Limited Wrist Arthrodesis
Introduction and Epidemiology
Limited wrist arthrodesis encompasses a spectrum of motion-preserving salvage procedures designed to address posttraumatic, degenerative, and inflammatory conditions of the carpus, as well as symptomatic carpal instabilities. The primary surgical objective of these procedures is to reliably alleviate pain by selectively fusing the arthritic or unstable articulations while preserving functional motion through the uninvolved, cartilaginously intact joints. By converting a multi-link kinematic chain into a more stable, simplified mechanical system, limited wrist arthrodesis improves the load-bearing capacity and overall function of the remaining un-fused carpal articulations.
The epidemiology of conditions requiring limited wrist arthrodesis is largely driven by the incidence of untreated or unrecognized carpal ligamentous injuries and scaphoid fractures. Scapholunate advanced collapse (SLAC) is the most common pattern of degenerative arthritis in the wrist, frequently resulting from chronic scapholunate interosseous ligament (SLIL) insufficiency. Scaphoid nonunion advanced collapse (SNAC) follows a similar epidemiological trajectory, representing the natural history of an ununited scaphoid fracture. Other conditions precipitating the need for limited carpal fusion include Kienböck disease (avascular necrosis of the lunate), perilunate fracture-dislocations, calcium pyrophosphate dihydrate (CPPD) deposition disease, and localized forms of rheumatoid or inflammatory arthritis. As a motion-preserving alternative to total wrist arthrodesis, limited carpal fusions—most notably the four-corner fusion (4CF) and scaphotrapeziotrapezoid (STT) fusion—have become cornerstones in the surgical armamentarium of the reconstructive hand and wrist surgeon.
Surgical Anatomy and Biomechanics
Osteology and Articular Configuration
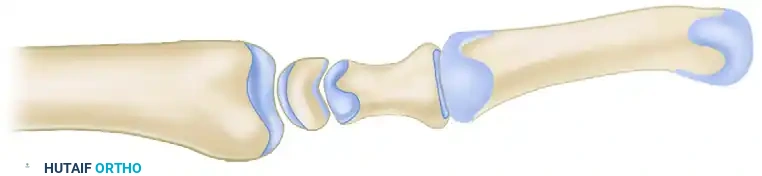
The carpus is an intricate arrangement of eight bones divided into two functional rows. The proximal row consists of the scaphoid, lunate, triquetrum, and pisiform. The distal row comprises the trapezium, trapezoid, capitate, and hamate. The proximal row acts biomechanically as an intercalated segment; it has no direct tendon insertions (excluding the pisiform, a sesamoid bone within the flexor carpi ulnaris tendon) and moves entirely in response to compressive mechanical forces transmitted from the distal row and the forearm.
The radiocarpal joint is formed by the articulation of the scaphoid and lunate with the distal radius. The scaphoid fossa of the radius is elliptical, whereas the lunate fossa is spherical. This anatomical distinction is critical to the natural history of carpal arthritis: the elliptical radioscaphoid joint is highly susceptible to shear forces and point loading when carpal alignment is altered, whereas the spherical radiolunate joint is remarkably tolerant of altered kinematics. Consequently, the radiolunate joint is typically spared from degenerative changes even in advanced SLAC or SNAC wrists, forming the anatomical basis for performing a radiolunate-sparing limited arthrodesis.
Ligamentous Architecture
The carpal bones are intimately stabilized by a complex network of intrinsic and extrinsic ligaments. Intrinsic ligaments connect carpal bones to one another, with the scapholunate interosseous ligament (SLIL) and lunotriquetral interosseous ligament (LTIL) being the most critical for proximal row stability. The SLIL is divided into dorsal, membranous, and volar regions. The dorsal region is the thickest and most biomechanically significant for resisting translational and rotational forces between the scaphoid and lunate.
Extrinsic ligaments span between the radius or ulna and the carpus. Volarly, the radioscaphocapitate (RSC), long radiolunate (LRL), and short radiolunate (SRL) ligaments provide critical stabilization. The RSC ligament acts as a fulcrum around which the scaphoid flexes. Dorsally, the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments form a V-shaped stabilizing structure that prevents dorsal translation of the carpus and assists in secondary stabilization of the proximal row.
Kinematics and Pathomechanics
Normal wrist motion occurs through five planes: flexion, extension, radial deviation, ulnar deviation, and circumduction. The primary functional axis of the wrist is the "dart thrower's motion" (DTM), an oblique plane moving from radial extension to ulnar flexion. This motion occurs predominantly at the midcarpal joint, which is why limited fusions that preserve the midcarpal articulation (or selectively fuse it while preserving radiocarpal motion) can maintain significant functional capacity.
The pathogenesis of carpal collapse begins with distraction forces across the joint or twisting motions under axial load, resulting in ligamentous rupture. Failure of the SLIL, either through trauma or inflammatory arthropathy, uncouples the scaphoid and lunate. The scaphoid naturally tends to flex, while the triquetrum naturally extends. Without the tethering effect of the scaphoid, the lunate follows the triquetrum into extension, leading to a dorsal intercalated segment instability (DISI) deformity.

