Arthrodesis with an Intramedullary Nail: Fixing Failed TKAs

Key Takeaway
For anyone wondering about Arthrodesis with an Intramedullary Nail: Fixing Failed TKAs, Arthrodesis with an intramedullary nail is a surgical fusion of the knee joint, primarily indicated for limb salvage following failed total knee arthroplasty, particularly with infection, bone loss, or loss of the extensor mechanism. It aims to provide a stable, pain-free limb for ambulation, though it eliminates knee motion. Prior infection treatment is crucial.
Introduction and Epidemiology
Knee arthrodesis remains a critical limb salvage procedure in the armamentarium of the reconstructive orthopedic surgeon. While the vast majority of primary and revision total knee arthroplasties (TKA) yield satisfactory outcomes, a subset of patients experience catastrophic failure necessitating salvage interventions. When revision arthroplasty is no longer viable due to insurmountable bone loss, unyielding periprosthetic joint infection (PJI), or irreversible extensor mechanism disruption, the surgeon must choose between knee arthrodesis and above-knee amputation.
The epidemiology of failed TKA leading to arthrodesis is heavily skewed toward infectious etiologies. Periprosthetic joint infection accounts for the majority of these cases, often after multiple failed attempts at two-stage exchange arthroplasty. Aseptic failures, including severe massive osteolysis, recurrent instability, and catastrophic periprosthetic fractures with inadequate bone stock for fixation or revision implants, constitute the remainder. Historically, knee arthrodesis was performed for primary osteoarthritis, tuberculosis, or poliomyelitis; however, in contemporary practice, it is almost exclusively reserved as a salvage option for the multiply revised, failed total knee arthroplasty.

Pathophysiology of the Failed Total Knee Arthroplasty
The pathophysiologic cascade leading to a non-reconstructable knee joint typically involves chronic indolent infection or massive particulate wear debris leading to macrophage-induced osteolysis. In the setting of PJI, the formation of a robust bacterial biofilm on prosthetic surfaces and necrotic bone renders systemic antibiotics ineffective. Repeated surgical debridements and implant exchanges often result in progressive devascularization of the distal femur and proximal tibia. The resultant metaphyseal and diaphyseal bone loss creates a mechanical environment where standard or even highly constrained revision arthroplasty implants cannot achieve durable fixation.
Surgical Anatomy and Biomechanics
A thorough understanding of the altered surgical anatomy and the unique biomechanics of a fused lower extremity is paramount for successful execution and patient counseling. The anatomy encountered during salvage arthrodesis is invariably distorted by prior surgical approaches, chronic inflammation, and severe bone deficiency.
Osteology and Ligamentous Deficiencies
In the multiply revised knee, the epicondylar axis, joint line, and standard anatomic landmarks are frequently obliterated. The extensor mechanism is often attenuated, scarred, or completely absent. The medial and lateral collateral ligaments may be incompetent or resected during prior constraint escalations. Vascular anatomy, particularly the popliteal artery and vein, may be tethered to the posterior capsule due to chronic scarring, increasing the risk of iatrogenic vascular injury during posterior capsular release or aggressive bony resection.

Biomechanical Implications of a Fused Knee
The biomechanical conversion of a dynamic hinge joint to a static bony column fundamentally alters lower extremity kinematics and energy expenditure. Arthrodesis with an intramedullary nail provides the most rigid biomechanical construct compared to external fixation or dual plating, as the load-sharing intramedullary device neutralizes bending moments across the fusion site.
However, the absence of knee flexion during the swing phase of gait necessitates compensatory mechanisms. Patients must utilize circumduction or vaulting to clear the foot, which increases the metabolic cost of walking by approximately 25 to 30 percent compared to normal ambulation. This compensatory gait places significantly increased abnormal stress on the ipsilateral hip, ipsilateral ankle, and the contralateral limb. Consequently, pre-existing degenerative joint disease in these adjacent joints can be rapidly accelerated.

Indications and Contraindications
The decision to proceed with knee arthrodesis using an intramedullary nail requires meticulous patient selection. The primary goal is to provide a stable, painless, and infection-free limb capable of weight-bearing, thereby avoiding amputation.
Patient Selection Criteria
Indications for knee arthrodesis include limb salvage after the failure of delayed exchange and re-implantation of an infected TKA. It is also indicated in cases of complete loss of the extensor mechanism where allograft reconstruction or synthetic mesh has failed or is deemed inappropriate. Additionally, severe bone loss after failed repeat re-implantation or posttraumatic osteoarthritis where prosthetic joint reconstruction is anatomically impossible serves as a primary indication.

