Complete Wrist Arthrodesis
Introduction and Epidemiology
Complete wrist arthrodesis represents the definitive surgical salvage procedure for end-stage, pan-carpal arthritis and severe structural instability of the radiocarpal and midcarpal joints. While joint-preserving procedures (e.g., proximal row carpectomy) and partial arthrodeses (e.g., four-corner fusion) are prioritized in early-stage degenerative disease, complete wrist arthrodesis remains the gold standard for providing durable, predictable pain relief and establishing a stable kinetic chain for power grip. By permanently eliminating motion across the radiocarpal, midcarpal, and carpometacarpal (CMC) articulations, the procedure sacrifices spatial positioning of the hand in exchange for robust mechanical stability.
Historically, the most common indication for complete wrist arthrodesis was advanced, destructive rheumatoid arthritis (RA). However, the advent of disease-modifying antirheumatic drugs (DMARDs) and targeted biologic therapies has dramatically altered the epidemiological landscape of wrist arthropathy. Currently, post-traumatic osteoarthritis constitutes the primary indication in the developed world. This encompasses end-stage scapholunate advanced collapse (SLAC), scaphoid nonunion advanced collapse (SNAC), and intra-articular distal radius fracture malunions with secondary joint degeneration.
Other less frequent but significant etiologies include crystalline arthropathies (gout, pseudogout), primary generalized osteoarthritis, Kienböck disease with pan-carpal collapse (Lichtman Stage IV), neuromuscular disorders presenting with severe spasticity or paralytic deformities (e.g., cerebral palsy, brachial plexus birth palsy), and salvage following failed total wrist arthroplasty (TWA) or failed limited intercarpal fusions. The procedure is predominantly performed in younger, high-demand manual laborers who require maximal grip strength and cannot adhere to the strict functional and weight-bearing restrictions mandated by total wrist arthroplasty.
Surgical Anatomy and Biomechanics
The wrist is an exquisitely complex biomechanical linkage comprising the distal radius, the triangular fibrocartilage complex (TFCC), eight carpal bones, and the bases of the metacarpals. These osseous structures are governed by a highly sophisticated array of intrinsic ligaments (e.g., scapholunate and lunotriquetral interosseous ligaments) and extrinsic capsular ligaments (e.g., radioscaphocapitate, radiolunotriquetral).
Functionally, the carpus is divided into two distinct rows. The distal carpal row, consisting of the trapezium, trapezoid, capitate, and hamate, functions as a tightly bound unit that moves synchronously with the metacarpals via rigid CMC articulations. The proximal carpal row, encompassing the scaphoid, lunate, and triquetrum, acts as an intercalated segment. It possesses no direct tendinous insertions; instead, it relies entirely on articular contact morphology and ligamentous constraints to dictate its spatial orientation during radiocarpal and midcarpal motion.

Wrist arthritis fundamentally occurs when these codependent joints lose the ability to rotate and translate normally around one another, thereby impairing wrist kinematics. Single ligament disruptions, such as a scapholunate interosseous ligament tear, alter the transmission of forces across the radiocarpal joint. This leads to predictable patterns of cartilage wear—beginning at the radioscaphoid styloid, progressing to the entire radioscaphoid fossa, and eventually encompassing the capitolunate articulation (SLAC pattern).
From a biomechanical perspective, complete wrist arthrodesis profoundly alters the function of the upper extremity. Because spatial positioning of the hand is lost at the wrist, compensatory motion must occur at the elbow, shoulder, and trunk. However, the fusion position is critical for optimizing the remaining function of the hand. The wrist is optimally fused in 10 to 15 degrees of extension and slight ulnar deviation. This specific orientation maximizes the length-tension relationship of the extrinsic digital flexors (flexor digitorum profundus and superficialis), thereby optimizing grip strength. Excessive extension can lead to extensor tendon irritation and fatigue, while fusion in flexion severely compromises power grip due to active insufficiency of the finger flexors.
