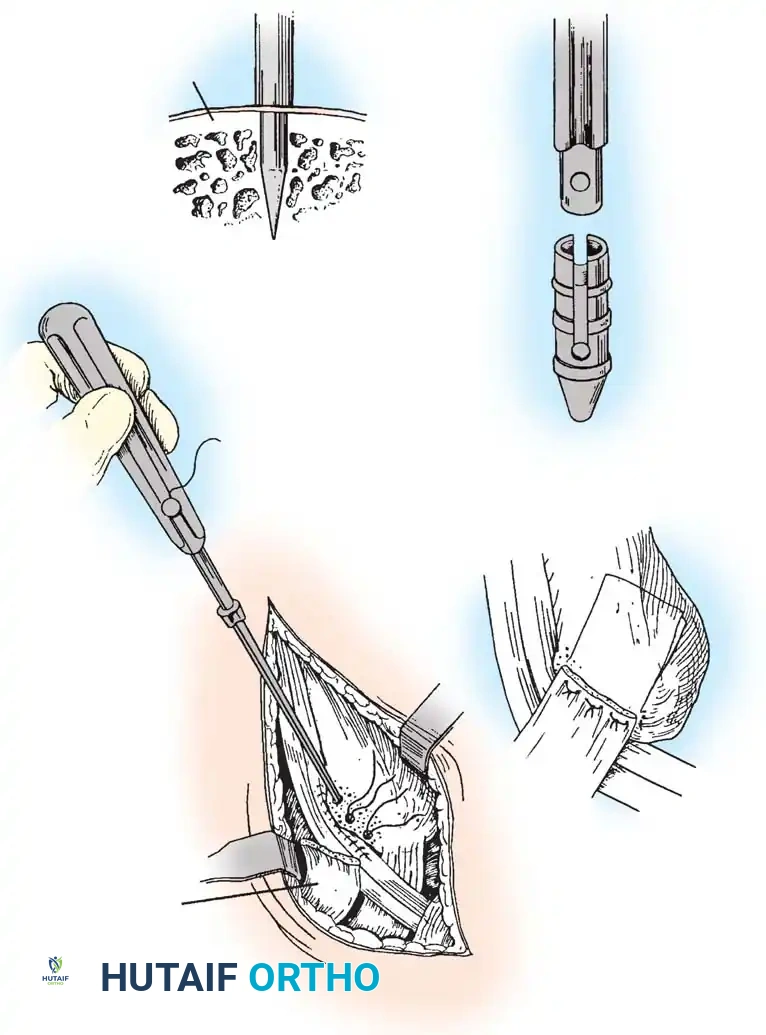
2. Surgical Approach
Begin the incision 10 to 12 cm proximal to the tip of the lateral malleolus, positioned approximately 1 cm posterior to the subcutaneous border of the fibula. Continue the incision distally and slightly obliquely to accommodate the bulbous posterior aspect of the lateral malleolus. Curve the incision gently 1 cm distal to the tip of the lateral malleolus, extending toward the base of the fifth metatarsal for another 3 to 4 cm.
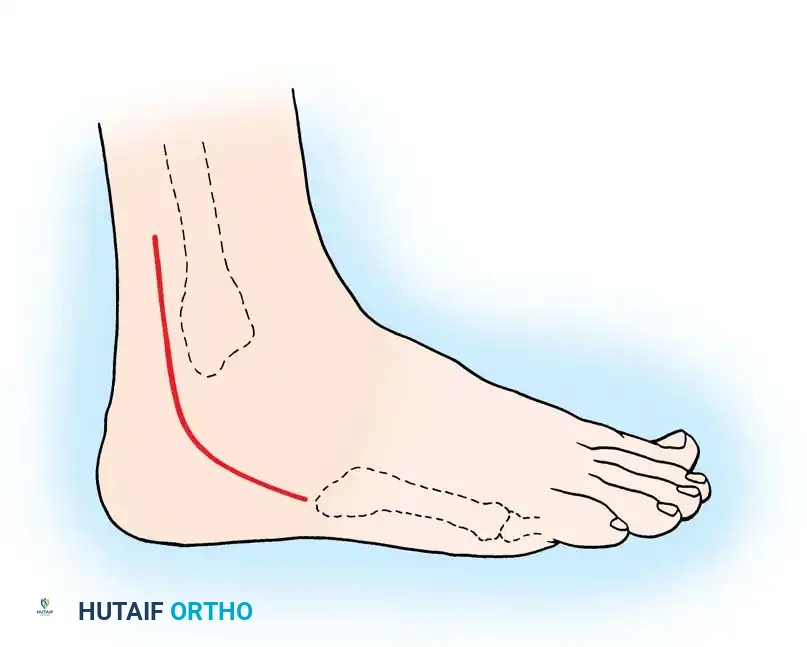
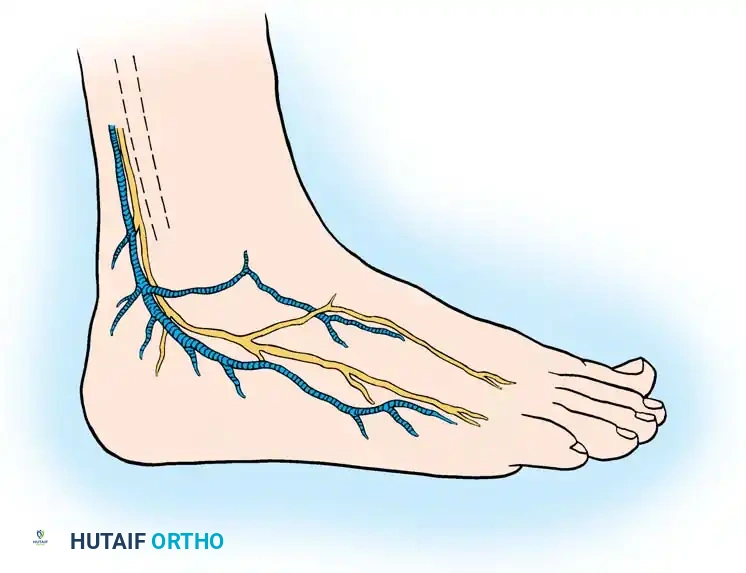
Surgical Pitfall: The sural nerve and the small saphenous vein course just posterior to the peroneal tendons and are strictly subcutaneous at this level. Meticulous dissection is required to avoid iatrogenic neuroma formation, which can be more debilitating than the primary tendon pathology.
3. Retinaculum Release and Exploration
Open the sheath of the peroneal tendons proximally and trace the tendons distally to the superior peroneal retinaculum (SPR).
