Talar Fractures & Subtalar Arthrodesis: Surgical Guide
Key Takeaway
Talar and calcaneal fractures frequently result in post-traumatic subtalar arthrosis, necessitating salvage procedures such as subtalar distraction bone block arthrodesis. This comprehensive guide details the biomechanics, surgical indications, and step-by-step operative techniques for managing complex hindfoot trauma, including calcaneal tuberosity avulsions and sustentaculum fractures. Mastery of these techniques ensures optimal restoration of hindfoot alignment and functional recovery.
COMPLEX HINDFOOT TRAUMA: TALAR FRACTURES AND SUBTALAR SALVAGE
The management of complex hindfoot trauma, encompassing both talar fractures and severe calcaneal fractures, remains one of the most challenging domains in orthopedic traumatology. Despite meticulous acute management, a significant subset of these injuries progresses to post-traumatic subtalar arthrosis, severe hindfoot deformity, and chronic pain. To gain full confidence in the treatment of these injuries, the orthopedic surgeon must possess a thorough knowledge of the osseous and vascular anatomy, have extensive experience with modern methods of internal fixation, and be fully prepared to manage the complex soft-tissue complications that frequently arise.
When addressing post-traumatic subtalar arthrosis—often the sequela of a displaced talar body fracture or a severely comminuted intra-articular calcaneal fracture—the primary goal is the restoration of a plantigrade, painless foot. While in situ subtalar arthrodesis is generally preferred for isolated arthrosis without significant loss of height, more complex deformities require advanced reconstructive techniques.
Pathoanatomy and Clinical Outcomes
In the setting of calcaneal malunion or talar subsidence, the hindfoot often collapses into varus, accompanied by a profound loss of calcaneal height and widening of the lateral calcaneal wall. This lateral extrusion frequently leads to severe subfibular impingement and entrapment or irritation of the peroneal tendons.
Interestingly, long-term outcome studies indicate that there is no direct statistical correlation between the final clinical outcome and specific radiographic parameters such as talar angle declination, absolute talar height, or calcaneal width. Instead, poor clinical scores are statistically associated with:
* Peroneal tendon and subfibular impingement.
* Persistent anterior ankle tenderness.
* Iatrogenic or traumatic sural nerve injury.
* Patient smoking status (which drastically increases nonunion and wound complication rates).
Clinical Pearl: If widening of the calcaneus is causing subfibular impingement, a lateral wall decompression (ostectomy) must be added to the arthrodesis procedure. Failing to decompress the subfibular space will result in persistent lateral hindfoot pain despite a solidly fused subtalar joint.
SUBTALAR DISTRACTION BONE BLOCK ARTHRODESIS (CARR ET AL.)
For patients presenting with severe loss of hindfoot height and anterior ankle impingement secondary to talar or calcaneal collapse, a subtalar distraction bone block arthrodesis is indicated. This procedure, popularized by Carr et al., restores the talocalcaneal height, corrects hindfoot varus/valgus malalignment, and decompresses the subfibular space simultaneously.
Preoperative Planning and Positioning
- Imaging: Weight-bearing anteroposterior (AP), lateral, and Harris axial views of the foot and ankle are mandatory. A fine-cut computed tomography (CT) scan is highly recommended to assess bone stock, the extent of arthrosis, and the exact degree of lateral wall blowout.
- Positioning: Position the patient in the lateral decubitus position with the affected side up. Ensure all bony prominences are heavily padded.
- Preparation: Prepare and drape the affected lower extremity up to the knee. Concurrently, prepare and drape the ipsilateral posterior iliac crest for structural bone graft harvesting.
Surgical Approach and Decompression
- Incision: Under pneumatic tourniquet control, utilize a longitudinal posterolateral Gallie-type approach to access the subtalar joint.
