Masterclass in Knee Arthrodesis: Indications, Techniques, and Outcomes
Key Takeaway
Knee arthrodesis is a powerful salvage procedure primarily indicated for failed total knee arthroplasty, severe trauma, or chronic infection. Achieving a solid fusion requires meticulous bone preparation, optimal alignment (0-15° flexion, 5-8° valgus), and rigid fixation. Techniques include compression external fixation for minimal bone loss and intramedullary nailing for extensive defects. Proper patient selection and preoperative counseling regarding functional limitations are critical for postoperative satisfaction.
Introduction and Historical Context
Arthrodesis of the knee is a formidable and historically significant orthopedic procedure. It was first performed by Albert of Vienna in 1878 to address severe instability caused by poliomyelitis. The technique evolved rapidly over the following decades: Hibbs performed arthrodesis on a tuberculous knee in 1911, and Key introduced the concept of arthrodesis with external fixation in 1932. This foundational approach was later modified by Charnley in 1948, establishing the biomechanical principles of compression arthrodesis that remain relevant today.
Simultaneously, internal fixation techniques were advancing. Intramedullary fixation for knee arthrodesis was first described in 1948 by Chapchal, who introduced a Küntscher nail through an anterior femoral window, achieving solid fusion in 85% of patients. Subsequent modifications by Brashear, Hill, Knutson, and Lidgren refined the antegrade and retrograde nailing techniques, laying the groundwork for the modern modular and custom intramedullary devices used in contemporary orthopedic oncology and arthroplasty salvage.
Indications and Patient Selection
With the overwhelming clinical success and survivorship of primary and revision total knee arthroplasty (TKA), knee arthrodesis is seldom performed as a primary operation. Today, it is predominantly reserved as a definitive salvage procedure for patients who are no longer candidates for joint reconstruction.
Primary Indications:
* Salvage of Failed TKA: The most frequent modern indication, particularly in the setting of recalcitrant periprosthetic joint infection (PJI), massive bone loss, or extensor mechanism disruption.
* Severe Arthrosis in Specific Demographics: Occasionally appropriate for young, highly active laborers or morbidly obese patients where TKA would carry an unacceptably high risk of early mechanical failure.
* Infection and Ankylosis: Painful ankylosis secondary to pyogenic infection, tuberculosis, or severe post-traumatic osteoarthritis.
* Neuropathic Arthropathy: Charcot joint destruction where arthroplasty is contraindicated due to the high risk of catastrophic failure.
* Oncologic Resection: Malignant or aggressive benign bone tumors around the knee requiring wide resection and intercalary reconstruction.
Clinical Pearl: The Preoperative Trial
Patients must be extensively counseled regarding the functional limitations of a fused knee. Common postoperative complaints include attracting unwanted public attention, difficulty navigating public transportation, spatial constraints in theaters or stadiums, and difficulty rising from a fall. A preoperative trial of long-leg immobilization (using a cast or rigid brace) is highly recommended to help the patient psychologically and physically adapt to the realities of a stiff knee before committing to irreversible surgery.
Studies by Harris et al. comparing functional outcomes after amputation, arthrodesis, and arthroplasty for periarticular knee tumors demonstrated that walking speeds and metabolic efficiency are similar across all three cohorts. However, patients with knee arthrodesis possessed the most stable limbs, allowing them to perform the most demanding physical labor, albeit with greater difficulty sitting and higher self-consciousness regarding their gait.
Preoperative Planning and Biomechanics
The primary goal of knee arthrodesis is to achieve a painless, stable, and mechanically aligned lower extremity. The amount and quality of residual bone stock dictate the choice of fixation and the necessity for structural bone grafting.