Indications and Contraindications
The decision to proceed with complete wrist arthrodesis requires careful evaluation of the patient's functional demands, pain levels, and the integrity of surrounding joints (particularly the distal radioulnar joint, elbow, and shoulder). A comprehensive understanding of the indications and contraindications is paramount for achieving optimal surgical outcomes.
| Clinical Scenario | Operative Indications | Non-Operative Indications and Contraindications |
|---|---|---|
| Post-Traumatic Osteoarthritis | SLAC/SNAC Stage III or IV with severe pain; failed conservative management; high-demand manual laborer. | SLAC/SNAC Stage I or II (consider limited fusion or PRC); asymptomatic radiographic disease. |
| Rheumatoid Arthritis | End-stage destruction; severe volar subluxation; failed medical management; painful instability. | Well-controlled disease with preserved motion; low-demand patient suitable for total wrist arthroplasty. |
| Neuromuscular Disorders | Severe spastic flexion contractures (e.g., cerebral palsy) causing hygiene issues or skin breakdown. | Quadriplegia relying on tenodesis grasp (ABSOLUTE CONTRAINDICATION to fusion in neutral/extension). |
| Salvage Procedures | Failed total wrist arthroplasty; infected arthroplasty (after clearance); failed partial arthrodesis. | Active deep soft tissue or bone infection (requires staged management with cement spacers). |
| Patient Factors | Intractable pain limiting ADLs; willingness to sacrifice motion for strength and stability. | Open physes (relative contraindication); poor soft tissue envelope; active smoking (relative); non-compliance. |
A critical absolute contraindication exists in patients with cervical spinal cord injuries (e.g., C6 quadriplegia) who rely on the tenodesis effect. These patients utilize active wrist extension (via preserved extensor carpi radialis longus/brevis) to passively flex the digits for grasping objects. Fusing the wrist eliminates this tenodesis effect, profoundly devastating the patient's independence and functional capacity.
Pre Operative Planning and Patient Positioning
Preoperative evaluation begins with a meticulous physical examination to assess the quality of the soft tissue envelope, the presence of prior surgical incisions, and the status of the extrinsic tendons. Grip strength and digital range of motion should be documented. The distal radioulnar joint (DRUJ) must be carefully assessed; if concurrent DRUJ arthritis is present, a concomitant procedure such as a Darrach resection or Sauvé-Kapandji procedure must be planned.
Standard posteroanterior, lateral, and oblique radiographs of the wrist are mandatory. These images confirm the extent of pan-carpal arthritis and help evaluate the bone stock available for hardware fixation. In cases of significant deformity, bone loss, or when planning a salvage procedure for a failed total wrist arthroplasty, a computed tomography (CT) scan without contrast is highly recommended. The CT scan provides a three-dimensional understanding of cystic changes, subchondral sclerosis, and structural defects, assisting in determining the need for structural autograft or allograft.
Templating is performed to select the appropriate implant. Modern fixation typically utilizes a specialized dorsal wrist fusion plate. These plates are pre-contoured with a built-in extension angle of 10 to 15 degrees and possess a hybrid hole configuration accommodating both locking and non-locking screws. The surgeon must determine whether a straight plate or a plate with a radial or ulnar bend is required, depending on the patient's anatomy and the planned axis of fixation (usually down the third metacarpal, though the second metacarpal is an alternative in specific deformities or when the third metacarpal is compromised).
The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Intravenous antibiotics are administered prior to tourniquet inflation. The ipsilateral iliac crest should be prepped and draped if autogenous structural bone grafting is anticipated, although local cancellous bone graft from the distal radius or advanced allograft matrices are frequently sufficient for primary arthrodesis. Fluoroscopy (C-arm) is positioned either parallel to the hand table or coming in from the distal end to allow for unencumbered orthogonal intraoperative imaging.