When DISI occurs, the normal load distribution (80% radius, 20% ulna) is severely disrupted. The flexed scaphoid presents a smaller, incongruous surface area to the elliptical scaphoid fossa of the radius, creating point loading. This abnormal distribution of force leads to progressive cartilage wear, initiating the SLAC sequence. A similar biomechanical failure occurs in SNAC wrists, where the distal pole of the ununited scaphoid flexes, causing impingement and localized arthritis at the radial styloid and subsequently the midcarpal joint.
Indications and Contraindications
Patient History and Physical Examination
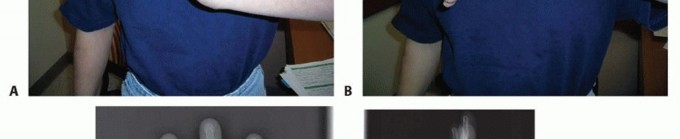
Patients typically present with a history of a traumatic wrist injury, though the absence of a distinct traumatic event does not exclude conditions like CPPD, Kienböck disease, or unrecognized chronic ligamentous attrition. Chief complaints include deep, aching wrist pain exacerbated by heavy loading or repetitive motion, significantly reduced grip strength, and a limited arc of motion compared to the contralateral side.
Physical examination reveals painful wrist motion and localized tenderness, often over the anatomic snuffbox or dorsal radiocarpal joint. The finger extension test is a highly sensitive provocative maneuver. The wrist is passively flexed while the examiner resists active finger extension. A positive test yields pain and suggests periscaphoid inflammatory changes, radiocarpal or midcarpal instability, or Kienböck disease. A negative test essentially excludes dorsal wrist syndrome, Kienböck disease, midcarpal instability, and SLAC as the cause of symptoms. Additional tests include the Watson scaphoid shift test, which may demonstrate a palpable clunk or pain in cases of dynamic scapholunate instability prior to fixed arthritic collapse.
Staging Systems and Selection Criteria
The selection of a specific limited wrist arthrodesis depends entirely on the precise location of articular degeneration.
SLAC and SNAC wrists are staged based on the predictable progression of arthritis:
* Stage I: Arthritis localized to the radial styloid (often seen as styloid beaking).
* Stage II: Arthritis involving the entire radioscaphoid joint.
* Stage III: Arthritis extending to the capitolunate joint (midcarpal joint).
* Stage IV: Pancarpal arthritis (involving the radiolunate joint).
Limited wrist arthrodesis, particularly the four-corner fusion (capitate, hamate, lunate, triquetrum) with scaphoid excision, is indicated for Stage II and Stage III SLAC/SNAC wrists. The absolute prerequisite for a four-corner fusion is a preserved, cartilaginously intact radiolunate joint. If the radiolunate joint is arthritic (Stage IV), a total wrist arthrodesis is required.
Operative vs Non Operative Management
| Clinical Condition | Non Operative Management | Operative Management |
|---|---|---|
| SLAC Stage I | NSAIDs, splinting, corticosteroid injections, activity modification. | Radial styloidectomy, scaphoid stabilization, PIN neurectomy. |
| SLAC/SNAC Stage II | Corticosteroid injections, custom orthoses. | Proximal Row Carpectomy (PRC) OR Scaphoid excision + Four-Corner Fusion. |
| SLAC/SNAC Stage III | Prolonged splinting, palliative pain management. | Scaphoid excision + Four-Corner Fusion (PRC contraindicated due to capitate head arthritis). |
| SLAC/SNAC Stage IV | Palliative care, rigid immobilization. | Total Wrist Arthrodesis. |
| Kienböck Disease (Stage II/IIIa) | Immobilization, bisphosphonates (limited evidence). | Joint leveling procedures, STT fusion, or SC fusion to offload the lunate. |
| Isolated STT Arthritis | Thumb spica splinting, targeted injections. | STT Arthrodesis or distal pole scaphoid excision. |
Pre Operative Planning and Patient Positioning
Imaging Modalities
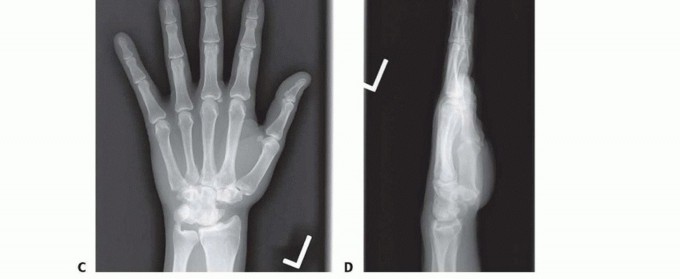
Thorough preoperative imaging is mandatory to define the extent of articular involvement and plan the appropriate salvage procedure. Standard posteroanterior (PA), lateral, oblique, and scaphoid views are obtained. The PA view assesses carpal height, ulnar variance, and radiocarpal joint space. The lateral view is critical for measuring the scapholunate angle (normal 30-60 degrees) and the radiolunate angle to quantify the degree of DISI deformity.

