Mastering Posterolateral Arthrodesis for Spondylolisthesis
Key Takeaway
We review everything you need to understand about Mastering Posterolateral Arthrodesis for Spondylolisthesis. Arthrodesis for spondylolisthesis is a surgical fusion performed to stabilize a vertebra that has translated from its normal position. Spondylolisthesis typically involves sagittal plane slippage, often at the L5–S1 junction, causing symptoms like low-grade back pain. The procedure aims to prevent further slippage by permanently joining the affected vertebral segment, restoring stability.
Introduction and Epidemiology
Spondylolisthesis is defined as the translation of one vertebra relative to the adjacent caudal vertebra in the sagittal plane. In the pediatric and adolescent populations, this pathology most frequently manifests at the L5-S1 junction. The etiology and natural history of the disease dictate the clinical approach, ranging from benign neglect to complex surgical reconstruction. While the majority of patients remain asymptomatic or present with self-limiting, low-grade axial back pain, a subset of patients will experience progressive deformity, sagittal imbalance, and neurologic compromise necessitating operative intervention.
Epidemiologically, the incidence of spondylolysis (the anatomic precursor to isthmic spondylolisthesis) in the general population is approximately 6%. However, certain athletic populations subjected to repetitive lumbar hyperextension—such as gymnasts, divers, interior football linemen, and weightlifters—demonstrate a significantly higher prevalence. Slip progression occurs in less than 4% of patients with isthmic spondylolisthesis. Risk factors for progression include female sex, presentation prior to the adolescent growth spurt, and an initial slip magnitude greater than 50%.

Pathogenesis and Classification
The pathogenesis of spondylolisthesis is broadly categorized by the Marchetti-Bartolozzi classification, which divides the condition into developmental and acquired etiologies, superseding the older Wiltse classification in many academic centers due to its prognostic value.
Developmental spondylolisthesis includes dysplastic and isthmic variants. An isthmic defect results from chronic mechanical loading and fatigue failure of a genetically susceptible pars interarticularis. Conversely, dysplastic spondylolisthesis arises from congenital anomalies of the lumbosacral articulation. These anomalies include maloriented, sagittally aligned, or hypoplastic facet joints, as well as sacral deficiency. In dysplastic variants, the pars interarticularis may be intact but elongated, or it may eventually separate, permitting forward translation. Dysplastic slips carry a significantly higher risk of progression, a greater likelihood of neurologic sequelae, and a higher rate of surgical intervention.

Clinical Presentation and Physical Examination
Patients typically present with an insidious onset of axial low back pain. Radicular symptoms and bowel or bladder dysfunction are exceedingly rare in low-grade slips but may manifest in high-grade deformities due to traction on the cauda equina or direct foraminal compression.
Physical examination often reveals a flattened lumbar lordosis and a vertical orientation of the sacrum, resulting in a characteristic "heart-shaped" appearance of the buttocks. A visible or palpable step-off at the spinous processes is a hallmark of high-grade slips.

Hamstring tightness is a nearly universal finding in symptomatic pediatric spondylolisthesis, leading to a mild crouched gait (Phalen-Dickson sign). This is assessed via the popliteal angle; angles greater than 40 degrees indicate significant hamstring contracture, likely representing a neurologic reflex to stabilize the unstable lumbosacral junction rather than a primary muscular deficit.

Surgical Anatomy and Biomechanics
A profound understanding of lumbosacral anatomy and spino-pelvic biomechanics is paramount for safe and effective surgical management.
Osteology and Ligamentous Structures
The pars interarticularis is the anatomic bridge connecting the superior and inferior articular processes, lamina, transverse processes, and pedicle. In isthmic spondylolisthesis, the mechanical discontinuity at the pars results in the anterior translation of the L5 vertebral body, pedicles, and superior articular processes relative to the sacrum. The posterior elements of L5, including the lamina, spinous process, and inferior articular processes, remain anchored to the sacrum via the facet capsules and ligamentum flavum. This detached posterior arch is referred to as the Gill fragment.
In longstanding or high-grade cases, the altered biomechanics lead to characteristic osseous remodeling. The superior endplate of the sacrum becomes dome-shaped due to chronic shear forces, while the inferior endplate of L5 becomes concave, developing a prominent beak at its anteroinferior corner.

