Wrist Arthrodesis: Comprehensive Surgical Principles and Techniques
Key Takeaway
Wrist arthrodesis is a highly effective salvage procedure indicated for severe wrist flexion contractures in nonfunctional hands. Primarily utilized to control position and facilitate hygiene, the procedure often incorporates a proximal row carpectomy to correct deformity and supply autologous bone graft. To prevent physeal arrest, fusion is delayed until skeletal maturity. This guide details the step-by-step surgical technique, including the dorsal approach, cartilage denudation, and Steinmann pin fixation for optimal outcomes.
Introduction to Total Wrist Arthrodesis
Total wrist arthrodesis is a highly reliable and definitive salvage procedure in orthopedic surgery, designed to provide stability, correct severe deformity, and alleviate pain in the radiocarpal and intercarpal joints. While frequently employed for end-stage post-traumatic arthritis, rheumatoid arthritis, and paralytic conditions, its application in the severely contracted, nonfunctional hand represents a unique and challenging clinical scenario.
In patients presenting with a severe wrist flexion contracture and a nonfunctional hand—often secondary to cerebral palsy, severe traumatic brain injury, stroke, or advanced Volkmann ischemic contracture—the primary goal of surgery shifts from restoring fine motor kinematics to facilitating basic patient care. In these complex cases, wrist arthrodesis is utilized primarily to control the resting position of the limb, prevent skin maceration, and dramatically improve hygiene in a hand with poor motor control and absent or diminished sensibility.
This comprehensive guide details the indications, biomechanical considerations, preoperative planning, and step-by-step surgical execution of wrist arthrodesis using Steinmann pin fixation, specifically tailored for the severely contracted wrist.
Indications and Patient Selection
The decision to proceed with a total wrist arthrodesis in a nonfunctional hand must be made after careful multidisciplinary evaluation. The procedure is indicated when conservative measures, such as aggressive splinting, botulinum toxin injections, and physical therapy, have failed to prevent progressive deformity.
Primary Indications
- Severe Flexion Contractures: Fixed deformities that preclude passive extension to neutral, often resulting in the fingers being driven into the palm.
- Hygiene and Nursing Care: Inability to clean the palmar crease, leading to recurrent fungal infections, skin maceration, and breakdown.
- Cosmesis and Positioning: Improving the overall appearance of the limb, which provides significant psychological benefit to the patient and caregivers.
- Spasticity Management: Providing a stable skeletal platform to counteract severe flexor spasticity.
💡 Clinical Pearl: The Functional vs. Nonfunctional Hand
It is critical to distinguish between a hand with residual functional capacity and a truly nonfunctional hand. In a functional hand, arthrodesis position is dictated by grip strength optimization (typically 10° to 15° of extension). In the nonfunctional, spastic hand, the goal is purely positional and hygienic; therefore, neutral or even slight flexion is preferred to avoid excessive tension on the neurovascular structures during deformity correction.
Preoperative Planning and Timing
Physeal Considerations in the Pediatric Patient
A critical limitation in the timing of wrist arthrodesis is the skeletal maturity of the patient. The distal radial physis is responsible for approximately 75% of the longitudinal growth of the radius.
🚨 Surgical Warning: Timing of Arthrodesis
Because the surgical preparation of the radiocarpal joint inevitably damages the epiphysis of the distal radius, fusion must be delayed until the patient is at least 12 years old (or until skeletal maturity is confirmed radiographically). Premature arthrodesis will result in complete physeal arrest, leading to severe ulnar positive variance, distal radioulnar joint (DRUJ) dislocation, and a progressive, painful Madelung-type deformity.
Biomechanics and Optimal Positioning
The ideal position for wrist arthrodesis in this specific patient population is neutral flexion and slight ulnar deviation.
* Neutral Flexion: Aligns the metacarpals with the longitudinal axis of the radius. While slight extension is favored in functional hands to maximize the tenodesis effect for grip, neutral positioning in the spastic hand minimizes the risk of median nerve stretch neuropathy and skin necrosis over the volar wrist crease following the correction of a severe flexion contracture.
* Mild Flexion Tolerance: In cases of extreme, long-standing contracture where bringing the wrist to neutral places undue tension on the volar neurovascular bundle, a mild degree of flexion is well tolerated and often safer.
* Ulnar Deviation: A slight ulnar deviation (5° to 10°) follows the natural resting cascade of the hand and improves the cosmetic appearance of the limb.
Surgical Anatomy and Approaches
The procedure utilizes a standard dorsal longitudinal approach to the wrist. A thorough understanding of the extensor compartments is essential for adequate exposure and subsequent soft tissue coverage of the fusion site.
