Arthrodesis of the Wrist: Surgical Techniques & Protocols
Key Takeaway
Wrist arthrodesis is a highly effective salvage procedure for advanced radiocarpal arthritis, severe trauma, and paralytic deformities. Achieving a stable, painless wrist requires meticulous surgical technique, optimal positioning in 10 to 20 degrees of extension, and rigid internal fixation. This guide details evidence-based approaches, including AO/ASIF plating and specialized tenodesis techniques, ensuring high fusion rates and maximal postoperative grip strength for complex wrist pathologies.
ARTHRODESIS OF THE WRIST: COMPREHENSIVE PRINCIPLES AND TECHNIQUES
Wrist arthrodesis (total radiocarpal fusion) remains a highly reliable and durable salvage procedure designed to provide a stable, painless wrist while maximizing the functional grip strength of the hand. Although motion-preserving alternatives such as proximal row carpectomy or partial carpal fusions have gained popularity, total wrist arthrodesis remains the gold standard for end-stage pan-carpal arthritis, severe structural collapse, and complex neuromuscular deformities.
This comprehensive guide delineates the indications, biomechanical principles, surgical approaches, and postoperative protocols required to achieve optimal outcomes in wrist arthrodesis, integrating both historical foundations and modern AO/ASIF rigid fixation techniques.
Indications and Patient Selection
The decision to proceed with a total wrist arthrodesis is predicated on the presence of debilitating pain, profound instability, or severe deformity that cannot be addressed through joint-sparing procedures. The primary indications include:
- Post-Traumatic Osteoarthritis: Most frequently arising from ununited or malunited fractures of the carpal scaphoid (Scaphoid Nonunion Advanced Collapse - SNAC) with associated radiocarpal traumatic arthritis.
- Severe Distal Radius Trauma: Highly comminuted fractures of the distal radius with irreparable intra-articular destruction.
- Inflammatory Arthropathies: Advanced rheumatoid arthritis (RA) presenting with pan-carpal destruction, ulnar translation of the carpus, and profound instability.
- Neuromuscular Disorders:
- Positioning and stabilizing the wrist following Volkmann ischemic paralysis.
- Stabilization in spastic cerebral palsy to improve hygiene and hand positioning.
- Poliomyelitis resulting in flail wrist.
- Infectious Sequelae: Joint destruction secondary to tuberculosis or other pyogenic infections (performed after the eradication of active infection).
Clinical Pearl: In patients with rheumatoid arthritis exhibiting ulnar translation of the carpus, a limited radiolunate fusion has been found to be an effective method to prevent further translation if the midcarpal joint remains preserved. However, if pan-carpal disease is present, a total wrist arthrodesis is mandatory.
Biomechanics and Optimal Positioning
The functional success of a wrist arthrodesis relies entirely on the position in which the joint is fused. The wrist must be immobilized in a posture that prevents fatigue while optimizing the length-tension relationship of the extrinsic finger flexors, thereby allowing maximal grasping strength.
- Sagittal Alignment: The optimal position is typically 10 to 20 degrees of extension.
- Coronal Alignment: The long axis of the third metacarpal shaft must be perfectly aligned with the long axis of the radial shaft.
- Clinical Determination: Intraoperatively and preoperatively, this optimal functional angle is determined by observing the position that the wrist normally assumes when the patient makes a strongly clenched fist.
Fusing the wrist in excessive extension (greater than 30 degrees) can lead to extensor tendon irritation and fatigue, while fusion in flexion severely compromises grip strength due to active insufficiency of the finger flexors.
Surgical Approaches and Techniques
Historically, pseudarthrosis rates for wrist fusions were unacceptably high, generally ranging from 8% to 29% when relying on cast immobilization or non-rigid fixation (e.g., Steinmann pins). The advent of rigid internal fixation, specifically the addition of a dorsal plate and screws as popularized by the AO/ASIF technique (Heim and Pfeiffer), revolutionized the procedure, yielding fusion rates from 93% to 100%.
1. The Dorsal Approach with AO/ASIF Plating
The dorsal approach utilizing a specialized wrist fusion plate is currently the most widely utilized technique. Modification of the standard straight plate, such as the pre-contoured plate described by Weiss and Hastings, accommodates the natural 10 to 20 degrees of extension and minimizes the need for subsequent plate removal due to tendon irritation.