- If the tendons appear normal both proximal and distal to the SPR, incise only half of the retinaculum (about 1 cm or less) to preserve its stabilizing function.
- If the SPR is thickened or the sheath is fibrotic—suggesting impaired tendon excursion—incise the entire retinaculum and inspect the inferior peroneal retinaculum (IPR). In isolated tenosynovitis, it is unusual to require the release of both retinacula.
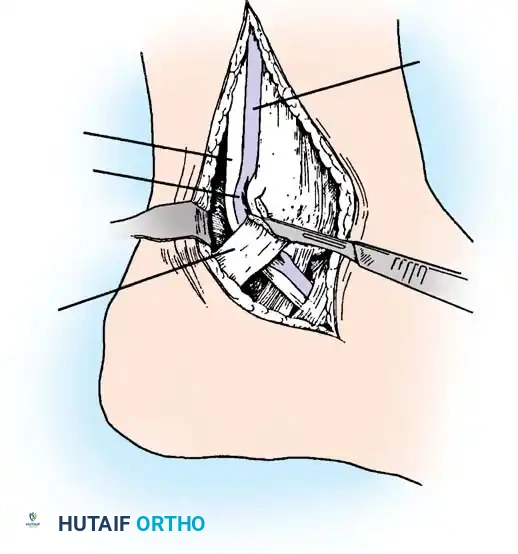
Carefully evaluate the septum that extends from the fibula to the SPR, separating the peroneus longus and brevis. An accessory peroneal tendon (peroneus quartus) may be present in a separate compartment, contributing to overcrowding and stenosis. Release this septum and inspect the peroneus brevis, looking for any accessory slips.
4. Tenosynovectomy and Tendon Debridement
Perform a complete tenosynovectomy, sharply debriding hypertrophic portions of the tendon sheath with a small rongeur or dissecting scissors. The findings at surgery represent a continuum: from clear fluid and relatively normal-appearing tendons, to small linear tears, to thickened, fibrotic sheaths encasing grayish, degenerative tendons.