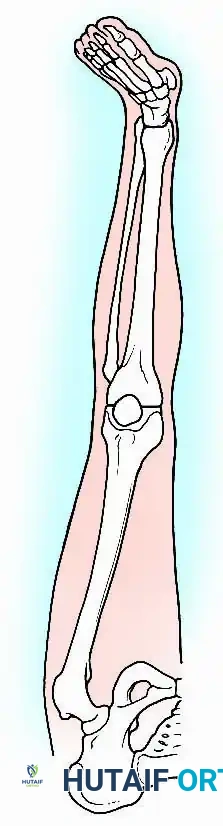
Optimal Positioning for Fusion
Achieving the correct multiplanar alignment is critical for maximizing gait efficiency and minimizing adjacent joint degeneration (particularly in the ipsilateral hip and lumbar spine).
- Flexion: 0 to 15 degrees. While Charnley historically advocated for complete extension for cosmetic reasons, a slight flexion angle (10-15 degrees) significantly aids in clearing the foot during the swing phase of gait and provides a more functional posture for sitting.
- Valgus: 5 to 8 degrees. This restores the normal mechanical axis of the lower extremity, ensuring physiological load distribution through the hip and ankle.
- Rotation: 10 degrees of external rotation, matching the normal foot progression angle.
Surgical Approaches and Joint Exposure
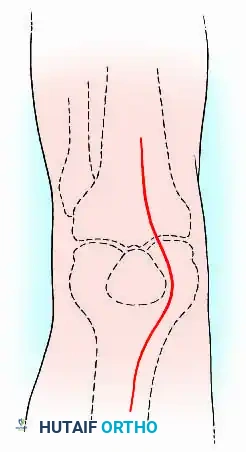
The surgical approach must be meticulously planned, especially in the setting of previous surgeries, to avoid soft tissue necrosis and wound breakdown.
-
Incision: For primary arthrodesis or when extensive exposure is required, a robust anterior longitudinal incision is preferred. In cases of salvage after failed TKA, the knee should be approached through the most lateral previous midline or parapatellar scar to preserve the vascular supply to the skin flaps.
-
Deep Dissection: The quadriceps and patellar tendons are split longitudinally. The patella is typically excised to provide autogenous bone graft, unless it is required for anterior structural support.
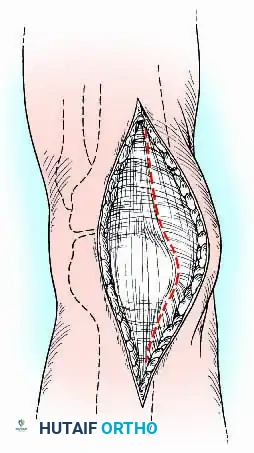
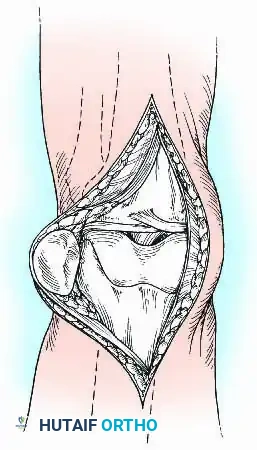
-
Joint Preparation: The joint capsule is detached from the anterior tibia, and the medial and lateral collateral ligaments are divided. The knee is hyperflexed, allowing the extensor mechanism and capsule to fall posteriorly. All residual synovium, menisci, cruciate ligaments, and the infrapatellar fat pad are radically excised to expose pristine bone.
Bone Resection and Preparation
The success of arthrodesis relies heavily on maximizing the surface area of viable, bleeding cancellous bone.