- Sural Nerve Management: The sural nerve is at high risk during this approach. Identify the sural nerve in the proximal extent of the incision. Depending on its condition and preoperative symptoms, either meticulously protect it or, if it is already damaged/neuromatous, excise it and bury the proximal stump deep within the muscle belly to prevent painful neuroma formation.
- Lateral Wall Decompression: Subperiosteally expose the lateral calcaneal wall. Use an osteotome or oscillating saw to excise the prominent lateral wall, restoring it to a more normal anatomical width. This critical step ensures adequate decompression of the fibula and the peroneal tendons.
Joint Preparation and Distraction
- Exposure: Identify the posterior facet of the subtalar joint.
- Application of Distractor: To achieve adequate exposure and correct deformity, apply a femoral distractor or a robust external fixator. Place half-pins in the medial subcutaneous border of the tibia and the medial calcaneal tuberosity.
- Biomechanical Note: Medial application of the distractor is highly advantageous as it naturally helps to correct the typical hindfoot varus deformity as distraction is applied.
- Cartilage Removal: Apply distraction. Use a laminar spreader within the joint space to maximize exposure. Meticulously denude the subtalar joint surfaces (talar and calcaneal sides) down to bleeding subchondral bone using curettes, osteotomes, and a high-speed burr.
- Deformity Correction: Direct attention to any residual heel varus or valgus. Manipulate the hindfoot into 5 degrees of valgus. Obtain intraoperative fluoroscopic radiographs to ensure the lateral talocalcaneal angle is corrected to the normal physiological range of 25 to 45 degrees.
Bone Grafting and Rigid Fixation
- Graft Harvesting: Measure the exact dimensions of the distracted subtalar joint gap. Harvest an appropriately sized tricortical structural graft from the posterior iliac crest. For severe deformities, a bone block up to 2.5 cm in height may be required.
- Surgical Tip: Two separate pieces of tricortical graft may be necessary to completely fill the void and provide a broad base of support, thereby preventing late collapse into varus or valgus.
- Graft Insertion: Insert the structural graft into the defect and carefully release the distraction forces, allowing the talus and calcaneus to compress the graft.
- Screw Fixation: Insert two fully threaded 6.5-mm AO cancellous screws through stab incisions in the posterior heel, directing them across the calcaneus, through the bone block, and firmly into the talar body.
- Biomechanical Rationale: Two screws are mandatory to provide rigid fixation and prevent rotatory micro-movements around the axis of subtalar motion. Fully threaded screws are specifically chosen over partially threaded lag screws to maintain the distracted height and prevent the screws from compressing and crushing the structural bone block.
- Verification: Obtain final intraoperative radiographs (lateral and Harris axial views) to confirm correct hardware positioning, graft placement, and hindfoot alignment.
Postoperative Protocol
- Close the wound in layers, utilizing interrupted nylon sutures for the skin to minimize tension.
- Place the patient in a well-padded, short-leg non-weight-bearing cast.
- Weight-Bearing Status: The patient is kept strictly non-weight-bearing in the cast for the first 6 weeks. Following radiographic evidence of early incorporation at 6 weeks, weight-bearing as tolerated is permitted in a controlled ankle motion (CAM) boot for an additional 6 weeks (total 12 weeks of immobilization).
CALCANEAL TUBEROSITY AND AVULSION FRACTURES
While late complications of hindfoot trauma require complex arthrodesis, acute injuries such as calcaneal tuberosity avulsion fractures demand immediate, precise surgical intervention. These fractures are often driven by the massive pull of the Achilles tendon and present a profound risk to the posterior soft tissue envelope.
Classification of Calcaneal Tuberosity Fractures
Understanding the morphology of the avulsion is critical for selecting the appropriate fixation strategy. These fractures are generally classified into three distinct types:
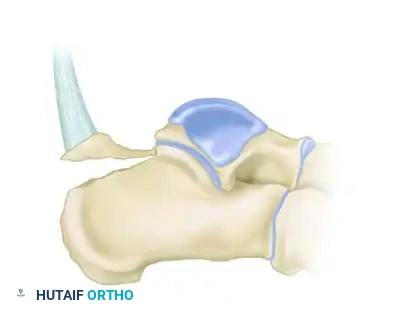
Type I: Sleeve Fracture
A thin sliver of cortical bone is avulsed from the posterior tuberosity, often involving the direct insertion of the Achilles tendon.