Contraindications must be strictly observed to prevent disastrous functional outcomes. The procedure is absolutely contraindicated for patients with a contralateral above-knee amputation, as bilateral stiff limbs or one stiff limb and one high-level prosthesis severely preclude functional ambulation and transfers. It is relatively contraindicated for patients with severe ipsilateral hip or ankle degenerative arthritis due to the aforementioned biomechanical stresses. Furthermore, arthrodesis does not guarantee the eradication of infection; therefore, active, uncontrolled infection is an absolute contraindication to definitive intramedullary nailing. Any infection must be successfully treated prior to arthrodesis surgery, most commonly involving staged debridements and the use of antibiotic-eluting cement spacers.

| Clinical Scenario | Operative Arthrodesis Indication | Non Operative or Alternative Management |
|---|---|---|
| Recurrent PJI with massive bone loss | Definitive IM nail arthrodesis (after clearance) | Suppressive antibiotics or Amputation if clearance fails |
| Absent extensor mechanism with stable bone | IM nail arthrodesis | Extensor mechanism allograft (if viable soft tissue envelope) |
| Contralateral Above-Knee Amputation | Contraindicated | Above-Knee Amputation or Resection Arthroplasty |
| Severe ipsilateral hip/ankle OA | Relative Contraindication | Total Hip/Ankle Arthroplasty prior to knee fusion |
| Active untreated PJI | Contraindicated for definitive hardware | Debridement, explant, antibiotic spacer |
Pre Operative Planning and Patient Positioning
Preoperative planning is arguably the most critical phase of knee arthrodesis. The surgeon must anticipate the degree of bone loss, the required length of the implant, and the quality of the host bone.

Advanced Imaging and Templating
Arthrodesis should be preceded by any or all necessary treatments for infection, including the removal of implants, cement debris, and necrotic tissue, followed by the implantation of an antibiotic cement spacer. Once inflammatory markers have normalized and aspiration cultures are negative, definitive planning begins.
Anteroposterior and lateral plain radiographs of the affected knee and the entire lower extremity from hip to ankle are mandatory. The length of the femur and the tibia must be determined, and any unusual bowing or canal abnormalities must be identified. The length of the femur and the tibia can be obtained from plain radiographs with a measuring template in place.

