Forearm Malunion: Advanced Osteotomy and Plating Techniques
Key Takeaway
Forearm malunion significantly impairs pronosupination and grip strength. Corrective osteotomy and plating aim to restore the complex biomechanical relationship between the radius and ulna. This procedure requires meticulous preoperative planning, including bilateral radiographic and CT evaluation, to quantify angular and rotational deformities. Surgical execution involves precise uniplanar or multiplanar osteotomies, restoration of the radial bow, and rigid internal fixation using 3.5-mm dynamic compression plates, often supplemented with autogenous bone grafting.
Introduction to Forearm Malunion
The forearm functions as a highly complex, articulated ring, mechanically analogous to the pelvic ring but designed for intricate, multi-axial mobility rather than pure weight-bearing. The radius and ulna articulate at the proximal radioulnar joint (PRUJ) and the distal radioulnar joint (DRUJ), bound together by the interosseous membrane. A fracture of the diaphyseal shafts of the radius and ulna that heals in a malaligned position—a malunion—disrupts this delicate kinematic chain.
Even minor degrees of angular, rotational, or length discrepancy can lead to a profound loss of pronation and supination, altered load transmission across the radiocapitellar and ulnocarpal joints, and subsequent early-onset post-traumatic osteoarthritis. Corrective osteotomy and plating for forearm malunion, utilizing the modified principles of Trousdale and Linscheid, is a technically demanding procedure. It requires a profound understanding of forearm biomechanics, meticulous preoperative templating, and precise surgical execution to restore the anatomical radial bow and the precise length relationship between the radius and ulna.
Pathoanatomy and Biomechanics of Deformity
Understanding the deforming forces that lead to malunion is critical for planning the corrective osteotomy. The forearm musculature exerts predictable vectors of pull on fracture fragments, which dictate the typical patterns of rotational and angular malunion.
- Proximal Fragment Kinematics: The proximal radial fragment is typically driven into strong supination by the unopposed pull of the biceps brachii (inserting on the radial tuberososity) and the supinator muscle.
- Distal Fragment Kinematics: The distal fragment is conversely drawn into pronation by the pronator teres (inserting on the mid-lateral radius) and the pronator quadratus (inserting on the distal volar radius).
- The Radial Bow: The radius possesses a natural lateral convexity (the radial bow) that is essential for allowing the radius to rotate around the fixed ulna during pronosupination. Loss of the magnitude or location of the maximum radial bow directly correlates with a mechanical block to rotation.
Clinical Pearl: A loss of normal radial bow magnitude of more than 5% or a shift in the location of the maximum bow will result in a clinically significant loss of forearm rotation. Restoring this bow is the primary biomechanical objective of radial osteotomy.
Preoperative Evaluation and Planning
Clinical Assessment
A rigorous clinical examination forms the foundation of surgical decision-making.
* Range of Motion (ROM): Accurately record the exact degrees of forearm pronation and supination, as well as elbow flexion and extension. Compare these metrics to the contralateral, uninjured extremity.
* Joint Stability: Evaluate the stability of both the DRUJ and the PRUJ. Apply manual stress palmarly and dorsally to the distal ulna to assess for DRUJ subluxation or instability, which often accompanies significant radial shortening or angular deformity.
* Neurologic Assessment: Document the preoperative status of the posterior interosseous nerve (PIN), anterior interosseous nerve (AIN), and superficial sensory nerves, as these may be tethered by scar tissue or at risk during surgical exposure.
Radiographic and Advanced Imaging Protocol
Standard orthogonal imaging is insufficient for complex multiplanar deformities. A comprehensive imaging protocol is mandatory.
- Standard Radiographs: Obtain full-length anteroposterior (AP), lateral, and specific pronation and supination radiographs of the involved forearm. Crucially, obtain identical views of the contralateral normal forearm to serve as an anatomical template.
- Deformity Analysis: Assess the relative lengths of the radius and ulna (ulnar variance). Identify the exact site, apex, and magnitude of the angular deformity in both the coronal and sagittal planes.
- Computed Tomography (CT): CT scanning is the gold standard for evaluating rotational deformities, which are notoriously difficult to quantify on plain radiographs. Scans should be performed with both forearms in maximal pronation and supination. Cross-sectional axial cuts proximal and distal to the malunion site are compared with the uninjured side to calculate the exact degree of rotational malalignment.
Surgical Decision Making: The Trousdale and Linscheid Algorithm
The decision of whether to osteotomize one or both bones depends entirely on the location and severity of the deformity. The modified Trousdale and Linscheid algorithm provides a systematic approach to this complex problem.
- Isolated Malunion: Determine whether one or both bones are significantly malaligned. If only one bone is malunited (e.g., an isolated radial shaft fracture that healed in angulation), osteotomy of only the involved bone is performed.
- Combined Malunion (Unequal Severity): If both bones are malaligned, the fundamental rule is to perform the osteotomy, realignment, and stabilization on the more severely deformed bone first.
