Isolated Subtalar Arthrodesis: When & Why It's Preferred

Key Takeaway
We review everything you need to understand about Isolated Subtalar Arthrodesis: When & Why It's Preferred. **Isolated subtalar arthrodesis** is a surgical fusion of the talocalcaneal joint, used to treat various hindfoot conditions such as primary arthrosis, posttraumatic arthritis, rheumatoid arthritis, and talocalcaneal coalition. This procedure is preferred when pathology is isolated to the subtalar joint, as it preserves hindfoot motion, is relatively simple, and reduces the risk of degenerative changes in adjacent joints compared to triple arthrodesis.
Introduction and Epidemiology
An isolated subtalar arthrodesis is a highly effective surgical intervention utilized in the treatment of a myriad of different hindfoot conditions. Historically, the triple arthrodesis was the workhorse for hindfoot pathology; however, modern orthopedic foot and ankle surgery has shifted toward joint-sparing procedures whenever possible. When the pathologic process resides solely in the talocalcaneal articulation, isolated subtalar arthrodesis is strongly preferred over a triple arthrodesis. This preference is driven by its preservation of transverse tarsal hindfoot motion, its decreased potential for the development of degenerative changes in neighboring joints, its relative technical simplicity, and its significantly lower potential for pseudarthrosis of the talonavicular and calcaneocuboid joints.

The epidemiology of subtalar joint arthritis is heavily skewed toward post-traumatic etiologies. The most common precursor to end-stage subtalar arthrosis is a displaced intra-articular calcaneal fracture, though talar neck and body fractures also contribute significantly to the incidence. Primary arthrosis of the subtalar joint, defined as articular cartilage degeneration of unknown etiology, is relatively rare compared to secondary arthritis caused by traumatic articular cartilage damage or increased joint stresses following an arthrodesis of an adjacent joint.

Inflammatory arthritis, such as rheumatoid arthritis or psoriatic arthritis, represents another significant epidemiological subset, characterized by autoimmune joint destruction that frequently targets the hindfoot complex. Additionally, talocalcaneal coalition, an abnormal fusion between the talus and calcaneus most likely secondary to a failure of segmentation of the primitive mesenchyme, often necessitates surgical fusion when conservative measures fail and degenerative changes have developed.

The natural history of subtalar arthritis, regardless of the specific etiology, is generally progressive in nature. Despite the waxing and waning of clinical symptoms, there is no spontaneous resolution of the underlying pathologic process. As the articular cartilage continues to degrade, patients experience escalating pain, progressive deformity, and severe functional limitations, ultimately necessitating surgical arthrodesis to restore a plantigrade, stable, and pain-free foot.


Surgical Anatomy and Biomechanics
The term subtalar refers to the complex articulation between the anterior, middle, and posterior facets of the inferior talus and the corresponding anterior, middle, and posterior facets located on the superior aspect of the calcaneus. The posterior facet is the largest and bears the majority of the load, making it the primary focus during joint preparation for arthrodesis. The anterior and middle facets are frequently continuous and are separated from the posterior facet by the tarsal canal and sinus tarsi.

The subtalar joint operates as a plane type synovial joint with a relatively weak fibrous capsule. Stability is primarily conferred by robust ligamentous structures, including the medial, lateral, and posterior talocalcaneal ligaments, as well as the critical interosseous talocalcaneal ligament and the cervical ligament residing within the sinus tarsi. The interosseous ligament acts as the primary restraint to excessive eversion, while the cervical ligament resists excessive inversion.

Biomechanically, this important articulation provides for inversion and eversion of the hindfoot. This motion is critical for the proper adaptation of the foot during ambulation on uneven terrain and for the efficient dissipation of heel-strike forces. The subtalar joint functions as a torque transmitter, converting the internal and external rotation of the tibia into pronation and supination of the foot, respectively.

Understanding the coupled motion of the hindfoot is paramount when considering an isolated fusion. The talocalcaneal, talonavicular, and calcaneocuboid joints function synergistically as the acetabulum pedis. Isolated fusions of the subtalar joint have been shown in classic biomechanical studies to reduce talonavicular joint motion by 74 percent and calcaneocuboid joint motion by 44 percent. Therefore, while an isolated subtalar fusion is joint-sparing compared to a triple arthrodesis, it significantly alters the biomechanics of the entire transverse tarsal joint complex, predisposing adjacent joints to long-term degenerative changes.