The transverse processes of L5 are frequently hypoplastic in this population, which significantly reduces the available surface area for posterolateral bone grafting and arthrodesis. The L5 nerve root is particularly vulnerable in this pathology. As the L5 vertebral body translates anteriorly, the L5 root becomes stretched and draped over the posterior prominent dome of the sacrum and can be compressed by the fibrocartilaginous tissue at the pars defect.
Spino Pelvic Parameters
Modern surgical decision-making relies heavily on spino-pelvic parameters. Pelvic Incidence is a fixed morphologic parameter defined as the angle between a line perpendicular to the sacral endplate at its midpoint and a line connecting this point to the center of the femoral heads. Pelvic Incidence dictates the required lumbar lordosis.

Patients with high-grade spondylolisthesis often exhibit a high Pelvic Incidence, leading to a high Pelvic Tilt (pelvic retroversion) as a compensatory mechanism to maintain sagittal balance. The slip angle (angle of lumbosacral kyphosis) is another critical measurement; a high slip angle indicates a dysplastic, unstable lumbosacral junction that generates massive shear forces, increasing the risk of pseudarthrosis and hardware failure if not adequately addressed during arthrodesis.
Indications and Contraindications
The decision to proceed with operative intervention involves a careful analysis of the patient's symptoms, slip grade, documented progression, and spino-pelvic alignment. Non-operative management remains the gold standard for asymptomatic patients and those with low-grade slips without progression.
| Parameter | Non-Operative Management | Operative Management |
|---|---|---|
| Symptom Duration | Acute or intermittent pain responding to rest/PT | Persistent, refractory pain > 6 months despite conservative care |
| Slip Grade (Meyerding) | Grade I and II (< 50% translation) | Grade III, IV, and Spondyloptosis (> 50% translation) |
| Slip Progression | Stable on serial standing radiographs | Documented progression beyond Grade II |
| Neurologic Status | Intact, isolated hamstring tightness | Radiculopathy, motor weakness, bowel/bladder dysfunction |
| Etiology | Isthmic (low risk of progression) | Dysplastic (high risk of progression) |
| Spino-Pelvic Alignment | Balanced sagittal profile | High slip angle, lumbosacral kyphosis, decompensated sagittal balance |
Absolute contraindications to posterolateral arthrodesis include active systemic or local spinal infection, severe medical comorbidities precluding general anesthesia, and patient non-compliance. Relative contraindications include profound osteopenia or osteoporosis, which may compromise pedicle screw purchase and necessitate alternative fixation strategies or cement augmentation, though this is rare in the pediatric and adolescent populations.

Pre Operative Planning and Patient Positioning
Imaging and Templating
Comprehensive preoperative imaging is mandatory. Standing posteroanterior and lateral full-length spine radiographs are required to assess global coronal and sagittal balance. Coned-down lateral views of the lumbosacral junction allow for accurate measurement of the slip percentage, slip angle, and spino-pelvic parameters. Dynamic flexion-extension radiographs help evaluate segmental instability.

Advanced imaging includes a thin-cut CT scan to define the bony anatomy, assess the size of the L5 transverse processes, evaluate the sacral dome, and template pedicle screw diameters and trajectories. MRI is indicated for any patient with neurologic symptoms to evaluate the neural foramina, the central canal, and the condition of the adjacent segment intervertebral discs.
Patient Positioning
The patient is induced under general anesthesia and intubated. Neuromonitoring (somatosensory evoked potentials and transcranial motor evoked potentials) is established and baselines are obtained prior to positioning.
The patient is then carefully log-rolled onto a radiolucent Jackson spinal table. Proper positioning is critical to surgical success. The abdomen must hang completely free to avoid compression of the inferior vena cava; such compression forces venous return through the epidural Batson's plexus, leading to excessive intraoperative bleeding.