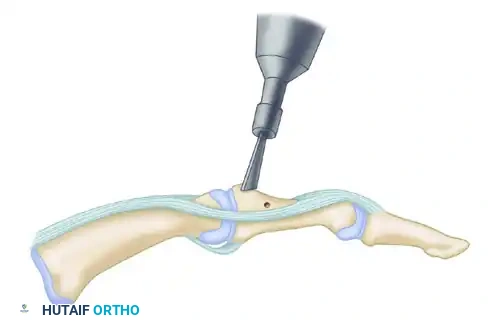
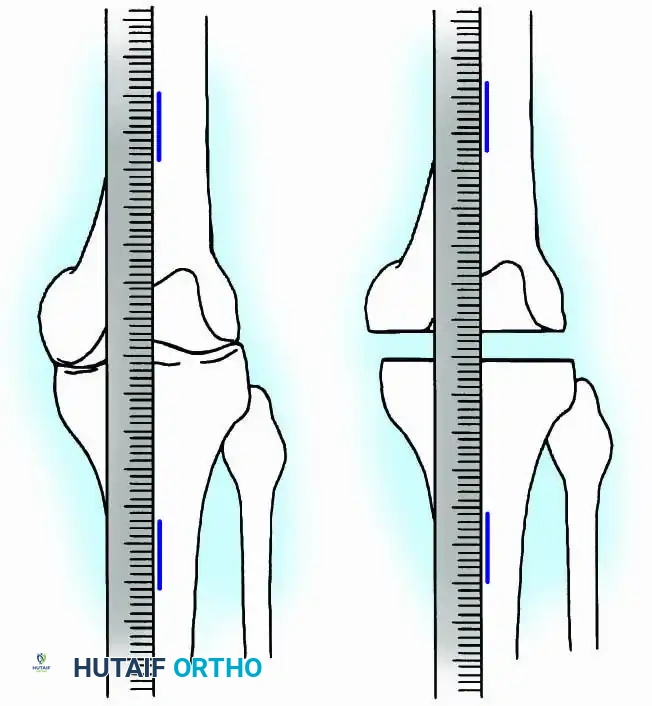
- Tibial Preparation: Using an oscillating power saw with continuous saline irrigation to prevent thermal necrosis, the superior surface of the tibia is cut exactly transverse to the long axis of the bone. A wafer of cartilage and subchondral bone (approximately 1 cm thick) is removed.
- Femoral Preparation: An appropriately sized segment of the distal femur is resected to ensure that the raw bony surfaces appose perfectly when the knee is held in the desired alignment (0-15° flexion, 5-8° valgus). Standard TKA cutting blocks and intramedullary alignment guides are highly useful for making these precise cuts.
Surgical Warning: Bone Preservation in Salvage Cases
If arthrodesis is being performed after a failed TKA, the surgeon must avoid removing additional bone from the femur and tibia. Instead, thoroughly debride the sclerotic surfaces with a high-speed burr and attempt to interdigitate the irregular metaphyseal surfaces to maximize contact area without further shortening the limb.
Fixation Techniques
The selection of fixation is dictated by the presence of infection, the volume of remaining bone stock, and the surgeon's expertise.
1. Compression Arthrodesis with External Fixation
Compression arthrodesis is generally indicated for knees with minimal bone loss and broad, flat cancellous surfaces that allow for excellent bony apposition.
Advantages: Provides stable, dynamic compression across the fusion site; avoids placing hardware directly into the medullary canal (crucial in active infections); allows for postoperative alignment adjustments.
Disadvantages: Pin track infections, poor patient tolerance, bulky frames, and the frequent need for prolonged cast immobilization after frame removal.
Surgical Technique:
* Once the bone ends are apposed in optimal alignment, transfixation pins are inserted.
* If using a traditional Charnley or Calandruccio clamp, pins are placed parallel to the joint line. The clamps are tightened to achieve a compression load of approximately 45 kg.
* Modern techniques utilize monolateral, bilateral, or circular (Ilizarov/Taylor Spatial Frame) multipin fixators.
