Peroneal Tendon Surgery: Debridement & Tenodesis Guide

Key Takeaway
Peroneal tendon pathology, including tears, os peroneum syndrome, and intrasheath subluxation, requires meticulous surgical management. This guide details the operative techniques for peroneus longus debridement, os peroneum excision, and tenodesis to the peroneus brevis. It provides orthopedic surgeons with step-by-step approaches, biomechanical considerations, and evidence-based postoperative protocols to optimize functional recovery and restore lateral hindfoot stability.
Introduction to Peroneal Tendon Pathology
Disorders of the peroneal tendons encompass a broad spectrum of pathology, ranging from acute traumatic ruptures and superior peroneal retinaculum (SPR) avulsions to chronic stenosing tenosynovitis, longitudinal split tears, and painful os peroneum syndrome (POPS). The peroneus longus (PL) and peroneus brevis (PB) tendons are critical dynamic stabilizers of the lateral hindfoot. The peroneus brevis acts as the primary evertor of the foot, while the peroneus longus plantarflexes the first ray, stabilizing the medial column during the stance phase of gait.
Surgical intervention is indicated when conservative measures—such as immobilization, orthotic management, and targeted physical therapy—fail to relieve pain or restore mechanical stability. This comprehensive guide details the advanced surgical management of three distinct peroneal pathologies: (1) pathology of the peroneus longus and os peroneum, (2) intrasheath peroneal tendon subluxation, and (3) complex ruptures and attritional tears of the peroneal tendons within the retromalleolar groove.
Preoperative Evaluation and Imaging
A meticulous clinical examination is paramount. Patients typically present with posterolateral ankle pain, swelling along the peroneal sheath, and weakness in active eversion. Provocative testing, including resisted eversion in dorsiflexion, may elicit pain or palpable subluxation.
Standard weight-bearing radiographs of the foot and ankle are required to assess for structural malalignment (e.g., varus hindfoot), avulsion fractures of the fibula (fleck sign), and the morphological status of the os peroneum.

Magnetic Resonance Imaging (MRI) is the gold standard for evaluating tendon integrity, identifying longitudinal split tears, tenosynovitis, and anomalous muscle bellies (e.g., peroneus quartus) that may contribute to retromalleolar overcrowding.


Débridement of the Peroneus Longus Tendon, Removal of Os Peroneum, and Tenodesis
The os peroneum is a sesamoid bone located within the substance of the peroneus longus tendon, articulating with the cuboid. Painful os peroneum syndrome (POPS) can result from acute fracture, diastasis of a multipartite os peroneum, or chronic stenosing tenosynovitis at the cuboid tunnel. When the tendon is irreparably damaged or the sesamoid is highly fragmented, excision with subsequent tenodesis is indicated.
Patient Positioning and Preparation
- Positioning: Place the patient in the lateral decubitus position. Utilize a vacuum bean bag to secure the torso and place a sandbag or padded bump under the operative limb to allow unrestricted access to the lateral hindfoot and midfoot.
- Tourniquet: Apply a well-padded thigh tourniquet to ensure a bloodless surgical field, which is critical for identifying fine neurovascular structures and assessing tendon viability. Exsanguinate the limb with an Esmarch bandage prior to inflation.
- Preparation: Prepare and drape the limb in the standard sterile orthopedic fashion.
Surgical Approach
- Incision: Make a longitudinal incision approximately 4 cm in length over the lateral aspect of the foot, following the course of the peroneus longus tendon toward the plantar aspect of the cuboid.
- Neurological Protection:
Surgical Warning: Meticulous superficial dissection is mandatory. The lateral dorsal cutaneous nerve (a terminal branch of the sural nerve) crosses the peroneal tendon sheath in this region. Iatrogenic injury or aggressive retraction can lead to a debilitating postoperative neuroma.
- Deep Exposure: Reflect the abductor digiti quinti muscle and its overlying plantar fascia inferiorly (plantarly). This maneuver exposes the peroneus longus tendon as it courses from the inferior peroneal retinaculum, past the peroneal tubercle of the calcaneus, and into the peroneal tunnel on the lateral plantar aspect of the cuboid.
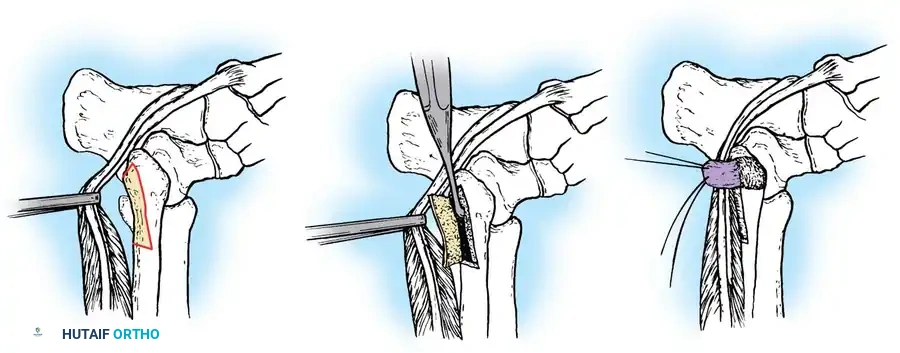
Tendon Débridement and Os Peroneum Excision
- Excision: Identify the os peroneum within the tendon substance. Using sharp dissection, carefully shell out and excise the os peroneum. Attempt to preserve as much continuity of the surrounding tendinous envelope as possible.
