Femoroacetabular Impingement: Comprehensive Surgical Management
Key Takeaway
Femoroacetabular impingement (FAI) is a pathologic biomechanical condition characterized by abnormal contact between the proximal femur and the acetabulum during terminal hip motion. This abutment leads to progressive chondrolabral dysfunction and is a primary precursor to secondary osteoarthritis of the hip. Management requires a meticulous understanding of cam and pincer pathomorphologies, precise radiographic evaluation, and advanced arthroscopic or open surgical techniques to restore impingement-free kinematics and preserve the native joint.
Introduction to Femoroacetabular Impingement
Femoroacetabular impingement (FAI) represents a dynamic, pathomechanical process defined by abnormal, premature contact between the proximal femur and the acetabulum during terminal ranges of motion. This pathologic abutment generates deleterious shear and compressive forces across the hip joint, leading to the progressive degradation of the acetabular labrum and adjacent articular cartilage. Historically, many cases of hip degeneration were classified as "idiopathic osteoarthritis"; however, pioneering work by Ganz et al., based on observations from over 600 surgical hip dislocations, established FAI as a primary etiologic factor in the development of secondary osteoarthritis of the hip.

The fundamental goal of recognizing and treating FAI is joint preservation. By identifying the specific morphological abnormalities and correcting them before irreversible chondral damage occurs, orthopedic surgeons can alter the natural history of the disease, alleviate pain, and restore high-level function to the patient.
Pathoanatomy and Classification
Ganz and colleagues delineated two distinct, yet frequently overlapping, morphological types of femoroacetabular impingement: Cam and Pincer impingement. While they are described as separate entities, the majority of patients (up to 86%) present with a mixed impingement pattern exhibiting features of both.
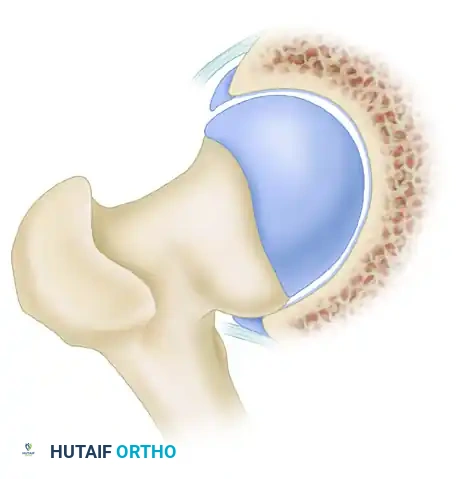
Cam Impingement
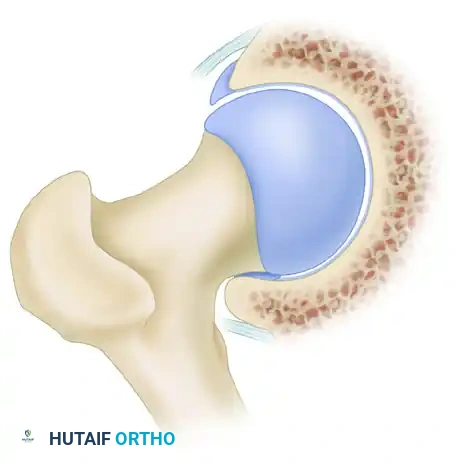
Cam impingement is predominantly observed in young, active male patients. It is characterized by an abnormally shaped, nonspherical femoral head with a decreased head-neck offset. This aspherical extension of the epiphysis (often referred to as a "pistol grip" deformity) creates a cam effect as the femoral head rotates into the acetabulum.
During dynamic hip flexion and internal rotation, the prominent cam lesion forcefully abuts the anterosuperior acetabular rim. Because the cam lesion is larger than the corresponding acetabular opening, it acts as a wedge, generating massive shear forces across the articular surface.
Over time, this repetitive shearing leads to delamination of the acetabular cartilage from the subchondral bone and subsequent avulsion or detachment of the labrum from the articular margin. The labrum itself is often pushed outward, resulting in an "outside-in" pattern of failure.
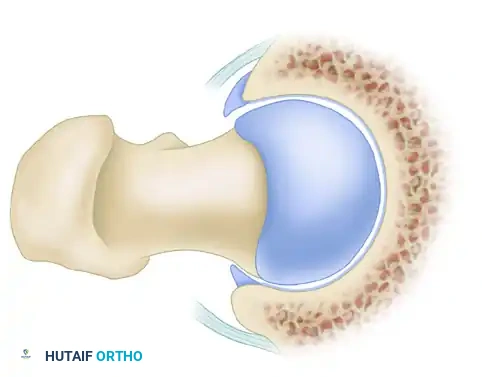
Pincer Impingement
Pincer impingement is most commonly identified in middle-aged women and is characterized by focal or global overcoverage of the femoral head by the acetabulum.

