Masterclass: Corrective Calcaneal Osteotomy & Subtalar Arthrodesis for Malunion
Key Takeaway
This masterclass guides fellows through calcaneal osteotomy and subtalar arthrodesis for malunited fractures. We cover intricate anatomy, meticulous preoperative planning, and a granular, real-time intraoperative execution. Learn precise instrument use, critical decision-making, and techniques to restore hindfoot alignment and function, addressing post-traumatic arthritis and impingement. Pearls for avoiding pitfalls and managing complications are also discussed.
Alright, team, gather 'round. Welcome to the operating theater. Today, we're tackling a challenging case: a calcaneal malunion requiring a corrective osteotomy and subtalar arthrodesis. This isn't just about fixing a bone; it's about restoring the intricate biomechanics of the hindfoot, alleviating chronic pain, and preventing further degenerative changes. These malunions are complex, often presenting with a constellation of issues from post-traumatic arthritis to neurovascular impingement. Our goal is to systematically address each component of the deformity.
Understanding the Pathology: Why This Surgery Matters
A malunited calcaneal fracture is far more than just a crooked heel. The initial trauma, often a high-energy axial load, disrupts the normal architecture of the calcaneus, particularly the posterior facet. When this heals in a pathologic position, it sets off a cascade of problems:
- Posttraumatic Subtalar Arthritis: The primary fracture line often involves the posterior facet, leading to incongruity and degenerative changes within the subtalar joint. This is a major source of pain and stiffness.
- Fibulocalcaneal Impingement: The lateral wall of the calcaneus often "blows out" with the initial fracture, widening the heel. When this malunites, it impinges directly against the distal fibula, causing pain and displacing the peroneal tendons.
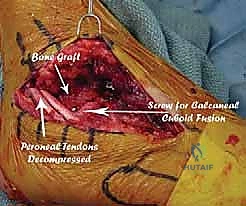
- Peroneal Tendinopathy/Tear: The displaced peroneal tendons (longus and brevis) are forced into an abnormal, often compressed, course over the expanded lateral wall. This can lead to chronic irritation, tendinosis, and eventually, rupture.
- Talotibial Impingement: The loss of calcaneal height, specifically the reduction of the talar inclination angle, can lead to the talus impinging against the anterior tibia during dorsiflexion, limiting ankle range of motion and causing pain.
- Sural Nerve Entrapment: The lateral soft tissue scarring and bony expansion can entrap the sural nerve, leading to chronic neuropathic pain, hypoesthesia, or dysesthesia in its distribution.
- Calcaneocuboid Arthritis: In some cases, the malalignment can also lead to secondary arthritic changes at the calcaneocuboid joint, which may require concomitant arthrodesis.
- Talonavicular Joint Stress: The stiff, malpositioned hindfoot places increased stress on the transverse tarsal articulation, potentially causing secondary arthritis at the talonavicular joint.
Remember, the calcaneus is exposed to axial loading, with stress occurring obliquely across the tuberosity as it sits lateral to the axis of the tibia. This anatomical orientation makes it particularly vulnerable to the types of fractures we see.
Figure 2A: Diagram illustrating the primary oblique fracture line, lateral and proximal displacement of the tuberosity, impaction of the posterolateral facet, and expansion of the lateral wall, which are hallmarks of calcaneal fractures.

Figure 2B: An acute CT scan demonstrating the fracture and displacement, highlighting the immediate post-injury anatomy.
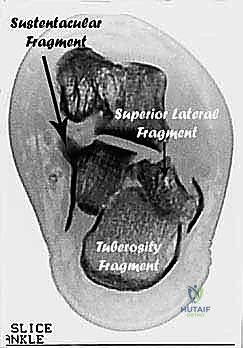
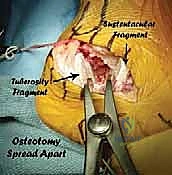
The typical fracture patterns involve four major fragments: the tuberosity, the posterolateral facet, the sustentaculum tali, and the anterolateral fragment. Crucially, the sustentacular fragment often retains its anatomic position, serving as a relatively stable landmark.
