Glenohumeral Arthrodesis: Maximize Function, ed Philadelphia Lippincott

Key Takeaway
Here are the crucial details you must know about Glenohumeral Arthrodesis: Maximize Function, ed Philadelphia Lippincott. Glenohumeral arthrodesis is a technically demanding procedure to fuse the shoulder, creating a stable base for the upper extremity to optimize elbow and hand function. It involves meticulous technique, often decorticating joint surfaces. This treatment option is detailed in medical texts like the one edited by Iannotti and Williams, ed Philadelphia Lippincott, for selected patients.
Comprehensive Introduction and Patho-Epidemiology
Despite significant advances in shoulder arthroplasty, reverse total shoulder reconstructive procedures, and complex soft tissue transfers, glenohumeral arthrodesis remains an indispensable treatment modality in appropriately selected patients. The primary goal of glenohumeral arthrodesis is to provide a stable, painless base for the upper extremity, thereby optimizing distal function at the elbow, wrist, and hand. In the setting of an unstable, flail, or profoundly painful shoulder where arthroplasty is strictly contraindicated, fusion establishes a rigid, osseous link between the humerus and the scapula. This allows the robust periscapular musculature—specifically the trapezius, levator scapulae, rhomboids, and serratus anterior—to motor the entire upper extremity via the scapulothoracic articulation.

The epidemiology of glenohumeral arthrodesis has shifted dramatically over the past several decades, reflecting broader changes in global public health and orthopedic innovation. Historically, this procedure was frequently performed to manage the debilitating sequelae of anterior poliomyelitis or tuberculosis of the shoulder. In these historical cohorts, flaccid paralysis of the deltoid and rotator cuff, combined with a relatively preserved periscapular motor unit, made arthrodesis the gold standard for restoring upper extremity utility. In contemporary orthopedic practice, the incidence of primary glenohumeral arthrodesis has decreased due to the advent and widespread success of the reverse total shoulder arthroplasty (RTSA), which can effectively manage rotator cuff arthropathy and certain cases of pseudoparalysis.

However, glenohumeral arthrodesis is still heavily utilized as a definitive salvage procedure in tertiary referral centers. Current epidemiological trends indicate that the most common contemporary indications include severe high-energy brachial plexus injuries, isolated irreparable axillary nerve palsies, salvage of failed total shoulder arthroplasty with massive uncontained glenoid bone loss, chronic indolent periprosthetic joint infections, and limb-sparing oncologic resections. The demographic profile of the modern arthrodesis patient is often distinctly bimodal: young, predominantly male patients suffering from high-energy traumatic brachial plexus palsies (often motorcycle accidents), and older patients facing catastrophic failure of primary or revision shoulder arthroplasty.

Given the tremendous normal range of motion of the native glenohumeral joint and the relatively small amount of surface area available for osseous fusion—particularly on the scapular side—successful arthrodesis is technically demanding and fraught with potential pitfalls. It requires meticulous surgical technique, precise intraoperative positioning, and rigid internal fixation to prevent nonunion or catastrophic hardware failure. The physiological burden of the procedure is significant, as it permanently alters the biomechanical vectors of the shoulder girdle, transferring all mechanical stress to the scapulothoracic articulation and the acromioclavicular and sternoclavicular joints, which may predispose these joints to accelerated degenerative changes over time.

Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Morphology
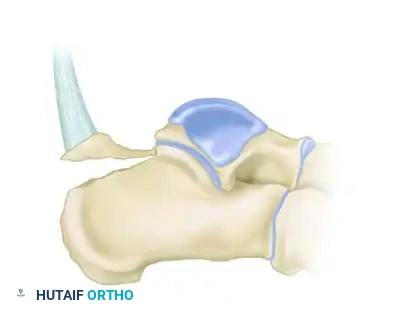
The glenohumeral joint is inherently unstable due to the profound mismatch in surface area between the large, spherical humeral head and the shallow, pyriform glenoid fossa. In the context of arthrodesis, this osteological mismatch presents a significant challenge for achieving adequate osseous contact and subsequent fusion. The glenoid provides a relatively small surface area for decortication; therefore, to maximize the fusion mass, the arthrodesis construct must frequently incorporate the undersurface of the acromion. This establishes a dual-site fusion mass—an intra-articular glenohumeral fusion and an extra-articular acromiohumeral fusion—which significantly increases the overall biomechanical rigidity of the construct.

