Traditional Triple Arthrodesis: Fixing Severe Foot Deformity

Key Takeaway
We review everything you need to understand about Traditional Triple Arthrodesis: Fixing Severe Foot Deformity. Traditional triple arthrodesis is a surgical procedure performed to restore and maintain physiologic hindfoot alignment. It is typically reserved for severe fixed deformities not amenable to joint-sparing procedures or inflammatory arthropathy of the hindfoot. This involves fusing the subtalar, talonavicular, and calcaneocuboid joints to correct rigid foot conditions.
Introduction and Epidemiology
Triple arthrodesis is a foundational orthopedic procedure performed to restore and maintain physiologic hindfoot alignment, eliminate pain, and provide a stable plantigrade foot. Historically described by Ryerson in 1923, the procedure involves the surgical fusion of three distinct but functionally interdependent articulations: the subtalar (talocalcaneal), talonavicular, and calcaneocuboid joints. This operation is typically reserved for severe fixed deformities not amenable to joint-sparing procedures and for advanced inflammatory arthropathy of the hindfoot.

The epidemiology of patients requiring a triple arthrodesis spans a diverse range of pathology. Adult acquired flatfoot deformity (AAFD), secondary to posterior tibial tendon dysfunction (PTTD), represents one of the most common precursors. When PTTD progresses to a rigid, fixed pes planovalgus deformity with associated subtalar and transverse tarsal arthritis, joint-sparing osteotomies are no longer viable. Similarly, end-stage cavovarus deformities, frequently driven by neuromuscular conditions such as Charcot-Marie-Tooth (CMT) disease, poliomyelitis, or cerebral palsy, often culminate in rigid hindfoot malalignment necessitating arthrodesis.

Post-traumatic osteoarthritis following calcaneus or talus fractures, as well as systemic inflammatory conditions like rheumatoid arthritis or seronegative spondyloarthropathies, constitute the remainder of the epidemiological spectrum. While the advent of modern disease-modifying antirheumatic drugs (DMARDs) has decreased the incidence of severe rheumatoid foot deformities, post-traumatic and degenerative etiologies remain highly prevalent in the adult orthopedic population.

Surgical Anatomy and Biomechanics
The hindfoot comprises the talus, calcaneus, navicular, and cuboid. Physiologic alignment is generally defined as a congruent talar-first metatarsal alignment in both the anteroposterior (AP) and lateral planes with weight bearing. The talar-calcaneal articulation is referred to as the subtalar joint. The combination of the talonavicular and calcaneocuboid articulations is known as the transverse tarsal joint (or Chopart's joint).

Multiple ligamentous static restraints support the hindfoot. In fact, in the stance phase, the physiologically normal foot is balanced and plantigrade without any dynamic muscle forces acting on it. The spring ligament complex (calcaneonavicular ligament), the bifurcate ligament, and the interosseous talocalcaneal ligament within the sinus tarsi are critical static stabilizers. Physiologic hindfoot alignment is influenced by the ankle, midfoot, and forefoot. The hindfoot is a component of the ankle-hindfoot complex. To an extent, ankle malalignment can be compensated by the hindfoot.

The foot is balanced when there is a relatively even pressure distribution on the heel, first metatarsal-sesamoid complex, and the fifth metatarsal (ie, a plantigrade foot). Physiologically normal hindfoot alignment can be distorted by ankle, midfoot, and forefoot deformity. Although the ankle is primarily responsible for dorsiflexion and plantarflexion, the hindfoot has some capacity to compensate in the sagittal plane with ankle stiffness, as evidenced by residual dorsiflexion and plantarflexion following ankle arthrodesis.

During ambulation, the hindfoot exhibits complex kinematic behavior. With the transition from heel strike to stance phase, the hindfoot becomes accommodative to the surface it contacts by “unlocking” the hindfoot joints. This unlocking occurs because the calcaneus assumes a valgus position, rendering the axes of the talonavicular and calcaneocuboid joints parallel. This parallel orientation allows for increased flexibility and shock absorption.

With push-off, the posterior tibial tendon (PTT) inverts the hindfoot, thereby locking the transverse tarsal joints and hindfoot. As the calcaneus moves into varus, the axes of the talonavicular and calcaneocuboid joints become divergent and non-parallel. This converts the foot's accommodative function to one of biomechanical advantage with the creation of a rigid lever arm for the Achilles tendon, facilitating efficient forward propulsion.