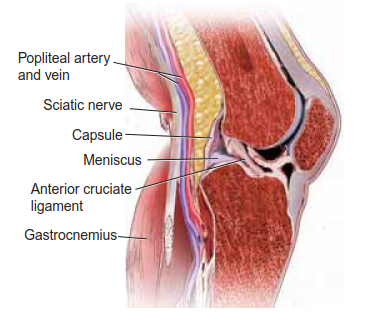
Comprehensive Surgical Anatomy
Before we make any incision, let's review the critical anatomy we'll encounter and protect.
-
Osteology:
- Calcaneus: The largest tarsal bone. We'll be primarily concerned with the tuberosity (posterior weight-bearing portion), the posterior facet (articulates with the talus), the sustentaculum tali (medial shelf supporting the talar head), and the lateral wall. The angle of Gissane, a critical angle formed by the posterior facet and the anterior process, is often disrupted. Bohler's angle, formed by the intersection of two lines on a lateral radiograph, is typically diminished or even reversed in malunions, indicating loss of heel height.
- Talus: Sits atop the calcaneus, forming the subtalar joint. Its inclination angle is key to normal ankle mechanics.
- Fibula: Its distal tip forms the lateral malleolus. The fibulocalcaneal impingement occurs between the lateral wall of the calcaneus and the fibula.
- Cuboid: Articulates with the anterior calcaneus, forming the calcaneocuboid joint. This joint can also be affected by the malunion.
-
Neurovascular Structures:
- Sural Nerve: This is our primary nerve of concern laterally. It typically runs posterior to the lateral malleolus, then courses anteriorly along the lateral aspect of the foot. With lateral wall blowout, it's highly susceptible to entrapment and injury during our approach and dissection. It provides sensation to the lateral foot and fifth toe.
- Peroneal Tendons (Peroneus Longus and Brevis): These tendons run in a groove posterior to the lateral malleolus. In a calcaneal malunion, the expanded lateral wall often displaces them anteriorly and superiorly, leading to impingement and tendinopathy. We must identify, protect, and retract them throughout the procedure.
- Posterior Tibial Neurovascular Bundle: This bundle (posterior tibial artery, tibial nerve, and posterior tibial vein) runs medially, posterior to the medial malleolus. Our osteotomy will exit the medial wall of the calcaneus posterior and inferior to this bundle. Extreme caution is paramount to avoid injury.
-
Muscular Intervals & Ligaments:
- Peroneal Retinaculum: This fibrous band holds the peroneal tendons in place. It will need to be incised or released to mobilize the tendons for retraction.
- Fibulocalcaneal Ligament: Part of the lateral collateral ligament complex, it often becomes scarred and tethered in the setting of impingement. We will incise this laterally to mobilize the subtalar joint.
- Interosseous Ligaments (Cervical and Interosseous Talocalcaneal Ligaments): These strong ligaments within the sinus tarsi connect the talus and calcaneus. The raw text states, "Do not incise the interosseous ligaments if possible, as these will help stabilize the sustentacular fragment to the talus." This is a critical pearl. Preserving them helps maintain the connection between the sustentacular fragment and the talus, which is often in an anatomically more correct position. This stability is invaluable.
- Flexor Hallucis Longus (FHL) Tendon: This tendon runs medially, deep to the neurovascular bundle, and can be observed through the joint after clearing posterior calcaneal tissue. We need to be aware of its course.
- Triceps Surae (Gastrocnemius-Soleus Complex): A contracture here can limit ankle dorsiflexion, which might require an Achilles tendon lengthening.
Preoperative Planning: The Blueprint for Success
Thorough preoperative planning is non-negotiable for these complex cases. This is where we create our surgical blueprint.
Patient History and Physical Findings
- History: Expect a history of a calcaneal fracture, though not all patients may be aware of it if initially treated non-operatively or if the diagnosis was missed. Symptoms typically include increasing pain with activity, particularly at the fibulocalcaneal junction and sinus tarsi. Hypoesthesia or dysesthesia in the sural nerve distribution is common.