- If the radius is the primary site of severe malalignment, correct the radius first. If rigid provisional fixation of the radius restores smooth, full forearm rotation during passive intraoperative manipulation, the ulna may not require an osteotomy.
- Combined Malunion (Equal Severity): If both bones are equally malaligned, it is biomechanically preferable to osteotomize and correct the ulna first. The ulna acts as the straight, stable axis of the forearm. Establishing proper ulnar alignment provides a fixed reference point, allowing the surgeon to then osteotomize the radius and contour it to conform perfectly to the newly established ulnar axis.
- Simultaneous Correction: In severe, chronic cases with significant soft tissue contracture, osteotomy of both bones may be required simultaneously before either can be properly realigned and provisionally fixed.
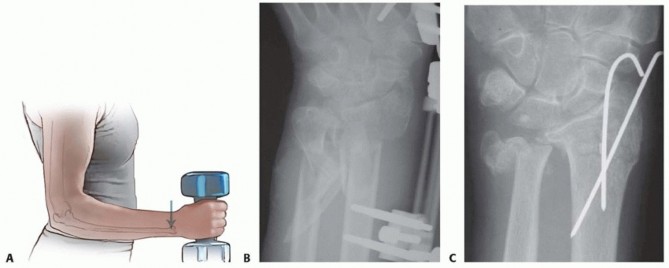
Patient Positioning and Preparation
- Positioning: The patient is placed supine on the operating table with the affected arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied high on the brachium.
- Fluoroscopy: The C-arm fluoroscope should be positioned to allow unimpeded AP and lateral imaging of the entire forearm, elbow, and wrist without compromising the sterile field.
Surgical Approaches
Meticulous surgical exposure is required to access the malunion sites while preserving the vital neurovascular structures and minimizing the risk of postoperative radioulnar synostosis.
The Anterior Volar (Henry) Approach to the Radius
- Expose the radius through a 10- to 15-cm longitudinal anterior Henry approach, centered precisely over the apex of the malunion site.
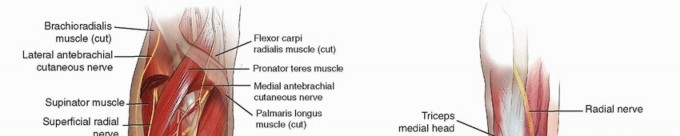
- Develop the internervous plane between the brachioradialis (radial nerve) and the flexor carpi radialis (median nerve).
- Ligate the radial recurrent vessels to mobilize the mobile wad laterally.
- For proximal exposures, carefully identify and protect the PIN as it traverses the supinator muscle. Supinate the forearm to move the PIN laterally and away from the surgical field before elevating the supinator from the radius.
The Subcutaneous Approach to the Ulna
- If ulnar osteotomy is required, expose the ulna through a separate 10- to 15-cm longitudinal subcutaneous approach.
- Utilize the internervous plane between the extensor carpi ulnaris (PIN) and the flexor carpi ulnaris (ulnar nerve).
- Incise the periosteum directly over the subcutaneous border of the ulna.
Surgical Warning: Minimize all dissection within the interosseous space between the radius and ulna. Violation of the interosseous membrane, especially in the presence of bone dust from the osteotomy, drastically increases the risk of heterotopic ossification and devastating radioulnar synostosis.
Step-by-Step Surgical Technique (Modified Trousdale & Linscheid)
1. Defining the Osteotomy Plane
Determine the type of osteotomy required to restore alignment in all three planes (coronal, sagittal, and axial/rotational).
* Uniplanar Deformity: If the deformity exists purely in one plane, a simple transverse or oblique uniplanar osteotomy at the apex of the deformity is sufficient.
* Multiplanar Deformity: If preoperative CT and radiographs reveal a complex deformity involving angulation, rotation, and shortening, a multiplanar osteotomy (often requiring a closing wedge, opening wedge, or step-cut technique) is necessary.
2. Executing the Osteotomy
- Make the osteotomy exactly according to the preoperative template at the apex of the deformity.
- Technique A (Oscillating Saw): Divide the bone using a small, motorized oscillating saw under continuous saline irrigation to prevent thermal necrosis of the bone ends.
- Technique B (Drill and Osteotome): Alternatively, outline the planned plane of the osteotomy with multiple contiguous drill holes using a 2.0-mm drill bit. Complete the division with a sharp osteotome. This technique minimizes bone loss and thermal injury.
- Medullary Canal Restoration: The medullary canal is often obliterated by sclerotic bone at the malunion site. Use a drill or a hand reamer to carefully reestablish the medullary canal in both the proximal and distal fragments. This is critical for restoring endosteal blood supply and facilitating potential intramedullary bone grafting, provided it can be accomplished without excessive soft tissue stripping.
3. Deformity Correction and Plate Contouring
- Following the osteotomy, manually correct the rotational and angular deformities.
