Mastering the Surgical Management of Chronic Unreduced Patellar and Hip Dislocations
Key Takeaway
Chronic unreduced dislocations of the patella and hip present complex reconstructive challenges. Management requires a thorough understanding of adaptive biomechanics, soft-tissue contractures, and articular cartilage viability. Treatment ranges from observation and open reduction to complex osteotomies and arthroplasty. This guide details evidence-based surgical techniques, including patellar realignment, intertrochanteric osteotomies for anterior hip dislocations, and heavy traction protocols for neglected posterior hip dislocations, optimizing functional outcomes in delayed presentations.
INTRODUCTION TO CHRONIC UNREDUCED DISLOCATIONS
The management of chronic, unreduced (neglected) dislocations represents a formidable challenge in orthopedic surgery. Unlike acute dislocations, where the primary goal is immediate concentric reduction to preserve articular cartilage and vascularity, chronic dislocations are complicated by adaptive soft-tissue contractures, capsular fibrosis, articular degeneration, and profound biomechanical alterations. This comprehensive guide explores the pathoanatomy, clinical evaluation, and advanced surgical techniques required to manage old unreduced dislocations of the patellofemoral and coxofemoral joints.
CHRONIC UNREDUCED PATELLAR DISLOCATIONS
Old unreduced dislocations of the patella following trauma are exceedingly rare in modern practice but must be meticulously distinguished from congenital patellar dislocations. The distinction is critical, as the underlying pathoanatomy and subsequent surgical algorithms differ significantly.
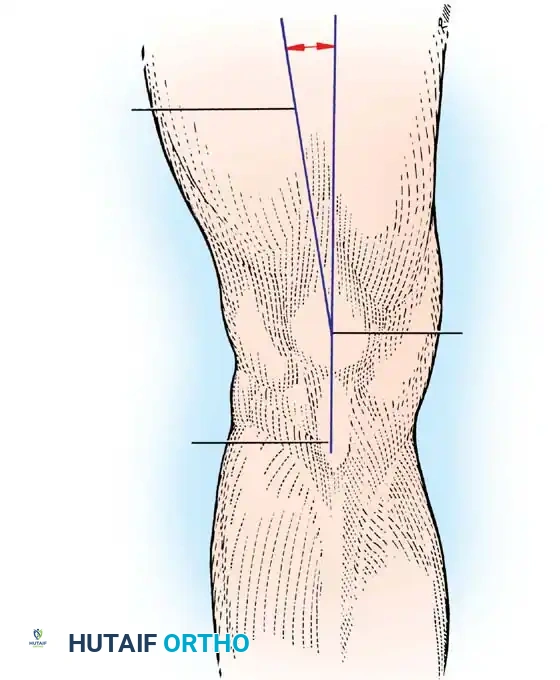
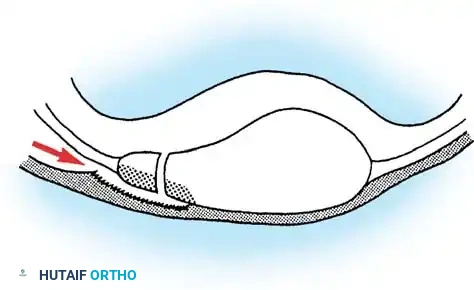
Congenital dislocations often go unrecognized in infancy because normal patellar ossification does not occur until approximately 3 years of age. The congenital lesion is characterized by primary dysplasia: a flexion contracture of the knee, severe incongruity of the patella and trochlea, and an obligate lateral tracking mechanism that is part of the original pathological process. Conversely, in posttraumatic chronic dislocations, the anatomical abnormalities are secondary. An adaptive flattening of the patellar articular surface occurs due to the loss of normal compressive forces within the trochlear groove, and the associated knee flexion contracture is a reactive, rather than primary, change.
Clinical Pearl: A high index of suspicion must be maintained in the setting of multiligamentous knee injuries. Literature indicates that up to 16% of traumatic patellar dislocations are missed when an associated tibiofemoral knee dislocation is present, particularly when the medial structures (e.g., medial patellofemoral ligament, medial collateral ligament) have been catastrophically disrupted.
Treatment Rationale and Indications
The treatment of old traumatic patellar dislocations is dictated by the duration of the dislocation, the severity of patellofemoral arthritis, and the functional demands of the patient. Options include:
1. Observation: If the knee functions satisfactorily despite the unreduced patella, observation is the treatment of choice.