Hindfoot alignment is easily distorted by an imbalance of its dynamic stabilizers, in particular, the posterior tibial and peroneal tendons. If the imbalance persists and becomes chronic, the hindfoot's static ligamentous restraints may weaken, creating a hindfoot deformity that ultimately may become fixed. PTT dysfunction leads to a flatfoot deformity with attenuation of the medial static restraints (spring ligament complex, medial talonavicular capsule) and pes planovalgus (flatfoot) deformity. Conversely, peroneal tendon dysfunction or overpowering by the posterior tibialis and anterior tibialis may lead to lateral ankle-hindfoot attenuation and a pes cavovarus (hindfoot varus) deformity. Posttraumatic or inflammatory arthritis may also create a stiff and painful hindfoot, with or without deformity.

Indications and Contraindications
The decision to proceed with a triple arthrodesis hinges on a careful assessment of joint mobility, bone stock, and the presence of degenerative changes. The primary indication is a severe, rigid deformity of the hindfoot that is accompanied by arthritic changes in the subtalar and transverse tarsal joints. In cases where the deformity is entirely flexible and the articular cartilage is preserved, joint-sparing procedures such as calcaneal osteotomies, lateral column lengthening, and tendon transfers are heavily favored to preserve hindfoot kinematics.

Relative contraindications include active infection, severe peripheral arterial disease compromising soft tissue healing, and profound peripheral neuropathy (such as acute Charcot neuroarthropathy), which may dictate alternative surgical timing or the use of specialized super-constructs rather than standard arthrodesis techniques. Furthermore, isolated disease of a single joint (e.g., isolated subtalar arthritis) is generally treated with an isolated fusion rather than a complete triple arthrodesis to preserve motion in the unaffected articulations.

| Clinical Scenario | Operative Indication for Triple Arthrodesis | Non-Operative or Alternative Management |
|---|---|---|
| Adult Acquired Flatfoot | Stage III rigid pes planovalgus with subtalar/Chopart arthritis | Stage II flexible deformity (managed via osteotomy/tendon transfer) or bracing |
| Neuromuscular Cavovarus | Rigid, fixed hindfoot varus deformity with degenerative joint changes | Flexible deformity managed with soft tissue releases, tendon transfers, and first metatarsal osteotomy |
| Rheumatoid Arthritis | Advanced, painful, destructive arthropathy of the hindfoot complex | Early synovitis managed with DMARDs and custom orthoses |
| Post-Traumatic Degeneration | Severe incongruity and arthritis of subtalar and transverse tarsal joints | Mild/isolated arthritis managed with localized fusion or NSAIDs/injections |
| Charcot Neuroarthropathy | Chronic, stable phase with severe unbraceable deformity | Acute active phase (managed with Total Contact Casting) |

Pre Operative Planning and Patient Positioning
The patient typically describes aching in the hindfoot, particularly in the sinus tarsi area, with weight bearing. There may be a report of a progressive deformity. Stiffness and swelling are common complaints. It is important to elicit a history of an inflammatory arthropathy. A neurologic and vascular examination is required. The patient should be examined while standing and ambulating. The deformity may not be obvious with the patient nonweight bearing. Typically, the patient will walk with a limp.

A single limb heel rise for a patient with pes planovalgus deformity, if possible, will determine if the deformity is flexible and if the PTT is functional. With the patient seated, range of motion (ROM) is assessed. Inversion and eversion are almost always restricted in patients being considered for triple arthrodesis. The talus can be stabilized with a thumb on the talar neck to determine dorsiflexion and plantarflexion in the hindfoot. Ankle ROM and stability also should be evaluated. An equinus contracture may be present and must be addressed with gastrocnemius recession or Achilles tendon lengthening.

Radiographic evaluation is paramount. Standard weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot, along with weight-bearing AP, lateral, and mortise views of the ankle, are mandatory. The lateral foot view allows for the assessment of the talocalcaneal angle, talonavicular coverage, and the medial longitudinal arch (Meary's angle). A hindfoot alignment view (Saltzman view) is highly useful to quantify the degree of coronal plane malalignment of the calcaneal tuberosity relative to the tibial axis. Advanced imaging, specifically computed tomography (CT), is frequently utilized to assess bone stock, the exact morphology of the articular surfaces, and the presence of subchondral cysts or avascular necrosis, particularly in the talus or navicular.