Advanced imaging, particularly high-resolution computed tomography (CT) without contrast, is the gold standard for evaluating the articular surface of the radiolunate joint. Subchondral sclerosis, cyst formation, or joint space narrowing at the radiolunate articulation on CT dictates a mandatory shift in the surgical plan from a limited carpal fusion to a total wrist arthrodesis. Magnetic resonance imaging (MRI) is less useful for assessing cortical bone stock but is highly sensitive for evaluating lunate vascularity in suspected Kienböck disease or assessing the integrity of the interosseous ligaments.
Operating Room Setup
The patient is placed in the supine position with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Regional anesthesia (supraclavicular or axillary brachial plexus block) is preferred, providing excellent intraoperative muscle relaxation, decreasing the required depth of general anesthesia, and affording prolonged postoperative analgesia. Intraoperative fluoroscopy (C-arm) is positioned parallel to the arm board, allowing for orthogonal views without repositioning the patient's shoulder.
Detailed Surgical Approach and Technique
Most reconstructive wrist procedures require a dorsal approach to the wrist. The wrist and finger extensor tendons are separated into six compartments by the dorsal extensor retinaculum. The most common and versatile interval for exposure of the radiocarpal and midcarpal joints is between the third and fourth extensor compartments.

Surgical Dissection and Exposure
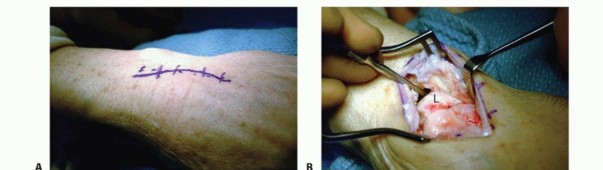
A dorsal longitudinal incision is made centered over the Lister tubercle, extending from the distal radius to the base of the third metacarpal. Skin flaps are elevated, taking care to protect the dorsal sensory branches of the radial and ulnar nerves.
The dorsal extensor retinaculum is incised over the third extensor compartment, and the extensor pollicis longus (EPL) tendon is mobilized and transposed radially. The floor of the third compartment and the roof of the fourth compartment are incised, allowing the extensor digitorum communis (EDC) and extensor indicis proprius (EIP) tendons to be retracted ulnarly.

At this stage, a posterior interosseous nerve (PIN) neurectomy is routinely performed. The PIN is identified on the floor of the fourth compartment, resting on the interosseous membrane just proximal to the radiocarpal joint. Resection of a 1-cm segment of the PIN provides partial denervation of the dorsal wrist capsule, significantly improving postoperative pain relief without compromising motor function.
A ligament-sparing capsulotomy is then performed. A radially based rectangular flap or a distally based capsular flap (Berger approach) is elevated, meticulously preserving the dorsal radiocarpal and dorsal intercarpal ligaments for later robust repair. This exposes the proximal and distal carpal rows.
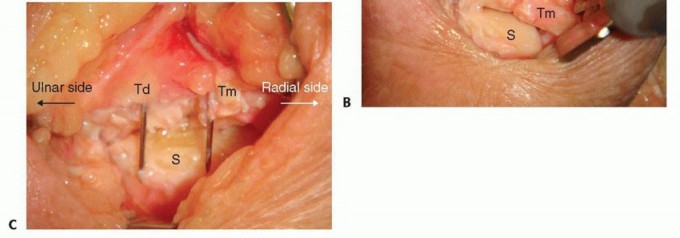
Scaphoid Excision
For a four-corner fusion, the scaphoid must be entirely excised to eliminate the arthritic radioscaphoid articulation. The scaphoid is identified, and its attachments to the trapezium, trapezoid, capitate, and radius are sharply divided.