- Select a heavy-duty 3.5-mm dynamic compression plate (DCP) or limited contact dynamic compression plate (LC-DCP).
- Restoring the Radial Bow: The plate must be meticulously contoured to match the normal anatomical bow of the radius. Use the preoperative template of the contralateral normal arm as a guide. An under-contoured or over-contoured plate will force the radius into a non-anatomical shape upon screw tightening, immediately restricting pronosupination.
4. Provisional Fixation and Kinematic Testing
- Clamp the contoured plate to each fragment using bone holding forceps.
- Clinical Assessment: Before drilling any screws, rigorously evaluate the passive range of motion. Assess flexion and extension of the elbow, and critically, the pronation and supination of the forearm. Ensure that the correction of the malunion has definitively improved passive kinematics and eliminated any mechanical blocks.
- Radiographic Assessment: Obtain intraoperative fluoroscopic views to confirm the restoration of the radial bow, ulnar variance, and DRUJ/PRUJ congruity. Make adjustments to the osteotomy or plate contour as necessary.
5. Definitive Fixation
- Once alignment is satisfactory and significant motion has been restored, proceed with definitive fixation.
- Provisionally fix the plate to the bone with one screw on each side of the osteotomy to maintain rotation and length.
- The Cortical Purchase Rule: Place the remaining screws through the plate. The biomechanical gold standard requires a plate long enough to provide a minimum of six cortices of fixation (three bicortical screws) both proximal and distal to the osteotomy site.
- Proximal Radius Exception: If the malunion is located in the proximal third of the radius, resulting in a short proximal fragment, it may be anatomically impossible to obtain more than four cortices of fixation without placing the posterior interosseous nerve (PIN) at severe risk of iatrogenic injury. In such cases, four cortices of robust fixation in the proximal fragment are acceptable, provided the patient is protected postoperatively.
6. Sequential Correction (If Applicable)
- If the ulna was osteotomized and realigned first (per the algorithm for equally severe deformities), but intraoperative testing reveals that the radius remains significantly deformed and restricts motion, proceed to correct the radial alignment using the exact same principles described above.
7. Management of Bone Gaps and Grafting
- After multiplanar realignment, perfect cortical apposition at the osteotomy site is not always possible, particularly if an opening wedge technique was utilized to restore length.
- Bone Grafting: It is imperative to place autogenous cancellous bone graft (typically harvested from the iliac crest or distal radius) into any residual bone gaps.
- Grafting is also strictly indicated in patients with any systemic or local risk factors for delayed union or nonunion (e.g., smoking, diabetes, previous infection, highly sclerotic bone ends).
Isolated Ulnar Shaft Malunion
An operation for malunion of the ulna alone is rarely necessary, as the ulna does not rotate around the radius; rather, it serves as the stable axis. However, significant ulnar angulation can tether the interosseous membrane or cause DRUJ subluxation. If surgical intervention is deemed necessary for an isolated ulnar malunion, the exact same biomechanical principles, preoperative planning steps, and fixation techniques described for the radial shaft must be meticulously followed.
Postoperative Protocol and Rehabilitation
The success of a forearm osteotomy relies as much on postoperative rehabilitation as it does on surgical execution.
- Immediate Postoperative Phase (0-2 Weeks): The arm is placed in a bulky Jones dressing with a well-molded posterior splint holding the forearm in neutral rotation and the elbow at 90 degrees of flexion. Elevation and strict digital range of motion are encouraged immediately to reduce edema.
- Early Motion Phase (2-6 Weeks): Once the incision has healed and sutures are removed, the splint is transitioned to a removable functional brace. If rigid internal fixation (minimum 6 cortices per segment) was achieved, gentle, active-assisted range of motion exercises for pronation and supination are initiated under the guidance of a specialized hand therapist. Passive stretching is strictly avoided to prevent hardware failure or loss of fixation.
- Strengthening Phase (6-12 Weeks): Radiographic union is typically assessed at 6 to 8 weeks. Once bridging callus is visible and the osteotomy site is non-tender, progressive resistance exercises and grip strengthening are incorporated. Full return to heavy manual labor or contact sports is generally restricted until complete radiographic consolidation is confirmed, often taking 4 to 6 months.
Complications and Avoidance
- Radioulnar Synostosis: The most devastating complication. Avoided by strictly respecting the interosseous membrane, utilizing separate surgical approaches, and thoroughly irrigating bone dust generated by the saw.
- Posterior Interosseous Nerve (PIN) Palsy: Prevented by careful identification during the proximal Henry approach, supinating the forearm during supinator elevation, and avoiding excessive proximal screw placement on the radius.
- Nonunion/Delayed Union: Minimized by utilizing rigid 3.5-mm DCP/LC-DCP fixation, reestablishing the medullary canal, and aggressively utilizing autogenous bone graft for any structural gaps or sclerotic interfaces.
You Might Also Like