Patient positioning in the operating room is critical for optimal exposure and intraoperative fluoroscopy. The patient is placed in the supine position on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the lower extremity until the patella points directly toward the ceiling; this neutralizes the natural external rotation of the hip and provides excellent access to both the medial and lateral aspects of the foot. A thigh or calf tourniquet is applied to provide a bloodless surgical field. The extremity is prepped and draped free to allow for dynamic manipulation of the ankle and hindfoot during the procedure.

Fluoroscopy should be positioned to enter from the contralateral side or the foot of the bed, ensuring unobstructed AP, lateral, and oblique imaging of the hindfoot without compromising the sterile field.

Detailed Surgical Approach and Technique
The traditional triple arthrodesis is most reliably performed utilizing a two-incision technique. This approach minimizes the risk of extensive soft tissue stripping and devascularization of the talus, navicular, and intervening skin bridges.
Lateral Approach and Exposure
The lateral incision provides access to the subtalar and calcaneocuboid joints. The incision begins just distal to the tip of the lateral malleolus and extends distally and slightly plantarly toward the base of the fourth metatarsal. The internervous plane lies between the sural nerve (inferiorly) and the superficial peroneal nerve (superiorly). Extreme care must be taken during superficial dissection to identify and protect these neural structures, as well as the lesser saphenous vein.

Once the subcutaneous tissue is divided, the extensor digitorum brevis (EDB) muscle belly is identified. The EDB is sharply elevated off the calcaneus at its origin and reflected distally. This exposes the capsule of the calcaneocuboid joint and the lateral aspect of the subtalar joint. The contents of the sinus tarsi, including the cervical and interosseous talocalcaneal ligaments, are thoroughly evacuated using a rongeur and electrocautery. A lamina spreader is then inserted into the sinus tarsi to distract the subtalar joint, providing visualization of the posterior, middle, and anterior facets.

Medial Approach and Exposure
The medial incision is utilized to access the talonavicular joint. It begins at the tip of the medial malleolus and extends distally along the medial column to the level of the navicular tuberosity or the medial cuneiform. The incision is placed carefully to avoid the saphenous nerve and vein, which typically course slightly dorsal to the incision line.

Deep dissection involves incising the capsule of the talonavicular joint longitudinally. The posterior tibial tendon is retracted plantarly, and the anterior tibial tendon is retracted dorsally. Subperiosteal dissection exposes the complete medial, dorsal, and plantar aspects of the talonavicular articulation. A capsulotomy is performed, and a lamina spreader or distractor is utilized to open the joint space.

Joint Preparation and Deformity Correction
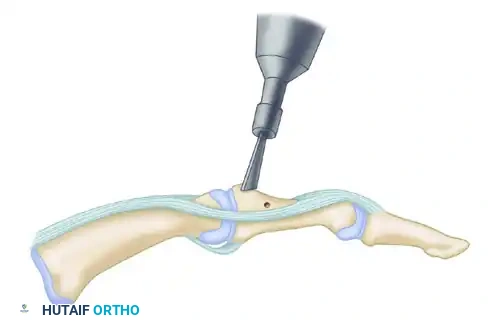
Meticulous joint preparation is the cornerstone of a successful arthrodesis. All remaining articular cartilage must be aggressively denuded to expose healthy, bleeding subchondral bone. This is achieved using a combination of sharp curettes, osteotomes, and high-speed burrs.

For the subtalar joint, the posterior facet is systematically debrided. The cartilage of the middle and anterior facets must also be addressed, though access can be challenging. In the talonavicular joint, the convex talar head and the concave navicular must be decorticated while maintaining their congruent shape to allow for optimal positioning. The calcaneocuboid joint is similarly prepared, ensuring flat, bleeding cancellous surfaces.

Following cartilage removal, the subchondral bone is "feathered" or "fish-scaled" using a fine osteotome or a drill. This technique penetrates the sclerotic subchondral plate, releasing marrow elements and osteoprogenitor cells into the fusion site to promote osteogenesis.