- Physical Exam:
- Loss of "Fibular Sulcus": Palpate just distal to the tip of the fibula on both ankles. In a malunion, the normal indentation for the peroneal tendons will be absent due to lateral displacement of the tuberosity and lateral wall blowout. This is a key diagnostic sign.
- Hindfoot Stiffness: Assess subtalar inversion and eversion. Expect little to no motion, often painful, indicative of subtalar arthritis and scarring.
- Ankle Dorsiflexion: Look for loss of ankle dorsiflexion, which suggests talotibial impingement and increased stress on the transverse tarsal articulation.
- Sural Nerve: Check for hypoesthesia in its distribution and a positive Tinel's sign with percussion along its course.
Imaging and Diagnostic Studies
Quality imaging is paramount. This is our roadmap.
- Plain Radiographs:
- Weight-bearing AP, Lateral, Axial Heel, and Broden Views: These are essential.
- Weight-bearing Lateral of Unaffected Foot: Crucial for establishing normal parameters for the patient and templating the desired correction.
- AP View: Will show the calcaneocuboid joint, assessing for involvement.
- Lateral View: Demonstrates loss of heel height, loss of talar inclination, and anterior tibial-talar impingement. We'll see a diminished or reversed angle of Bohler.
- Axial Heel View: Reveals the oblique primary fracture line and the characteristic lateral and proximal shift of the tuberosity.
- Broden Views: Specifically designed to visualize the subtalar joint and demonstrate fibulocalcaneal impingement.
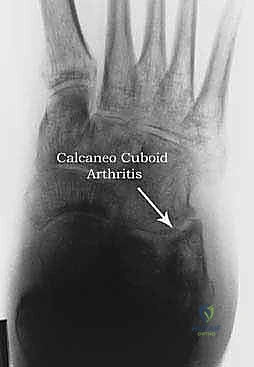
Figure 4A: AP radiograph of a foot with calcaneal malunion affecting the calcaneocuboid joint, showing potential arthritic changes.
*
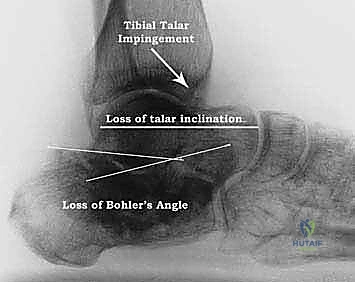
Figure 4B: Lateral view of a calcaneal malunion, clearly demonstrating the loss of Bohler's angle, diminished talar inclination, and anterior tibial-talar impingement.
*
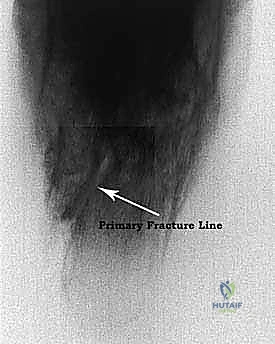
Figure 4C: Broden view of a calcaneal malunion, highlighting tuberosity translation, lateral impingement, and subtalar arthritis.
*
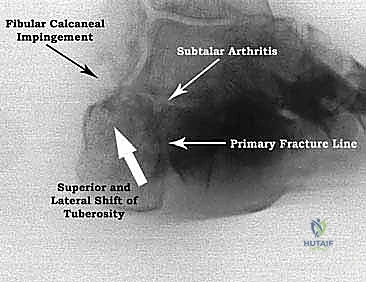
Figure 4D: Axial heel view of a calcaneal malunion, showing the oblique primary fracture line, displacement of the tuberosity, and lateral impingement.
- CT Scan (Axial, Semicoronal, Sagittal, and 3D Volumetric Reconstructions): This is the gold standard. It confirms all findings from plain films, provides a detailed "blueprint" of the internal architecture, clarifies the deformity, impingements, and extent of arthritis. It helps us differentiate between joint depression and tongue-type fractures; joint depression fractures are generally better suited for correction by this procedure.

Figure 3B: CT scan of a calcaneal malunion, revealing post-traumatic subtalar arthritis, the characteristic lateral and proximal displacement of the tuberosity, and fibulocalcaneal impingement.
*

Figure 3C: Three-dimensional volumetric reconstruction of a calcaneal malunion, providing a comprehensive view of the complex deformity.