- Incision: Centered over the Lister tubercle, extending from the distal third of the radius to the base of the third metacarpal.
- Extensor Retinaculum: The third dorsal compartment is opened to transpose the extensor pollicis longus (EPL) tendon radially. The second compartment (ECRL, ECRB) and fourth compartment (extensor digitorum communis) are elevated subperiosteally to expose the dorsal radiocarpal ligaments and the joint capsule.
- Neurovascular Structures: The superficial sensory branch of the radial nerve and the dorsal sensory branch of the ulnar nerve must be meticulously protected during the superficial dissection.
Step-by-Step Surgical Technique (Technique 72-7)
The following technique describes wrist arthrodesis utilizing Steinmann pin fixation, which is particularly advantageous in spastic patients with poor bone stock or when a proximal row carpectomy (PRC) is performed, making standard dorsal plate application technically challenging.
1. Soft Tissue Release and Preparation
- Place the patient supine with the operative arm on a hand table. Apply a well-padded proximal tourniquet.
- Before addressing the skeletal deformity, evaluate the flexor tendons. In severe spasticity, fractional lengthening of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP), or a flexor pronator slide, may be necessary to allow the wrist to be brought out of flexion.
- Perform these releases as necessary before proceeding to the dorsal skeletal work.
2. Dorsal Approach and Exposure
- Make a dorsal longitudinal incision over the wrist, centered over the radiocarpal joint.
- Incise the extensor retinaculum over the third dorsal compartment. Retract the EPL tendon radially.
- Elevate the second and fourth extensor compartments subperiosteally, raising thick, full-thickness flaps of the dorsal capsule to expose the radiocarpal and midcarpal joints.
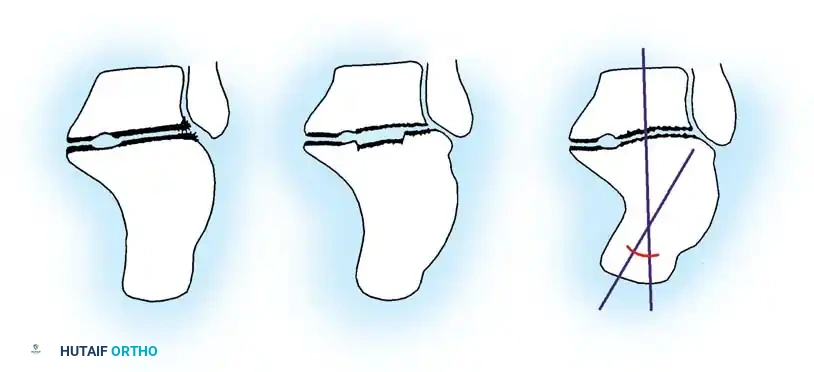
3. Proximal Row Carpectomy (PRC)
A proximal row carpectomy is typically incorporated with the fusion in these severe cases.
* Rationale: Excising the proximal carpal row (scaphoid, lunate, and triquetrum) effectively shortens the skeletal column of the wrist. This skeletal shortening is paramount; it allows the severe flexion contracture to be corrected without placing catastrophic stretch on the median nerve or requiring massive, morbid flexor tendon lengthenings.
* Execution: Use a combination of sharp dissection, elevators, and rongeurs to excise the proximal row. Take care to protect the volar radiocarpal ligaments to maintain a soft tissue hinge.
4. Joint Preparation and Cartilage Denudation
- To achieve a solid arthrodesis, all remaining articular cartilage must be meticulously removed down to bleeding subchondral bone.
- Denude the cartilage from the distal radius (scaphoid and lunate fossae), the proximal surfaces of the distal carpal row (capitate and hamate), and the intercarpal joints.
- Extend the preparation distally to include the second and third carpometacarpal (CMC) joints to ensure a rigid, unified block from the radius to the metacarpals.
5. Bone Grafting
- Autograft Utilization: The excised proximal carpal bones (scaphoid, lunate, triquetrum) serve as an excellent source of local corticocancellous autograft.
- Use a rongeur to morselize these bones. Pack the corticocancellous portions tightly into the decorticated radiocarpal, intercarpal, and CMC spaces to supplement the fusion mass.
- If the local bone graft is insufficient (e.g., due to severe osteopenia or cystic changes), harvest supplemental cancellous graft from the ipsilateral iliac crest.
6. Skeletal Fixation
Once the wrist is reduced into the optimal position (neutral flexion, slight ulnar deviation), rigid fixation is achieved using heavy Steinmann pins.
- Transfix the carpus with two stout Steinmann pins measuring 7/64 to 9/64 of an inch in diameter.