2. Open Reduction and Realignment: Indicated for dislocations of relatively short duration where degenerative changes of the patella are minimal, and the tibiofemoral joint remains essentially normal.
3. Patellectomy or Patellaplasty: Indicated in long-standing dislocations where severe traumatic arthritis has developed, resulting in limited motion, intractable pain, and profound disability. Note that patellar resurfacing or isolated patellar prostheses are generally not recommended for this specific condition due to the high risk of failure and altered extensor mechanism kinematics.
Surgical Warning: The long-term prognosis for restoring entirely normal knee function is guarded regardless of the procedure selected. Extensive patient counseling regarding expectations is mandatory.
Open Reduction and Extensor Realignment Technique
This procedure aims to restore the anatomical tracking of the extensor mechanism while addressing the contracted lateral structures and the attenuated medial restraints.
Preoperative Preparation and Positioning:
* The patient is placed supine on a radiolucent operating table.
* A high thigh tourniquet is applied but not inflated until exsanguination is complete.
* The limb is prepped and draped free to allow full range of motion during intraoperative tracking assessment.
Surgical Steps:
* Incision and Exposure: Make a longitudinal midline incision approximately 7.5 cm long, centered over the patella and extending from the distal quadriceps tendon to the tibial tubercle.
* Lateral Dissection: Dissect laterally deep to the subcutaneous tissue to expose the contracted lateral retinaculum and joint capsule.
* Lateral Release: Incise the capsule and synovium over the patella parallel with the lateral border of the quadriceps tendon. This release must be extensive enough to allow the patella to be mobilized medially without excessive tension.
* Mobilization: Free the deep surfaces of the quadriceps tendon and the patella from underlying adhesions. Carefully elevate the extensor mechanism and place these structures into their normal anatomical positions within the trochlear groove.
* Medial Plication: Excise the redundant, attenuated portion of the capsule from the medial side of the knee. Close the capsule on this side under appropriate tension to act as a static medial restraint.
* Dynamic Realignment (VMO Advancement): It is critical that the general alignment of the extensor mechanism be normalized at the completion of the procedure to prevent lateral redislocation. The fibers of the vastus medialis obliquus (VMO) muscle must be appropriately oriented. This often requires the distal and lateral advancement of the VMO, reattaching a portion of the muscle to the adductor tubercle of the femur and the superomedial pole of the patella.
* Distal Realignment: If the Q-angle remains abnormal or lateral tracking persists despite proximal soft-tissue balancing, transfer the tibial tuberosity medially (e.g., Elmslie-Trillat procedure) to realign the distal portion of the extensor mechanism.
* Management of Degeneration: If the articular surface of the patella is found to be severely degenerated upon exposure, a patellectomy or patellaplasty must be performed concurrently. Crucially, realignment of the extensor mechanism is just as important after a patellectomy as it is after an open reduction to ensure central tracking of the quadriceps tendon.
Postoperative Protocol:
The knee is immobilized in a hinged knee brace locked in extension. Isometric quadriceps exercises are initiated immediately. Gradual flexion is introduced based on the tension of the medial repair, typically allowing 0-30 degrees in the first two weeks, progressing slowly to prevent stretching of the medial plication.
CHRONIC UNREDUCED HIP DISLOCATIONS
Old unreduced dislocations of the hip are relatively uncommon in adults in developed nations but remain a frequent presentation in developing countries. They are typically the result of high-energy motor vehicle accidents accompanied by distracting injuries—such as traumatic brain injury, ipsilateral femoral fractures, or contralateral pelvic/hip injuries—which draw clinical attention away from the dislocated hip.
Treatment of chronic hip dislocations is highly complex and depends heavily on the viability of the femoral head, the condition of the acetabulum, and the duration of the dislocation. Treatment modalities include closed reduction, open reduction, heavy skeletal traction and abduction, subtrochanteric osteotomy, Girdlestone resection arthroplasty, arthrodesis, and total hip arthroplasty (THA).
Chronic Unreduced (Old) Anterior Dislocations
Traumatic anterior dislocations of the hip are comparatively rare, accounting for less than 10% of all hip dislocations. Consequently, chronic unreduced anterior dislocations are exceedingly rare, and literature is limited primarily to case series. The primary goal of surgery in these neglected cases is to correct the severe external rotation and abduction deformity to improve body mechanics, gait, and overall balance.