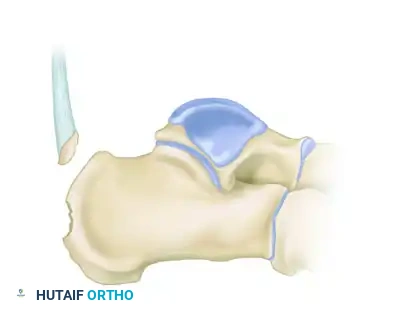
Type II: Beak Fracture
An oblique fracture exiting dorsally, creating a distinct "beak" fragment. This fragment is highly prone to proximal displacement due to the Achilles tendon.

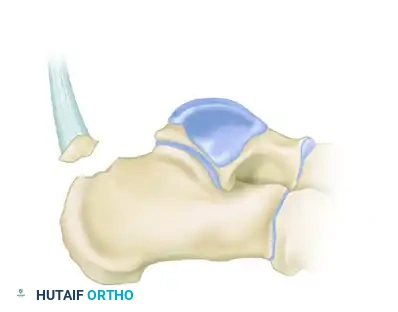
Type III: Infrabursal Fracture
An avulsion fracture occurring lower on the tuberosity, typically sparing the primary Achilles insertion but involving the retrocalcaneal bursa region.
Soft Tissue Compromise: A Surgical Emergency
Displaced calcaneal avulsion fractures, particularly Type II beak fractures, represent a true orthopedic emergency. The proximally displaced fragment places immense pressure on the posterior skin of the heel. If not reduced expediently, the skin will blanch, blister, and rapidly progress to full-thickness necrosis.
Surgical Warning: A displaced calcaneal tuberosity fracture with skin blanching must be reduced immediately. Delaying surgery will result in catastrophic soft tissue loss over the Achilles tendon, necessitating complex flap coverage and drastically increasing the risk of deep infection.
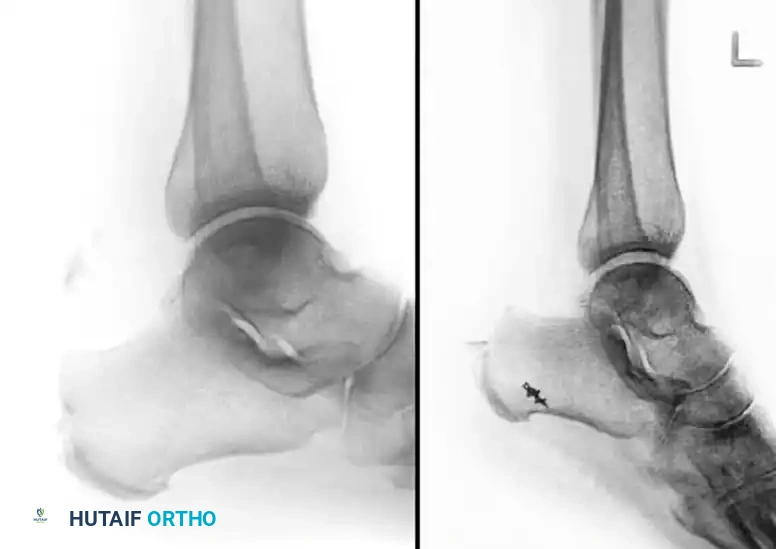
Below is an example of a severe calcaneal avulsion with a large fragment threatening the posterior envelope:

Failure to treat these injuries expediently leads to devastating open wounds and skin necrosis, as demonstrated in the clinical images below:

Clinical presentation of an open wound on the posterior heel that developed when the fracture was not treated expediently.

Radiograph demonstrating a severely displaced beak fracture tenting the posterior skin.

Full-thickness skin necrosis observed 1 month after the initial injury due to delayed intervention.
Operative Fixation Strategies
The goal of surgery is anatomic reduction of the tuberosity to restore the Achilles tendon lever arm and rigid fixation to allow early range of motion. The choice of fixation depends on the size and comminution of the avulsed fragment.
1. Plate and Screw Fixation
For large, robust Type II beak fractures, lag screw fixation supplemented by a neutralization plate provides excellent biomechanical stability. The plate acts to buttress the fragment against the massive pull of the triceps surae.


Anteroposterior and lateral radiographs demonstrating rigid plate and screw fixation of a type II calcaneal avulsion fracture.
2. Tension Band Wiring
In osteoporotic bone or when dealing with smaller, comminuted sleeve fractures (Type I) where screws may cut out, a modified tension band wiring technique is highly effective. The tension band converts the tensile forces of the Achilles tendon into compressive forces across the fracture site.