Key Surgical Steps:
1. Incision and Exposure: A longitudinal dorsal incision is made centered over Lister's tubercle, extending from the distal radius to the mid-shaft of the third metacarpal.
2. Retinacular Flap: The extensor retinaculum is divided, typically stepping cut to allow for later repair over the plate. The extensor pollicis longus (EPL) is mobilized and retracted radially.
3. Joint Preparation: Lister's tubercle is excised to create a flat bed for the plate. The articular cartilage and subchondral bone of the radiocarpal, midcarpal, and third carpometacarpal (CMC) joints are meticulously decorticated down to bleeding cancellous bone.
4. Bone Grafting: Autogenous cancellous bone graft (often harvested from the excised Lister's tubercle, distal radius, or iliac crest) is packed into the decorticated joint spaces.
5. Plate Application: The pre-contoured fusion plate is applied. It is critical to secure the plate to the radius proximally, the capitate centrally, and the third metacarpal distally.
Surgical Warning: Haddad and Riordan recommended that the second and third carpometacarpal joints always be included in the fusion mass. Failure to include these joints can lead to the development of painful micromotion, especially since disease processes frequently extend into these articulations.
2. The Radial/Lateral Approach (Haddad and Riordan)
Haddad and Riordan described an alternative technique for arthrodesis of the wrist through a radial or lateral approach.
Advantages of the Radial Approach:
* The distal radioulnar joint (DRUJ) is not entered, preserving its mechanics if unaffected by disease.
* The extensor tendons to the digits are not disturbed, drastically reducing the risk of postoperative extensor tenosynovitis or rupture.
* Because dorsal hardware and bone graft thickening are avoided, the cosmetic appearance of the dorsal wrist is not altered.
* Outcomes: These authors reported exceptional success, noting only one failure in 24 wrists using this technique.
3. Limited and Partial Fusions
In highly selected patients, a complete pan-carpal arthrodesis may be avoided to preserve a small degree of functional "wrist" motion.
* Radioscapholunate (RSL) Fusion: In patients with post-traumatic arthritis strictly limited to the radiocarpal joint (without midcarpal involvement), proximal row fusion (RSL) was reported by Bach et al. to be highly successful in relieving pain in 29 of 31 patients.
* Smith-Petersen Technique: Described primarily for severe rheumatoid arthritis, this method utilizes the excised distal end of the ulna as a bone graft inserted between the radius and the carpus. Caveat: This technique should not be used unless there is pre-existing disease or derangement of the DRUJ necessitating ulnar head resection. It also has the distinct disadvantage of allowing only limited access to the radiocarpal joint for decortication.
Distal Ulnar Stabilization: FCU and ECU Tenodesis
In cases where wrist arthrodesis is combined with a distal ulnar resection (e.g., Darrach procedure) due to DRUJ destruction, stabilizing the remaining ulnar stump is critical to prevent painful dorsal subluxation. A highly effective combination tenodesis utilizing slips of the flexor carpi ulnaris (FCU) and extensor carpi ulnaris (ECU) can be employed.
Step-by-Step Tenodesis Technique:
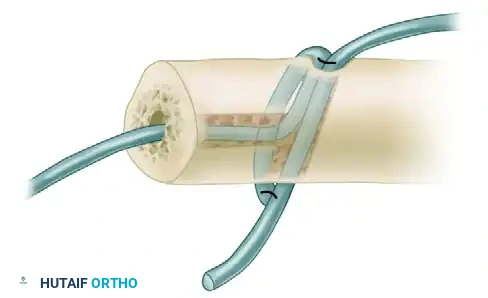
- Bone Tunnel Preparation: Prepare the distal cut end of the ulna. Drill a medullary canal tunnel from the distal, cut end of the ulna to connect with a first, transverse dorsal tunnel. Create a second dorsopalmar transverse tunnel through the distal ulnar shaft.
- FCU Slip Passage: Use a suture passer or a 20-gauge wire loop to pass a distally based slip of the flexor carpi ulnaris into the medullary canal tunnel, entering from the distal cut end of the ulna and exiting out through the dorsal tunnel.