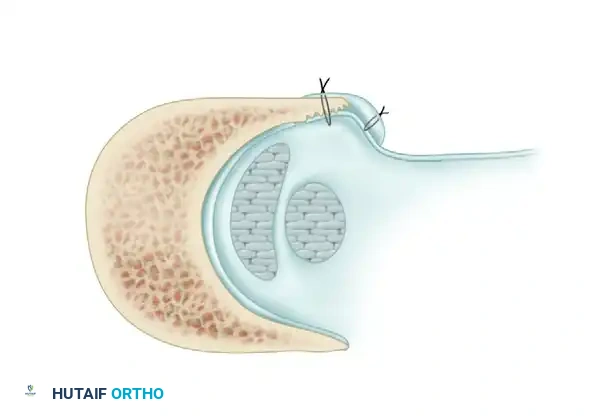
Inspect the tendons meticulously for attritional, longitudinal fissuring. This pathology is most commonly located on the deep (anterior) surface of the peroneus brevis tendon, where it is compressed against the fibula by the overlying peroneus longus.

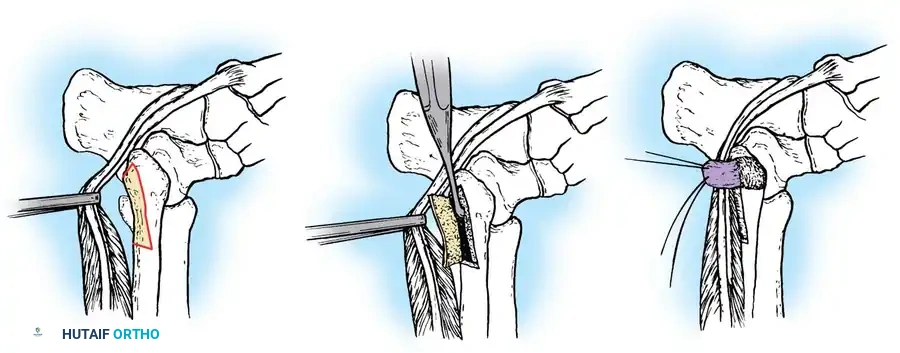
5. Tendon Repair Based on Tear Grade
For Grade I Tears (≤ 50% involvement):
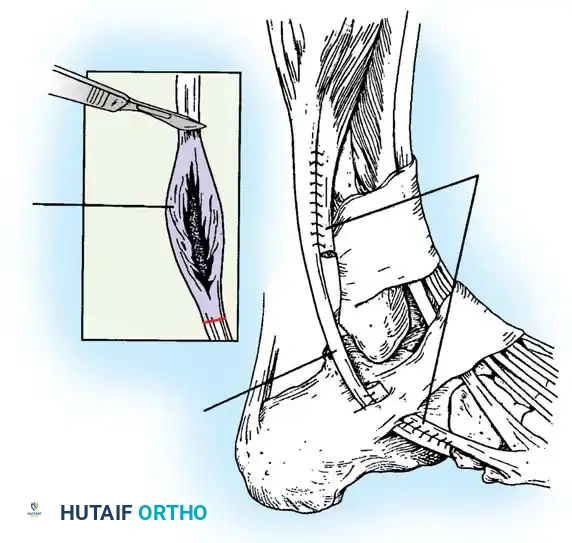
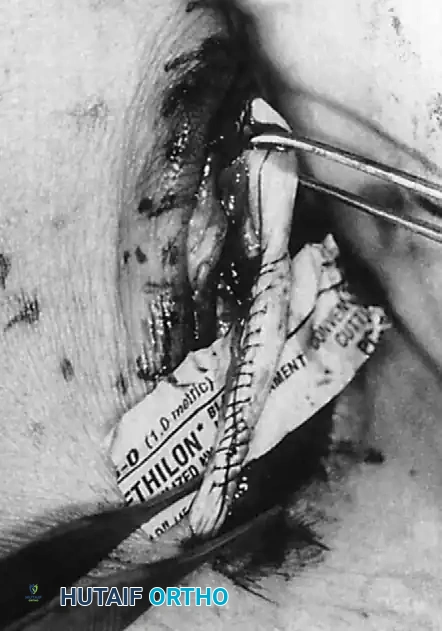
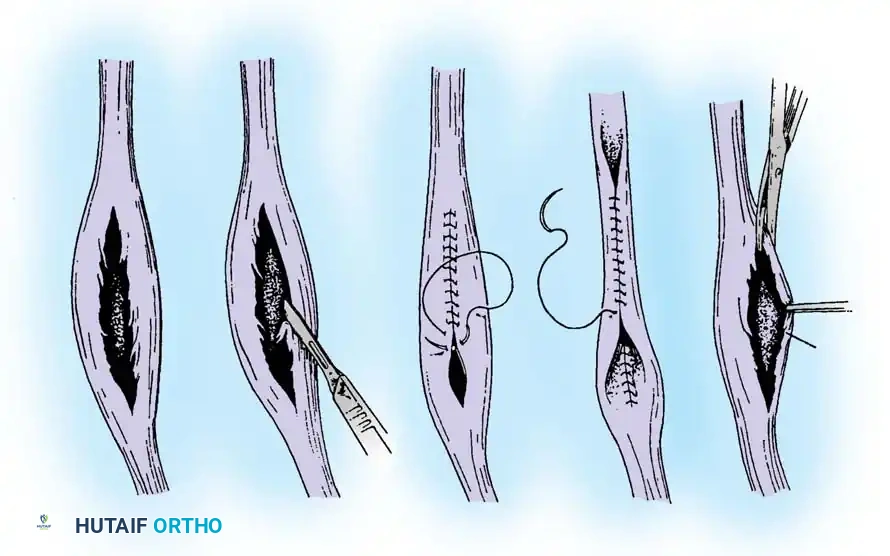
If the tear involves less than 50% of the tendon's cross-sectional area, excise the smaller, degenerative section of the tendon completely. The remaining viable portion is then tubularized to restore a smooth gliding surface. This is achieved using a running 3-0 absorbable, braided suture, burying the knots to minimize friction.