*

Figure 3D: Lateral radiograph showing significant malunion, a reversed Bohler's angle, and tibial-calcaneal impingement.
*

Figure 3E: Diagram depicting peroneal tendon compression due to the expanded lateral wall.
*
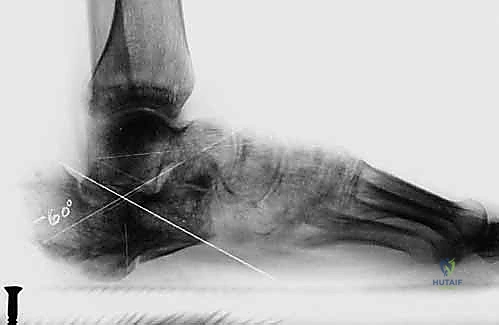
Figure 3F: Diagram illustrating tibial-talar impingement resulting from the loss of calcaneal height.
*
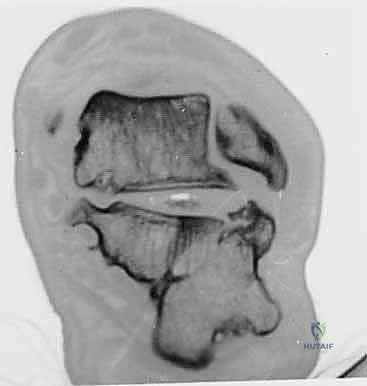
Figure 3G: CT scan demonstrating the displacement of the peroneal tendons in a calcaneal malunion.
Nonoperative Management (When to Consider)
While we're here for surgery, it's important to acknowledge nonoperative options for milder symptoms or non-surgical candidates:
* NSAIDs for pain and inflammation.
* Judicious steroid injections into the sinus tarsi.
* Bracing, heel cups, or heel lifts for support and cushioning.
However, for significant deformities causing impingement, severe arthritis, and functional limitations, surgical correction is typically indicated.
Surgical Management Indications & Contraindications
Indications:
* Symptomatic malunited calcaneal fractures exhibiting:
* Fibulocalcaneoperoneal impingement.
* Posttraumatic subtalar arthritis.
* Loss of Bohler's angle and talar inclination.
* Widening of the heel.
* Sural nerve entrapment.
* Tibial-talar impingement.
* Painful calcaneocuboid arthritis (may require concomitant fusion).
Contraindications:
* Severe medical comorbidities (e.g., uncontrolled diabetes, severe peripheral vascular disease, active infection).
* Smoking: A significant risk factor for nonunion and wound complications. Aggressive smoking cessation counseling is essential.
* Poor soft tissue envelope.
* Unrealistic patient expectations.
Correction-Limiting Factors:
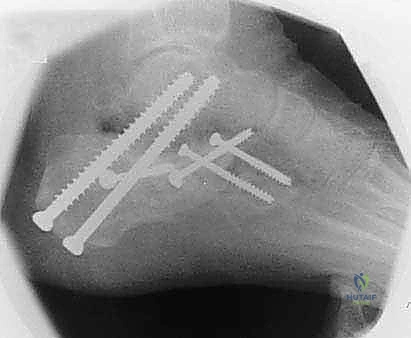
* The amount of bone available for transverse fixation. We aim to move fixation anteriorly as less translation occurs in this portion of the calcaneus, providing better windows for screw placement.
* Height losses up to 1.5 cm can typically be corrected. Greater loss may necessitate an interpositional bone block.
Essential Instruments
Let's ensure we have everything ready:
* 7.0-mm cannulated screws: We favor fully threaded screws for robust fixation.
* Anterior cruciate ligament (ACL) drill guide: This is invaluable for precise guidewire placement for the 7.0-mm screws.
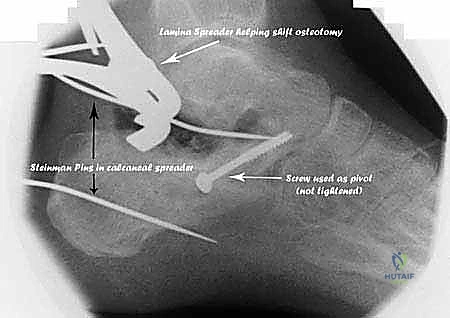
* Baby Inge lamina spreaders: Both with and without serrations for careful distraction.