The hips and knees should be extended to maximize lumbar lordosis and facilitate reduction of the lumbosacral kyphosis. All bony prominences are meticulously padded to prevent pressure neuropathies. The sterile prep and drape should extend widely to allow access to the posterior superior iliac spine (PSIS) for autologous bone graft harvest.
Detailed Surgical Approach and Technique
Exposure and Dissection
A standard midline longitudinal incision is made over the lower lumbar spine and sacrum. Subcutaneous tissues are dissected down to the lumbodorsal fascia. The fascia is incised in the midline, and subperiosteal dissection is performed bilaterally along the spinous processes and laminae of L4, L5, and S1.

Meticulous hemostasis is maintained using bipolar electrocautery. The dissection is carried laterally over the facet joints to expose the transverse processes of L5 and the sacral alae. Extreme care must be taken to preserve the facet joint capsules at the adjacent cranial level (L4-L5 in an L5-S1 fusion) to prevent iatrogenic adjacent segment disease. The pars defect is identified, and the fibrocartilaginous tissue within the defect is aggressively excised using rongeurs and curettes to expose the underlying L5 nerve root, which must be protected throughout the procedure.
Decompression and the Gill Procedure
In patients with radicular symptoms or high-grade slips undergoing reduction, decompression of the L5 nerve root is indicated. The Gill procedure involves the complete excision of the loose posterior elements of L5 (the Gill fragment). The ligamentum flavum is detached from the cranial lamina of L5 and the sacrum. The loose lamina and inferior articular processes are then removed en bloc or piecemeal. This unroofs the L5 nerve roots, allowing direct visualization as they course over the sacral ala. The roots must be traced laterally into the foramen to ensure they are completely free from compression by the fibrocartilaginous pars mass or the L5 pedicle during any subsequent reduction maneuvers.
Instrumentation and Screw Trajectory
Pedicle screw instrumentation is utilized to provide immediate biomechanical stability, enhance arthrodesis rates, and allow for deformity correction.
For L5, the entry point is at the intersection of the mid-transverse process and the lateral border of the superior articular process. The trajectory is convergent and parallel to the superior endplate of L5. Due to the anterior translation in spondylolisthesis, the L5 pedicles may be difficult to locate and are often situated more anteriorly and inferiorly than expected.

For S1, the entry point is at the junction of the S1 superior articular process and the sacral ala. The trajectory is directed medially toward the sacral promontory to achieve bicortical purchase, which is essential for resisting the massive shear forces at the lumbosacral junction.

In high-grade slips, reduction remains controversial. If reduction is attempted, it should focus primarily on correcting the lumbosacral kyphosis (slip angle) rather than achieving complete anatomic translation, as excessive translation places the L5 nerve root at significant risk for a stretch injury. Reduction is achieved using specialized instrumentation, leveraging cantilever forces and gradual translation.
Arthrodesis and Bone Grafting
A robust posterolateral arthrodesis is the ultimate goal of the procedure. The transverse processes of L5, the lateral aspect of the L5 superior articular processes, and the sacral alae are meticulously decorticated using a high-speed burr until punctate bleeding is observed.

Autologous iliac crest bone graft (ICBG) remains the gold standard for posterolateral fusion. A fascial incision is made over the PSIS, and cancellous bone is harvested using gouges and curettes.