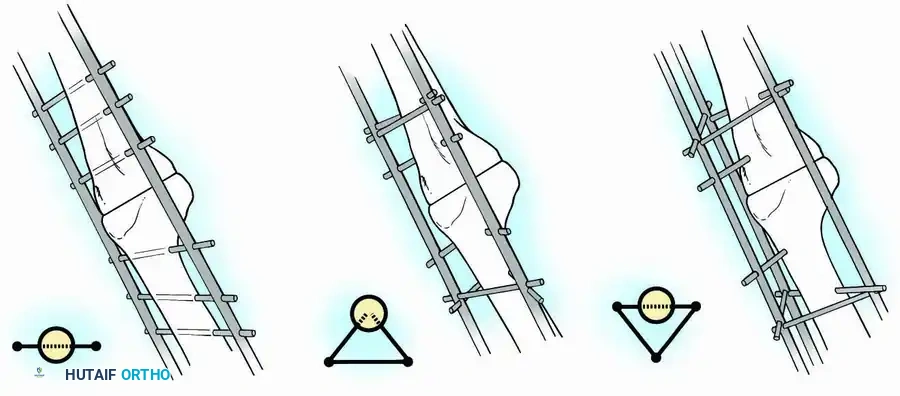
* For a biplanar fixator, three parallel transfixation pins are placed through the distal femur and three through the proximal tibia. If anteroposterior instability is noted, additional half-pins are inserted at divergent angles.
* A triangular frame configuration (using 6.5-mm half-pins placed at a 45-degree angle to the AP and mediolateral planes) provides exceptional rigid multiplanar stability and is generally better tolerated by the patient.
Postoperative Protocol for External Fixation:
The triangular frame is usually rigid enough to permit early protected weight-bearing with crutches. The frame is maintained for 8 to 12 weeks. Upon removal, a long-leg cylinder cast is applied, and graduated weight-bearing is advanced until radiographic union is confirmed (typically another 6 to 8 weeks).
2. Arthrodesis with Intramedullary Nailing
Intramedullary (IM) nailing is the gold standard when extensive bone loss precludes the use of compression across broad cancellous surfaces (e.g., post-tumor resection, failed hinged TKA).
Advantages: Immediate structural stability, early full weight-bearing, absence of pin-track complications, higher fusion rates (85% to 100%), and superior patient comfort.
Disadvantages: Significant intraoperative blood loss, technically demanding alignment control, and the risk of disseminating localized infection throughout the entire medullary canal.

Surgical Technique:
* Infection Management: In cases of infected TKA, a strict two-stage procedure is mandatory. Stage one involves complete hardware explantation, radical debridement, and placement of an articulating or static antibiotic-impregnated cement spacer, followed by a 6-week course of targeted intravenous antibiotics.
* Nail Insertion: Once infection is eradicated, the bony surfaces are prepared. The medullary canals of the femur and tibia are sequentially reamed using flexible reamers.
* Implant Selection: Long, custom, or modular titanium nails are utilized. The nail must extend at least 4 to 6 cm beyond the isthmus of both the femur and the tibia to ensure adequate diaphyseal purchase.
* Fixation: The femoral segment is often inserted retrograde, and the tibial segment antegrade. The segments are joined via a conical coupling mechanism and stabilized with proximal and distal interlocking screws to control rotation.
* Bone Grafting: The fusion site is meticulously packed with autogenous bone graft (iliac crest or local bone) and allogenic cancellous chips to stimulate osteogenesis.

Clinical Pearl: Short Locked Nails
Cheng and Gross described the use of short, locked intramedullary nails designed specifically for knee fusions. These devices avoid the need for a secondary proximal incision (required for long antegrade nails) and bypass the bulkiness of double-plating techniques, offering an excellent alternative for patients with adequate diaphyseal bone stock.