Alternatively, and highly recommended, a computed tomography (CT) scan from the tip of the greater trochanter to the distal femur, and then from the proximal tibia to the distal tibia, should be utilized. CT scans are invaluable for identifying the narrowest portion of the isthmus of the tibia and femur, which dictates the maximum allowable diameter of the intramedullary nail. Coronal and sagittal CT reformats help identify endosteal sclerosis, retained cement mantles, or occult cortical defects that could lead to intraoperative fracture during reaming.
The arthrodesis nail should extend from the tip of the greater trochanter to well within the isthmus of the distal tibia. The final nail position should be within 3 to 5 inches above the tibial plafond. If there is significant distraction at the level of the knee to restore leg length, this amount of length must be meticulously calculated and added to the final nail length.
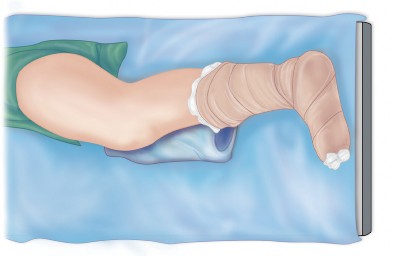
Operating Room Setup and Positioning
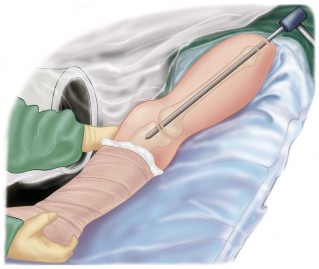
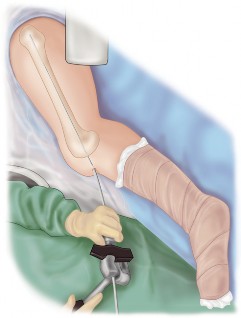
The patient is positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to correct external rotation and allow true anteroposterior and lateral fluoroscopic views of the femur and tibia. The entire lower extremity from the iliac crest to the toes must be prepped and draped free to allow for manipulation, assessment of alignment, and access to the greater trochanter for antegrade nail insertion.
Fluoroscopy is positioned on the contralateral side of the operative field. Prior to incision, the surgeon must verify that clear orthogonal views of the hip, knee, and ankle can be obtained without obstruction from the table column.
Detailed Surgical Approach and Technique
The surgical technique for knee arthrodesis with a long intramedullary nail is complex and requires meticulous attention to both soft tissue handling and bone preparation.
Soft Tissue Exposure and Implant Removal
The previous midline longitudinal incision is typically utilized. A medial parapatellar arthrotomy is performed to expose the joint. If an antibiotic spacer is present, it is removed. Radical synovectomy and debridement of all fibrotic and potentially infected tissue are performed. Thorough irrigation is mandatory. Deep tissue cultures should be obtained prior to the administration of systemic perioperative antibiotics, even in presumed aseptic cases.
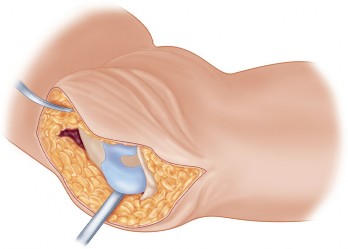
Joint Preparation and Bone Loss Management
The opposing surfaces of the distal femur and proximal tibia must be prepared to maximize bony contact. Sclerotic bone should be resected to bleeding cancellous bone using an oscillating saw. The cuts should be made perpendicular to the mechanical axis of each respective bone. In cases of massive bone loss, structural allografts (such as femoral head allografts or intercalary segments) or highly porous metal cones may be utilized to bridge the gap and restore leg length. However, shortening the limb by up to 2 to 3 centimeters is often well-tolerated and can facilitate primary bone-on-bone apposition, which significantly increases the probability of successful fusion.
Intramedullary Canal Preparation
The femoral canal is accessed retrogradely through the intercondylar notch or antegradely through the piriformis fossa or greater trochanter, depending on the specific nail design. A ball-tipped guide wire is passed into the femoral canal. Sequential flexible reaming is performed.

Similarly, the tibial canal is accessed via the proximal tibial plateau. The guide wire is passed down to the distal tibial metaphysis. Reaming of the tibia is performed sequentially. It is critical to ream both canals to at least 1 to 1.5 millimeters larger than the anticipated nail diameter to prevent incarceration of the implant, particularly in sclerotic diaphyseal bone. The narrowest portion of the tibial isthmus, identified on preoperative CT, will ultimately dictate the maximum nail diameter.

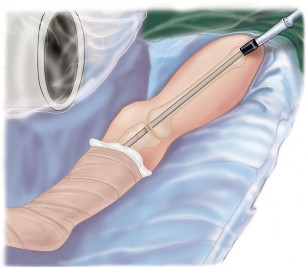
Nail Insertion and Interlocking
Once both canals are adequately prepared, the femur and tibia are aligned. Antegrade insertion of a modular or custom long arthrodesis nail is most common. The nail is introduced through the greater trochanter, passed down the femoral canal, across the prepared knee joint, and into the tibial canal.
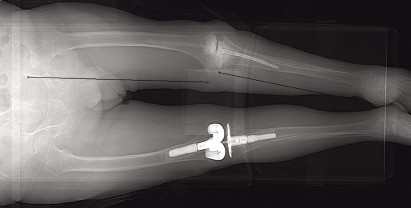
Fluoroscopy is used to confirm the trajectory of the nail across the joint line to avoid posterior cortical perforation of the proximal tibia. The final nail position should be 3 to 5 inches above the tibial plafond.
Once the nail is fully seated, proximal interlocking screws are placed in the femur. Axial compression is then applied across the arthrodesis site. This can be achieved manually or via the internal compression mechanism of the nail system. After adequate compression and bony apposition are confirmed fluoroscopically, distal interlocking screws are placed in the tibia to secure the construct.
Bone graft, either autograft from reamings, allograft, or demineralized bone matrix, is packed meticulously around the arthrodesis site to promote osteogenesis. The soft tissues are closed in layers over a suction drain. If the soft tissue envelope is severely compromised, a gastrocnemius rotational flap may be required to achieve adequate coverage.