The harvested autograft is often mixed with allograft or local bone from the Gill laminectomy to increase volume. The graft material is packed tightly into the lateral gutters over the decorticated transverse processes and sacral alae. In cases of high-grade slips, an interbody fusion (ALIF, TLIF, or PLIF) may be added to provide anterior column support, increase the fusion surface area, and improve sagittal alignment, though isolated posterolateral fusion remains a validated technique for appropriately selected patients.
Complications and Management
Surgical intervention for spondylolisthesis carries a distinct complication profile, particularly in high-grade deformities. Thorough preoperative counseling and meticulous surgical technique are required to mitigate these risks.
| Complication | Incidence | Etiology and Risk Factors | Prevention and Salvage Strategy |
|---|---|---|---|
| L5 Nerve Root Injury | 5-15% (Higher in reduction) | Stretch injury during translation or compression by pedicle/pars tissue. | Limit translational reduction; focus on slip angle. Direct visualization of the root. Administer intraoperative steroids if stretch is suspected. |
| Pseudarthrosis | 5-10% | High shear forces, inadequate decortication, smoking, poor graft volume. | Rigid bicortical S1 fixation. Meticulous decortication. Use of robust autograft (ICBG). Consider interbody support for high-grade slips. |
| Hardware Failure | 2-8% | Cyclic loading prior to solid fusion, pseudarthrosis. | Optimize spino-pelvic parameters. Ensure adequate screw diameter and length. Revision surgery required if symptomatic. |
| Adjacent Segment Disease | 10-20% (Long-term) | Altered biomechanics, iatrogenic injury to cranial facet capsule. | Preserve L4-L5 facet capsule during exposure. Restore optimal lumbar lordosis to prevent compensatory stress at L4-L5. |
| Dural Tear | 2-5% | Adhesions between dura and Gill fragment or pars defect. | Meticulous dissection. Primary repair with 4-0 Nurolon. Fibrin glue and Valsalva maneuver to confirm watertight seal. |
Postoperative imaging must be scrutinized for hardware placement, restoration of alignment, and maintenance of reduction.

Lateral radiographs should confirm the correction of the lumbosacral kyphosis and the proper trajectory of the pedicle screws.

Post Operative Rehabilitation Protocols
Postoperative rehabilitation is tailored to the stability of the construct and the grade of the initial deformity.
For low-grade slips treated with rigid pedicle screw fixation, patients are typically mobilized on postoperative day one. A rigid thoracolumbosacral orthosis (TLSO) is generally not required, though a soft corset may be provided for comfort. Patients are instructed in spine precautions, strictly avoiding bending, lifting (greater than 10 pounds), and twisting (the "BLT" restrictions) for the first 6 to 12 weeks.
For high-grade slips, particularly those undergoing complex reductions or where bone quality is a concern, a custom-molded TLSO with a unilateral thigh extension may be utilized to lock out the pelvis and eliminate motion at the lumbosacral junction.
Physical therapy commences at 6 weeks postoperatively, focusing initially on isometric core strengthening and gentle hamstring stretching. Dynamic lumbar stabilization exercises are introduced progressively. Return to non-contact sports is generally permitted at 6 months, provided there is radiographic evidence of solid arthrodesis. Return to collision sports (e.g., football, rugby) remains controversial; many surgeons permit return at 12 months if a solid fusion is confirmed on CT scan and the patient is entirely asymptomatic with full functional recovery.
Summary of Key Literature and Guidelines
The management of spondylolisthesis is supported by a robust body of orthopedic literature.
Historically, Wiltse and Jackson established the foundational understanding of the isthmic defect and advocated for the paraspinal muscle-splitting approach to access the transverse processes while preserving the midline ligamentous tension band.
For pediatric and adolescent isthmic spondylolisthesis, the Scoliosis Research Society (SRS) guidelines support non-operative management for Grade I and II slips, noting that the natural history is largely benign. Operative intervention via posterolateral arthrodesis with or without instrumentation is strongly recommended for symptomatic high-grade slips (Grade III and above) and documented progressive slips.
The controversy regarding in-situ fusion versus reduction for high-grade slips has been extensively debated. Seminal studies by Lenke et al. and Bradford et al. highlight that while reduction improves spino-pelvic parameters and may enhance the biomechanical environment for fusion, it carries a significantly higher risk of L5 nerve root neurapraxia. Current consensus suggests a partial reduction—prioritizing the correction of lumbosacral kyphosis (slip angle) over complete anatomic translation—optimizes sagittal balance while minimizing neurologic morbidity.
Furthermore, recent literature emphasizes the critical role of Pelvic Incidence in surgical planning. Patients with high Pelvic Incidence require greater lumbar lordosis to achieve global sagittal balance; failure to restore this alignment during arthrodesis is a primary driver of adjacent segment breakdown and poor long-term clinical outcomes. Therefore, modern posterolateral arthrodesis must be viewed not merely as a localized fusion, but as a comprehensive reconstruction of the spino-pelvic axis.
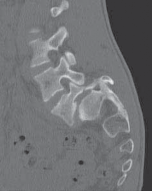
Clinical & Radiographic Imaging
You Might Also Like