Detailed Surgical Approach and Technique
Incision and Superficial Dissection
A dorsal longitudinal incision is utilized, typically measuring 10 to 12 centimeters. The incision is centered over Lister's tubercle and extends distally along the axis of the third metacarpal. Careful subcutaneous dissection is performed. It is imperative to identify and retract the dorsal sensory branches of the radial nerve (SRN) radially, and the dorsal branch of the ulnar nerve (DBUN) ulnarly. Hemostasis is achieved using bipolar electrocautery to minimize thermal injury to adjacent cutaneous nerves and preserve the delicate dorsal venous network.
Extensor Retinaculum and Tendon Management
The extensor retinaculum is exposed. The third dorsal compartment is opened longitudinally, and the extensor pollicis longus (EPL) tendon is mobilized and transposed radially. This tendon will be left in the subcutaneous tissues during closure to prevent attrition against the dorsal hardware. The second compartment (ECRL, ECRB) and fourth compartment (EDC, EIP) are then elevated subperiosteally from the distal radius. It is critical to elevate these compartments in a manner that preserves the underlying dorsal radiocarpal capsule, often utilizing a step-cut technique in the retinaculum to facilitate robust closure later.
Capsulotomy and Joint Exposure
A ligament-sparing dorsal capsulotomy is performed. A radially based rectangular flap or an inverted T-shaped capsulotomy provides excellent exposure of the radiocarpal and midcarpal joints while preserving capsular tissue for subsequent hardware coverage. The capsular flaps are tagged with heavy non-absorbable sutures for later repair.

Articular Surface Preparation
The success of the arthrodesis relies entirely on meticulous joint preparation. The articular cartilage and subchondral bone of the radiocarpal joint (radioscaphoid and radiolunate fossae), the midcarpal joint (scaphotrapezial, scaphocapitate, lunocapitate, and triquetrohamate articulations), and the third carpometacarpal joint must be denuded.
Using a combination of sharp osteotomes, rongeurs, and a high-speed motorized burr under constant saline irrigation, the surgeon decorticates these surfaces down to healthy, bleeding cancellous bone (the "paprika sign"). The second carpometacarpal joint may also be included if arthritic or if the plate will span this articulation. The proximal pole of the scaphoid and the lunate are often sclerotic, cystic, or avascular; aggressive decortication or partial excision of these necrotic segments is necessary to prevent nonunion.
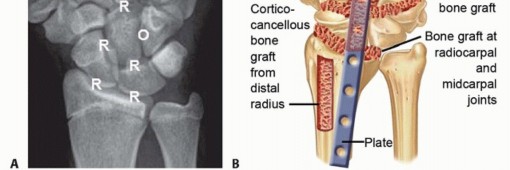
Bone Grafting Strategies
The interstices created by the joint decortication must be densely packed with bone graft to provide osteoconductive and osteoinductive properties. Local cancellous autograft can be harvested from the distal radius metaphysis via a separate cortical window proximal to the fusion site or directly from Lister's tubercle. Alternatively, if a large structural defect exists (e.g., following TWA extraction), iliac crest bone graft is harvested. The graft is morselized and impacted tightly into the radiocarpal, midcarpal, and carpometacarpal spaces.

Osteosynthesis and Plate Application
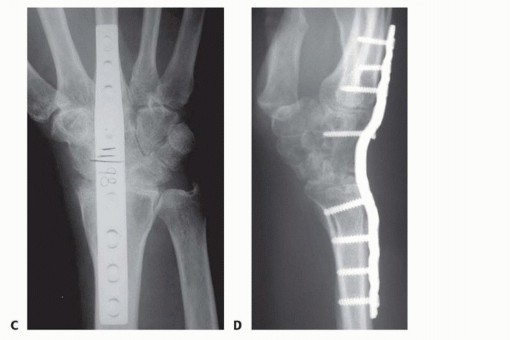
A pre-contoured dorsal wrist fusion plate is selected. The plate is positioned such that the distal segment rests securely on the dorsal diaphysis of the third metacarpal, the central segment spans the carpus, and the proximal segment lies on the flat dorsal surface of the distal radius.