This overcoverage can manifest in several forms:
* Global Overcoverage: Seen in conditions such as coxa profunda or protrusio acetabuli.
* Focal Overcoverage: Typically observed in the anterosuperior acetabulum due to acetabular retroversion.
In pincer impingement, the abnormal contact occurs directly between the prominent acetabular rim and the structurally normal femoral head-neck junction. This linear contact crushes the labrum between the bone of the femoral neck and the acetabular rim, causing intrasubstance tears and ossification of the labrum.
Clinical Pearl: The Contrecoup Lesion
As pincer impingement progresses and the anterior femoral neck repeatedly strikes the anterior acetabular rim, the femoral head is levered out of the socket posteriorly. This subluxation force drives the posteromedial femoral head into the posteroinferior acetabulum, creating a secondary "contrecoup" chondral injury in the posterior joint space.

Clinical Evaluation
Patient History
Patients with FAI typically present with an insidious onset of groin pain. The pain is often described as a deep, aching discomfort that is exacerbated by athletic activities, pivoting, or prolonged periods of hip flexion. Patients frequently report the "C-sign," where they cup their hand over the greater trochanter with the thumb posterior and fingers deep in the anterior groin to localize the pain. Positional pain is a hallmark; patients often complain of discomfort when sitting in low chairs, driving for extended periods, or performing activities of daily living such as putting on socks and shoes. Mechanical symptoms, including clicking, catching, or locking, strongly suggest an associated labral tear or loose chondral flap.
Physical Examination
A comprehensive examination begins with the observation of the patient's posture, pelvic tilt, and gait mechanics. Palpation of the anterior joint structures rarely reproduces the deep joint pain, though secondary trochanteric bursitis or iliopsoas tenderness may be present.
Range of motion (ROM) testing is critical. Both hips must be evaluated to identify asymmetrical motion. The affected hip classically demonstrates restricted internal rotation, particularly when measured in 90 degrees of flexion.
The Impingement Test (FADIR):
The anterior impingement test is the most sensitive physical examination maneuver for FAI. With the patient supine, the examiner passively flexes the hip to 90 degrees, then applies adduction and internal rotation. A positive test reproduces the patient's characteristic sharp groin pain, indicating anterosuperior chondrolabral abutment.


The FABER Test:
The FABER (Flexion, Abduction, External Rotation) test is also utilized. The patient's ankle is placed above the contralateral knee, and the symptomatic knee is allowed to fall toward the examination table. In patients with FAI or associated intra-articular pathology, the distance from the lateral knee to the table is often increased compared to the contralateral side, and the maneuver may provoke lateral or posterior hip pain.
Radiographic Evaluation
A meticulous radiographic analysis is paramount for diagnosing FAI, classifying the morphology, and planning surgical intervention. The standard imaging protocol should include an anteroposterior (AP) pelvis, a false profile view, and lateral views of the hip (cross-table lateral, frog-leg lateral, or Dunn view).
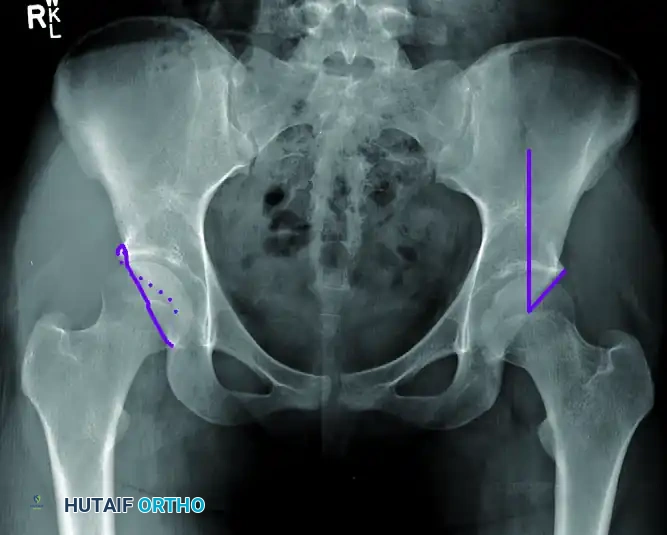
The AP Pelvis Radiograph
The AP pelvis must be perfectly standardized to accurately assess acetabular version. A well-centered view is confirmed when the tip of the coccyx points directly to the symphysis pubis, and the distance between the coccyx and the symphysis is exactly 1 to 2 cm.