The vascular anatomy is also critical for surgical planning and healing. The blood supply to the talus is notoriously tenuous, relying heavily on the artery of the tarsal canal (a branch of the posterior tibial artery) and the artery of the sinus tarsi (formed by anastomoses from the perforating peroneal and anterior tibial arteries). Disruption of these vessels during aggressive sinus tarsi dissection can compromise talar perfusion, increasing the risk of nonunion or avascular necrosis.


Indications and Contraindications
The decision to proceed with an isolated subtalar arthrodesis hinges on a precise localization of the pathology to the talocalcaneal joint. Primary indications include primary osteoarthrosis, posttraumatic arthritis secondary to calcaneal or talar fractures, and inflammatory arthritides such as rheumatoid arthritis.

Other significant etiologies that may necessitate an isolated subtalar arthrodesis include instability or deformity secondary to muscular imbalance. This is frequently observed in posterior tibial tendon insufficiency (adult acquired flatfoot deformity), where an isolated subtalar fusion may be utilized to correct flexible or rigid hindfoot valgus while preserving transverse tarsal motion. Neuromuscular disorders presenting with instability of the subtalar joint, such as Charcot-Marie-Tooth disease or sequelae of poliomyelitis, also represent strong indications for this procedure to restore a plantigrade and stable base of support.

Contraindications must be carefully evaluated. Absolute contraindications include active localized or systemic infection, severe peripheral arterial disease that precludes wound healing, and significant medical comorbidities rendering the patient unfit for anesthesia. Relative contraindications include adjacent joint arthritis (talonavicular or calcaneocuboid), which would necessitate a triple arthrodesis rather than an isolated procedure. Active Charcot neuroarthropathy is generally a contraindication for standard arthrodesis until the acute inflammatory phase has consolidated.

| Indication Category | Operative Indications for Subtalar Arthrodesis | Non-Operative Management Strategies |
|---|---|---|
| Post-Traumatic | End-stage arthritis post calcaneus/talus fracture, severe hindfoot malalignment | Custom Arizona brace, rigid AFO, NSAIDs, intra-articular corticosteroid injections |
| Inflammatory | Rheumatoid arthritis with localized subtalar destruction and pain | Disease-modifying antirheumatic drugs (DMARDs), biologic therapies, custom orthotics |
| Degenerative | Primary osteoarthritis unresponsive to conservative care | Activity modification, rocker-bottom shoe modifications, physical therapy |
| Neuromuscular | Charcot-Marie-Tooth with rigid varus, Poliomyelitis with instability | High-top supportive footwear, custom bracing (SMO or AFO) |
| Congenital | Symptomatic talocalcaneal coalition with secondary degenerative changes | Cast immobilization, orthotics, NSAIDs |


Pre Operative Planning and Patient Positioning
A thorough problem-focused history and physical examination are the cornerstones of preoperative planning. The history should include direct questioning regarding the exact nature of the symptoms, specific location, duration, progression, aggravating or alleviating factors, prior therapeutic interventions, and functional disability. Patients typically complain of deep, aching lateral ankle pain and marked difficulty ambulating on uneven terrain. The pain often improves with rest and may be mitigated by wearing high-top shoes or rigid boots.

Physical examination findings consistent with subtalar joint arthritis include hindfoot swelling, tenderness directly within the sinus tarsi, and pain exacerbated by passive inversion and eversion of the hindfoot. An antalgic gait is nearly universal in symptomatic patients. To accurately assess the subtalar joint, the examiner must passively dorsiflex the ankle to neutral to lock the talus within the mortise, thereby isolating subtalar motion. Because descriptions of normal subtalar range of motion vary widely, it is highly useful to describe the range as a fraction of the asymptomatic, contralateral side.

Diagnostic imaging begins with standard weight-bearing radiographs of the foot and ankle, including anteroposterior, lateral, and axial (Harris heel) views. These images evaluate joint space narrowing, subchondral sclerosis, osteophyte formation, and overall hindfoot alignment (varus or valgus). Computed Tomography (CT) is the gold standard for assessing the extent of subtalar arthritis, the presence of subchondral cysts, and bone stock quality, which is critical for planning hardware trajectory and assessing the need for structural bone grafting. Magnetic Resonance Imaging (MRI) is rarely indicated unless there is concern for avascular necrosis of the talus or concurrent soft tissue pathology.