A, Proximally displaced avulsion fracture of the calcaneus. B, Lateral tension band fixation utilizing heavy non-absorbable sutures or wire to secure the fragment in osteoporotic bone.
SUSTENTACULUM TALI FRACTURES
Isolated fractures of the sustentaculum tali are rare but functionally significant injuries. The sustentaculum tali serves as the critical medial support for the talus (the middle facet of the subtalar joint) and acts as a pulley for the flexor hallucis longus (FHL) tendon.
In complex intra-articular calcaneal fractures, the sustentaculum tali is often referred to as the "constant fragment" because it remains securely tethered to the talus by the strong interosseous talocalcaneal and deltoid ligaments. However, when fractured and displaced, it must be anatomically reduced to prevent medial hindfoot collapse and FHL impingement.
Surgical Approach and Fixation
- Approach: A medial approach to the hindfoot is utilized, carefully retracting the neurovascular bundle (posterior tibial artery and tibial nerve) and the FHL tendon.
- Reduction: The fragment is reduced anatomically to restore the middle facet of the subtalar joint.
- Fixation: Fixation is typically achieved using a single or double cortical lag screw directed from medial to lateral into the dense bone of the calcaneal body.

Radiograph demonstrating precise internal fixation of an isolated sustentaculum fracture with a single lag screw.
CONCLUSION AND SURGICAL PITFALLS
The management of talar fractures, calcaneal avulsions, and their late sequelae requires a high degree of surgical acumen. Orthopedic surgeons are often frustrated by the high complication rates associated with these injuries, including wound dehiscence, deep infection, sural nerve neuromas, and nonunion.
To mitigate these risks, the surgeon must adhere strictly to biomechanical principles:
1. Respect the Soft Tissues: Delay surgery for intra-articular calcaneal fractures until the "wrinkle sign" appears, but treat tuberosity avulsions with skin blanching as absolute emergencies.
2. Decompress the Lateral Wall: Never perform a subtalar arthrodesis for calcaneal malunion without assessing and addressing subfibular impingement.
3. Restore Alignment: Use structural bone blocks (Carr technique) to restore talocalcaneal height and correct varus deformity, ensuring the foot is plantigrade.
By combining a profound understanding of hindfoot anatomy with meticulous surgical technique, the orthopedic surgeon can successfully navigate these complex injuries and optimize patient outcomes.
📚 Medical References
- Subtalar arthrodesis by cancellous grafts and metallic internal fi xation, J Bone Joint Surg 58B:507, 1976.
- Drennan JC: Congenital vertical talus, Instr Course Lect 45:315, 1996.
- Green NA: One-stage release for congenital vertical talus. Paper presented at the meeting of the Pediatric Orthopaedic Society of North America, Hilton Head, SC, May 1989.
- Grice DS: An extra-articular arthrodesis of the subastragalar joint for correction of paralytic fl at feet in children, J Bone Joint Surg 34A:927, 1952.
- Grice DS: Further experience with extraarticular arthrodesis of the subtalar joint, J Bone Joint Surg 37A:246, 1955.
- Guttman G: Modifi cation of the Grice-Green subtalar arthrodesis in children, J Pediatr Orthop 1:219, 1981.
- Harrold AJ: Congenital vertical talus in infancy, J Bone Joint Surg 49B:634, 1967.
- Harrold AJ: The problem of congenital vertical talus, Clin Orthop Relat Res 97:133, 1973.
- Jacobsen ST, Crawford AH: Congenital vertical talus, J Pediatr Orthop 3:306, 1983.
- Jayakumar S, Cowell HR: Rigid fl atfoot, Clin Orthop Relat Res 122:77, 1977.
- Kodros SA, Dias LS: Single-stage surgical correction of congenital vertical talus, J Pediatr Orthop 19:42, 1999.
- Kumar SJ, Cowell HR, Ramsey PL: Foot problems in children, I: vertical and oblique talus, Instr Course Lect 31:235, 1982.
- McCall RE, Lillich JS, Harris JR, et al: The Grice extraarticular subtalar arthrodesis: a clinical review, J Pediatr Orthop 5:442, 1985.
- Schrader LF, Gilbert RJ, Skinner SR, et al: Congenital vertical talus: surgical correction by a one-stage medial approach, Orthopedics 13:1233, 1990.
- Scott SM, Janes PC, Stevens PM: Grice subtalar arthrodesis followed to skeletal maturity, J Pediatr Orthop 8:176, 1988.
- Seimon LP: Surgical correction of congenital vertical talus under the age of 2 years, J Pediatr Orthop 7:405, 1987.
- Stricker SJ, Rosen E: Early one-stage reconstruction of congenital vertical talus, Foot Ankle Int 18:535, 1997.
You Might Also Like