For Grade II Tears (> 50% involvement):
If more than 50% of the peroneus brevis tendon is disrupted and fissured, the remaining section is generally too attenuated to be tubularized effectively. In this scenario, resect the entire diseased segment of the peroneus brevis.
Perform a side-to-side tenodesis of the proximal and distal stumps of the peroneus brevis to the intact peroneus longus tendon.
* The proximal tenodesis should be performed well above the level of the SPR, approximately 3 to 4 cm proximal to the ankle joint, generally at the musculotendinous junction of the peroneus brevis.
* Complete the repair using 2-0 nonabsorbable, braided sutures (e.g., Ethibond or FiberWire), ensuring appropriate tension is maintained to preserve eversion strength.

Note: In the rare event that both the peroneus longus and peroneus brevis tendons have ruptured and cannot be reconstructed locally, a tendon transfer utilizing the flexor digitorum longus (FDL) tendon is indicated, as described by Borton et al.
6. Closure
Distally, leave the tendon sheaths for both the brevis and longus open to prevent postoperative stenosis. Suture the brevis and longus tendons together distally with 2-0 nonabsorbable sutures if a tenodesis was performed.
Repair the superior peroneal retinaculum over the tendons using 2-0 absorbable sutures, ensuring the tendons do not subluxate during passive dorsiflexion and eversion. Leave the remainder of the tendon sheath open. Close the subcutaneous tissues and skin in a standard layered fashion.

Postoperative Protocol and Rehabilitation
Meticulous postoperative care is critical to ensure tendon healing while preventing debilitating stiffness.
Phase I: Immediate Postoperative (0-2 Weeks)
* In the operating room, apply a well-padded posterior plaster splint over a bulky dressing.
* The ankle is immobilized in slight plantarflexion and eversion to remove tension from the repair.
* Strict non-weight-bearing (NWB) status is maintained.
* The patient is seen in the clinic at 2 weeks postoperatively for wound check and suture removal.
Phase II: Intermediate Protection (2-6 Weeks)
* Following suture removal, the patient is transitioned into a CAM boot or a short-leg cast.
* Weight-bearing is gradually advanced based on the extent of the repair (tubularization allows faster progression than tenodesis).
* Gentle active range of motion (ROM) exercises in plantarflexion and dorsiflexion are initiated, avoiding forced inversion.
Phase III: Rehabilitation and Strengthening (6-12 Weeks)
* The CAM boot is weaned, and the patient transitions to supportive footwear, often utilizing an ankle-lacing brace or orthotic with a lateral post if a mild varus tendency persists.
* Formal physical therapy commences, focusing on peroneal strengthening, proprioception, and restoration of full subtalar and tibiotalar kinematics.
* Return to high-impact sports or heavy labor is typically permitted between 3 to 6 months, contingent upon the recovery of symmetric eversion strength and dynamic stability.
Conclusion
Disorders of the peroneal tendons require a high index of suspicion, as they are frequently masked by or concomitant with chronic lateral ankle instability and cavovarus foot deformities. A systematic approach to clinical evaluation, augmented by MRI or dynamic ultrasound, allows for accurate grading of tendon pathology. By adhering to the Krause and Brodsky classification intraoperatively, the orthopedic surgeon can reliably choose between tendon tubular
You Might Also Like