Temporary fixation is achieved using smooth Kirschner wires or olive wires. Fluoroscopy confirms plate positioning in both AP and lateral planes, ensuring that the hardware does not impinge on the metacarpophalangeal joint distally or the distal radioulnar joint proximally.
Screw insertion follows a specific sequence to maximize compression across the fusion mass based on AO principles. First, a non-locking cortical screw is placed in the slotted hole of the third metacarpal to appose the plate to the bone. Next, a non-locking screw is placed in the slotted hole of the distal radius. Using the dynamic compression principle, eccentric drilling is performed to compress the carpus longitudinally between the radius and the metacarpal. Once adequate compression is verified fluoroscopically, the remaining holes are filled. Locking screws are highly recommended in the distal radius and metacarpal to construct a fixed-angle construct, particularly in osteopenic bone. A central screw is often directed through the plate into the capitate to secure the intercalated carpal segment and prevent volar subluxation of the carpus.
Closure and Soft Tissue Coverage
Following final fluoroscopic verification of hardware placement, screw length, and joint reduction, the tourniquet is deflated, and meticulous hemostasis is obtained. The dorsal capsular flaps are closed tightly over the fusion plate using non-absorbable or slowly absorbable braided sutures. This capsular interposition is a critical step to isolate the extensor tendons from the rigid titanium or stainless steel plate, thereby minimizing the risk of postoperative extensor tendon tenosynovitis or attritional rupture.
The extensor retinaculum is repaired over the extensor digitorum communis tendons, leaving the extensor pollicis longus transposed in the subcutaneous tissue. The skin is closed in a layered fashion, and a bulky, sterile compressive dressing incorporating a volar plaster splint is applied.
Complications and Management
Despite rigorous surgical technique, complete wrist arthrodesis carries a distinct complication profile. Surgeons must be prepared to identify and manage these issues promptly to preserve upper extremity function.

| Complication | Estimated Incidence | Etiology and Pathophysiology | Management and Salvage Strategies |
|---|---|---|---|
| Nonunion (Pseudarthrosis) | 3% - 10% | Inadequate joint decortication, insufficient bone grafting, smoking, or micro-motion. Most common at the 3rd CMC joint due to stress shielding. | Asymptomatic nonunions may be observed. Symptomatic nonunions require revision osteosynthesis, aggressive debridement, and structural iliac crest bone grafting. |
| Hardware Prominence and Tendon Irritation | 10% - 20% | Inadequate capsular coverage over the dorsal plate; prominent screw heads; thin soft tissue envelope. | Conservative management with therapy and NSAIDs. Persistent tenosynovitis or impending rupture necessitates hardware removal after radiographic confirmation of solid fusion. |
| Extensor Tendon Rupture | 1% - 3% | Attritional wear of the EDC or EPL tendons against the dorsal plate or sharp screw edges. | Hardware removal. Tendon reconstruction using intercalary grafts or tendon transfers (e.g., Extensor Indicis Proprius to EDC). |
| Carpal Tunnel Syndrome | 2% - 5% | Altered carpal arch mechanics post-fusion; postoperative hematoma; prolonged positioning in extension. | Acute postoperative CTS requires emergent hematoma evacuation and carpal tunnel release. Delayed CTS is managed with standard open carpal tunnel release. |
| Deep Surgical Site Infection | 1% - 2% | Poor soft tissue envelope, particularly in rheumatoid patients on immunosuppressive biologic therapies. | Prompt operative irrigation and debridement. Suppressive antibiotics. Hardware may be retained if stable, but must be removed if loosening occurs, followed by external fixation. |
| Complex Regional Pain Syndrome | < 5% | Abnormal autonomic response to surgical trauma, prolonged immobilization, or unrecognized nerve injury. | Aggressive early mobilization of digits. Multidisciplinary pain management, gabapentinoids, and stellate ganglion blocks. |
The third carpometacarpal joint represents the most frequent site of nonunion. This occurs because the rigid dorsal plate bypasses the mechanical load, leading to stress shielding of the CMC joint. To mitigate this, some surgeons advocate for omitting the decortication of the 3rd CMC joint if it is completely free of arthritic change, though standard AO technique recommends its inclusion to create a monolithic osseous block.