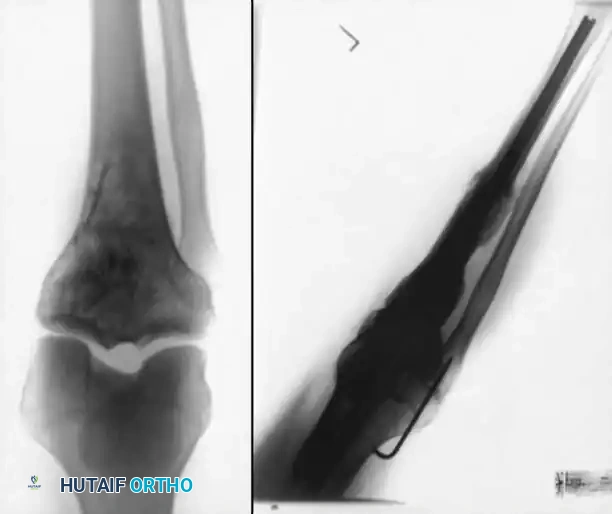
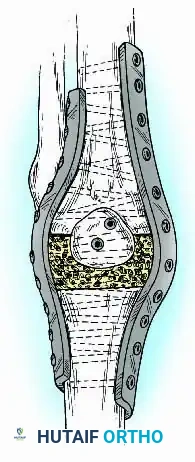
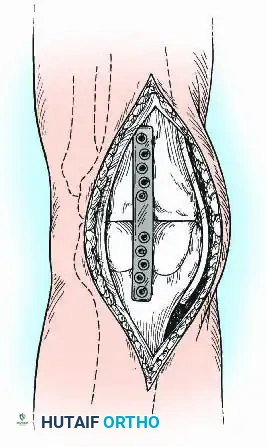
3. Plate Fixation and Adjunctive Techniques
While external fixation and IM nailing are the most common techniques, internal fixation using heavy-duty plates is a viable alternative, particularly when the medullary canal is obstructed (e.g., retained hardware, severe deformity) or when rotational control is paramount.
Technique:
* Anterior Plating: A broad, heavy-duty dynamic compression plate (DCP) or locking compression plate (LCP) can be contoured to the anterior surface of the femur and tibia. This acts as a tension band when the knee is subjected to flexion forces during weight-bearing.
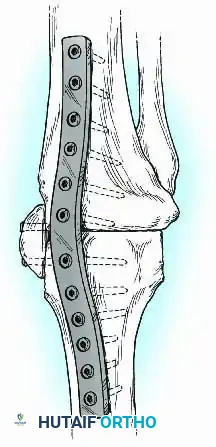
- Dual Plating: For enhanced biomechanical stability, orthogonal or dual parallel plating (medial and lateral) can be employed. This is particularly useful in cases of massive segmental bone loss where structural allografts or massive autogenous grafts (e.g., vascularized fibula) are utilized to bridge the defect.
Postoperative Protocols and Rehabilitation
The postoperative rehabilitation protocol is heavily dependent on the rigidity of the chosen fixation construct.
- Intramedullary Nailing: Due to the load-sharing nature of the IM nail, patients are typically allowed immediate, protected weight-bearing as tolerated. Physical therapy focuses on hip and ankle range of motion, core strengthening, and gait training with assistive devices.
- External Fixation / Plating: Patients are generally restricted to toe-touch or partial weight-bearing for the first 6 to 8 weeks. Serial radiographs are obtained at 4, 8, and 12 weeks to assess callus formation and trabecular bridging.
- Immobilization: If internal fixation is deemed tenuous, supplementary immobilization with a long-leg cast or a rigid knee immobilizer is maintained until clinical and radiographic union is achieved, which typically requires 12 to 16 weeks.
Complications and Outcomes
Knee arthrodesis is a major salvage procedure and carries a significant complication profile.
- Nonunion: The most challenging complication, occurring in 5% to 15% of cases. Risk factors include inadequate bone resection (failure to reach bleeding bone), insufficient compression, smoking, and residual infection. Treatment requires revision fixation, aggressive decortication, and the application of autologous bone graft or orthobiologics (e.g., BMP-2).
- Infection: Recurrent or new-onset infection is a severe threat, particularly in patients with
📚 Medical References
- Knee arthrodesis using a short locked intramedullary nail: a new technique, Am J Knee Surg 8:56, 1995.
- Damon TA, McBeath AA: Arthrodesis following failed total knee arthroplasty: comprehensive review and meta-analysis of recent literature, Orthopedics 18:361, 1995.
- Donley BG, Matthews LS, Kaufer H: Arthrodesis of the knee with an intramedullary nail, J Bone Joint Surg 73A:907, 1991.