FIGURE A: The FCU slip is passed through the medullary canal and out the dorsal tunnel of the distal ulna.
- ECU Slip Passage: In a similar way, pass a distally based slip of the extensor carpi ulnaris through the dorsopalmar tunnel. The slip should enter dorsally and pass out through the palmar side of the ulna.
- Tensioning and Suturing: Supinate the forearm completely. Pull both of the tendon slips taut to ensure rigid stabilization of the ulnar stump. Suture the FCU and ECU slips to each other securely using a heavy nonabsorbable suture.
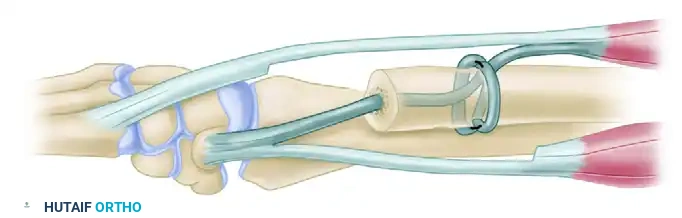
FIGURE B: Completion of the weave. The ECU and FCU tendons are pulled taut with the forearm in supination and sutured to each other, creating a robust dynamic stabilization of the distal ulna.
- Dorsal Stabilization: Further stabilize the extensor carpi ulnaris dorsally by securing it with a loop created from the extensor retinaculum.
- Closure: Close the incisions in layers.
Pediatric Considerations in Wrist Arthrodesis
Performing a wrist arthrodesis in the pediatric population presents unique anatomical challenges and requires strict adherence to physiological principles regarding skeletal maturity.
- Physeal Preservation: Because the distal radial physis does not close until approximately 17 years of age, extreme care must be taken not to damage it in patients younger than 17. Iatrogenic injury to the physis during joint decortication or hardware placement will result in severe growth arrest and secondary deformity.
- Management of Prior Physeal Damage: If the distal radial physis has already undergone partial destruction due to disease (e.g., infection) or trauma, the remaining healthy portion of the physis should be intentionally excised (epiphysiodesis) at the time of fusion to prevent unequal, tethered growth.
- Timing of Surgery: Fusion of the wrist in young children is notoriously difficult to secure due to the massive amount of unossified cartilage present in the carpal joints. If clinically possible, the operation should be postponed until the patient is at least 10 to 12 years old, allowing for sufficient ossification to support rigid fixation and bone grafting.
Postoperative Care and Rehabilitation
Meticulous postoperative care is essential to ensure high fusion rates and to restore functional utility to the upper extremity.
- Immediate Postoperative Phase: Following closure, apply a well-padded long-arm cast or rigid splint. The elbow must be flexed to 90 degrees, and the forearm should be positioned in full supination (particularly if a distal ulnar tenodesis was performed).
- First Clinic Visit (10 to 14 Days): If removable sutures or staples have been used, they are removed at 10 to 14 days. The surgical site is inspected for signs of infection or wound breakdown. The long-arm cast or splint is then changed.
- Immobilization Period: Strict immobilization is continued for a minimum of 6 weeks after the operation. Radiographs are obtained at the 6-week mark to assess the progression of trabecular bridging across the arthrodesis sites.
- Rehabilitation: Once clinical and radiographic signs of early fusion are confirmed, a program of therapist-supervised rehabilitation is begun. The patient advances systematically through a program of range-of-motion exercises for the digits, elbow, and shoulder, followed by progressive strengthening exercises.
- Return to Activity: Unrestricted activity, including heavy manual labor or weight-bearing, is typically permitted only after solid radiographic union is achieved, which may take 12 to 16 weeks depending on patient biology and the specific surgical technique employed.
Conclusion
Arthrodesis of the wrist is a highly reliable procedure that transforms a painful, unstable, or paralyzed hand into a functional, pain-free unit capable of strong grasp. By adhering to strict biomechanical principles—specifically fusing the wrist in 10 to 20 degrees of extension—and utilizing modern rigid AO/ASIF plating techniques, surgeons can consistently achieve fusion rates approaching 100%. Careful management of the distal radioulnar joint, appropriate handling of pediatric physes, and structured postoperative rehabilitation are paramount to maximizing long-term clinical success.
You Might Also Like