Post Operative Rehabilitation Protocols
The immediate postoperative phase focuses on edema control, pain management, and the absolute prevention of digital stiffness. The patient is discharged in the bulky surgical splint, which immobilizes the wrist but must allow for full, unencumbered metacarpophalangeal (MCP) and interphalangeal (IP) joint motion.
At 10 to 14 days postoperatively, the patient returns to the clinic for suture removal and wound evaluation. Radiographs are obtained to ensure maintenance of hardware position and alignment. The patient is then transitioned to a short arm fiberglass cast or a custom-molded rigid thermoplastic splint.
Strict elevation and immediate active range of motion of the fingers, thumb, elbow, and shoulder are initiated. Occupational therapy plays a vital role during this phase to guide tendon gliding exercises, preventing extrinsic tendon adhesions and intrinsic tightness.
Immobilization is typically maintained for 6 to 8 weeks. At the 6-week mark, serial radiographs are evaluated for evidence of trabecular bridging across the arthrodesis sites. Once clinical stability (absence of pain with stress) and radiographic consolidation are confirmed, the cast is discontinued. The patient is transitioned to a removable splint for high-risk activities and begins a progressive strengthening program. Maximal grip strength recovery is a prolonged process and can take up to 12 to 18 months following the procedure. High-demand laborers may require work hardening programs prior to full occupational release.
Summary of Key Literature and Guidelines
The evolution of complete wrist arthrodesis is well-documented in orthopedic literature, transitioning from uninstrumented cast immobilization to advanced rigid internal fixation.
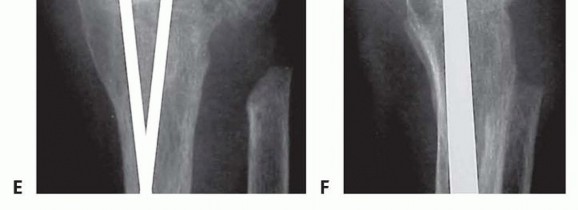
Early techniques, such as those described by Mannerfelt and Malmsten in the 1970s, utilized intramedullary Steinmann pins, particularly in rheumatoid patients. While effective for deformity correction, these constructs lacked rotational stability, frequently backed out, and required prolonged cast immobilization, leading to profound digital stiffness.
The introduction of rigid dorsal plate fixation by the AO Foundation revolutionized the procedure. Hastings et al. published seminal work demonstrating that rigid plate fixation combined with local bone grafting yielded union rates exceeding 95% and allowed for earlier mobilization. The AO principles of absolute stability—achieved via dynamic compression and fixed-angle locking screws—remain the contemporary standard of care.
Recent comparative literature frequently evaluates total wrist arthroplasty (TWA) versus complete wrist arthrodesis. While TWA offers the distinct advantage of motion preservation and is highly successful in low-demand rheumatoid patients, long-term survivorship studies indicate high rates of implant loosening, subsidence, and catastrophic failure in active, post-traumatic osteoarthritis patients. Consequently, current clinical guidelines from the American Society for Surgery of the Hand (ASSH) and the American Academy of Orthopaedic Surgeons (AAOS) firmly support complete wrist arthrodesis as the procedure of choice for young, high-demand individuals requiring durable, lifetime resolution of pan-carpal arthritic pain. Future directions in the field focus on optimizing plate metallurgy, reducing plate profile to minimize tendon attrition, and utilizing advanced orthobiologics (e.g., rhBMP-2, cellular allografts) to accelerate fusion mass consolidation in high-risk nonunion patients.
You Might Also Like