- Ellingsen DE, Rand JA: Intramedullary arthrodesis of the knee after failed total knee arthroplasty, J Bone Joint Surg 76A:870, 1994.
- Fern ED, Stewart HD, Newton G: Curved Küntscher nail arthrodesis after failure of knee replacement, J Bone Joint Surg 71B:588, 1989.
- Figgie HE III, Brody GA, Inglis AE, et al: Knee arthrodesis following total knee arthroplasty in rheumatoid arthritis, Clin Orthop Relat Res 224: 237, 1987.
- Goldberg JA, Drummond RP, Bruce WJM, et al: Huckstep nail arthrodesis of the knee: a salvage for infected total knee replacement, Aust N Z J Surg 59:147, 1989.
- Hak DJ, Lieberman JR, Finerman GA: Single plane and biplane external fi xators for knee arthrodesis, Clin Orthop Relat Res 316:134, 1995.
- Hankin F, Louie KW, Matthews LS: The effect of total knee arthroplasty prostheses design on the potential for salvage arthrodesis: measurements of volumes, lengths, and trabecular bone contact areas, Clin Orthop Relat Res 155:52, 1981.
- Harris IE, Leff AR, Gitelis S, et al: Function after amputation, arthrodesis, or arthroplasty for tumors about the knee, J Bone Joint Surg 72A:1477, 1990.
- Hessmann M, Gotzen L, Baumgaertel F: Knee arthrodesis with a unilateral external fi xator, Acta Chir Belg 96:123, 1996.
- Hibbs RA, von Lackum HL: End-results in treatment of knee joint tuberculosis, JAMA 85:1289, 1925.
- Holden DL, Jackson DW: Considerations in total knee arthroplasty following previous knee fusion, Clin Orthop Relat Res 227:223, 1988.
- Jorgensen PS, Torholm C: Arthrodesis after infected knee arthroplasty using long arthrodesis nail: a report of fi ve cases, Am J Knee Surg 8:110, 1995.
- Key J: Positive pressure in arthrodesis for tuberculosis of the knee joint, South Med J 25:909, 1932.
- Kim YH, Kim JS, Cho SH: Total knee arthroplasty after spontaneous osseous ankylosis and takedown of formal knee fusion, J Arthroplasty 15:453, 2000.
- Knutson K, Lidgren L: Arthrodesis after infected knee arthroplasty using an intramedullary nail: reports of four cases, Arch Orthop Trauma Surg 100:49, 1982.
- Knutson K, Lindstrand A, Lidgren L: Arthrodesis for failed knee arthroplasty: a report of 20 cases, J Bone Joint Surg 67B:47, 1985.
- LaVelle DG: Knee fusion nail: technique manual, Memphis, Tenn, 1997, Smith & Nephew. Lucas DB, Murray WR: Arthrodesis of the knee by doubleplating, J Bone Joint Surg 43A:795, 1961.
- Moore FH, Smillie JS: Arthrodesis of the knee joint, Clin Orthop 13:215, 1959.
- Morrey BF, Shives TC: The knee: arthrodesis. In Morrey BF, ed: Reconstructive surgery of the joints, 2nd ed, New York, 1996, Churchill Livingstone. Morrey BF, Westholm F, Schoifet S, et al: Long-term results of various treatment options for infected total knee arthroplasty, Clin Orthop Relat Res 248:120, 1989.
- Nichols SJ, Landon GC, Tullos HS: Arthrodesis with dual plates after failed total knee arthroplasty, J Bone Joint Surg 73A:1020, 1991.
- Osgood RB: The end results of excision of the knee for tuberculosis with and without the use of bone plates, Boston Med Surg J 169:123, 1913.
- Papilion JD, Heidt RS Jr, Miller EH, et al: Arthroscopic-assisted arthrodesis of the knee, Arthroscopy 7:237, 1991.