Intertrochanteric Osteotomy (Aggarwal and Singh)
For patients where open reduction is deemed impossible or the femoral head is severely deformed, a compensatory intertrochanteric osteotomy can realign the mechanical axis of the lower extremity.
Surgical Steps:
* Approach: The hip is approached via the Gibson (posterolateral) approach, allowing excellent visualization of the intertrochanteric region.
* Osteotomy: The femur is divided along the intertrochanteric line joining the greater and lesser trochanters.
* Realignment: The distal femoral fragment is then adducted, extended, and internally rotated to correct the clinical deformity. Rigid internal fixation (e.g., dynamic hip screw or blade plate) is applied to maintain the correction.
Postoperative Protocol:
Historically, patients were kept in skin traction for 6 weeks to prevent recurrence of the rotational deformity. Modern rigid fixation may allow for earlier mobilization. The patient is allowed to walk with crutches 6 weeks postoperatively, with full weight-bearing permitted at 3 to 4 months once radiographic union is confirmed.
Modified Subcapital Displacement Osteotomy (Nagi)
Nagi et al. described a modified Girdlestone arthroplasty designed to preserve proximal femoral bone stock for future THA, indicated for neglected anterior dislocations present for 6 months or more in young patients.
Surgical Steps:
* Approach: The femoral neck is exposed through an anterior Smith-Petersen or a Watson-Jones anterolateral approach.
* Osteotomy: A subcapital osteotomy is performed. The surgeon must attempt to leave as much of the femoral neck as possible with the distal fragment, without disturbing the incarcerated femoral head.
* Displacement: By manipulating the leg, the cut proximal end of the femoral neck is displaced upward and seated directly into the empty acetabulum.
Postoperative Protocol:
Postoperative skeletal traction of 5 kg is maintained for 6 weeks. Gentle active hip flexion is initiated 10 days postoperatively. Non-weight-bearing ambulation with crutches begins at 6 weeks, with gradual weight-bearing at 3 months. This temporizing procedure provides a stable, albeit shortened, limb while preserving the femoral neck to facilitate a definitive total hip arthroplasty later in life.
Chronic Unreduced (Old) Posterior Dislocations
Unreduced posterior dislocations are significantly more common than anterior dislocations. The prognosis and treatment algorithm are heavily influenced by the presence of associated fractures and the vascular status of the femoral head.
Classification and Prognostic Factors:
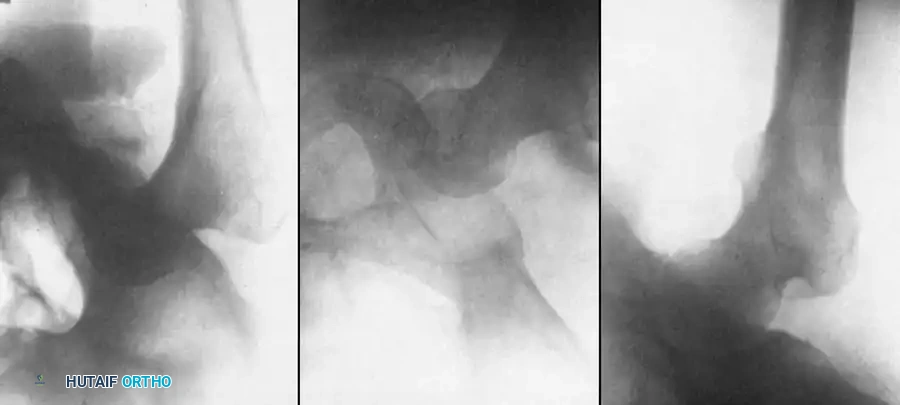
Garrett et al. utilized the Thompson and Epstein classification for old unreduced posterior dislocations. They identified two primary factors contributing to poor outcomes:
1. Fractures: Fracture of the femoral head or medial acetabular wall (Epstein types IV and V).
2. Osteonecrosis (AVN): An unpredictable complication that may not manifest on plain radiographs for many months.
Clinical Pearl: The viability of the femoral head is the single most critical determinant in the treatment algorithm for old unreduced posterior dislocations. Advanced imaging, specifically MRI or a Technetium-99m bone scan, is mandatory to assess femoral head vascularity before initiating any joint-preserving treatment.