On this view, the surgeon must evaluate for:
* Coxa Profunda: Diagnosed when the floor of the acetabular fossa (teardrop) touches or crosses medial to the ilioischial line.
* Protrusio Acetabuli: Diagnosed when the femoral head itself lies medial to the ilioischial line.
* Acetabular Retroversion: Indicated by the "crossover sign." In a normal anteverted acetabulum, the anterior wall line remains medial to the posterior wall line. In retroversion, the anterior wall crosses lateral to the posterior wall in the superior aspect of the joint.

Center-Edge Angle (CEA):
The lateral center-edge angle of Wiberg assesses global acetabular coverage. It is formed by a vertical line drawn perpendicular to the transverse axis of the pelvis passing through the center of the femoral head, and a second line drawn from the center of the femoral head to the lateral edge of the acetabular sourcil. A CEA of less than 20 to 25 degrees indicates dysplasia (undercoverage), while an angle greater than 39 degrees suggests pincer overcoverage.
Lateral Radiographs and the Alpha Angle
Lateral views (particularly the 45-degree Dunn view) are optimal for evaluating femoral head sphericity and the anterior head-neck offset.
The Alpha Angle:
The alpha angle quantifies the severity of a cam lesion. It is constructed by drawing a best-fit concentric circle around the femoral head. A line is drawn through the central axis of the femoral neck to the center of the head. A second line is drawn from the center of the head to the exact point where the anterior cortical margin of the femoral head-neck junction deviates from the concentric circle. An alpha angle greater than 50 to 55 degrees is diagnostic of a cam deformity and loss of sphericity.
Advanced Imaging (CT and MRI)
- Computed Tomography (CT): 3D CT reconstructions are invaluable for preoperative planning. They provide a precise topographic map of the cam lesion and allow for accurate measurement of femoral version and acetabular morphology.
- Magnetic Resonance Imaging (MRI / MRA): MRI, particularly MR arthrography with intra-articular gadolinium, is the gold standard for evaluating the soft-tissue envelope. It provides high-resolution visualization of labral tears, chondral delamination, and subchondral edema.
Indications and Nonoperative Management
Initial management of FAI is strictly nonoperative. The protocol includes:
1. Activity Modification: Avoidance of deep flexion and pivoting activities.
2. Pharmacotherapy: Nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce capsular and synovial inflammation.
3. Physical Therapy: Focused on core stabilization, pelvic tilt control, and strengthening of the hip abductors and external rotators to optimize dynamic joint kinematics.
Surgical Indications:
Patients who fail a comprehensive 3-to-6-month trial of conservative management are candidates for surgical intervention. The ideal surgical candidate has symptomatic FAI, radiographic evidence of correctable cam or pincer morphology, and minimal to no preexisting osteoarthritis (Tonnis Grade 0 or 1).
Surgical Warning:
Several outcome studies have definitively shown that patients with preexisting moderate-to-severe osteoarthritis (joint space < 2 mm or Tonnis Grade 2/3) experience little to no clinical improvement following FAI surgery and have a high rate of early conversion to Total Hip Arthroplasty (THA).
Surgical Management: Arthroscopic Technique
The primary goals of FAI surgery are to repair or debride labral pathology, stabilize chondral lesions, remove all sites of bony impingement, and reestablish a normal, impingement-free femoral head-neck offset. While open surgical dislocation remains a powerful tool, hip arthroscopy has become the standard of care due to lower morbidity and faster rehabilitation.
1. Patient Positioning and Setup
The procedure is performed under general anesthesia with profound muscle relaxation. The patient is placed supine on a specialized hip distraction table. A well-padded, oversized perineal post is utilized to minimize the risk of pudendal nerve neuropraxia. The operative leg is placed in slight flexion, 15 degrees of internal rotation, and neutral abduction. Traction is applied under fluoroscopic guidance to achieve a minimum of 10 mm of joint distraction, breaking the suction seal of the hip.
2. Portal Placement
Precise portal placement is critical to avoid neurovascular injury and achieve optimal trajectory for anchors and osteotomes.