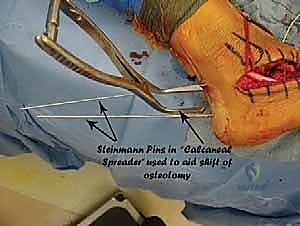
* "Calcaneal spreaders": Wide, flat-faced, and Steinmann pin fixation spreaders. These are specialized tools for fragment manipulation.
* Smaller cannulated screws: 3.5-, 4.0-, or 4.5-mm for transverse fixation.
* Power osteotome: Very helpful for precise bone cuts.
* Saw: For starting the osteotomy.
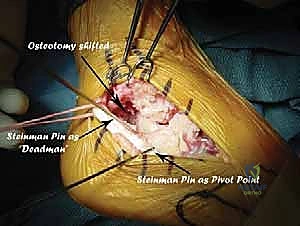
* Smooth Steinmann pins: For temporary fixation and pivot points.
* Bone graft harvest instruments: If autograft is planned from the iliac crest.
Patient Positioning and Preparation
"Alright team, let's get our patient positioned."
- Positioning: We'll place the patient in the lateral decubitus position, with the affected limb up. This allows excellent access to the lateral aspect of the hindfoot. Ensure adequate padding at pressure points.
- Tourniquet: A pneumatic tourniquet is applied to the thigh of the affected limb. We'll inflate this after exsanguination to maintain a bloodless field, which is critical for identifying subtle anatomical structures and achieving precise cuts.
- Prep and Drape: The entire leg, from the tourniquet down to the toes, is meticulously prepared and draped in a sterile fashion. Crucially, if we anticipate needing autogenous bone graft, the ipsilateral iliac crest must also be prepared and draped into the sterile field. This allows for simultaneous harvest if needed.
- Fluoroscopy Setup: The C-arm should be positioned and draped to allow for immediate AP, lateral, axial heel, and Broden views of the calcaneus without repositioning the patient. We'll need to verify its range of motion and image quality before we start.
Intraoperative Execution: The Oblique Calcaneal Osteotomy with Subtalar Arthrodesis
"Alright fellows, let's begin. Scalpel, please."
1. Incision and Initial Exposure
"We're making a straight incision here, starting just below the tip of the fibula. Follow the line anteriorly, extending in the direction of the fourth and fifth ray, past the calcaneocuboid joint. We might need to extend it slightly posteriorly if more exposure is required."
- Incision: A straight lateral incision is preferred. This provides excellent exposure while minimizing soft tissue stripping.

Figure 6: The planned skin incision, extending from just below the fibular tip anteriorly along the line of the 4th-5th metatarsal ray.
"As we deepen the incision, be mindful of the sural nerve. It's often superficial and can be tethered by scar tissue in these malunions. Identify it, gently dissect it free, and protect it with vessel loops or a Penrose drain. The area around the fibular tip is often congested and scarred due to the chronic impingement. You'll likely see the peroneal tendons displaced anteriorly and superiorly from their normal sulcus."
- Sural Nerve Protection: Isolate the sural nerve. This nerve typically runs superficially along the lateral aspect of the foot. In malunion cases, it can be encased in scar tissue or stretched. Use careful blunt dissection to free it and retract it superiorly or inferiorly, away from the surgical field.
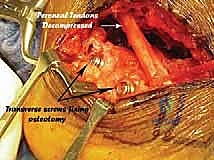
- Peroneal Tendons: Identify the peroneus longus and brevis tendons. They will almost certainly be displaced. Incise the peroneal retinaculum to allow for their full mobilization. Use a broad Hohmann retractor or a small malleable retractor to gently retract them superiorly and anteriorly, exposing the underlying lateral wall of the calcaneus and the sinus tarsi.