- Phillips HT, Mears DC: Knee fusion with external skeletal fi xation after an infected hinge prosthesis: a case report, Clin Orthop Relat Res 151:147, 1980.
- Pritchett JW, Mallin BA, Matthews AC: Knee arthrodesis with a tension-band plate, J Bone Joint Surg 70A:285, 1988.
- Puranen J, Kortelainen P, Jalvaara P: Arthrodesis of the knee with intramedullary nail fi xation, J Bone Joint Surg 72A:433, 1990.
- Rand JA, Bryan RS, Chao EYS: Failed total knee arthroplasty treated by arthrodesis of the knee using the Ace-Fischer apparatus, J Bone Joint Surg 69A:39, 1987.
- Rasmussen MR, Bishop AT, Wood MB: Arthrodesis of the knee with a vascularized fi bular rotatory graft, J Bone Joint Surg 77A:751, 1995.
- Stewart MJ, Bland WG: Compression in arthrodesis: a comparative study of methods of fusion of the knee in ninety-three cases, J Bone Joint Surg 40A:585, 1958.
- Stiehl JB, Hanel DP: Knee arthrodesis using combined intramedullary rod and plate fi xation, Clin Orthop Relat Res 294:238, 1993.
- Stulberg SD: Arthrodesis in failed total knee replacements, Orthop Clin North Am 13:213, 1982.
- Thornhill TS, Dalziel RW, Sledge CB: Alternatives to arthrodesis for the failed total knee arthroplasty, Clin Orthop Relat Res 170:131, 1982.
- Vander Griend R: Arthrodesis of the knee with intramedullary fi xation, Clin Orthop Relat Res 181:146, 1983.
- Velazco A, Fleming LL: Compression arthrodesis of the knee and ankle with the Hoffman external fi xator, South Med J 76:1393, 1983.
- Vlasak R, Gearen PF, Petty W: Knee arthrodesis in the treatment of failed total knee replacement, Clin Orthop Relat Res 321:138, 1995.
- Waldman BJ, Mont MA, Payman KR, et al: Infected total knee arthroplasty treated with arthrodesis using a modular nail, Clin Orthop Relat Res 367:230, 1999.
- Weiner SD, Scarborough M, Vander Griend RA: Resection arthrodesis of the knee with an intercalary allograft, J Bone Joint Surg 78A:185, 1996.
- Wilde AH, Stearns KL: Intramedullary fi xation for arthrodesis of the knee after infected total knee arthroplasty, Clin Orthop Relat Res 248:87, 1989.
- Windsor RE: Arthrodesis. In Insall JN, ed: Surgery of the knee, 2nd ed, New York, 1995, Churchill Livingstone. Wolf RE, Scarborough MT, Enneking WF: Long-term followup of patients with autogenous resection arthrodesis of the knee, Clin Orthop Relat Res 358:36, 1999.
- Woods GW, Lionberger DR, Tullos HS: Failed total knee arthroplasty: revision and arthrodesis for infection and noninfectious complications, Clin Orthop Relat Res 173:184, 1983.
- Hip Abbott LC, Fischer FJ: Arthrodesis of the hip, with special reference to the method of securing ankylosis in massive destruction of joint, Surg Gynecol Obstet 52:863, 1931.
- Abbott LC, Lucas DB: Arthrodesis of the hip in wide abduction, J Bone Joint Surg 36A:1129, 1954.
- Abbott LC, Lucas DB: Arthrodesis of the hip: a two-stage method for diffi cult cases, Surg Clin North Am 36:1035, 1956.
- Albee FH: Arthritis deformans of the hip: a preliminary report of a new operation, JAMA 50:1977, 1908.
- Albee FH: Extraarticular arthrodesis of the hip for tuberculosis, Ann Surg 89:404, 1929.
- Barnhardt T, Stiehl JB: Hip fusion in young adults, Orthopedics 19:303, 1996.
- Benaroch TE, Richards BS, Haideri N, et al: Intermediate follow-up of a simple method of
You Might Also Like