* Anterolateral (AL) Portal: Established first under fluoroscopic guidance, entering the joint just superior and anterior to the tip of the greater trochanter. This portal avoids the superior gluteal nerve and lateral femoral cutaneous nerve (LFCN).
* Midanterior Portal (MAP): Established under direct arthroscopic visualization from the AL portal. It is placed approximately 5 to 7 cm distal and slightly anterior to the AL portal, traversing the interval between the tensor fasciae latae and the sartorius. This portal is essential for anchor placement during labral repair.
3. Central Compartment Arthroscopy
Once portals are established, an interportal capsulotomy is performed parallel to the acetabular rim to allow instrument maneuverability. The central compartment is systematically inspected.

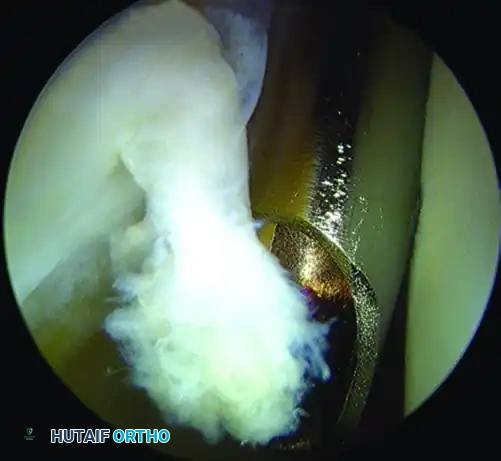
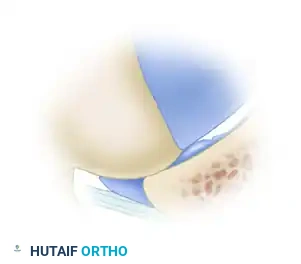
Figure: Arthroscopic view demonstrating articular cartilage sheared from the subchondral bone of the acetabulum, a classic finding in cam impingement.
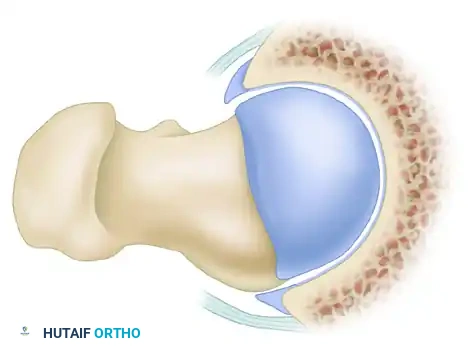
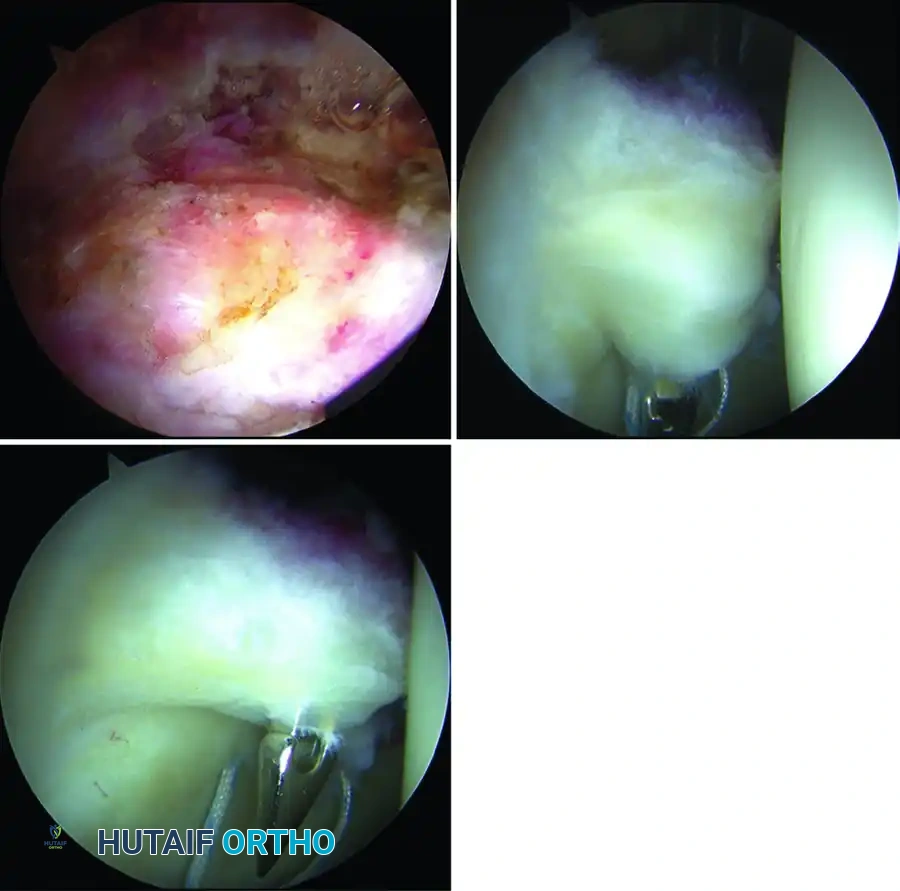
Figure: Arthroscopic view of a complex labral tear.