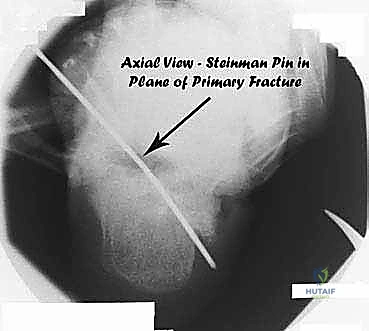
Figure 1A: Peroneal tendons retracted, exposing the sinus tarsi and lateral calcaneus.

Figure 1B: Close-up view of the peroneal tendons retracted, providing clear access to the underlying bone.
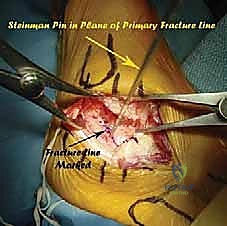
2. Subtalar Joint Mobilization and Preparation
"Now, let's focus on the subtalar joint. We need to enter it and mobilize it thoroughly. Use a baby Inge lamina spreader to gently distract the joint in the sinus tarsi. This will help us visualize the joint surfaces and release the surrounding scar tissue."
- Sinus Tarsi Dissection: Carefully dissect through the sinus tarsi, releasing scar tissue and hypertrophic synovium.
- Capsular Incision: Incise the scarred capsule and the fibulocalcaneal ligament laterally. This is crucial for gaining mobility and releasing the impingement.
*
Additional Intraoperative Imaging & Surgical Steps







REFERENCES
-
Bradley SA, Davies AM. Computerized tomographic assessment of old calcaneal fractures. Br J Radiol 1990;63:926–933.
-
Burdeaux BD. Reduction of calcaneal fractures by the McReynolds medial approach technique and its experimental basis. Clin Orthop Relat Res 1983;177:87–103.
-
Carr JB, Hansen ST, Benirshke SK. Subtalar distraction bone block fusion for late complications of the os calcis fractures. Foot Ankle 1988;9:81–86.
-
Conn HR. The treatment of fractures of the os calcis. J Bone Joint Surg 1935;17:392.
-
Gallie WE. Substragalar arthrodesis in fractures of the os calcis. J Bone Joint Surg 1943;25:731–736.
-
Hansen ST Jr. Calcaneal osteotomy in multiple planes for correction of major posttraumatic deformity. In: Functional Reconstruction of the Foot and Ankle, pp. 380–383. Philadelphia: Lippincott Williams & Wilkins, 2000.
-
Leung K, Chan W, Shen W, et al. Operative treatment of intra articular fractures of the os calcis—the role of rigid internal fixation and primary bone grafting: preliminary results. J Trauma 1989;3:232–240.
-
Palmer I. The mechanism and treatment of fracture of the calcaneus: open reduction with the use of cancellous bone grafts. J Bone Joint Surg Am 1948;30A:2–8.
-
Romash MM. Reconstructive osteotomy of the calcaneus with subtalar arthrodesis for malunited calcaneal fractures. Master Techniques in Orthopedic Surgery series: The Foot and Ankle, 1st and 2nd eds. Philadelphia: Lippincott Williams & Wilkins.
-
Romash MM. Reconstructive osteotomy of the calcaneus with subtalar arthrodesis for malunited calcaneal fractures. Clin Orthop Relat Res 1993;228:157–167.
-
Physical therapy is prescribed to gain ankle range of motion and calf strengthening.
OUTCOMES
- The first cases were reported in
- We have continued to perform this procedure over the intervening years; about 45 procedures have been performed. The results have been reproducible. A 1.5-cm correction and increase of the Bohler angle of 25 degrees can be expected. There have been no osteotomy nonunions and one nonunion of the subtalar fusion in a smoker. There have been two patients treated by osteotomy alone (no subtalar arthrodesis) with satisfactory results.
COMPLICATIONS
- Nonunions of the osteotomy or arthrodesis sites are possible but have not proven to be a problem. Malposition of the arthrodesis is possible, but attention to inversion–eversion before fixation of the calcaneal construct to the talus avoids this potential complication.
- Inadequate correction can be avoided by proper selection of patients. The magnitude of the deformity should be within the limits of correction described above. The surgeon should have patience and be persistent in gaining correction, especially in the initial procedures undertaken. The correction is
You Might Also Like