Deformity correction requires a comprehensive understanding of the coxa pedis. In a severe pes planovalgus deformity, the talar head is often plantarflexed and medially subluxated. The correction involves elevating the talar head, rotating the navicular dorsally and laterally over the talus, and shifting the calcaneus out of valgus into a neutral or slightly valgus (approximately 5 degrees) alignment. In a cavovarus deformity, the calcaneus must be mobilized out of varus, and the midfoot supination must be corrected. Structural bone graft (autograft from the iliac crest or proximal tibia, or bulk allograft) may be required to fill defects resulting from the realignment, particularly in the lateral column for planovalgus corrections or medial column for cavovarus corrections.

Sequence of Reduction and Fixation
The sequence of reduction and fixation is critical and typically dictates the final alignment of the foot. The most widely accepted sequence begins with the talonavicular joint.

- Talonavicular Joint: Reducing the TN joint corrects the transverse and sagittal plane deformities and establishes the medial longitudinal arch. Once reduced, it is provisionally fixed with K-wires.
- Subtalar Joint: With the TN joint fixed, the subtalar joint is reduced to correct the coronal plane (valgus/varus) deformity. The calcaneus is translated and rotated to achieve 0 to 5 degrees of valgus. Provisional K-wire fixation is placed from the plantar heel into the body of the talus.
- Calcaneocuboid Joint: The CC joint is typically addressed last. Because the TN and ST joints dictate the primary architecture, the CC joint simply falls into alignment. Any resulting gap in the CC joint must be grafted to prevent lateral column shortening and subsequent abduction deformity.

Definitive fixation is achieved using rigid internal hardware. The subtalar joint is classically fixed with one or two large-fragment (6.5 mm or 7.3 mm) cannulated compression screws, introduced from the non-weight-bearing aspect of the plantar calcaneal tuberosity, directed dorsally, medially, and anteriorly into the central body and neck of the talus.

The talonavicular joint is notoriously difficult to fuse due to its spherical anatomy and high shear forces. Fixation usually involves two crossing 4.5 mm or 5.5 mm cannulated screws, or a combination of a screw and a low-profile anatomic locking plate.

The calcaneocuboid joint is typically stabilized with a low-profile plate, compression staples, or crossed screws.

Intraoperative fluoroscopy must be utilized extensively to confirm perfect hardware placement, ensuring no screws violate the ankle joint, the naviculocuneiform joint, or protrude into the soft tissues.

Complications and Management
Despite rigorous surgical technique, triple arthrodesis carries a recognized profile of complications. The rigid locking of the hindfoot profoundly alters the biomechanics of the lower extremity, placing increased stress on adjacent joints.

Nonunion is a primary concern, with the talonavicular joint being the most frequent site of pseudoarthrosis. The TN joint's watershed blood supply, combined with the difficulty of achieving absolute rigid compression across a spherical joint surface, contributes to its higher nonunion rate (historically reported between 5% and 15%). Subtalar and calcaneocuboid nonunions are less common but can occur, particularly in patients with significant medical comorbidities such as diabetes, obesity, or a history of tobacco use.

Malunion is arguably the most debilitating complication. A hindfoot fused in varus is poorly tolerated, leading to lateral column overload, recurrent ankle sprains, and rapid degeneration of the ankle joint. A hindfoot fused in excessive valgus can lead to subfibular impingement and medial column breakdown.

Adjacent segment disease is an inevitable long-term consequence of a successful triple arthrodesis. The elimination of accommodative motion in the hindfoot transfers stress proximally to the tibiotalar (ankle) joint and distally to the midfoot (naviculocuneiform and tarsometatarsal joints). Long-term follow-up studies demonstrate a high incidence of radiographic osteoarthritis in the ankle joint decades after the index procedure.

| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Talonavicular Nonunion | 5% - 15% | Prevention: Meticulous joint decortication, bone grafting, multi-planar rigid fixation (plate + screw). Salvage: Revision arthrodesis with structural graft and orthobiologics (e.g., BMP-2). |
| Malunion (Varus/Valgus) | 5% - 10% | Prevention: Intraoperative fluoroscopic alignment views (Saltzman); correct TN joint first. Salvage: Corrective calcaneal or midfoot osteotomies; revision arthrodesis. |
| Wound Dehiscence / Infection | 2% - 8% | Prevention: Respect angiosomes; adequate skin bridges between incisions; careful EDB reflection. Salvage: Local wound care, negative pressure wound therapy, IV antibiotics, hardware removal if consolidated. |
| Adjacent Segment Arthritis | > 5 |
Clinical & Radiographic Imaging


You Might Also Like