Complications and Management
Knee arthrodesis in the salvage setting is fraught with potential complications. The surgeon must be prepared to manage these complex scenarios.
Infection Recurrence and Hardware Failure
The most devastating complication is the recurrence of periprosthetic joint infection. Spread of infection along the nail proximally into the femur or distally into the tibia has led some authors to recommend alternative techniques for fusion, such as a short intramedullary nail, plates and screws, or external fixation. While a variety of published reports do not indicate the spread of infection as a highly prevalent complication, the consequences are severe. If infection recurs after a long IM nail has been placed, the entire medullary canal of the lower extremity is compromised. Furthermore, a short intramedullary nail or a fully integrated modular nail can be extremely difficult to remove once arthrodesis has been achieved or if the hardware fails.

Nonunion is another significant pitfall, occurring in up to 10 to 15 percent of cases despite rigid fixation. Risk factors include inadequate bone apposition, residual infection, smoking, and severe host compromise. Management of nonunion may require dynamization of the nail, exchange nailing, or augmentation with plates and autologous bone grafting.
Inability to maintain knee extension after previously failed TKA, or the presence of a neuropathic joint (Charcot arthropathy), significantly increases the risk of hardware failure and nonunion. Extreme obesity and severe degenerative knee disease further compound the mechanical stresses on the implant, leading to fatigue failure of the nail or interlocking screws.

| Complication | Estimated Incidence | Salvage and Management Strategies |
|---|---|---|
| Nonunion | 10 - 15% | Dynamization, Exchange nailing, Plate augmentation with bone graft |
| Recurrent Infection | 5 - 10% | Hardware removal, aggressive debridement, suppressive antibiotics, Amputation |
| Periprosthetic Fracture | 3 - 5% | Open reduction internal fixation with locking plates, Revision nailing |
| Hardware Failure (Breakage) | 2 - 5% | Removal of broken hardware, Revision IM nailing with larger diameter |
| Leg Length Discrepancy (>3cm) | 15 - 20% | Shoe lift, Contralateral epiphysiodesis (rare in adults), Contralateral shortening |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is dictated by the rigidity of the fixation and the quality of the host bone.

Weight Bearing and Mobility Training
In cases where excellent cortical contact and rigid compression are achieved, patients may be allowed touch-down weight bearing (TDWB) or partial weight bearing immediately postoperatively. Progression to full weight bearing is typically delayed until radiographic evidence of bridging callus is observed, usually between 8 to 12 weeks.
If structural allografts were used or if bone quality is exceptionally poor, strict non-weight bearing may be enforced for the first 6 weeks. Deep vein thrombosis (DVT) prophylaxis is mandatory, as these patients are at high risk due to altered mobility and extensive intramedullary instrumentation.

Physical therapy focuses on maximizing the range of motion of the ipsilateral hip and ankle to compensate for the fused knee. Gait training is essential. Patients must be taught how to safely perform transfers, navigate stairs, and ambulate with assistive devices while managing a stiff, extended limb. Shoe lifts may be prescribed if the limb length discrepancy exceeds 1.5 to 2 centimeters to prevent compensatory pelvic obliquity and secondary lumbar spine pathology.
Summary of Key Literature and Guidelines
The literature surrounding salvage knee arthrodesis heavily favors intramedullary nailing over alternative techniques when anatomically feasible.

Evidence Based Outcomes and Controversies
The most effective method of surgical arthrodesis remains somewhat debatable in highly specific clinical scenarios, but the highest reported fusion rates are consistently achieved with an intramedullary nail. Biomechanical studies validate that IM nails provide superior resistance to bending and torsional forces compared to dual plating or external fixation.
Additional techniques previously described, including external fixation, are now generally reserved for cases of active, recalcitrant infection where internal hardware is strictly contraindicated. Plate fixation is occasionally utilized when intramedullary canal deformity or retained hardware precludes nail passage, though it carries a higher risk of hardware prominence and soft tissue breakdown.
The primary controversy revolves around the use of long versus short intramedullary nails in the setting of previous infection. While long nails crossing the hip, knee, and ankle provide unmatched stability, the theoretical risk of pan-medullary infection spread remains a concern for some authors. However, modern systematic reviews and a variety of published reports do not report the spread of infection as a statistically significant complication when strict two-stage protocols and appropriate antibiotic spacers are utilized prior to definitive nailing.
Ultimately, arthrodesis with an intramedullary nail may provide union, substantial pain relief, and a stable limb for ambulation. While the absence of knee motion introduces practical drawbacks and functional limitations, it remains a highly successful and indispensable limb salvage technique for the multiply failed total knee arthroplasty.
You Might Also Like