- Tenosynovectomy: Inspect the remainder of the peroneus longus tendon. If the tendon architecture appears grossly normal but is surrounded by hypertrophic, inflamed synovium, perform a meticulous tenosynovectomy.
- Repair of Minor Tears: Identify any small, longitudinal split tears in the peroneus longus. Debride the degenerative edges and repair the tendon using a running, locking non-absorbable suture (e.g., 4-0 or 5-0 Prolene) to restore its tubular structure.
- Cuboid Tunnel Decompression: Assess the cuboid tunnel. If the tunnel is constricted and impeding tendon glide, enlarge it. Use a small osteotome and a fine rasp to widen the fibro-osseous canal.
Clinical Pearl: Apply bone wax generously to the newly exposed cancellous bone surfaces within the cuboid tunnel. This critical step minimizes postoperative bleeding and prevents the formation of restrictive fibro-osseous adhesions.
Tenodesis of Peroneus Longus to Peroneus Brevis
If the peroneus longus tendon is severely degenerated, or if excision of a large os peroneum leaves an insufficient tendon bridge for primary repair, a tenodesis must be performed to maintain the biomechanical function of the first ray.
1. Preparation: Debride the diseased segment of the peroneus longus back to healthy, viable tissue.
2. Tenodesis: Perform a side-to-side tenodesis of the proximal stump of the peroneus longus to the adjacent, intact peroneus brevis tendon. Use a robust, non-absorbable braided suture (e.g., #0 or 2-0 FiberWire) in a Krackow or Pulvertaft weave fashion to ensure a biomechanically stable construct.
3. Sheath Management: Leave the peroneal tendon sheath open at the site of the tenodesis to prevent postoperative stenosis and allow for uninhibited tendon excursion.
Closure and Postoperative Protocol
- Closure: Thoroughly irrigate the wound with sterile saline. Deflate the tourniquet and obtain meticulous hemostasis using electrocautery. Close the subcutaneous tissue with absorbable sutures and the skin with non-absorbable sutures or staples.
- Immobilization: Apply a bulky, short-leg, non-weight-bearing (NWB) cast in neutral ankle dorsiflexion and slight eversion to remove tension from the repair.
- Rehabilitation:
- Weeks 0-4: Strict non-weight-bearing in the cast.
- Weeks 4-8: Transition to a controlled ankle motion (CAM) walking boot. Initiate protected, progressive weight-bearing. Begin gentle active range-of-motion (ROM) exercises for the ankle and subtalar joints, avoiding forced inversion.
- Week 8+: Commence formal physical therapy focusing on peroneal strengthening, proprioception, and gait retraining.
Intrasheath Peroneal Tendon Subluxation
Originally described by Bassett in 1985, intrasheath peroneal tendon subluxation is a distinct clinical entity wherein the peroneal tendons subluxate within the intact peroneal tendon sheath, without escaping over the posterior lateral fibular groove.
Pathomechanics and Diagnosis
This phenomenon typically occurs as the foot is brought into active extension and eversion. The peroneus brevis and longus tendons abruptly switch relative positions within the retromalleolar space. On physical examination, a distinct popping or snapping is palpable and audible, yet the tendons remain contained by the superior peroneal retinaculum (SPR).
Surgical Correction Technique
Surgical intervention is highly successful for refractory cases. The procedure is typically performed on an outpatient basis under regional or general anesthesia.
1. Exposure: Expose the superior peroneal retinaculum as described in standard retromalleolar approaches.
2. Retinaculum Modification: To prevent the tendons from rolling over one another, the SPR is modified to create a physical septum. A segment of the SPR (approximately the anterior half) is incised, leaving its posterior attachment intact.
3. Septum Creation: This retinacular flap is mobilized, brought up between the peroneus longus and peroneus brevis tendons, and sutured directly to the posterolateral aspect of the fibula.
4. Outcome: This technique effectively creates two separate, distinct tendon sheaths for the longus and brevis tendons at the proximal level of the SPR, eliminating the space required for intrasheath subluxation. Raikin reported good-to-excellent results in over 90% of patients using this septation technique.
Rupture and Complex Tears of the Peroneal Tendons (Sobel and Bohne Technique)
Peroneal tendons within the retromalleolar groove are highly susceptible to longitudinal split tears, particularly the peroneus brevis, which is compressed between the fibula and the peroneus longus during forced dorsiflexion and eversion. Chronic tears lead to tendon thickening, tenosynovitis, and limited excursion.