The scapular spine serves as a critical osseous landmark and the primary structural buttress for internal fixation. The dense cortical bone of the scapular spine provides excellent purchase for the proximal screws of the fixation plate, which is typically contoured to run from the medial aspect of the scapular spine, over the acromion, and down the lateral aspect of the humeral shaft. The trajectory of these proximal screws must be carefully planned to maximize cortical engagement while avoiding penetration of the suprascapular notch or the spinoglenoid notch, which house the vital suprascapular nerve and vessels.

Distally, the lateral cortex of the humeral shaft provides the necessary structural support for the distal extent of the fixation plate. The humerus must be adequately mobilized to allow for precise positioning relative to the scapula. The deltoid tuberosity serves as a landmark for the distal extension of the plate, and care must be taken to ensure that screws placed in this region do not inadvertently injure the radial nerve as it spirals through the spiral groove on the posterior aspect of the humerus. The quality of the humeral bone stock, particularly in revision arthroplasty settings where stress shielding or osteolysis may be present, dictates the type of fixation (locking versus non-locking) required.

Neuromuscular Topography and Periscapular Motors
The success of a glenohumeral arthrodesis is entirely dependent on the integrity and strength of the periscapular musculature. Once the glenohumeral joint is fused, the upper extremity functions as a single, elongated lever arm extending directly from the scapulothoracic articulation. The trapezius (innervated by the spinal accessory nerve, CN XI) and the serratus anterior (innervated by the long thoracic nerve, C5-C7) are the primary motors for scapular upward rotation, elevation, and protraction. Without the robust function of these two muscles, the fused limb will remain functionally useless and act as a dead weight.

The levator scapulae and rhomboids (innervated by the dorsal scapular nerve, C5) assist in scapular elevation and retraction, providing necessary stabilization during dynamic movements of the fused limb. In the setting of a brachial plexus injury, it is absolutely imperative to clinically and electrodiagnostically verify the function of these nerves prior to offering an arthrodesis. If the trapezius and serratus anterior are paralyzed, a glenohumeral arthrodesis is strictly contraindicated, as the procedure will result in a flail, heavy limb that causes severe downward traction on the brachial plexus, debilitating neck pain, and profound scapular winging.

Meticulous dissection is required to protect the regional neurovascular structures during the surgical approach. During the superior approach, the suprascapular nerve is at significant risk as it traverses the suprascapular notch beneath the superior transverse scapular ligament and winds around the spinoglenoid notch. Aggressive retraction, errant screw placement in the base of the coracoid, or misdirected drilling through the lateral scapular spine can cause devastating iatrogenic injury to this nerve, compromising the supraspinatus and infraspinatus (if they are still functioning and relevant to the clinical picture).

Kinematic Alterations and Scapulothoracic Dynamics
The biomechanics of the shoulder are fundamentally and permanently altered following glenohumeral arthrodesis. Normal shoulder abduction is a synergistic movement involving a roughly 2:1 ratio of glenohumeral to scapulothoracic motion. Post-arthrodesis, this ratio is obliterated; 100% of upper extremity elevation occurs via the scapulothoracic articulation. Consequently, the massive mechanical stresses normally dissipated by the mobile glenohumeral joint are transferred directly to the acromioclavicular (AC) and sternoclavicular (SC) joints, predisposing them to accelerated degenerative changes and potential future symptomatology.