Patient positioning is dictated by surgeon preference and the planned surgical approach. The lateral decubitus position is frequently utilized as it provides excellent, unobstructed access to the lateral hindfoot and sinus tarsi. Alternatively, the patient may be positioned supine with a large bump placed under the ipsilateral hip to internally rotate the leg, bringing the lateral aspect of the foot forward. A well-padded thigh tourniquet is applied to maintain a bloodless surgical field, and fluoroscopy must be positioned to allow for orthogonal views of the hindfoot without compromising the sterile field.



Detailed Surgical Approach and Technique
Incision and Soft Tissue Dissection
The most common surgical approach for an isolated subtalar arthrodesis is the lateral approach, often utilizing a limited Ollier incision or a direct sinus tarsi approach. The incision typically begins at the tip of the lateral malleolus and extends distally and anteriorly toward the base of the fourth metatarsal. Careful subcutaneous dissection is paramount to avoid injury to the intermediate dorsal cutaneous nerve superiorly and the sural nerve inferiorly.

The inferior extensor retinaculum is incised, and the extensor digitorum brevis muscle belly is sharply elevated from its origin on the calcaneus and reflected distally. This exposes the contents of the sinus tarsi. The adipose tissue, cervical ligament, and interosseous talocalcaneal ligament are sharply excised to provide clear visualization of the posterior, middle, and anterior facets. A lamina spreader is then inserted into the sinus tarsi to distract the joint, providing the necessary exposure for meticulous joint preparation.

Joint Preparation and Arthrodesis Site Management
The success of any arthrodesis relies heavily on the meticulous preparation of the articular surfaces. All remaining articular cartilage must be thoroughly denuded from the posterior, middle, and anterior facets of both the talus and the calcaneus using a combination of curettes, osteotomes, and a high-speed burr. It is critical to remove the cartilage down to bleeding subchondral bone while preserving the underlying contour of the joint to maintain inherent stability and prevent excessive shortening of the hindfoot.

Once the cartilage is removed, the subchondral bone plates are penetrated to expose the underlying vascular cancellous bone. This is achieved through aggressive subchondral drilling using a 2.0 mm or 2.5 mm drill bit, or by "fish-scaling" (feathering) the surfaces with a sharp osteotome. This step is vital for allowing the influx of osteoprogenitor cells and vascular ingrowth necessary for bony consolidation.

If there are large subchondral cysts or significant bone loss (frequently encountered in post-traumatic cases or severe rheumatoid arthritis), bone grafting is required. Local autograft obtained from the surgical site may be sufficient, but larger defects may necessitate cancellous autograft harvested from the proximal tibia or iliac crest. Structural allograft or autograft blocks may be required to restore calcaneal height and correct severe varus or valgus malalignment.


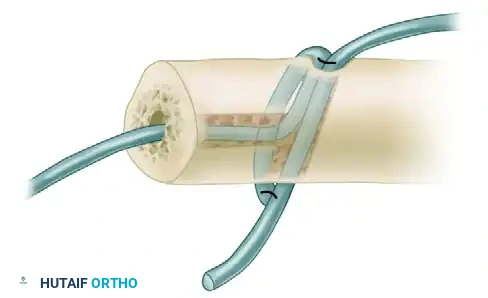
Reduction Mechanics and Hardware Fixation
Correct alignment of the subtalar joint is the most critical biomechanical aspect of the procedure. The hindfoot must be fused in approximately 5 degrees of valgus. Fusion in varus is poorly tolerated, leading to a rigid transverse tarsal joint, lateral column overload, and an increased risk of fifth metatarsal stress fractures and lateral ankle instability. The reduction is provisionally held with smooth Kirschner wires, and the alignment is rigorously checked both clinically and under multi-planar fluoroscopy.

Fixation is typically achieved using large-diameter (6.5 mm to 7.3 mm) cannulated partially threaded screws. The most biomechanically sound construct involves the use of two screws to provide rigid compression and rotational stability. The primary screw is usually directed from the non-weight-bearing portion of the posterior plantar calcaneal tuberosity, traversing the posterior facet, and anchoring into the dense bone of the talar body or neck.

A secondary screw can be placed parallel or divergent to the first screw, often extending into the anterior aspect of the talus, to enhance rotational control. Care must be taken to ensure that the screw threads fully cross the arthrodesis site to achieve maximal interfragmentary compression. Fluoroscopy is utilized to confirm that the hardware does not violate the ankle joint or the talonavicular joint.