To facilitate removal and minimize trauma to surrounding structures, the scaphoid can be fragmented using a rongeur or an oscillating saw. Extreme care must be taken to protect the volar radiocarpal ligaments (RSC and LRL) during the volar dissection of the scaphoid. Complete excision of the distal pole is verified fluoroscopically, as retained fragments can cause painful impingement against the trapezium and limit postoperative range of motion.
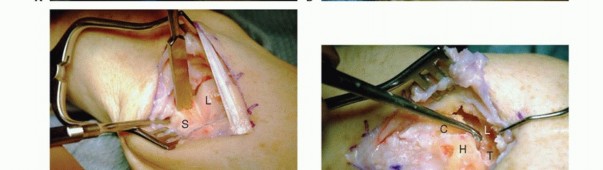
Joint Preparation and Debridement
The articular surfaces of the capitate, hamate, lunate, and triquetrum are meticulously prepared for arthrodesis.
Using a combination of a high-speed burr, curettes, and rongeurs, the hyaline cartilage and subchondral bone plate are removed down to bleeding, healthy cancellous bone. The specific articulations decorticated include the capitolunate, capitohamate, triquetrohamate, and lunotriquetral joints. It is imperative to preserve the anatomical contour and dimensions of the carpal bones to prevent collapse and loss of carpal height. The radiolunate joint must be strictly protected during this process to ensure the success of the salvage procedure.
Reduction and Bone Grafting
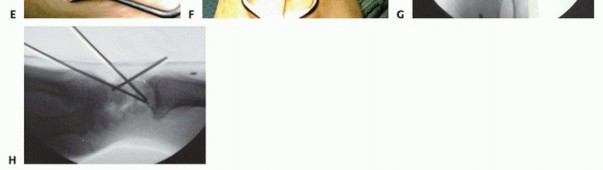
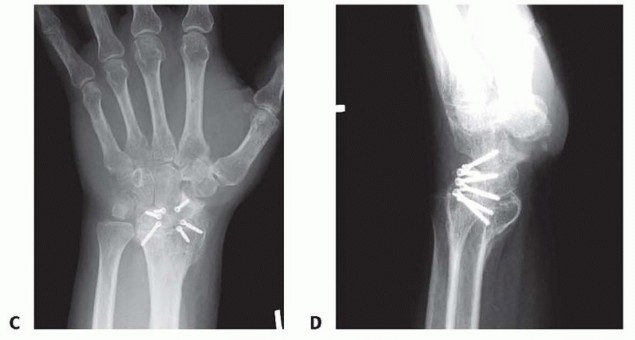
Correction of the DISI deformity is a critical step. The lunate, which is typically extended in SLAC/SNAC wrists, must be flexed back into a neutral, collinear alignment with the radius. A 0.062-inch Kirschner wire is often inserted dorsally into the lunate to act as a joystick, levering it out of extension.
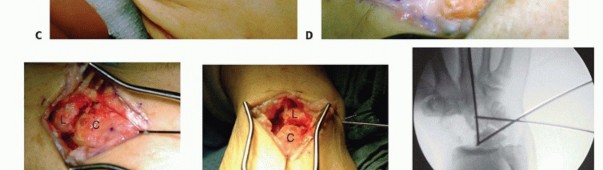
Once the lunate is reduced, the capitate is seated into the lunate fossa, and provisional K-wire fixation is placed across the capitolunate and triquetrohamate joints. Cancellous bone graft, harvested either from the excised scaphoid (if not excessively sclerotic), the distal radius (Lister tubercle area), or the iliac crest, is densely packed into the interstices of the four-corner junctions to promote osteogenesis.
Definitive Fixation Strategies
Historically, fixation was achieved with multiple K-wires, which required prolonged immobilization and carried a high risk of pin tract infection and nonunion. Modern techniques utilize rigid internal fixation, allowing for earlier rehabilitation and higher fusion rates.

Options include:
1. Headless Compression Screws: Screws are placed across the capitolunate, triquetrohamate, and capitohamate joints. This provides excellent interfragmentary compression and avoids dorsal hardware prominence.
2. Dorsal Circular Plates: Specifically designed circular plates (e.g., Spider plates) are recessed into the dorsal cortex of the carpus. A central reamer creates a bed for the plate, and locking screws secure the four bones. While biomechanically stable, dorsal plates carry a risk of extensor tendon irritation if not adequately countersunk.
3. Memory Staples: Nitinol compression staples can be utilized across the decorticated joints, providing continuous dynamic compression
Clinical & Radiographic Imaging



You Might Also Like