The optimal position for arthrodesis has evolved significantly over the past half-century. Early literature recommended high degrees of abduction (up to 60 degrees) to maximize overhead reach. However, this non-anatomic position resulted in severe scapular winging at rest, chronic trapezius fatigue, debilitating neck pain, and an inability to rest the arm at the side. Modern biomechanical studies and long-term clinical outcomes strongly support a more conservative position, often referred to as the "functional position" or a modification of Rowe's original positioning criteria.

The current consensus for optimal positioning dictates 20 to 30 degrees of abduction relative to the lateral border of the scapula, 20 to 30 degrees of flexion, and 20 to 30 degrees of internal rotation. The degree of internal rotation is perhaps the most critical parameter for postoperative independence. The patient must be able to reach their mouth and the midline of their body. Excessive external rotation severely limits functional independence, rendering the patient completely unable to feed themselves, button a shirt, or perform essential perineal hygiene.

Exhaustive Indications and Contraindications
Primary and Salvage Surgical Indications
The decision to proceed with glenohumeral arthrodesis requires rigorous, multidisciplinary patient selection. The procedure is irreversible and represents the absolute end of the reconstructive line for the shoulder joint. It is imperative to weigh the potential functional gains—namely, stability and pain relief—against the permanent loss of glenohumeral motion and the substantial physiological demand placed on the periscapular musculature. In patients with C5-C6 or C5-C7 root avulsions, the deltoid and rotator cuff are typically paralyzed, resulting in a flail, unstable shoulder. Arthrodesis provides a stable fulcrum that significantly improves the function of distal nerve transfers (e.g., Steindler flexorplasty) by preventing the shoulder from dissipating the force of the transferred muscle.

In the realm of salvage procedures, glenohumeral arthrodesis serves as a definitive reconstructive option following explantation and eradication of an offending pathogen in chronic periprosthetic joint infection (PJI). The incidence of PJI in shoulder arthroplasty ranges from 1% to 2%, but in cases of recurrent infection involving virulent or indolent organisms (e.g., Cutibacterium acnes, Methicillin-resistant Staphylococcus aureus), multiple revision arthroplasties are associated with diminishing functional returns and escalating complication rates. Arthrodesis eliminates the dead space of the joint cavity, provides a stable, vascularized environment conducive to infection eradication, and restores a functional baseline.

Catastrophic failure of total shoulder arthroplasty (TSA) or reverse total shoulder arthroplasty (RTSA) characterized by massive, uncontained glenoid bone loss, periprosthetic fracture, or severe rotator cuff and deltoid deficiency often precludes further revision arthroplasty. In these scenarios, the remaining bone stock is often insufficient to support a new glenoid baseplate. Arthrodesis, often requiring massive structural allografts or vascularized fibular grafts to span the osseous defect, provides the only viable alternative to a flail shoulder or forequarter amputation.

Absolute and Relative Contraindications
Absolute contraindications to glenohumeral arthrodesis revolve primarily around the neuromuscular integrity of the shoulder girdle. As previously emphasized, paralysis or profound weakness of the trapezius and serratus anterior muscles entirely precludes this procedure. Without these primary periscapular motors, the fused humerus and scapula will act as a massive, unyielding weight, leading to severe traction neuropathies of the remaining brachial plexus, intractable cervical spine pain, and catastrophic scapular winging. Clinical examination, supplemented by electromyography (EMG), must confirm the function of the spinal accessory and long thoracic nerves.

Active, untreated, or uncontrolled local infection is another absolute contraindication. While arthrodesis is an excellent salvage for PJI, it must be performed as a staged procedure. The primary joint must be aggressively debrided, all hardware explanted, and an antibiotic spacer placed, followed by a prolonged course of culture-directed intravenous antibiotics. Attempting an osseous fusion in the presence of active purulence guarantees nonunion, persistent sepsis, and eventual hardware failure. Furthermore, Charcot arthropathy of the shoulder (neuropathic joint) is a strong relative, if not absolute, contraindication due to the exceptionally high rates of nonunion and hardware pullout in dysvascular, insensate bone.