Complications and Management
Despite meticulous surgical technique, isolated subtalar arthrodesis is associated with several recognized complications. Pseudarthrosis (nonunion) is the most significant complication, with reported rates ranging from 5 to 15 percent, highly dependent on patient risk factors such as smoking, diabetes, and the presence of avascular necrosis.

Malunion, particularly fusion in varus, is a devastating complication that drastically alters foot biomechanics, leading to lateral border pain and gait dysfunction. Hardware prominence at the heel insertion site can cause significant morbidity, often requiring a secondary procedure for removal once the fusion is fully consolidated. Iatrogenic nerve injury, specifically to the sural nerve or the intermediate dorsal cutaneous nerve, can result in painful neuromas or chronic regional pain syndromes.

Adjacent segment disease is a long-term complication resulting from the altered kinematics of the transverse tarsal joint. Because an isolated subtalar fusion drastically reduces motion at the talonavicular and calcaneocuboid joints, these articulations experience increased stress, often leading to progressive osteoarthrosis over the subsequent decade.

| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Pseudarthrosis (Nonunion) | 5% - 15% | Prevention: Meticulous joint preparation, rigid compression, smoking cessation. Salvage: Revision arthrodesis with structural bone grafting and robust internal fixation. |
| Malunion (Varus/Excessive Valgus) | 2% - 8% | Prevention: Intraoperative clinical and fluoroscopic alignment checks. Target 5 degrees valgus. Salvage: Corrective osteotomy through the fusion mass with revision fixation. |
| Hardware Prominence / Pain | 10% - 20% | Prevention: Countersinking screw heads in the posterior calcaneus. Salvage: Hardware removal after CT confirmation of solid bony union. |
| Sural Nerve Neuritis / Neuroma | 3% - 7% | Prevention: Careful soft tissue handling, utilizing full-thickness flaps. Salvage: Neuroma excision, nerve burying into local muscle or bone. |
| Adjacent Joint Arthrosis | 20% - 40% (Long-term) | Prevention: Achieving optimal hindfoot alignment to minimize abnormal stress transfer. Salvage: Extension of fusion to a triple arthrodesis or specific midfoot fusions. |



Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is designed to protect the arthrodesis site while promoting optimal conditions for bony union. Immediately postoperatively, the patient is placed in a well-padded, short-leg bulky splint and maintained strictly non-weight-bearing. Elevation of the operative extremity is critical during the first two weeks to mitigate edema and minimize the risk of wound dehiscence.

At the two-week follow-up, the surgical splint and sutures are removed. Assuming the incision has healed adequately, the patient is transitioned into a rigid short-leg cast or a controlled ankle motion (CAM) boot. The patient remains strictly non-weight-bearing for an additional four weeks. Radiographs are obtained at the six-week mark to assess for early signs of trabecular bridging across the arthrodesis site.

If radiographic and clinical progression is satisfactory at six weeks, the patient may begin a progressive weight-bearing protocol in the CAM boot. This typically involves advancing from touch-down weight-bearing to full weight-bearing over a four-week period. Formal physical therapy is initiated to address ankle joint range of motion, calf atrophy, and proprioceptive deficits.

By 10 to 12 weeks postoperatively, a CT scan may be obtained if there is any clinical ambiguity regarding union. Once solid fusion is confirmed, the patient is weaned from the CAM boot into a supportive athletic shoe, often utilizing a custom orthotic to support the transverse tarsal joints and accommodate the newly rigid hindfoot. Return to high-impact activities is generally restricted until at least six months postoperatively.

Summary of Key Literature and Guidelines
The academic literature surrounding isolated subtalar arthrodesis provides robust support for its efficacy and delineates best practices for surgical technique. Classic biomechanical studies, notably those by Astion et al., quantified the kinematic coupling of the hindfoot, demonstrating that isolated subtalar fusion drastically reduces adjacent joint motion (74% reduction in talonavicular motion, 44% in calcaneocuboid motion). This data underscores the importance of precise anatomical alignment to prevent accelerated adjacent segment degeneration.

Clinical outcome studies, such as the seminal work by Easley et al., have established that isolated subtalar arthrodesis yields high patient satisfaction and union rates exceeding 85% to
Clinical & Radiographic Imaging

You Might Also Like