Patient Positioning and Exposure
- Positioning: Position the patient supine on the operating table. Place a large sandbag or bump under the ipsilateral greater trochanter to internally rotate the leg, bringing the lateral malleolus into direct view.
- Incision: Make a curved 7-cm incision through the skin and subcutaneous tissue, following the posterior third of the fibula, slightly off its central prominence to avoid placing the scar directly over the bone.
- Flap Elevation: Expose the superior peroneal retinaculum (SPR) and elevate full-thickness fasciocutaneous flaps.
- Dynamic Assessment: Before incising the SPR, dynamically assess the tendons. Subluxation of the anterior portion of the peroneus brevis tendon can sometimes be visualized or palpated beneath the exposed SPR. Determine the competence and laxity of the retinaculum.
Tendon Inspection and Debridement
- Sheath Incision: Sharply incise the peroneal sheath near its anterior attachment to the fibula. This preserves the posterior tissue for later repair.
Surgical Warning: Do not violate the synovial and vascular attachments (the mesotenon) located on the posterior aspect of the peroneal tendons. The blood supply to the tendons is tenuous in this watershed zone; devascularization will compromise healing and lead to further degeneration.
- Tendon Assessment: Apply proximal traction on the peroneus longus tendon. This maneuver often exacerbates and reveals the subluxation of the anterior portion of a split peroneus brevis tendon.
- Repair of Peroneus Brevis: Inspect the peroneus brevis tendon thoroughly. If attrition or a longitudinal split is evident, meticulously debride the attenuated, degenerative intrasubstance tissue. Repair and tubulate the remaining healthy tendon using a running 4-0 non-absorbable suture.
Management of Retromalleolar Overcrowding
A critical step in peroneal tendon surgery is addressing the underlying anatomical factors that caused the tear. Overcrowding in the fibular groove places excessive stress on the SPR and the tendons.
1. Low-Lying Muscle Belly: If the peroneus brevis muscle belly extends distally into the retromalleolar groove (a "low-lying" muscle belly), resect the distal muscle tissue to create more space for the tendons.
2. Peroneus Quartus: Look for an anomalous peroneus quartus muscle/tendon complex. If present and encroaching on the fibular groove, it must be excised. Failure to identify and remove anomalous tissue allows an overpacking phenomenon that will inevitably lead to surgical failure and recurrent symptoms.
Advanced Surgical Treatment Options
Depending on the severity of tendon degeneration encountered, several advanced reconstructive options may be necessary:
1. Tenodesis: Excision of a severely diseased, non-reconstructable segment of the peroneus brevis, followed by suturing the proximal and distal stumps to the adjacent intact peroneus longus tendon.
2. Resection in Continuity: Resection of a localized, thickened, degenerative nodule of the peroneus brevis tendon, leaving the remaining tendon in continuity if sufficient cross-sectional area remains.
3. Tendon Weaving (Chrisman-Snook Modification): Utilizing the anterior half of a split peroneus brevis tendon to perform a lateral ankle ligament reconstruction (e.g., modified Chrisman-Snook procedure) if concomitant chronic lateral ankle instability is present.
4. Flexor Hallucis Longus (FHL) Transfer: For massive, irreparable combined tears of both the peroneus brevis and longus tendons, a tendon transfer is required. The FHL is the preferred graft. This may require a staged approach: inserting a silicone Hunter rod into the peroneal sheath during the first stage to create a proper gliding tunnel, followed by the definitive FHL tendon transfer in a second procedure.
Superior Peroneal Retinaculum (SPR) Reconstruction
To prevent postoperative subluxation, the SPR must be securely repaired, and the retromalleolar groove may need to be deepened.
1. Groove Deepening: Inspect the posterior aspect of the fibula. If the groove is shallow or convex, or if there is a sharp posterior ridge, use a rongeur and a high-speed burr or file to remove the sharp ridge and smooth the area. This creates a fresh, concave bony bed.
2. SPR Advancement: Advance the superior peroneal retinaculum into this fresh bony bed on the posterior aspect of the fibula. Secure the SPR using transosseous drill holes or small suture anchors. Careful, tensioned anatomical reconstruction of this structure is imperative to ensure the absolute stability of the tendons within the groove during active eversion.
Postoperative Care for Retromalleolar Reconstruction
Postoperative management mirrors that of the tenodesis protocol but requires strict adherence to immobilization to protect the SPR repair. Patients are placed in a non-weight-bearing cast for 4 to 6 weeks, followed by transition to a CAM boot with progressive weight-bearing. Inversion and eversion strengthening are delayed until 6 to 8 weeks postoperatively to ensure the retinacular repair has achieved sufficient tensile strength. Return to high-impact sports or heavy labor is typically anticipated between 4 to 6 months following surgery.
You Might Also Like