Relative contraindications include severe ipsilateral elbow or hand dysfunction. Because arthrodesis fixes the shoulder in a static position, the patient relies entirely on elbow flexion/extension and wrist mobility to position the hand in space. If the elbow is stiff or the hand is non-functional, fusing the shoulder may actually decrease the patient's overall functional envelope. Advanced physiological age and poor medical comorbidities that preclude a lengthy, blood-loss-heavy surgical procedure also represent relative contraindications. Patient compliance is paramount; those unable to adhere to strict postoperative immobilization protocols are at high risk for construct failure.
| Category | Indications | Contraindications |
|---|---|---|
| Neurological | Brachial plexus palsy (intact trapezius/serratus), Isolated axillary nerve palsy | Paralysis of trapezius or serratus anterior, Charcot neuropathic arthropathy |
| Infectious | Staged salvage of chronic PJI (post-eradication) | Active, untreated, or uncontrolled local infection |
| Arthroplasty | Failed TSA/RTSA with massive glenoid bone loss, severe cuff/deltoid deficiency | Functioning arthroplasty options available, adequate bone stock for revision |
| Oncologic/Trauma | Limb-sparing tumor resection, severe comminuted intra-articular fractures (unreconstructable) | Severe ipsilateral elbow/hand dysfunction (relative), poor patient compliance |

Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Three-Dimensional Templating
Thorough preoperative planning is the cornerstone of a successful glenohumeral arthrodesis. Standard orthogonal radiographs (true anteroposterior, scapular Y, and axillary lateral views) are mandatory but insufficient for complex salvage cases. A high-resolution computed tomography (CT) scan with three-dimensional (3D) reconstructions is essential to evaluate the remaining osseous architecture of the glenoid vault and the humeral head. In the setting of failed arthroplasty, the CT scan allows the surgeon to quantify the volume of bone loss, determine the necessity and size of structural bone grafts, and plan the trajectory of the fixation screws to maximize cortical purchase.

Advanced 3D templating software is increasingly utilized to simulate the arthrodesis preoperatively. By virtually resecting residual cartilage or hardware and manipulating the humerus into the optimal functional position (20-30 degrees of abduction, flexion, and internal rotation relative to the scapula), the surgeon can anticipate the required plate contour and screw lengths. This virtual rehearsal is particularly valuable in cases with severe anatomic distortion, allowing for the design of patient-specific instrumentation (PSI) or custom-milled structural allografts that perfectly match the patient's cavitary defects.

Magnetic resonance imaging (MRI) or ultrasound may be indicated to evaluate the integrity of the periscapular musculature if there is any clinical ambiguity regarding their function. Fatty infiltration or profound atrophy of the trapezius or serratus anterior on MRI serves as a definitive warning sign that the patient may not possess the motor strength required to utilize the fused limb. Additionally, preoperative infectious workups, including serum inflammatory markers (ESR, CRP) and joint aspirations for cell count and extended cultures, are mandatory in all revision scenarios to rule out indolent PJI.

Patient Positioning and Intraoperative Fluoroscopy
Patient positioning for glenohumeral arthrodesis is a subject of debate, with both the beach chair and lateral decubitus positions offering distinct advantages. The beach chair position is favored by many because it allows for a more anatomic assessment of the arm's resting posture relative to the torso. It facilitates the superior and posterior surgical approaches and provides excellent access to the superior aspect of the scapular spine and the acromion. However, assessing the exact scapulothoracic angle can be challenging in the beach chair position because the scapula is often pinned against the operating table.

Conversely, the lateral decubitus position allows the scapula to fall forward, freeing it from the constraints of the table. This complete mobility of the forequarter makes it significantly easier to measure the critical angles of arthrodesis relative to the lateral border of the scapula, rather than the thorax. A sterile Mayo stand or custom arm holder can be used to support the arm in the desired position during plate application. Regardless of the chosen position, the entire forequarter, from the base of the neck to the fingertips, must be prepped and draped free to allow for unencumbered manipulation of the limb.