Management of Type I Dislocations (No significant fracture)
If the dislocation is less than 12 weeks old and the femoral head is viable, a closed reduction under general anesthesia with profound muscle relaxation may be attempted. However, after 12 weeks, the acetabulum typically fills with dense fibrofatty tissue, making a concentric closed reduction virtually impossible.
If closed reduction fails or the dislocation is older than 12 weeks, heavy skeletal traction and abduction (as described by Gupta) should be considered.
Heavy Traction and Abduction Technique (Gupta)
This technique utilizes sustained, heavy traction to overcome severe soft-tissue contractures and gradually pull the proximally migrated femoral head down to the level of the acetabulum.
Surgical Steps:
* Pin Placement: Place a heavy threaded Steinmann pin in the proximal tibia in the region of the tibial tubercle.
* Initial Traction: Place the patient in 18 kg (approx. 40 lbs) of longitudinal skeletal traction. The patient must be kept strictly in bed, under adequate sedation, and provided with muscle relaxants to tolerate this massive force.
* Monitoring: Obtain anteroposterior radiographs of the pelvis on alternate days. Usually, by the fifth day, the femoral head will have descended to or below the level of the acetabulum.
* Reduction Maneuver: Once the head is at the appropriate level, gradually abduct the limb and reduce the traction weight by 3.6 kg every fourth day. The vector of traction combined with abduction guides the head into the acetabulum.
* Maintenance: Once concentric reduction is confirmed radiographically, maintain 7 kg of traction for the next 2 weeks to allow soft-tissue healing and prevent redislocation.
Postoperative Protocol:
Remove the traction after 2 weeks and begin non-weight-bearing range-of-motion exercises for the next 4 weeks. Strict non-weight-bearing is enforced for a total of 3 months to protect the vulnerable articular cartilage and allow revascularization.
Surgical Warning: The success of the heavy traction technique depends entirely on achieving a concentric reduction. If the reduction is nonconcentric (due to interposed capsule, labrum, or osteochondral fragments), an open reduction is mandatory to meticulously débride the acetabulum. Accepting a nonconcentric reduction universally leads to rapid joint destruction and poor clinical outcomes.
Open Reduction and Internal Fixation (ORIF)
For posterior dislocations with a viable femoral head complicated by large uncomminuted (Type II) or comminuted (Type III) fractures of the posterior acetabular rim, ORIF is indicated if the injury is less than 3 months old.
* If the femoral head is displaced superiorly, a period of preoperative skeletal traction is necessary to stretch the contracted abductors and neurovascular structures.
* Open reduction is performed (typically via a Kocher-Langenbeck approach) to clear the acetabulum of fibrous tissue, reduce the femoral head, and internally fix the posterior wall fragments with reconstruction plates and screws to restore posterior stability.
Salvage Procedures: Arthroplasty and Arthrodesis
Primary reconstructive salvage procedures are indicated for:
* Type IV (fracture of the acetabular rim and floor) or Type V (fracture of the femoral head) dislocations present for more than 3 months.
* Any chronic dislocation where the femoral head is proven avascular on MRI or bone scan.
Total Hip Arthroplasty (THA):
THA provides the best functional results for chronic, destructive dislocations. However, the surgeon must be prepared for profound technical challenges. The primary obstacle is the creation of adequate acetabular bone stock, especially when the posterior lip is fractured, dysplastic, or resorbed. This often requires complex reconstruction using the excised femoral head as a structural autograft (fixed with cancellous screws) to support the acetabular component, alongside the use of multi-hole revision shells.
Arthrodesis:
In very young, heavy laborers with unilateral hip destruction, hip arthrodesis remains a viable option. However, achieving a solid fusion is notoriously difficult in the presence of osteonecrosis. Furthermore, the surgeon must carefully evaluate the status of the ipsilateral knee, the contralateral hip, and the lumbar spine, as arthrodesis places significantly increased biomechanical stress on these adjacent joints.
Subtrochanteric Osteotomy:
In regions where arthroplasty implants are unavailable, or in patients with active infection precluding arthroplasty, a subtrochanteric osteotomy (e.g., Schanz osteotomy) can be utilized. This is indicated for patients who are relatively pain-free and possess a reasonable range of hip flexion but suffer from severe adduction contractures or significant limb-length inequality. The osteotomy realigns the limb, improves the abductor lever arm, and provides a stable platform for weight-bearing.
You Might Also Like