Pincer Resection and Labral Repair:
If a pincer lesion is present, the labrum is carefully detached from the overhanging bone. A motorized burr is used to perform an acetabular rim trimming, resecting the bony overcoverage until a normal center-edge angle is achieved. Following rim resection, the subchondral bone is decorticated to a bleeding bed. Suture anchors are placed precisely on the acetabular rim, and the labrum is refixed using looped or mattress suture configurations to restore the critical suction seal of the joint.
4. Peripheral Compartment Arthroscopy
Following central compartment work, traction is released. The hip is flexed to 45 degrees to relax the anterior capsule, allowing the arthroscope to enter the peripheral compartment.
Cam Resection (Osteochondroplasty):
The cam lesion is visualized on the anterior and anterolateral femoral head-neck junction. Using a high-speed burr, the surgeon performs a femoral osteochondroplasty. The resection begins at the articular cartilage margin and extends distally along the femoral neck to recreate a concave, spherical offset.
Surgical Pitfall: Over-resection
While adequate resection is necessary to prevent residual impingement, aggressive bony removal risks iatrogenic femoral neck fracture. In a landmark cadaveric study, Mardones et al. demonstrated that up to 30% of the anterolateral femoral head-neck junction can be safely resected without producing a statistically significant increase in the risk of femoral neck fracture. Resection depth should be continuously monitored with dynamic fluoroscopy.
5. Dynamic Testing and Capsular Closure
After the osteochondroplasty is complete, the hip is taken through a full, dynamic range of motion under direct arthroscopic visualization to confirm that all impingement has been eliminated and that the labral repair is stable. Finally, the capsulotomy is meticulously closed with high-strength sutures. Capsular closure is highly recommended to prevent postoperative microinstability, particularly in young, athletic patients or those with borderline dysplasia.
Postoperative Protocol and Clinical Outcomes
Rehabilitation
Postoperative rehabilitation is phased and strictly controlled to protect the labral repair and the femoral neck osteochondroplasty.
* Phase 1 (0-4 weeks): Flat-foot weight-bearing (20 lbs) with crutches. A hip brace is often used to limit flexion to 90 degrees and prevent external rotation. Continuous passive motion (CPM) or stationary biking without resistance is initiated early to prevent adhesions.
* Phase 2 (4-8 weeks): Progression to full weight-bearing. Focus shifts to restoring normal gait mechanics, core stability, and isometric abductor strengthening.
* Phase 3 (8-12 weeks): Advanced strengthening, dynamic balance, and closed-chain exercises.
* Phase 4 (3-6 months): Sport-specific training, plyometrics, and gradual return to play.
Clinical Outcomes
The literature demonstrates excellent outcomes following the surgical correction of FAI in properly selected patients.
* Return to Sport: Philippon et al. reported exceptional results in professional athletes. In a cohort of 28 professional hockey players treated arthroscopically for FAI, 100% returned to skating, with an average return-to-sport time of just 3.8 months. The average modified Harris Hip Score (mHHS) in this cohort improved dramatically from 70 preoperatively to 95 postoperatively.
* Adolescent Outcomes: Similar robust improvements are noted in adolescent athletes, with average mHHS increases of 35 points at short-term follow-up.
* Surgical Approach Comparison: In a comprehensive literature review, Botser et al. found that patients improved significantly regardless of the surgical approach (arthroscopic, open surgical dislocation, or mini-open). However, the data indicated that a higher percentage of professional athletes successfully returned to their sport following arthroscopic treatment compared to open surgical dislocation, likely due to the preservation of the abductor musculature and reduced surgical morbidity.
In conclusion, the successful management of femoroacetabular impingement relies on a high index of clinical suspicion, precise radiographic quantification of the deformity, and meticulous surgical execution to restore joint biomechanics and preserve the longevity of the hip.
You Might Also Like