Intraoperative fluoroscopy is absolutely critical and must be positioned and tested prior to incision. The C-arm should be brought in from the contralateral side or the head of the bed, ensuring that orthogonal views of the glenohumeral joint, the scapular spine, and the humeral shaft can be obtained without compromising the sterile field. Fluoroscopy is used to confirm the seating of structural grafts, verify the trajectory of screws (particularly those aimed at the base of the coracoid to avoid the suprascapular notch), and ensure that no hardware is penetrating the articular surface of the acromioclavicular joint.

Anesthetic Considerations and Neuromonitoring
The anesthetic plan must be carefully coordinated with the surgical team. General anesthesia is standard, often supplemented with a regional interscalene or supraclavicular nerve block to manage postoperative pain. However, if intraoperative neuromonitoring (IONM) is utilized—which is highly recommended in post-traumatic brachial plexus cases or complex revisions where the anatomy of the axillary, suprascapular, or musculocutaneous nerves is distorted—long-acting paralytic agents must be strictly avoided.

Blood loss during a glenohumeral arthrodesis can be substantial, particularly during the decortication of the glenoid and the preparation of the scapular spine. The anesthesiologist should be prepared for potential hemodynamic shifts, and large-bore intravenous access or a central line may be indicated. Tranexamic acid (TXA) should be administered preoperatively and prior to closure, barring any strict medical contraindications, to minimize perioperative blood loss and reduce the need for allogeneic blood transfusions.

Step-by-Step Surgical Approach and Fixation Technique
Optimal Surgical Approaches and Exposure
The most widely utilized approach for glenohumeral arthrodesis is a broad superior approach, often described as a "saber cut" incision. The incision begins at the posterior aspect of the scapular spine, extends anteriorly over the acromion, and curves distally down the anterolateral aspect of the humerus. This extensile exposure provides unparalleled access to the three critical zones of fixation: the scapular spine, the glenohumeral articulation, and the humeral shaft. Subcutaneous flaps are elevated to expose the deltoid fascia.

The deltoid muscle is split in line with its fibers distally, and its origin is sharply detached from the anterior, lateral, and posterior acromion. In salvage cases where the deltoid is already paralyzed or absent, this step is simplified, but care must still be taken to preserve any remaining vascularity to the skin flaps. The rotator cuff, if present, is excised to fully expose the humeral head and the glenoid face. The undersurface of the acromion is thoroughly denuded of soft tissue to prepare it as a secondary site for osseous fusion.
Meticulous hemostasis is critical during the exposure. The circumflex humeral vessels and the axillary nerve must be identified and protected as they traverse the quadrangular space, particularly when extending the humeral dissection distally. The suprascapular nerve is protected by avoiding aggressive retraction medial to the base of the coracoid and by maintaining a safe distance from the spinoglenoid notch when dissecting along the posterior scapular neck.
Joint Preparation and Osseous Decortication
The success of the arthrodesis relies entirely on the quality of the biological environment created at the fusion interfaces. The articular cartilage of both the glenoid and the humeral head must be aggressively resected down to bleeding, punctate cancellous bone. This is typically achieved using a combination of high-speed burrs, curved osteotomes, and curettes. The subchondral bone plate must be breached to allow for the influx of osteoprogenitor cells and robust neovascularization from the underlying medullary canals.
To maximize the contact area, the undersurface of the acromion and the superior aspect of the humeral head are similarly decorticated. The humerus is then manually reduced into the glenoid fossa and translated superiorly to engage the acromion. This creates a highly stable, dual-interface fusion mass. In cases of severe bone loss (e.g., post-explantation of a failed RTSA), the cavitary defects must be meticulously packed with autogenous bone graft (typically harvested from the anterior or posterior iliac crest) or structural allograft.