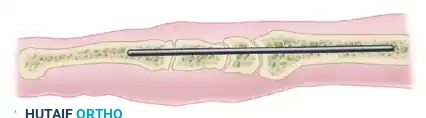
- The pins are typically driven in a retrograde fashion. Introduce the pins through the dorsal aspect of the second and third metacarpals, driving them proximally across the prepared carpal mass and seating them deeply into the medullary canal of the distal radius.
FIGURE 72-10 (A): Lateral schematic demonstrating the longitudinal trajectory of the Steinmann pin traversing the metacarpal, the remaining carpus, and seating securely within the medullary canal of the radius.
- Ensure the pins cross the fusion sites at divergent angles to maximize rotational stability.
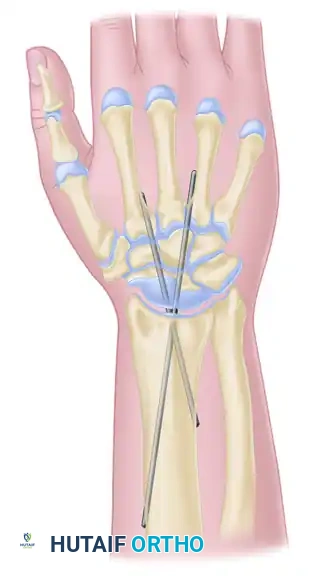
FIGURE 72-10 (B): Anteroposterior (AP) schematic illustrating wrist arthrodesis using two crossed Steinmann pins, providing rigid stabilization of the radiocarpal and midcarpal intervals.
- Cut the pins beneath the skin to prevent pin tract infections, or leave them protruding slightly if early removal in the clinic is planned (though buried pins are generally preferred in spastic patients to prevent self-injury or hardware back-out).
- Close the dorsal capsule meticulously over the fusion site and hardware, followed by routine skin closure.
Postoperative Care and Rehabilitation Protocol
Rigid postoperative immobilization is critical, as Steinmann pins provide less absolute stability than a dorsal spanning plate. The spasticity of the flexor musculature will constantly challenge the fixation.
Immediate Postoperative Phase (Weeks 0-4)
- Apply a well-padded, bivalved long-arm cast in the operating room.
- Positioning: The elbow must be immobilized at 90 degrees of flexion to control forearm rotation. The forearm is maintained in neutral pronation and supination.
- Finger Inclusion: If the finger flexors (FDS/FDP) have been lengthened during the procedure, extend the volar aspect of the cast to include the fingers in an extended position. This prevents the spastic flexors from contracting and compromising the tendon lengthening.
- Elevate the limb strictly for the first 48 to 72 hours to mitigate postoperative edema.
Intermediate Phase (Weeks 4-8)
- At 4 weeks postoperatively, the patient is evaluated in the clinic. Radiographs are obtained to assess hardware position and early callus formation.
- If clinical progression is satisfactory, the long-arm cast can be converted to a short-arm cast.
- At this stage, finger flexion is permitted and encouraged to prevent profound stiffness of the metacarpophalangeal (MCP) and interphalangeal (IP) joints, provided the flexor tendon lengthenings have healed sufficiently.
Late Phase (Weeks 8-12+)
- Immobilization is typically continued for a total of 8 to 12 weeks, or until definitive radiographic union is observed (bridging trabeculae across the radiocarpal and intercarpal joints).
- Once union is achieved, the cast is removed. A removable thermoplastic splint may be used for an additional 2 to 4 weeks during periods of high activity or severe spastic episodes.
- If the Steinmann pins were left prominent or become symptomatic under the skin after fusion is complete, they may be removed in a minor outpatient procedure.
Complications and Pitfalls
While highly effective, wrist arthrodesis in the spastic, nonfunctional hand carries specific risks that the surgeon must anticipate.
- Nonunion / Pseudarthrosis: The most common complication, particularly at the radiocarpal junction. Meticulous cartilage denudation and aggressive bone grafting are the best prevention. If an asymptomatic nonunion occurs in a nonfunctional hand, revision is rarely necessary unless it results in recurrent deformity or pain.
- Hardware Migration: Spasticity places immense bending and pull-out forces on the Steinmann pins. Pins may migrate proximally or distally. Routine radiographic surveillance is required.
- Median Nerve Neuropathy: Attempting to correct a severe, long-standing flexion contracture to neutral without performing a proximal row carpectomy (PRC) or adequate flexor lengthening can acutely stretch the median nerve, leading to ischemia and severe neuropathic pain.
- Wound Breakdown: The dorsal skin is thin and susceptible to necrosis, especially if the wrist is forced into extension or if the hardware is prominent. Meticulous capsular closure and tension-free skin approximation are mandatory.
You Might Also Like